

Abstract
A woman (49 years) with Chagas’ disease showed: ECG, right bundle‐branch block and left anterior–superior fascicular block; V1 has unusual R > R’, and elevated ST segment from V2 to V6. Additional imaging revealed concomitant HCM and Chagas, which is uncommon. Overlapping of ECG findings can be explained by this rare association of diseases.
Keywords: electrocardiography; Chagas heart failure; hypertrophic cardiomyopathy; echocardiography, 3D; magnetic resonance angiography
BACKGROUND
Chagas’ disease (CD) is an important health problem in Latin America, and cardiac involvement is associated with significant morbidity and mortality.1 Hypertrophic cardiomyopathy (HCM) is the most common genetic cardiac disease and can have extremely heterogeneous presentations. A subgroup of patients within this broad spectrum show left ventricular (LV) apical aneurysm in the absence of coronary artery disease.2
CASE PRESENTATION
A 49‐year‐old white female with hypertension, type 2 diabetes mellitus and Chagas’ disease came to the Electrocardiography Unit of the Heart Institute (InCor) of University of São Paulo Medical School Hospital, with complaints of sporadic, tachycardic palpitations. She was referred to diagnostic testing, with the following results:
ECG (Fig. 1 ): her electrocardiogram (ECG) revealed a right bundle‐branch block (RBBB) associated to left anterior–superior fascicular block (LASFB), which is a characteristic pattern in Chagas’ disease (CD). However, the QRS complex in V1 has an R wave taller than R’. There was also ST segment elevation from V2 to V6, as well as in the inferior wall. A characteristic repolarization +/− pattern was observed in V2–V6.
3D Echocardiogram (Fig. 2 ): a 3D‐echocardiogram showed normal diameter and ventricular function, significant hypertrophy in the apical area of the left ventricle (LV), with no dynamic obstruction of the outflow tract.
Coronary angiography (Fig. 3 ): a coronary angiography confirmed absence of obstructive lesion; additionally, the left ventriculography showed a “spade‐like” configuration.
Magnetic resonance imaging (Fig. 4 ): a magnetic resonance imaging showed preserved biventricular systolic function, hypertrophic cardiomyopathy (HCM) with apical predominance and a dyskinetic apex; also, there was nonischemic myocardial fibrosis in anterior, lateral and inferior walls.
Figure 1.
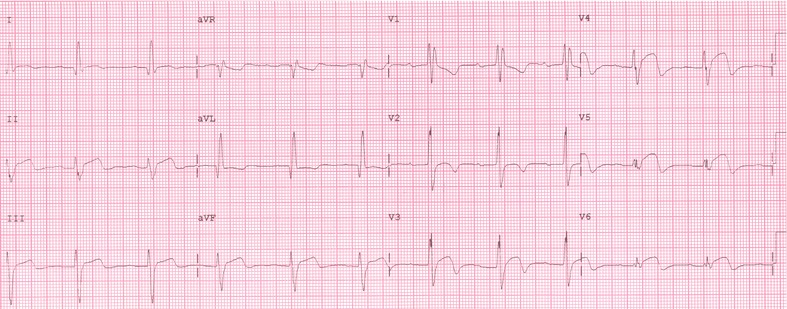
ECG: right bundle‐branch block (RBBB) associated to left anterior–superior fascicular block (LASFB), (characteristic pattern in Chagas’ disease). However, V1 has R > R’, in addition to ST segment elevation from V2 to V6 and in inferior wall, with +/− pattern in V2–V6.
Figure 2.
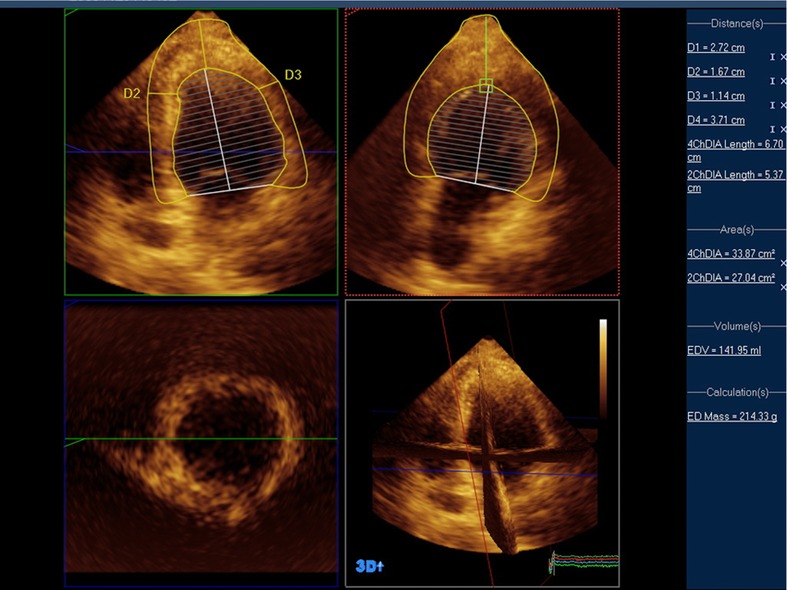
3D echocardiogram: diameter and ventricular function are normal, with significant hypertrophy in the apical area of the left ventricle (LV), and no dynamic obstruction of the outflow tract.
Figure 3.
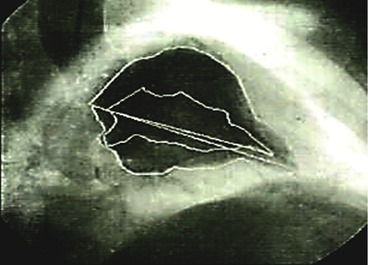
Coronary angiography: absence of obstructive lesion; left ventriculography with “spade‐like” configuration.
Figure 4.

Magnetic resonance imaging: preserved biventricular systolic function, hypertrophic cardiomyopathy (HCM) with apical predominance and dyskinetic apex; nonischemic (38 g) myocardial fibrosis in anterior, lateral and inferior walls.
DISCUSSION
The most common ECG finding in Chagas' disease (>50%) is RBBB associated to LASFB,3, 4, 5 followed by various degrees of atrioventricular blocks,3, 4, 5, 6, 7 in addition to ventricular repolarization abnormalities (ST segment and T wave).8 In the present case report, the ECG presented that common association of RBBB and LASFB, with a peculiar R wave taller than R’ in V1. Regarding the repolarization, there was a characteristic pattern that could lead us to consider the existence of a left ventricular aneurism. Apical aneurism is reported in 10% cases of Chagas’ disease.1
In HCM cases nearly 93% ECG results are abnormal, and these alterations are detected sooner by ECG, which is more sensitive than echocardiography for such detection.9 Ventricular repolarization changes are usually the most common and outstanding aspect, with down sloping J point and giant negative T waves (≥10 mm) in the precordial leads.10 Nonobstructive forms of ventricular hypertrophy in asymptomatic patients are observed in 58% of cases.11 In our case, the R wave taller than R’ in V1 could be explained by a possible septal enlargement, since the first vector (r wave in V1) is related to the septum activation. The characteristic giant negative T waves were not found in our case, but the ST segment elevation in V2–V6 could represent a left ventricular aneurism; however, this is scarcely found in HCM patients (2%).2 In both diseases the main electrocardiographic alteration found is ST elevation (>1 mm) from V3 to V5 .12
A “spade‐like” shape of the LV, as detected by left ventriculography, is also a characteristic finding in HCM.10 Echocardiography and MRI results confirmed left ventricular hypertrophic cardiomyopathy in the apical area.
Concomitant hypertrophic cardiomyopathy and Chagas’ disease is not commonly reported in the literature. Only one of these conditions could not explain all the ECG abnormalities. The overlapping of ECG findings in the present case report could indicate the rare association of these two diseases. This hypothesis can be confirmed by the results found in our imaging tests.
REFERENCES
- 1. Rassi A Jr, Rassi A, Little WC, et al. Development and validation of a risk score for predicting death in Chagas’ heart disease. N Engl J Med 2006;355:799–808. [DOI] [PubMed] [Google Scholar]
- 2. Efthimiadis GK, Pliakos C, Pagourelias ED, et al. Hypertrophic cardiomyopathy with midventricular obstruction and apical aneurysm formation in a single family: Case report. Cardiovasc Ultrasound 2009;7:26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Dias JC, Kloetzel K. The prognostic value of the electrocardiographic features of chronic Chagas’ disease. Rev Inst Med Trop São Paulo. 1968;10(3):158–162. [PubMed] [Google Scholar]
- 4. Maguire JH, Mott KE, Lehman JS, et al. Relationship of electrocardiographic abnormalities and seropositivity to Trypanosoma cruzi within a rural community in northeast Brazil. Am Heart J 1983;105(2):287–294. [DOI] [PubMed] [Google Scholar]
- 5. Rosenbaum MB, Alvarez AJ. The electrocardiogram in chronic chagasic myocarditis. Am Heart J 1955;50(4):492–527. [DOI] [PubMed] [Google Scholar]
- 6. Maguire JH, Holf R, Sherlock I, et al. Cardiac morbity due to Chagas heart disease. Circulation 1987;75(6):1140–1145. [DOI] [PubMed] [Google Scholar]
- 7. Porto CC. O eletrocardiograma no prognóstico e evolução da doença e Chagas. Arq Bras Cardiol 1964;17:313–346. [PubMed] [Google Scholar]
- 8. Gonçalves JGF, Prata A. Estudo comparativo de três códigos para leitura de eletrocardiogramas na doença de Chagas crônica. Pan Am J Public Health 2003;14:201–208. [DOI] [PubMed] [Google Scholar]
- 9. Al‐Mahadawi S, Chamberlain S, Chojnowska L, et al. The electrocardiogram is a more sensitive indicator than echocardiography of hypertrophic cardiomyopathy in families with a mutation in the MYH7 gene. Br Heart J 1994;72:105–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Yamaguchi H, Ishimura T, Nishiyama S, et al. Hypertrophic nonobstructive cardiomyopathy with giant negative T waves (apical hypertrophy): Ventriculographic and echocardiographic features in 30 patients. Am J Cardiol 1979;44(3):401–412. [DOI] [PubMed] [Google Scholar]
- 11. Pérez‐Riera AR, de Lucca AA, Barbosa‐Barros R, et al. Value of electro‐vectorcardiogram in hypertrophic cardiomyopathy. Ann Noninvasive Electrocardiol 2013;18:311–326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Ichida M, Nishimura Y, Kazuomi K. Clinical significance of left ventricular apical aneurysms in hypertrophic cardiomyopathy patients: The role of diagnostic electrocardiography. J Cardiol 2014;64:265–272. [DOI] [PubMed] [Google Scholar]