

Abstract
A 28‐year‐old previously healthy male presented with nonprodromal syncope and a 4‐day history of chest pain, shortness of breath, and malaise. His ECG showed rapidly progressive high‐degree AV block. His Suspicious Index in Lyme Carditis (SILC) score was 8, indicating high risk for Lyme carditis. Lyme serology revealed to be positive (anti‐Lyme IgM). During the second day of hospitalization, the patient deteriorated his AV conduction, and a temporary–permanent pacemaker was implanted allowing ambulating in hospital the very same day. Temporary–permanent pacemakers for the management of transient high‐degree heart block associated with Lyme carditis were only occasionally used in the past.
Keywords: bradyarrhythmias, conduction disturbances, electrophysiology, implantable devices, lead implantation/extraction, pacemaker
1. INTRODUCTION
Lyme disease is a bacterial infection caused by Borrelia burgdorferi, transmitted through certain Ixodes tick species (PHA of Canada, 2015). Affected patients can present with erythema migrans (EM), arthralgias, neurologic symptoms, and systemic symptoms such as malaise and fatigue. When the bacteria invade the heart, it can lead to Lyme carditis (Krause & Bockenstedt, 2013; Scheffold, Herkommer, Kandolf, & May, 2015). Symptoms include chest pain, shortness of breath, palpitations, dizziness, and syncope as about 90% of patients with Lyme carditis will present with high‐degree AV block (McAlister et al., 1989; Wan et al., 2018). Diagnosis often proves to be challenging as many patients do not remember a previous exposure to tick bites and do not have EM. The use of the Suspicious Index in Lyme Carditis (SILC) score (Besant et al., 2018) may help identifying Lyme carditis (Table 1). In this case report, we describe a different technique to transiently pace the heart using temporary–permanent pacing (TPP) during symptomatic bradycardia associated with Lyme carditis.
Table 1.
The SILC (Suspicious Index in Lyme Carditis) score (Besant et al., 2018). 0–2 points indicate low probability of Lyme carditis in a patient presenting with high‐degree AV block and it should be treated as per standard management 3–6 intermediate risk and 7–12 high risk for Lyme carditis. We proposed patients with intermediate‐high risk scores to quickly obtain Lyme serology, start antibiotic treatment, and to use temporary–permanent pacing if bradycardia is symptomatic (see text)
| Variable | Value |
|---|---|
| Age <50 | 1 |
| Male | 1 |
| Outdoor activity/Endemic area | 1 |
| Constitutional symptoms | 2 |
| Tick bite | 3 |
| Erythema migrans | 4 |
2. CASE REPORT
A 28‐year‐old previously healthy human presents to the emergency department (ED) with a nonprodromal syncope episode and a 4‐day history of chest pain, shortness of breath, and malaise. He denied any medical issues, medications, or recreational drug use. His ED vital signs and physical exam were within normal limits. His laboratory results showed elevated inflammatory markers with a CRP of 94.5 mg/L and ESR of 44 mm/hr, as well as mildly elevated troponin of 51 ng/L. His ECG showed a junctional rhythm at 70 bpm. The patient lives in a Lyme disease endemic region and upon further questioning, the patient disclosed a history of a tick bite 1–2 months prior. Lyme disease serology was taken. The patient was admitted for cardiac monitoring and initiation of antibiotic therapy.
Despite appropriate IV antibiotic therapy, the patient evolved into high‐degree AV block (Figure 1) on his second day of admission. An echocardiogram showed mild global hypokinesis mostly affecting the inferior and infero‐septal walls. A TPP was inserted (2160 Endurity, 6F Tendril STS 2088TC lead; Abbott). In contrast to the typical temporary pacing used for reversible heart block, we used an externalized permanent pacemaker with screw‐in endocardial lead providing additional stability and allowing for early ambulation. The patient continued to improve and his ECG progressively normalized with restoration of 1:1 conduction (initially with long PR interval) by day 8. The TPP was removed 12 days postadmission and he was discharged home on oral antibiotics. A predischarge stress test showed 1:1 conduction up to 180 bpm. A follow‐up ECG was obtained at 5 weeks (Figure 2) showing normal sinus rhythm with no other alterations. A follow‐up echocardiogram was requested.
Figure 1.
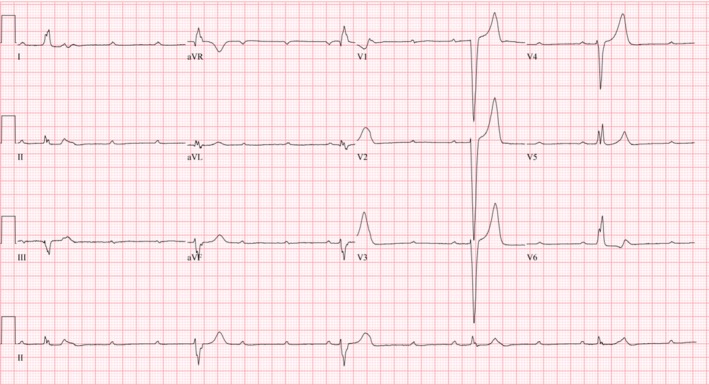
Rapidly progressive high‐degree AV block leading to insertion of a temporary–permanent pacemaker in a patient with early dissemination Lyme carditis
Figure 2.
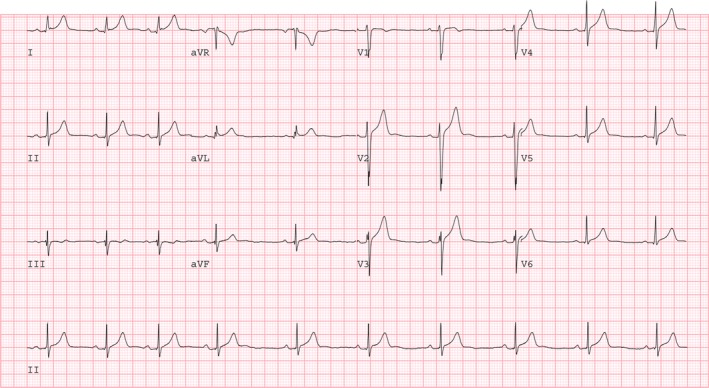
Resolution of high‐degree AV block. ECG obtained during first visit follow‐up
3. DISCUSSION
Lyme carditis is a rare complication of the B. burgdorferi infection affecting approximately 10% of reported cases (Krause & Bockenstedt, 2013). Patients may often first present with other features of Lyme disease such as cutaneous, neurologic, and joint manifestations. It is important to consider Lyme carditis in young patients who present with severe conduction abnormalities, especially if they live in a Lyme‐endemic region (Wan & Baranchuk, 2018). Though it can be difficult to diagnose high‐degree AV block associated with Lyme carditis, the SILC score identifies key risk factors through patient history (Table 1). Since most patients with Lyme carditis present with high‐degree AV block, it is important to recognize this reversible cause of heart block to prevent unnecessary permanent pacemaker implantation. Reversal of AV block can occur after days of initiating antibiotics (Fish, Pride, & Pinto, 2008; McAlister et al., 1989; Wan et al., 2018). Some patient with symptomatic bradycardia may require temporary pacing, leading to immobilization and increasing complications and costs. This is why we attempted the previously poorly explored opportunity of providing TPP for the management of this case. The “externalized” permanent pacemaker with temporary endocardial screw‐in leads maintains superior stability for many days when compared to the standard temporary pacemaker and allows early (almost immediate) mobilization of the patient (Dawood, Boerkircher, Rubery, Hire, & Soliman, 2016). Reversible causes of AV block are generally treated with transvenous temporary pacemakers, requiring prolonged bed‐rest and monitoring in the cardiac care unit due to the risk of lead dislodgement. Immobilization has been associated with complications such as loss of muscle mass and deconditioning, increased risk for venous thrombosis, and prolonged length of stay in hospital (Rion & Kautz, 2016). The use of the TPP enhances patient recovery and accelerates patients returning home. Only few cases of Lyme carditis have received TPP according to literature (Zei, Eckart, & Epstein, 2006), and this should be a technique to be considered during the course of symptomatic high‐degree AV block associated with early disseminated Lyme carditis.
4. CONCLUSION
We propose that TPP is a feasible and effective method to manage high‐degree AV block in Lyme carditis in conjunction with appropriate antimicrobial therapy. This may prevent the unnecessary implantation of permanent pacemakers and has the added benefit of allowing early mobilization when compared to traditional temporary pacemakers.
CONFLICT OF INTERESTS
None.
AUTHOR CONTRIBUTIONS
Dr. Chang Wang contributed to data interpretation and drafting of the article. Drs. Sanoj Chacko and Hoshiar Abdollah contributed to study concept and data collection. Dr. A. Baranchuk contributed to critical revision of the article.
Wang C, Chacko S, Abdollah H, Baranchuk A. Treating Lyme carditis high‐degree AV block using a temporary–permanent pacemaker. Ann Noninvasive Electrocardiol. 2019;24:e12599 10.1111/anec.12599
REFERENCES
- Besant, G. , Wan, D. , Blakely, C. , Branscombe, P. , Suarez‐Fuster, L. , Redfearn, D. , … Baranchuk, A. (2018). Lyme carditis presenting with high‐degree atrioventricular block: A systematic review. Journal of Electrocardiology. [Google Scholar]
- Dawood, F. Z. , Boerkircher, A. , Rubery, B. , Hire, D. , & Soliman, E. Z. (2016). Risk of early mortality after placement of a temporary‐permanent pacemaker. Journal of Electrocardiology, 49, 530–535. 10.1016/j.jelectrocard.2016.05.004 [DOI] [PubMed] [Google Scholar]
- Fish, A. E. , Pride, Y. B. , & Pinto, D. S. (2008). Lyme carditis. Infectious Disease Clinics of North America, 22, 275–288. vi. 10.1016/j.idc.2007.12.008 [DOI] [PubMed] [Google Scholar]
- Krause, P. J. , & Bockenstedt, L. K. (2013). Cardiology patient pages. Lyme disease and the heart. Circulation, 127, e451–e454. 10.1161/CIRCULATIONAHA.112.101485 [DOI] [PubMed] [Google Scholar]
- McAlister, H. F. , Klementowicz, P. T. , Andrews, C. , Fisher, J. D. , Feld, M. , & Furman, S. (1989). Lyme carditis: An important cause of reversible heart block. Annals of Internal Medicine, 110, 339–345. 10.7326/0003-4819-110-5-339 [DOI] [PubMed] [Google Scholar]
- PHA of Canada (2015). Surveillance of Lyme disease aem. Retrieved from https://www.canada.ca/en/public-health/services/diseases/lyme-disease/surveillance-lyme-disease.html. Published January 27, 2015.
- Rion, J. H. , & Kautz, D. D. (2016). The walk to save: Benefits of inpatient cardiac rehabilitation. MEDSURG Nursing Journal, 25, 159–162. [PubMed] [Google Scholar]
- Scheffold, N. , Herkommer, B. , Kandolf, R. , & May, A. E. (2015). Lyme carditis–diagnosis, treatment and prognosis. Deutsches Ärzteblatt International, 112, 202–208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wan, D. , & Baranchuk, A. (2018). Lyme carditis and atrioventricular block. Canadian Medical Association Journal, 190, E622–E622. 10.1503/cmaj.171452 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wan, D. , Blakely, C. , Branscombe, P. , Suarez‐Fuster, L. , Glover, B. , & Baranchuk, A. (2018). Lyme carditis and high‐degree atrioventricular block. American Journal of Cardiology, 121, 1102–1104. 10.1016/j.amjcard.2018.01.026 [DOI] [PubMed] [Google Scholar]
- Zei, P. C. , Eckart, R. E. , & Epstein, L. M. (2006). Modified temporary cardiac pacing using transvenous active fixation leads and external re‐sterilized pulse generators. Journal of the American College of Cardiology, 47, 1487–1489. 10.1016/j.jacc.2006.01.006 [DOI] [PubMed] [Google Scholar]