

Abstract
Down syndrome occurs more frequently in the offsprings of older pregnant women and may be associated with atrioventricular septal defect. This refers to a broad spectrum of malformations characterized by a deficiency of the atrioventricular septum and abnormalities of the atrioventricular valves caused by an abnormal fusion of the superior and inferior endocardial cushions with the midportion of the atrial septum and the muscular portion of the ventricular septum.
Keywords: atrioventricular septal defect, intraventricular conduction disturbances, left anterior fascicular block, right bundle branch block, ventricular preexcitation
1. CASE REPORT
The mother of a 39‐year‐old male, carrier of down syndrome said she had been informed since his birth, when she was 41 years old, that her son had a “heart murmur.”
At the age of 17, cardiac catheterization was performed, and it revealed an ostium primum atrial septal defect, posterobasal ventricular septal defect, and mitral valve regurgitation consequence of a cleft in the posterolateral leaflet. The electrocardiogram (ECG) and vectorcardiogram (VCG) are shown in Figure 1.
Figure 1.
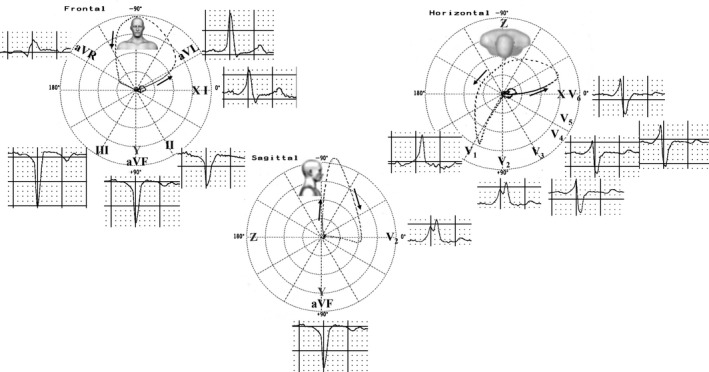
ECG/VCG before radiofrequency catheter ablation (RFCA). ECG: Short PR interval, QRS axis −75°, QRS duration 160 ms, δ waves, QS in II, III and aVF, RBBB pattern. VCG: The QRS loop leaves no doubt about the presence of LAFB in the frontal and horizontal planes (FP/HP) a typical RBBB VCG pattern with final conduction delay in the right anterior quadrant. Initial conduction delay in the three planes. Conclusion: ventricular preexcitation with posteroseptal accessory pathway (AP), atypical LAFB and RBBB
For about 3 months, he complained of fast palpitations, which resulted in several consultations in the emergency room, where ablation was recommended. After this procedure, ECG/VCG showed disappearance of ventricular preexcitation, and appearance of right bundle branch block (RBBB) associated with left anterior fascicular block (LAFB) (Figure 2).
Figure 2.
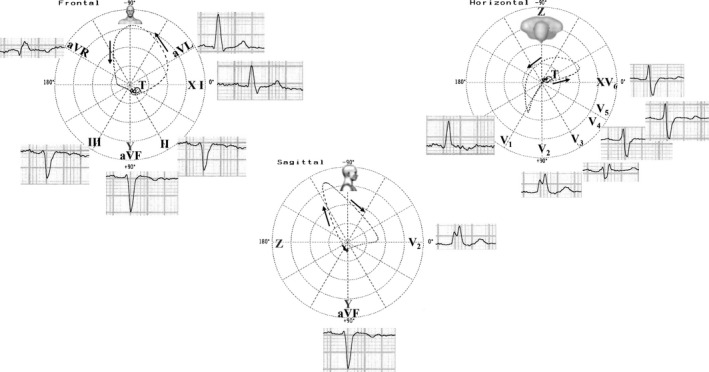
ECG/VCG after successful radiofrequency ablation. ECG: LAFB associated with RBBB. VCG: FP: initial vector directed downward, QRS loop with counterclockwise rotation and located predominantly in the upper left quadrant. HP: QRS loop with end conduction delay in the right anterior quadrant. Conclusion: LAFB + RBBB
2. DISCUSSION
We present a case of trisomy 21 in a young adult with AVSD. The patient presented rapid palpitations, probably due to ventricular preexcitation. The ablation of the accessory pathway (AP) unmasks a bifascicular block.
In the first ECG/VCG, the ventricular preexcitation in the FP partially conceals the LAFB, modifying only the initial portions of the QRS loop. Therefore, an rS pattern is present in the inferior leads. Due to the coexistence of an AP, the initial portions of the ventricular depolarization are directed to the left and above, originating a QS pattern in II, III and aVF, hiding LAFB. However, the remaining QRS loop shows counterclockwise rotation and left axis deviation, raising suspicion of LAFB. The ECG shows suspicion of RBBB pattern, but after ablative treatment, RBBB is evident.
The initial delay associated with the end indicates the association of ventricular preexcitation and RBBB.
Chiale and Elizari (2012) observed that the ECG diagnosis of intraventricular conduction disturbances may be hindered by the coexistence of ventricular preexcitation (Iturralde et al., 2006). In fact, the initial depolarization of ventricular myocardium through an AP tends to conceal any ECG manifestation of a bundle branch block and LAFB. This case presents unique aspects: (1) bifascicular block associated with ventricular preexcitation; (2) unmasking of RBBB and LAFB with disappearance of ventricular preexcitation.
3. CONCLUSION
We present the coexistence of bifascicular block and ventricular preexcitation demonstrated by ECG/VCG, unmasked with successful ablation.
CONFLICTS OF INTEREST
None.
Pérez‐Riera AR, Barbosa‐Barros R, Daminello‐Raimundo R, de Abreu LC, Nikus K. Electro‐vectorcardiographic demonstration of bifascicular block associated with ventricular preexcitation. Ann Noninvasive Electrocardiol. 2019;24:e12550 10.1111/anec.12550
REFERENCES
- Chiale, P. A. , & Elizari, M. V. (2012). The electrocardiographic diagnosis of intraventricular blocks coexisting with ventricular preexcitation. Journal of Electrocardiology, 45(5), 515–524. 10.1016/j.jelectrocard.2012.04.002 [DOI] [PubMed] [Google Scholar]
- Iturralde, P. , Nava, S. , Salica, G. , Medeiros, A. , Marquez, M. F. , Colin, L. , … Gonzalez, M. D. (2006). Electrocardiographic characteristics of patients with Ebstein's anomaly before and after ablation of an accessory atrioventricular pathway. Journal of Cardiovascular Electrophysiology, 17(12), 1332–1336. 10.1111/j.1540-8167.2006.00617.x [DOI] [PubMed] [Google Scholar]