

Abstract
Pregnancy may predispose to paroxysmal supraventricular tachycardia (SVT), in subjects with or without identifiable heart disease. Many physiological conditions such as autonomic nervous system changes, altered systemic hemodynamics, etc. can contribute to the onset of arrhythmias during pregnancy. Some cases reported the occurrence of arrhythmias in relation to systemic fluid variations. We report the case of a pregnant woman who experienced SVT due to fluid depletion, detected by bioimpedance vector analysis (BIVA), which was successfully treated by water repletion under tight BIVA monitoring. Emergency physicians can overcome dangerous drug administration by considering historical examination and using fast and reproducible techniques such as BIVA.
Keywords: arrhythmias, bioimpedance vector analysis, hydration, pregnancy
1. INTRODUCTION
Pregnancy may predispose to exacerbation or new onset of paroxysmal supraventricular tachycardia (SVT) (Nakagawa et al., 2004; Tan & Lie, 2001; Tawam et al., 1993) in subjects with or without identifiable heart disease (Robins & Lyons, 2004; Shotan, Ostrzega, Mehra, Johnson, & Elkayam, 1997). Humoral, hemodynamic, and autonomic nervous system changes can promote its occurrence and maintenance (Kay & Priano, 1987). The upright position can trigger SVT due to the increase in sympathetic activity related to blood volume and cardiac output (Hammill et al., 1984).
During pregnancy, the autonomic nervous system shows sequential changes: the increase in blood volume in the first trimester lowers sympathetic and intensifies vagal activities (Kuo, Chen, Yang, Lo, & Tsai, 2000; Yoshimura et al., 1994). Bioimpedance vector analysis (BIVA) and hemoglobin/hematocrit variations can indirectly and noninvasively outline plasma volume variations and their influence on heart performance (Di Somma et al., 2012; Dill & Costill, 1974; Lukaski, Siders, Nielsen, & Hall, 2007; Massari et al., 2016). All of these changes can enhance the occurrence of SVT during pregnancy (Kay & Priano, 1987; Robins & Lyons, 2004; Shotan et al., 1997; Tawam et al., 1993).
The treatment of SVT during pregnancy is challenging. Aside from the physio‐pathological consequences, the major issue is related to the safety of the pharmacological treatment during pregnancy. Most antiarrhythmic drugs cross the placenta and potential adverse effects can affect the fetus (Task Force on the Management of Cardiovascular Diseases During Pregnancy of the European Society of Cardiology 2003). Therefore, new safer approaches are needed in order to overcome the limitation of the existing pharmacological treatments. This case report provides new insights into this issue.
2. CASE REPORT
In March 2015, a 26‐year‐old pregnant woman (at thirteenth week gestation in a first pregnancy) was admitted to the Emergency Department of “F. Perinei” Hospital complaining of palpitations and fainting.
A 12‐lead ECG showed a narrow‐QRS complex tachycardia (180 beats/min) when in the upright position which disappeared in the supine position (Figure 1a).
Figure 1.
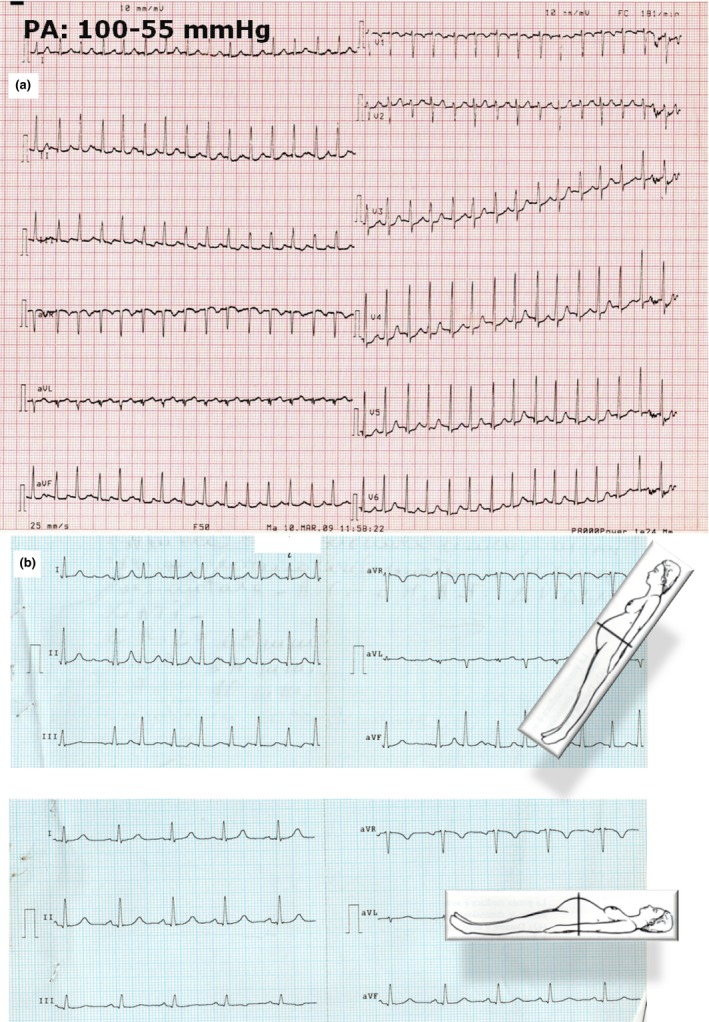
(a) The ECG of the subject on admission to the emergency department. (b) Variation in arrhythmia onset: arrhythmia onset in the upright position (upper strip); disappearance of the arrhythmia in the supine position (lower strip)
The subject had no history of heart disease nor previous episodes of palpitations. No pharmacological history was outlined. Arterial pressure was 100/55 mm Hg and the subject continued to present tachycardia. Cardiac and pulmonary assessments were normal. The subject admitted to having autonomously reduced hydro‐saline intake in the weeks prior to hospital admission in order to counteract a slight increase in systemic blood pressure.
Transthoracic echocardiography as well as fetal echocardiography were normal.
Blood tests, urea and electrolyte and liver and thyroid function tests were normal. In particular, we noticed a slight increase in total white blood cells: 12,600/mm3 (normal range [nr]: 4,300–10,000/mm3) and red blood cell distribution width (RDW): 14.8% (nr: 11.5–14.5%), while a slight decrease in creatinine: 0.34 mg/dl (nr: 0.5‐1.2 mg/dl) was observed. The slightly higher RDW values in parallel with normal mean corpuscular volume (MCV) and hemoglobin values could have suggested anemia masked by dehydration, but all of these are unspecific conditions. BNP was extremely lower than normal (BNP: 41 pg/ml, nr: 145‐250 pg/ml), which could also have revealed a nonspecific dehydration condition.
ECG Holter suggested an “adrenergic drive” of the arrhythmias due to sleep suppression of the arrhythmias and their predominant daytime distribution (Figure 2a). In order to decide on a suitable drug to administer and bearing in mind the clinical history of the subject (i.e., the restricted intake of water and mineral salt in the previous weeks), the woman was evaluated by BIVA (Cardio‐EFG, Akern) in order to determine total body water composition. The use of BIVA was suggested based on the subject's personal decision to reduce hydro‐saline intake in the weeks prior to hospital admission.
Figure 2.
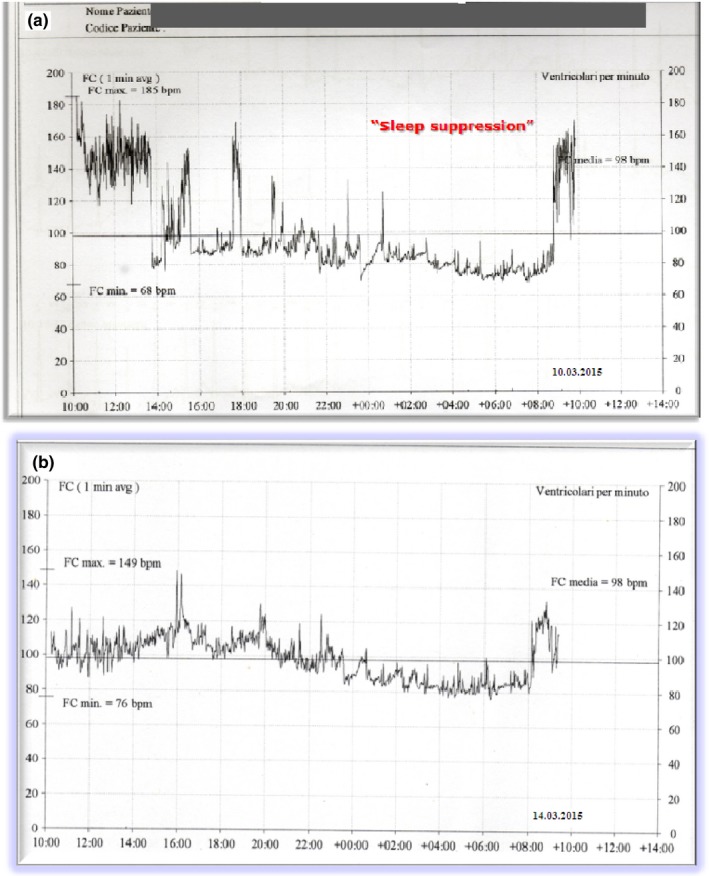
(a) Variation in heart rate from admission till 24 hr after arrhythmia onset at ECG Holter monitoring: note the daily onset of arrhythmic events and their sleep suppression. (b) Heart rate variation at ECG Holter monitoring on day 4 from admission
Dedicated software (Bodygram 1.4, Akern RJL Systems, Florence, Italy) estimated body hydration and percentage of fat free mass (Lukaski, et al., 2007; Massari et al., 2016). BIVA documented a dehydration condition (biavector at the upper pole of the seventy‐fifth percentile) (Figure 3). Therefore, treatment with 500 cc infusion of physiological saline solution at 5% NaCl per day was begun rather than drug administration while inviting the subject to drink at least 1,500 cc of water per day. The progressive hydration status normalized on days four and five (biavector in Figure 3, third point). Plasma volume and BNP values progressively increased [plasma volume: day 4 = 9.8%, day 5 = 37.9%; BNP: 252 pg/ml day 5).
Figure 3.
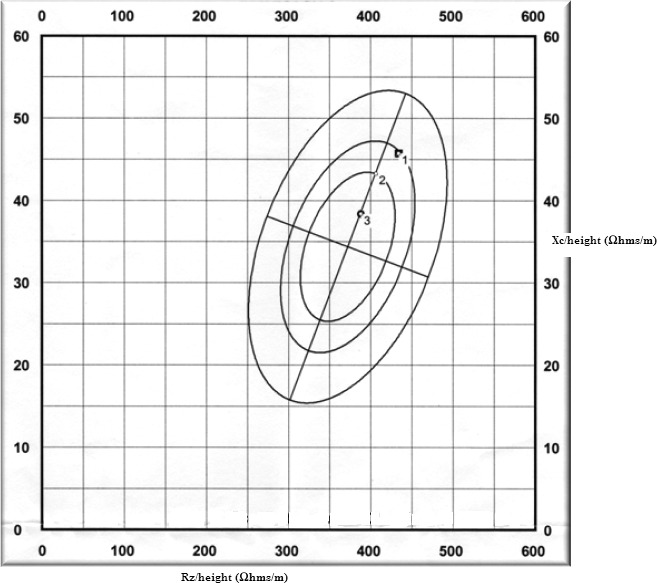
Semiquantitative analysis by mean of biavector impedance analysis. Point n.1 indicates the evaluation on admission: its position at the upper pole of the seventy‐fifth percentile indicates dehydration (Hydration Index [HI] 71%). Points n. 2 (HI: 72%) and n.3 (HI: 73%) indicate the progressive improvement in hydration due to fluid infusion
On day 4, the arrhythmia regressed (Figure 1b) and no other arrhythmic signs were observed in the clinical and ECG monitoring of the subject. A net clinical benefit for the subject (Figures 2b and 4) was determined without the use of anti‐arrhythmic drugs.
Figure 4.

ECG on day 4 from admission
3. DISCUSSION
The possible action of the entire fluid load within the treatment of cardiovascular diseases is still a question of debate (De Vecchis, Baldi, Cioppa, Giasi, & Fusco, 2016; Mestan, Babu, & Kvasnicka, 2006). Fluid depletion is able to improve atrial contraction, increase heart rate and shorten atrioventricular conduction time, possibly through adrenergic activation (Mestan et al., 2006). A reduction in body fluid load may activate baroreceptors in the carotid sinus, thus promoting sympathetic activation. Sympathetic nervous system mediators seem to shorten the ventricular refractory period and action potential duration and promote a nonuniform cardiac anisotropy which can induce the dispersion of muscle cell refractoriness (which increases susceptibility to arrhythmias) (Ng, 2016). Narayan, Drinan, Lackey, and Edman (2007) observed that the acute volume overload in dogs with structurally normal hearts was able to elevate T‐wave alternans, thus influencing the occurrence of arrhythmias. The ventricular stretching of the muscular cardiac fibers can effectively promote changes in repolarization and conduction of the action potential. Such considerations increase the importance of a full evaluation of subject hydration on admission. The combined use of clinical information, BIVA evaluation and biochemical data related to BNP values can provide initial insights into the hydration conditions of such subjects and new advances in the understanding of pregnancy arrhythmias. This case report showed the clinical application of such considerations in a real clinical setting related to a pregnant woman, i.e., a person for whom anti‐arrhythmic drugs are forbidden or dangerous (Cox & Gardner, 1993; Fagih & Sami, 1999; Joglar & Page, 1999; Page, 1995). To the best of our knowledge, this is the first article showing these results. Clinical and better organized trials should be planned in order to improve knowledge on this issue.
CONFLICT OF INTEREST
The authors report no conflicts of interest.
Massari F, Scicchitano P, Potenza A, et al. Supraventricular tachycardia, pregnancy, and water: A new insight in lifesaving treatment of rhythm disorders. Ann Noninvasive Electrocardiol. 2018;23:e12490 10.1111/anec.12490
REFERENCES
- Cox, J. L. , & Gardner, M. J. (1993). Treatment of cardiac arrhythmias during pregnancy. Progress in Cardiovascular Diseases, 36, 137–178. [DOI] [PubMed] [Google Scholar]
- De Vecchis, R. , Baldi, C. , Cioppa, C. , Giasi, A. , & Fusco, A. (2016). Effects of limiting fluid intake on clinical and laboratory outcomes in patients with heart failure: Results of a meta‐analysis of randomized controlled trials. Herz, 41, 63–75. [DOI] [PubMed] [Google Scholar]
- Di Somma, S. , Navarin, S. , Giordano, S. , Spadini, F. , Lippi, G. , Cervellin, G. , … Maisel, A. S. (2012). The emerging role of biomarkers and bio‐impedance in evaluating hydration status in patients with acute heart failure. Clinical Chemistry and Laboratory Medicine, 50, 2093–2105. [DOI] [PubMed] [Google Scholar]
- Dill, D. B. , & Costill, D. L. (1974). Calculation of percentage changes in volumes of blood, plasma, and red cells in dehydration. Journal of Applied Physiology, 37, 247–248. [DOI] [PubMed] [Google Scholar]
- Fagih, B. , & Sami, M. (1999). Safety of antiarrhythmics during pregnancy: Case report and review of the literature. Canadian Journal of Cardiology, 15, 113–117. [PubMed] [Google Scholar]
- Hammill, S. C. , Holmes, D. R. Jr , Wood, D. L. , Osborn, M. J. , McLaran, C. , Sugrue, D. D. , … Gersh, B. J. (1984). Electrophysiologic testing in the upright position: Improved evaluation of patients with rhythm disturbances using a tilt table. Journal of the American College of Cardiology, 4, 65–71. [DOI] [PubMed] [Google Scholar]
- Joglar, J. A. , & Page, R. I. (1999). Treatment of cardiac arrhythmias during pregnancy; safety considerations. Drug Safety, 20, 85–94. [DOI] [PubMed] [Google Scholar]
- Kay, J. , & Priano, L. L. (1987). Paroxysmal atrial tachycardia in pregnancy. Anesthesiology Review, 14, 8–15. [Google Scholar]
- Kuo, C. D. , Chen, G. Y. , Yang, M. J. , Lo, H. M. , & Tsai, Y. S. (2000). Biphasic changes in autonomic nervous activity during pregnancy. British Journal of Anaesthesia, 84, 323–329. [DOI] [PubMed] [Google Scholar]
- Lukaski, H. C. , Siders, W. A. , Nielsen, E. J. , & Hall, C. B. (2007). Assessment of change in hydration in women during pregnancy and postpartum with bioelectrical impedance vectors. Nutrition, 23, 543–550. [DOI] [PubMed] [Google Scholar]
- Massari, F. , Iacoviello, M. , Scicchitano, P. , Mastropasqua, F. , Guida, P. , Riccioni, G. , … Di Somma, S. (2016). Accuracy of bioimpedance vector analysis and brain natriuretic peptide in detection of peripheral edema in acute and chronic heart failure. Heart and Lung, 45, 319–326. [DOI] [PubMed] [Google Scholar]
- Mestan, M. , Babu, A. , & Kvasnicka, J. (2006). The influence of fluid and diuretic administration on the index of atrial contribution in sequentially paced patients. Europace, 8, 273–278. [DOI] [PubMed] [Google Scholar]
- Nakagawa, M. , Katou, S. , Ichinose, M. , Nobe, S. , Yonemochi, H. , Miyaakawa, I. , … Saikawa, T. (2004). Characteristics of new‐onset ventricular arrhythmias in pregnancy. Journal of Electrocardiology, 37, 47–53. [DOI] [PubMed] [Google Scholar]
- Narayan, S. M. , Drinan, D. D. , Lackey, R. P. , & Edman, C. F. (2007). Acute volume overload elevates T‐wave alternans magnitude. Journal of Applied Physiology (1985), 102, 1462–1468. [DOI] [PubMed] [Google Scholar]
- Ng, G. A. (2016). Neuro‐cardiac interaction in malignant ventricular arrhythmia and sudden cardiac death. Autonomic Neuroscience, 199, 66–79. [DOI] [PubMed] [Google Scholar]
- Page, R. L. (1995). Treatment of arrhythmias during pregnancy. American Heart Journal, 130, 871–876. [DOI] [PubMed] [Google Scholar]
- Robins, K. , & Lyons, G. (2004). Supraventricular tachycardia in pregancy. British Journal of Anaesthesia, 92, 140–143. [DOI] [PubMed] [Google Scholar]
- Shotan, A. , Ostrzega, E. , Mehra, A. , Johnson, J. V. , & Elkayam, U. (1997). Incidence of arrhythmias in normal pregnancy and relation to palpitations, dizziness, and syncope. American Journal of Cardiology, 79, 1061–1064. [DOI] [PubMed] [Google Scholar]
- Tan, H. L. , & Lie, K. I. (2001). Treatment of tachyarrhythmias during pregnancy and lactation. European Heart Journal, 22, 458–464. [DOI] [PubMed] [Google Scholar]
- Task Force on the Management of Cardiovascular Diseases During Pregnancy of the European Society of Cardiology (2003). Expert consensus document on managment of cardiovascular disease during pregnancy. European Heart Journal, 24, 761–781. [DOI] [PubMed] [Google Scholar]
- Tawam, M. , Levine, J. , Mendelson, M. , Goldenberger, J. , Dyer, A. , & Kadish, A. (1993). Effect of pregnancy on paroxysmal supraventricular tachycardia. American Journal of Cardiology, 72, 838–840. [DOI] [PubMed] [Google Scholar]
- Yoshimura, T. , Yoshimura, M. , Yasue, H. , Ito, M. , Okamura, H. , Mukoyama, M. , … Nakao, K. (1994). Plasma concentration of atrial natriuretic peptide and brain natriuretic peptide during normal human pregnancy and the postpartum period. Journal of Endocrinology, 140, 393–397. [DOI] [PubMed] [Google Scholar]