

Abstract
Objectives: To find the relationship between anabolic androgenic steroids (AAS) using and QT interval in athletes.
Methods: Between January 1, 2005 and May 31, 2007, we examined QTc interval duration in 165 consecutive male professional bodybuilders [age: 32.1 ± 4.6 years]. Of these, 79 were AAS users. The control group included 90 sedentary age and gender matched subjects [none of them were AAS users].
Results: The QTc interval of AAS abusing bodybuilders was significantly shorter compared with QTc interval in AAS‐free bodybuilders and control group. Short QTc interval (≤380 ms) was an independent predictor of AAS abusing in the multivariate analysis.
Conclusions: To the best of our knowledge, there is no published report regarding electrocardiographic diagnosis and screening of AAS abusing athletes. In the present study, we present an easy and applicable method to screen and diagnose AAS abusing among professional bodybuilders. In the presence of QTc interval ≤ 380 ms in a bodybuilder, one would predict AAS abusing with 83% sensitivity and 88% specificity.
Keywords: anabolic steroid, bodybuilding, QT interval
The self‐administration of anabolic androgenic steroids (AAS) is a widespread practice among athletes to increase lean body mass and muscular strength. The misuse of AASs for the purpose of enhancing performance continues to be a difficult problem for major sport organizations. In recent years, strong evidences have revealed the cardiovascular toxicity of AAS. 1 , 2 , 3 Previous studies suggest that athletes may have prolonged QT intervals due to enhanced vagal activity 4 but in our Institute of Sports Science, we frequently observed short QT intervals in AAS abusing athletes. We hypothesized that the repeated use of AAS would shorten QT interval in athletes with a long‐term history of strength training and QT interval may be a marker of AAS abusing in strength trained athletes.
METHODS
Study Population
Professional male bodybuilders, candidates for bodybuilding‐fitness competitions in the country in the period of January 1, 2005 to May 31, 2007 were enrolled. All bodybuilders had been training for 8 to 10 hours/week for ≥5 years. The control group included healthy sedentary age and gender matched subjects. During the day before competition, each of the bodybuilders had one visit during which a history was taken concerning health, regular medications and androgen drug use. Supine resting blood pressure was measured and a urine sample was taken for drug screening. Two‐dimensional and Doppler echocardiography was performed. A 12‐lead electrocardiogram at an article speed of 50 mm/s was taken after a 20‐minute rest period. In the non–bodybuilding controls a similar history was taken, two‐dimensional and Doppler echocardiography was performed and urine sample test was done for drug screening. Urine samples were screened for AAS as standardized by the International Olympic Committee. 5 This study received approval from the Institutional Review Board and written informed consent was obtained from subjects.
Echocardiographic Study
Cardiac echocardiography was performed in the bodybuilders and controls using a 3.5‐MHz phased array transducer. Measurements of LV dimensions were obtained from both M‐mode and two‐dimensional echocardiography. The LV measurements were performed at end‐diastole and end‐systole according to the recommendations of the American Society of Echocardiography and the Penn Convention. 6 , 7 Only frames with optimal visualization of interventricular septum, posterior wall, and LV internal diameter throughout the entire cardiac cycle were used for measurements. The mean values from ≥3 measurements for each parameter were computed. The LV mass was calculated using the Devereux formula. 8
QT Interval Measurement
During the day before the competition, measurements were obtained from a 12‐lead electrocardiogram at a article speed of 50 mm/s after a 20‐minute rest period. With calipers on printed ECGs, the QT interval of each lead was measured from the beginning of the QRS complex to the visual return of the T‐wave to the isoelectric line by the same investigator who remained blinded to the group and identity of the subjects. The end of the T wave was defined as its return to the T–P baseline. When the end of the T wave could not be identified, the lead was excluded. When the T wave was interrupted by the U‐wave, the end of the T wave was defined as the nadir between the T wave and the U wave. All subjects had at least 10 measurable leads. Heart rate correction was done with the Bazett's formula, and QTc interval duration was defined as the mean duration of all QTc intervals measured. The intra‐observer variability of the QT interval measurements was tested by repeated measurements of a random sample of 30 electrocardiograms. The correlation coefficient of the samples was 0.91. In 40 randomly selected athletes, measurements were repeated in a blinded manner by a second observer. Differences between the two sets of measurements were examined using the paired t‐test and were found not statistically significant [P = 0.78].
Exclusion Criteria
Subjects treated with type I or type III antiarrhythmic drugs, antidepressive drugs (n = 2), antihistamines (n = 1), macrolide antibiotics (n = 1), familial short QT syndrome [based on history and familial ECG; n = 1] and long QT syndrome [based on history and familial ECG; n = 1] were excluded from the study.
Statistical Analysis
Differences between the AAS abusers, non‐AAS athletes and control group were analyzed with pair‐wise comparisons. Comparisons of categorical variables were made with a chi‐square test. To determine cutoff values, analysis of receiver operating characteristic (ROC) curve was made. A P value < 0.05 was considered significant.
RESULTS
Baseline Characteristics
A total of 165 consecutive male professional bodybuilders met all study criteria [age: 32.1 ± 4.6 years]. Of these, 79 were AAS users. The control group included 90 sedentary age and gender matched subjects [none of them were AAS users]. Subject characteristics are presented in Table 1. No differences were observed in age, height, or blood pressure among sedentary men and drug free and drug using bodybuilders. Drug using bodybuilders had greater weight and body surface area than drug free bodybuilders and age matched sedentary men.
Table 1.
Body Size Variables, Blood Pressures, and Electrocardiographic Parameters of the Bodybuilders and Controls
| Group A (n = 90) | Group B (n = 86) | Group C (n = 79) | P value | |||
|---|---|---|---|---|---|---|
| A versus B | A versus C | B versus C | ||||
| Age (years) | 31.4 ± 5 | 32.1 ± 4.6 | 33 ± 6 | 0.71 | 0.83 | 0.64 |
| Height (cm) | 178 ± 5 | 175 ± 8 | 179 ± 6 | 0.41 | 0.96 | 0.57 |
| Weight (kg) | 76 ± 9 | 79 ± 8 | 96 ± 8 | 0.53 | 0.001 | 0.003 |
| Body surface area (m2) | 1.93 ± 0.11 | 1.98 ± 0.14 | 2.19 ± 0.16 | 0.69 | 0.021 | 0.035 |
| Heart rate (bpm) | 78 ± 10.3 | 69 ± 8.5 | 68 ± 8.9 | 0.07 | 0.073 | 0.59 |
| Systolic blood pressure (mmHg) | 130 ± 10 | 132 ± 11 | 135 ± 11 | 0.59 | 0.23 | 0.25 |
| Diastolic Blood pressure (mmHg) | 80 ± 8 | 78 ± 12 | 82 ± 10 | 0.35 | 0.27 | 0.39 |
| QTc interval (ms) | 418 ± 23.6 | 422 ± 24.5 | 367 ± 17.1 | 0.61 | 0.001 | 0.001 |
Group A = sedentary men; Group B = drug‐free bodybuilders; Group C = drug user bodybuilders.
Echocardiography Results
The standard echocardiographic data are listed in Table 2. No differences were found in LV morphologic parameters (i.e., LV internal diameter, LV wall thickness, and LV mass) between drug free bodybuilders and sedentary controls. In contrast, effect of AAS use was observed on LV morphology. AAS using bodybuilders exhibited greater LV mass compared with the two other groups (this finding is consistent with previous observations that found AAS users have greater LV mass 9 ). No significant differences were found in stroke volume, heart rate, cardiac output, and the ejection fraction among the three groups, indicating that strength training and AAS use had no effect on LV systolic function.
Table 2.
Echocardiographic Data of the Bodybuilders and Controls
| Group A (n = 90) | Group B (n = 86) | Group C (n = 79) | P value | |||
|---|---|---|---|---|---|---|
| A versus B | A versus C | B versus C | ||||
| Septal wall thickness (mm) | 9.4 ± 1.7 | 9.7 ± 1.2 | 10.3 ± 1.5 | 0.65 | 0.81 | 0.94 |
| Posterior wall thickness (mm) | 9.2 ± 0.11 | 10.4 ± 0.7 | 10.2 ± 1.5 | 0.35 | 0.25 | 0.53 |
| LV end‐diastolic diameter (mm) | 50 ± 4 | 53 ± 5 | 54 ± 4 | 0.11 | 0.09 | 0.36 |
| LV end‐systolic diameter (mm) | 33 ± 5 | 34 ± 6 | 35 ± 7 | 0.48 | 0.21 | 0.35 |
| LV mass (g) | 181 ± 48 | 204 ± 46 | 247 ± 37 | 0.071 | 0.011 | 0.028 |
Group A = sedentary men; Group B = drug‐free bodybuilders; Group C = drug user bodybuilders.
Results of QTc Interval Measurement
The QTc interval of AAS users was significantly shorter than QTc interval of drug free bodybuilders and sedentary men. Sedentary men had QTc interval of 418 ± 23.6 ms, drug free bodybuilders had QTc interval of 422 ± 24.5 ms and AAS user bodybuilders had QTc interval of 367 ± 17.1 ms which is significantly shorter from sedentary men and drug free bodybuilders [P < 0.01]. Figure 1 shows the distribution of QTc interval of the three groups. The area under the ROC curve [restricted to the two athlete groups] of QTc interval for prediction of AAS abusing was 0.88 [cut point ≤ 380 ms; sensitivity = 83%, specificity = 88%] (Fig. 2). As demonstrated in Table 3, QTc ≤ 380 ms was the strongest predictor of AAS using [P= 0.0002].
Figure 1.
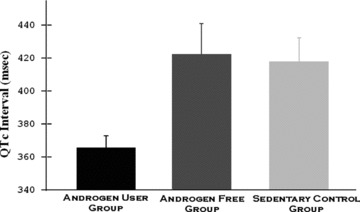
QTc interval duration in androgen abusing athletes, androgen free athletes and healthy age and gender matched subjects. Error bars represent the 95% confidence interval of a mean.
Figure 2.
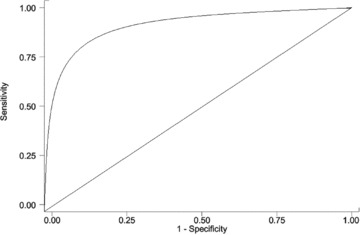
QTc interval ROC curve. The cut point that better optimizes the values of sensitivity and specificity are for values <380 ms.
Table 3.
Association between QTc ≤ 380 ms and Androgen using in Bodybuilders
| Drug‐Free Bodybuilders | Bodybuilders Drug Using | Total | |
|---|---|---|---|
| QTc ≤ 380 ms | |||
| Present | 10 | 66 | 76 |
| Absent | 76 | 13 | 89 |
| Total | 86 | 79 | 165 |
Statistics: Pearson chi‐square test [P = 0.0002]. Sensitivity = 83%. Specificity = 88%.
Dose–Response Relationship
When the AAS user athletes were divided into quartiles of duration of AAS using (first quartile: <2 years; second quartile: >2 and <5 years; third quartile: >5 and <8 years, and fourth quartile: >8 years), progressive decrease was found in QTc interval (Fig. 3).
Figure 3.
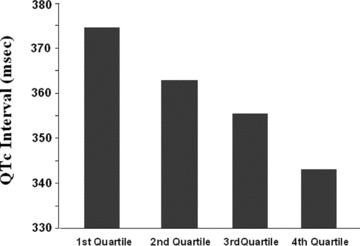
QTc interval (ms) in androgen using athletes compared by quartiles of duration of androgen use. When the athletes were divided into quartiles of duration of androgen use (first quartile: <2 years; second quartile: >2 and <5 years; third quartile: >5 and <8 years, and fourth quartile: >8 years), progressive decrease was found in QTc interval.
DISCUSSION
AAS enhances protein synthesis and increase muscle bulk. Consequently, AASs are widely used for performance enhancement and anabolic effects. Despite severe restrictions on the availability of AAS, their use is increasing 10 and has become more sophisticated with specific regimes devised for their administration to minimize unwanted side‐effects. Although the anthropometric benefits of AAS are well recognized, their cardiovascular consequences are less well appreciated. Anecdotally, reports of sudden death, thromboembolic disease and cerebro‐vascular events 2 , 11 , 12 implicate AAS. Over the last decade the number of laboratories accredited by the International Olympic Committee was increased to detect androgen abusing by athletes 13 but the cost of such laboratory drug testing makes it impractical to use routine testing to identify users of these agents.
In the present study we demonstrated a new and simple method to detect androgen abusing in professional strength trained athletes. Our findings demonstrate that among professional bodybuilders, those with AAS abusing have significantly shorter QT intervals than AAS‐free bodybuilders and their age and gender matched healthy counterparts. Our results are supported by previous experimental studies that showed androgens can shorten the QT interval. 14 , 15 Androgens facilitated the expression of two K+ channel proteins (Kir2.1 and Kv4.3) which are responsible for mediation of IK1 and Ito, respectively. IK1 is an important current involved in ventricular repolarization, thus its increase may account for the androgen induced shortening of QT and QTc intervals. 14 To the best of our knowledge, there is no published report regarding electrocardiographic screening of AAS abusing athletes. In the present study, we present an easy and applicable method to screen and diagnose AAS abusing among professional bodybuilders. In the presence of QTc interval ≤ 380 ms in a bodybuilder, one would predict AAS abusing with 83% sensitivity and 88% specificity.
Conflict of Interest: The authors have no conflict of interest.
REFERENCES
- 1. Hartgens F, Kuipers H. Effects of androgenic‐anabolic steroids in athletes. Sports Med 2004;34:513–554. [DOI] [PubMed] [Google Scholar]
- 2. Sullivan ML, Martinez CM, Gennis P, et al The cardiac toxicity of anabolic steroids. Prog Cardiovasc Dis 1998;41:1–15. [DOI] [PubMed] [Google Scholar]
- 3. Kutscher EC, Lund BC, Perry PJ. Anabolic steroids a review for the clinician. Sports Med 2002;32:285–296. [DOI] [PubMed] [Google Scholar]
- 4. Stolt A, Karila T, Viitasalo M, et al QT interval and QT dispersion in endurance athletes and in power athletes using large doses of anabolic steroids. Am J Cardiol 1999;84:364–366. [DOI] [PubMed] [Google Scholar]
- 5. Schanzer W. Abuse of androgens and detection of illegal use In: Nieschlag E, Behre HM. (eds.): Testosterone: Action, Deficiency, Substitution, Heidelberg , Springer, 1998, pp. 545–566. [Google Scholar]
- 6. Sahn DJ, DeMaria A, Kisslo J, et al Recommendations regarding quantitation in M‐mode echocardiography: Results of a survey of echocardiographic measurements. Circulation 1978;58:1072–1083. [DOI] [PubMed] [Google Scholar]
- 7. Devereux RB, Reichek N. Echocardiographic determination of left ventricular mass in man. Anatomic validation of the method. Circulation 1977;55:613–618. [DOI] [PubMed] [Google Scholar]
- 8. Devereux RB, Alonso DR, Lutas EM, et al Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am J Cardiol 1986;57:450–458. [DOI] [PubMed] [Google Scholar]
- 9. Nottin S, Nguyen LD, Terbah M, et al Cardiovascular effects of androgenic anabolic steroids in male bodybuilders determined by tissue Doppler imaging. Am J Cardiol 2006;97:912–915. [DOI] [PubMed] [Google Scholar]
- 10. Buckley W, Yesalis C, Friedl K, et al Estimated prevalence of anabolic steroid use among male high‐school seniors. JAMA 1988;260:3441–3445. [PubMed] [Google Scholar]
- 11. Melchert RB, Welder AA. Cardiovascular effects of androgenic anabolic steroids. Med Sci Sports Exerc 1995;27:1252–1262. [PubMed] [Google Scholar]
- 12. Ferenchick GS, Adelman S. Myocardial infarction associated with anabolic steroid use in a previously healthy 37‐year old weightlifter. Am Heart J 1992;124:507–508. [DOI] [PubMed] [Google Scholar]
- 13. IOC . Medical Code. Lausanne , Switzerland , International Olympic Committee, 1995, ISBN 92‐9149‐003‐2. [Google Scholar]
- 14. Fülöp L, Bányász T, Szabó G, et al Effects of sex hormones on ECG parameters and expression of cardiac ion channels in dogs. Acta Physiol (Oxf) 2006;188:163–171. [DOI] [PubMed] [Google Scholar]
- 15. Liu XK, Katchman A, Whitfield BH, et al In vivo androgen treatment shortens the QT interval and increases the densities of inward and delayed rectifier potassium currents in orchiectomized male rabbits. Cardiovasc Res 2003;57:28–36. [DOI] [PubMed] [Google Scholar]