

Abstract
An 82‐year‐old female presented lasting chest pain for stimulation and the ECG revealed ventricular fibrillation and ST segment elevation, so we considered acute myocardial infarction. However, after the clinical condition of the patient improved, symptoms recurred for stimulation again on day 4. An echocardiogram showed left ventricular apical ballooning, so, we diagnosed her as Takotsubo syndrome.
Keywords: recurrence, Takotsubo syndrome, echocardiogram
Takotsubo syndrome is also known as Stress‐induced cardiomyopathy or left ventricular apical ballooning syndrome. For years, this disease is concerned more and more, because it is misdiagnosed as acute myocardial infarction generally. Takotsubo syndrome has been classified as acquired cardiomyopathy by AHA in 2006 and undefined cardiomyopathy by ESC in 2008. Recurrence of this disease is possible, and the majority of cases occur in 4 years, the present report is focused on a case of Takotsubo syndrome recurrence after 3 days.
CASE PRESENTATION
An 82‐year‐old female was transferred to the Emergency Department of the First Affiliated Hospital of Liaoning Medical College for the treatment of chest pain (lasting for 1 hour). Suddenly, ventricular fibrillation appeared, and after cardioversion, she was transferred to CCU. An ECG (Biocare ECG‐1230, Shenzhen Biocare Bio Medical Equipment, Shenzhen, China) after cardioversion revealed ST segment elevation in I, aVL, V2–V6 leads (0.1–0.7 mV) and premature ventricular beats (Fig. 1). The patient had no history of hypertension or diabetes. On physical examination, blood pressure was 158/76 mmHg, heart rate was 92 beats per minute and there were no abnormal signs on heart and lung examination. After 30 minutes, we did another ECG (Fig. 2) for this patient and it revealed ST segment elevated in I, aVL, V2–V6 leads have fallen slightly, even >50% in V4, V5 leads. Laboratory examination:troponin T :1.6 ng/ml. So she was diagnosed as acute anterior wall myocardial infarction. Owing to the improvement of chest pain, we considered that perhaps it was because of thrombus autolysis in related infarct artery. So we gave her conventional therapy as acute anterior wall myocardial infarction, and coronary angiography was not performed. On day 2, the syndrome of chest pain disappeared, and ECG (Fig. 3) revealed ST segment elevated fallen further and inverted T waves appeared. However, on day 4, the patient suddenly presented lasting chest pain again, because she was scared by another patient in the same ward who had a sudden death. On physical examination, blood pressure was 140/70 mmHg, heart rate was 87 beats per minute. And ECG (Fig. 4) revealed ST segment elevated in II, V2–V6 leads again (0.05–0.4 mV). Urgent coronary angiography (Siemens AXIOM Artis, Siemens, Erlangen, Germany) (Fig. 5) was performed and showed normal coronary arteries except some stenosis in LAD (about 30%). A few hours later, chest pain improved progressively. Laboratory examination: troponin T:0.84 ng/ml. On day 5, echocardiogram (Philips iE33, Philips Medical Systems, Andover, MA)
Figure 1.
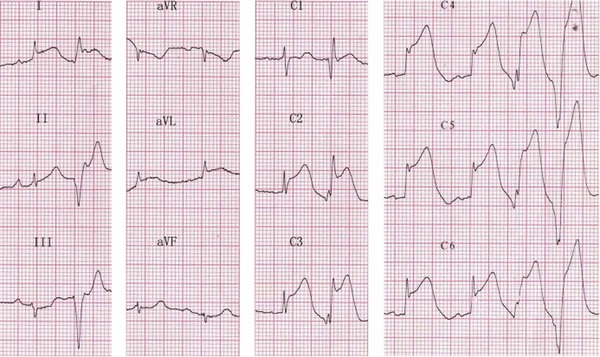
ECG recorded after cardioversion showing ST segment elevated in I, aVL, V2–V6 Leads and frequent premature ventricular arrhythmia.
Figure 2.
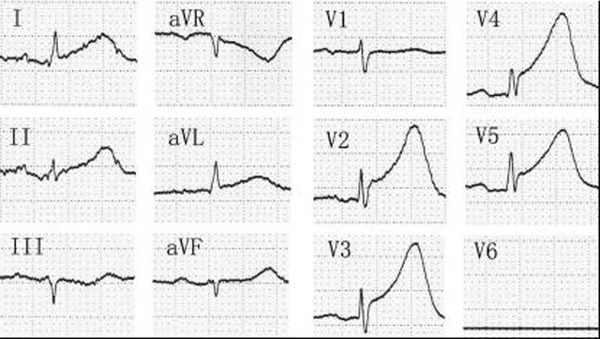
ECG recorded after 1st ECG about 30 min showing ST segment elevated in I, aVL, V2–V6 leads have fallen slightly, even >50% in V4–V5 leads.
Figure 3.
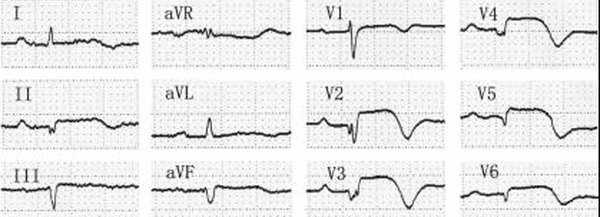
ECG recorded on day 2 showing ST segment elevated fallen ∼ and inverted T waves appeared.
Figure 4.
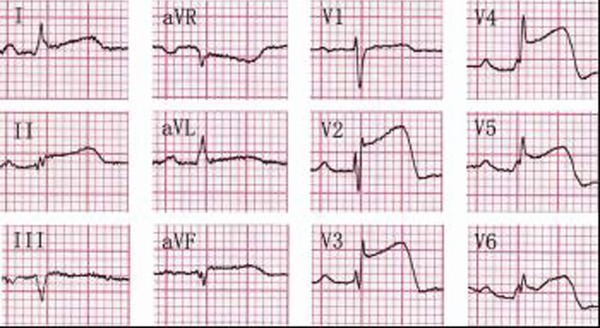
ECG recorded on day 4 when the patient suddenly presented lasting chest pain showing ST segment elevated in II, V2–V6 leads again.
Figure 5.
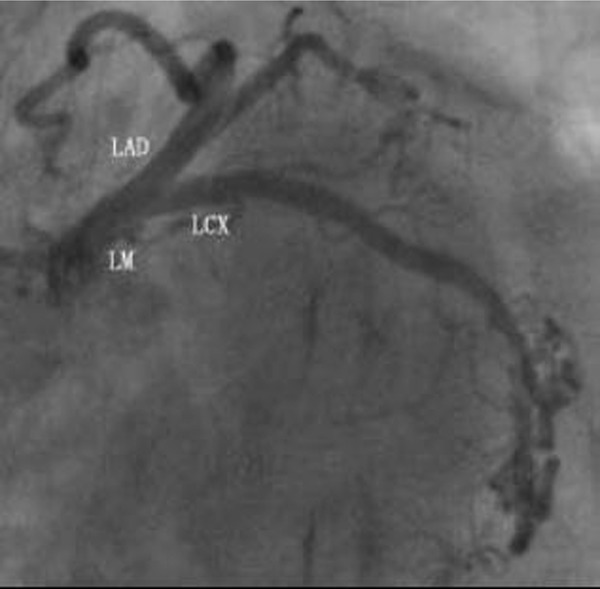
Urgent coronary angiography showed normal coronary arteries except some stenosis in LAD (about 30%).
(Fig. 6) showed left ventricular mid‐apical ballooning (3.2 × 3.1 cm), and the hypokinesia is marked at the middle part of the left ventricle and the apical region. On the contrary, hyper contractility is marked at the basal segment. It also demonstrated a left ventricular ejection fraction of 47%. The final diagnosis was Takotsubo syndrome. And 1 week later, the patient restored to health and was discharged. And 6 weeks later, she returned to hospital for reexamination and there were no abnormal indicators in myocardial injury marker. Additionally, another echocardiogram showed left ventricular mid‐apical ballooning (2.0 × 2.5 cm). And 2 years later, echocardiogram showed left ventricular function had restored basically (Fig. 7).
Figure 6.
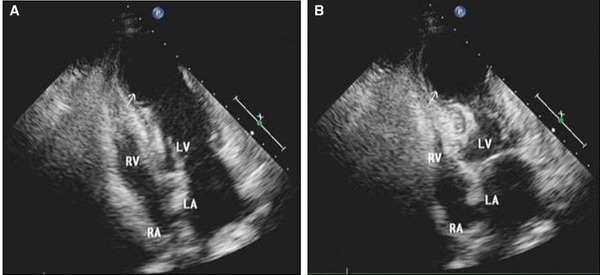
Echocardiogram showed characteristic apical dyskinesis and basal hyper contractility: (A) Diastole; (B) Systole.
Figure 7.
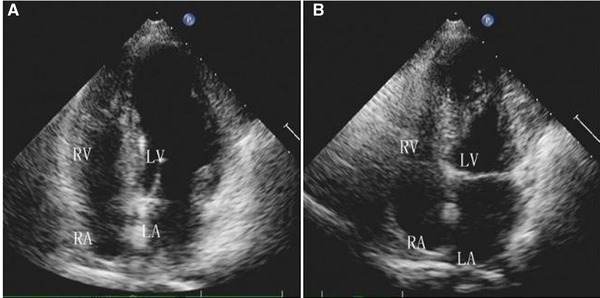
Figure showed left ventricular function had restored basically: (A) Diastole; (B) Systole.
DICUSSION
Since the first case of Takotsubo syndrome reported by Sato in Japan,1 many countries have reported this disease. The clinical presentation is similar to acute myocardial infarction including chest pain, ST‐T segment abnormalities, and slight troponine and CK‐MB increase, additionally, transient left ventricular apical ballooning alteration.2 However, no occlusion or stenosis in the coronary arteries revealed by coronary angiogram. The prognosis of Takotsubo syndrome is generally favorable, and in‐hospital mortality rate is from 1.1% to 1.7%,3 most patients can recover completely in few weeks.4 At present, the underlying mechanisms responsible for this syndrome have not yet been fully elucidated and several popular theories provided as follows: (1) Catecholamine excess. Takotsubo syndrome is frequently triggered by psychologically stressful events or severe physical disease.5, 6 Several studies 7, 8, 9 have indicated that in highly psychological stressing state, sympathetic activity is enhanced extraordinarily, and a large number catecholamine and neuropeptide are released in short time, finally, resulted in cardiomyopathy instant restrain. Meanwhile, the left ventricular apex is the most biggest part of surface/volume in heart, additionally, there are a great quantity of β‐receptors,10 so the apex could be affected easier. Therefore, people consider that there is a causal link between catecholamine excess and the development of Takotsubo syndrome. (2) Estrogen decrease. Most commonly, post‐menopausal woman are affected easier resulted from their estrogen level decreased and the ability of controlling both sympathetic and vessels weakened. And some studies11 provided that this process is associated with specific alteration of Ca2+ handling proteins which might be crucial for contractile dysfunction. On the contrary, a few literatures indicate that adding estrogen could reduce heart rate and constrain ventricle function.7 (3) Gene and heredity. Nef et al. consider that increased transcription of GPX1, CAT, RPS6, and eIF4E play a pivotal role in the recovery of Takotsubo syndrome, on the other hand, the defection of CD36 may be associated with the occurrence of this disease.12 Other theories include coronary artery spasm, microvascular spasm, coronary artery deformity, and virus infection; however, these are not approved extensively for less samples.
During the admission of the patient, we diagnosed acute myocardial infarction. However, coronary angiography showed no significant coronary artery disease, on the contrary, Echocardiogram showed left ventricular apical ballooning. According to the diagnose standards of Takotsubo syndrome suggested by Abe et al.,13 we diagnosed the patient as Takotsubo syndrome for the second paroxysm. Reviewing this case, there is explicit stressful stimulation before the first paroxysm, because this patient watched earthquake news on TV at home. Therefore, a retrospective diagnosis of the Takotsubo syndrome. Thus, can be applied for the first paroxysm, and the second paroxysm is the recurrence of this disease.
Recurrence of Takotsubo syndrome usually occurs in 4 years,14 on very rare occasions, recurrence has been observed after 10 years,15 and recurrence occurs in 1 year from the first presentation in 3% of patients. Nevertheless, this patient recurs in only 4 days, so, clinical doctors and families should pay close attention to the patients mood in long time, and avoid mind stimulation, thus, prevent the recurrence of Takotsubo syndrome.
REFERENCES
- 1. Dote K, Sato H, Tateishi H, et al. Myocardial stunning due to simultaneous multivessel coronary spasms: A review of 5 cases [J]. J Cardiol 1991;21(2):203–214. [PubMed] [Google Scholar]
- 2. Bielecka‐Dabrowa A, Mikhailidis DP, Hannam S, et al. Takotsubo cardiomyopathy the current state of knowledge [J]. Int J Cardiol 2010;142(2):20–125. [DOI] [PubMed] [Google Scholar]
- 3. Pilgrim TM,Wyss TR. Takotsubo cardiomyopathy or transient left ventricular Apical ballooning syndrome: A systematic review [J]. Int J Cardiol 2008;124(3):283–292. [DOI] [PubMed] [Google Scholar]
- 4. Wedekind H, Moller K, Scholz KH. Tako‐Tsubo cardiomyopathy: Incidence in Patients with acute coronary syndrome [J]. Herz 2006;31(4):339–346. [DOI] [PubMed] [Google Scholar]
- 5. Sharkey SW, Lesser JR, Andrey G, et al. Acute and reversible cardiomyopathy provoked by stress in women from the Unite States [J]. Circulation 2005;111(4):472–479. [DOI] [PubMed] [Google Scholar]
- 6. Wittstein IS, Thiemann DR, Lima JAC, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress [J]. N Engl J Med 2005;352(6):539–548. [DOI] [PubMed] [Google Scholar]
- 7. Ueyama T, Aki T, Senba E, et al. Emotional stress activates MAP kinase in the rat heart [J]. Life Sci 2001;69(16):1927–1934. [DOI] [PubMed] [Google Scholar]
- 8. Von‐Knobel, Abdel‐Aty H, Schulz‐Menger J. Takotsubo .cardiomyopathy after nasal application of epinephrine ‐amagnetic resonance study [J]. Int J Cardiol 2010;145(2):308–309. [DOI] [PubMed] [Google Scholar]
- 9. Pow‐Li Chia, David Foo. Tako‐tsubo cardiomyopathy precipitated by pheochromocytoma crisis [J]. Cardiol J 2011;5(18):564–567. [DOI] [PubMed] [Google Scholar]
- 10. Lyon AR, Rees PS, Prasad S, et al. Stress (Takotsubo) cardiomyopathy‐ a novel pathophysiological hypothesis to explain catecholamine‐induced acute myocardial stunnin [J]. Nat Clin Pract Cardiovasc Med 2008;5(1):22–29. [DOI] [PubMed] [Google Scholar]
- 11. Nef H, Mllman H, Troidl C, et al. Abnormalities in intracellular Ca2+ regulation contribute to the pathomechanism of Tako‐Tsubocardiomyopathy [J]. Eur Heart J 2009;30:2155–2164. [DOI] [PubMed] [Google Scholar]
- 12. Nef HM, Mllmann H, Troidl C, et al. Expression profiling of cardiac genes in Tako‐Tsubo cardiomyopathy: Insight into a new cardiac entity [J]. J Mol Cell Cardiol 2008;44(2):395–404. [DOI] [PubMed] [Google Scholar]
- 13. Abe Y, Kondo M, Matsuoka R, et al. Assessment of clinical features in transient left ventricular apical ballooning [J]. J Am Coll Cardiol 2003;41(5):737–742. [DOI] [PubMed] [Google Scholar]
- 14. Ahmad A, Elesber MD, Abhiram P, et al. Four‐year recurrence rate and prognosis of the apical Ballooning Syndrome [J]. J Am Coll Cardiol 2007;5(50):448–452. [DOI] [PubMed] [Google Scholar]
- 15. Marco Cerrito MD, Alberto Caragliano MD, Domenica Zema, MD , et al. Very late recurrence of Takotsubo Syndrome Universita Messina, 2012;1(17):58–60. [DOI] [PMC free article] [PubMed] [Google Scholar]