

Abstract
Background: Exercise‐induced ventricular arrhythmias (EIVA) are frequently observed during exercise testing. However, the clinical guidelines do not specify their significance and so we examined this issue in our population.
Methods: A retrospective analysis of prospectively collected data was performed on 5754 consecutive male veterans referred for exercise testing at two university‐affiliated Veterans Affairs Medical Centers. Exercise test responses were recorded and cardiovascular mortality was assessed after a mean follow‐up of 6 ± 4 years. EIVA were defined as frequent premature ventricular complexes (PVCs) constituting more than 10% of all ventricular depolarizations during any 30‐second ECG recording, or a run of three or more consecutive PVCs during the exercise test or recovery.
Results: EIVA occurred in 426 patients (7.4%). There were 550 (10.6%) cardiovascular deaths during follow‐up. Seventy two (17%) patients with EIVA died of cardiovascular causes, whereas 478 (9.0%) of patients without EIVA died of cardiovascular causes (P < 0.001). Patients with EIVA had a higher prevalence of cardiovascular disease, resting PVCs, resting ST depression, and ischemia during exercise than patients without EIVA. In a Cox hazards model adjusted for age, cardiovascular disease, exercise‐induced ischemia, ECG abnormalities, exercise capacity and risk factors, EIVA was significantly associated with time to cardiovascular death. The combination of both resting PVCs and EIVA was associated with the highest hazard ratio.
Conclusions: EIVA are independent predictors of cardiovascular mortality after adjusting for other clinical and exercise test variables; combination with resting PVCs carries the highest risk.
Keywords: premature ventricular contractions, mortality, exercise testing, prediction, risk
Exercise testing is an important prognostic tool, but the significance of exercise‐induced ventricular arrhythmias (EIVA) remains uncertain. 1 Ventricular arrhythmias can be induced by exercise testing in healthy individuals, 2 but some studies suggest that EIVA confer a poor prognosis 3 , 4 , 5 while others suggest that EIVA are benign. 6 , 7 , 8 Although a recent study found that healthy volunteers with EIVA had increased mortality, 9 earlier studies did not produce similar results. 10 , 11 The purpose of this study was to determine the relationship between EIVA and cardiovascular (CV) death in a population of 5754 male veterans referred for exercise testing. We previously found an association between EIVA and all‐cause mortality in a similar population. 12
METHODS
Population
The study population consisted of 5754 consecutive male patients without atrial fibrillation or taking digoxin referred to two clinical exercise laboratories (Long Beach VA, 1987–1991, Palo Alto VA, 1992–2000). Forty‐two percent were referred for testing because of angina pectoris, 35% for nonischemic chest pain, resting ECG abnormalities or elevated risk factors, 5% for exercise capacity assessment, 2% for dyspnea on exertion and the rest for miscellaneous reasons. Less than 2% were tested to evaluate arrhythmias.
Data Collection
All exercise tests were supervised and all tests were read by two of the investigators (VF and JM). A thorough clinical history including medications and risk factors were recorded prospectively at the time of the exercise tests using computerized forms. 13
Exercise Testing
Patients underwent symptom‐limited treadmill testing using progressive protocols with small but frequent incremental steps 14 , 15 followed by being placed supine immediately. 16 The recorders that were utilized (Mortara X‐scribe, Milwaukee, WI and Burdick Quest, Madison, WI) had arrhythmia sensing that provided tracings automatically and manually as well as freeze/playback capabilities. EIVA was considered to be present if frequent premature ventricular complexes (PVCs) (constituting more than 10% of all ventricular depolarizations during any 30‐second ECG recording) or ventricular tachycardia (three or more consecutive PVCs) were visually detected during the exercise test or recovery. Resting PVCs were considered to be present if a PVC was detected in the 10‐second ECG prior to exercise.
Cardiovascular disease was defined as a history of documented coronary artery disease, myocardial infarction, coronary bypass surgery, coronary angioplasty, congestive heart failure, or peripheral vascular disease.
Follow‐Up
The California Death registry was used to match all of the patients using name and social security number. Data on subsequent interventions or nonfatal CV events were not available. Death status was determined as of July 2000.
Statistical Methods
Demographics, medical history, clinical and exercise test findings were compared between individuals with and without EIVA. t‐Test, chi‐square, and ANOVA were used to compare variables. CV mortality was used as the endpoint for survival analysis.
A Cox proportional hazards model was used to determine which variables were independently and significantly associated with time to CV death. Factors that were entered into the Cox model to predict CV mortality included age, presence of CV and pulmonary disease, history of hypertension, diabetes, current tobacco use, resting PVCs, resting ST segment depression, other ECG abnormalities, METs achieved, maximum exercise heart rate, exercise‐induced ST depression, angina, and EIVA.
RESULTS
Prevalence
Patient demographics and exercise test findings are described in Table 1 (by the presence or absence of EIVA). EIVA were present in 426 patients (7.4%). Patients with EIVA were older and were more likely to have CV disease, abnormal ECGs, resting PVCs, and exercise‐induced ischemia compared to those without EIVA. Of the 211 patients with resting PVCs, 85 (41%) developed EIVA.
Table 1.
Population Demographics with Statistical Comparison between Those with and without Exercise‐Induced Arrhythmias
| Variable | Total | Without EIVA | With EIVA | P Value |
|---|---|---|---|---|
| Number | 5754 | 5328 | 426 (7.4%) | |
| Age | 63.6 ± 10.2 | 58.3 ± 11.2 | 63.6 ± 10.2 | 0.01 |
| Race caucasian | 4164 (72%) | 3845 (72%) | 319 (75%) | NS |
| African American | 717 (12%) | 671 (12.6%) | 46 (11%) | NS |
| BMI | 28 ± 5 | 28 ± 5 | 28 ± 5 | NS |
| Cardiovascular deaths | 550 (9.6%) | 478 (9.0%) | 72 (17%) | <0.001 |
| Clinical findings | ||||
| Q wave | 1006 (17%) | 920 (17%) | 86 (20%) | NS |
| Resting ST‐depression | 477 (8.3%) | 414 (7.8%) | 63 (15%) | <0.001 |
| ECG LVH with ST depression | 271 (4.7%) | 240 (4.5%) | 31 (7.3%) | 0.01 |
| Right BBB | 247 (4.3%) | 222 (4.2%) | 25 (5.9%) | NS |
| Resting PVCs | 211 (3.7%) | 126 (2.4%) | 85 (20%) | <0.001 |
| Abnormal ECG | 1825 (32%) | 1614 (31%) | 211 (50%) | <0.001 |
| Resting heart rate | 77 ± 15 | 77 ± 15 | 77 ± 15 | NS |
| Resting SBP | 134 ± 21 | 133 ± 21 | 138 ± 21 | 0.005 |
| Resting DBP | 82 ± 12 | 82 ± 12 | 82 ± 12 | NS |
| Medical history | ||||
| Cardiovascular disease | 1918 (33%) | 1741 (32.7%) | 177 (42%) | <0.001 |
| CHF | 154 (2.7%) | 127 (2.4%) | 27 (6.3%) | <0.001 |
| MI | 1219 (21.2%) | 1114 (20.9%) | 105 (25%) | NS |
| Pulmonary disease | 385 (6.7%) | 357 (6.7%) | 28 (6.6%) | NS |
| Hypertension | 2750 (48%) | 2534 (47%) | 216 (51%) | NS |
| Current smoking | 1797 (31%) | 1694 (32%) | 103 (24%) | 0.001 |
| Diabetes | 596 (10.4%) | 560 (10.5%) | 36 (8.5%) | NS |
| Percutaneous coronary Intervention | 354 (6.2%) | 325 (6.1%) | 29 (6.8%) | NS |
| Bypass surgery | 495 (8.6%) | 439 (8.2%) | 56 (13%) | <0.001 |
| Medications | ||||
| Calcium channel blocker | 1551 (27%) | 1416 (26.6%) | 135 (32%) | 0.02 |
| Beta‐blocker | 1100 (19%) | 1016 (19%) | 84 (20%) | NS |
| Nitrates | 1313 (23%) | 1210 (23%) | 103 (24%) | NS |
| Antihypertensive | 1321 (23%) | 1203 (23%) | 118 (28%) | 0.02 |
| Anti‐arrhythmic | 75 (1.3%) | 61 (1.1%) | 14 (3.3%) | <0.001 |
| Exercise test findings | ||||
| Angina occurred | 974 (17%) | 883 (17%) | 91 (21%) | 0.01 |
| Angina reason for stopping | 346 (6.0%) | 308 (5.8%) | 38 (8.9%) | 0.01 |
| Exercise‐induced ST depression | 1339 (23%) | 1203 (22.6%) | 136 (32%) | <0.001 |
| Exercise‐induced ischemia (angina and/or ST depression) | 1836 (32%) | 1660 (31%) | 176 (41%) | <0.001 |
| METs | 8.3 ± 3.7 | 8.3 ± 3.7 | 7.6 ± 3.3 | NS |
| Borg perceived exertion scale (6–20) | 17 ± 3 | 17 ± 2 | 17 ± 2 | NS |
| Max heart rate | 137 ± 25 | 137 ± 25 | 136 ± 23 | NS |
| Max SBP | 179 ± 29 | 179 ± 29 | 180 ± 27 | NS |
| Annual CV mortality | 1.1% | 1.0% | 2.0% | <0.001 |
Survival
There were 550 (10.6%) CV deaths during follow‐up, as well as 566 deaths from other causes (Table 2). Seventy‐two patients with EIVA (17%) died of CV causes, whereas 478 of patients without EIVA (9.0%) died of CV causes (P < 0.001). Of the patients who died of CV causes, 36 (6.5%) had resting PVCs, nearly twice the frequency in survivors (P < 0.0001). The total average annual CV mortality was 1.1% with a mean follow‐up 6 ± 4 years. The average annual mortality in those with EIVA was 1.8% whereas it was only 1% in patients without EIVA (P < 0.001).
Table 2.
Demographics of Study Population According to Outcomes
| Variable | Survivors | CV Death | P | All Other Deaths | P |
|---|---|---|---|---|---|
| Total | 4638 | 550 | 566 | ||
| Age | 58 ± 11 | 64 ± 9 | <0.001 | 63 ± 10 | <0.001 |
| Race caucasian | 3298 (71%) | 423 (77%) | 0.003 | 443 (78%) | <0.001 |
| African American | 604 (13%) | 54 (9.8%) | 0.035 | 59 (10%) | NSD |
| BMI | 28 ± 5 | 27 ± 5 | <0.001 | 27 ± 5 | <0.001 |
| In patients | 1039 (22%) | 195 (35%) | <0.001 | 194 (34%) | <0.001 |
| Clinical findings | |||||
| Q wave | 711 (15%) | 173 (31%) | <0.001 | 122 (22%) | <0.001 |
| Resting ST‐depression | 305 (6.5%) | 112 (20%) | <0.001 | 60 (11%) | <0.001 |
| ECG LVH with ST depression | 189 (4.1%) | 56 (10%) | <0.001 | 26 (4.6%) | NS |
| Right BBB | 171 (3.7%) | 33 (6%) | 0.011 | 43 (7.6%) | <0.001 |
| Resting PVCs | 153 (3.3%) | 36 (6.5%) | <0.001 | 22 (3.9%) | NS |
| Abnormal ECG | 1292 (28%) | 301 (55%) | <0.001 | 232 (41%) | <0.001 |
| Resting heart rate | 76.9 ± 14.8 | 76.7 ± 15.0 | NSD | 80.7 ± 16.6 | <0.001 |
| Resting SBP | 133.7 ± 22.8 | 134.6 ± 22.6 | NSD | 132.4 ± 22.9 | NS |
| Medical history | |||||
| Cardiovascular disease | 1369 (30%) | 330 (60%) | <0.001 | 219 (39%) | <0.001 |
| CHF | 95 (2.0%) | 39 (7.1%) | <0.001 | 20 (3.5%) | 0.03 |
| MI | 883 (19%) | 236 (43%) | <0.001 | 150 (27%) | <0.001 |
| Pulmonary Disease | 270 (5.9%) | 50 (9.1%) | 0.003 | 65 (11%) | <0.001 |
| Hypertension | 2176 (47%) | 324 (59%) | <0.001 | 250 (44%) | NSD |
| Current smoking | 1435 (30.9%) | 164 (29.8%) | NSD | 198 (35%) | 0.05 |
| Diabetes | 466 (10%) | 73 (13%) | 0.022 | 57 (10%) | NSD |
| Percutaneous coronary intervention | 286 (6.2%) | 38 (6.9%) | NSD | 30 (5.3%) | NSD |
| Bypass surgery | 339 (7.3%) | 118 (21%) | <0.001 | 38 (6.7%) | NSD |
| Medications | |||||
| Calcium channel blocker | 1146 (25%) | 242 (44%) | <0.001 | 163 (29%) | 0.04 |
| Beta‐blocker | 857 (18%) | 135 (25%) | <0.001 | 108 (19%) | NSD |
| Nitrates | 896 (19%) | 238 (43%) | <0.001 | 179 (32%) | <0.001 |
| Antihypertensive | 965 (21%) | 207 (38%) | <0.001 | 149 (26%) | 0.002 |
| Anti‐arrhythmic | 50 (1.1%) | 14 (2.5%) | 0.006 | 11 (1.9%) | NSD |
| Exercise test findings | |||||
| Angina occurred | 749 (16%) | 132 (24%) | <0.001 | 93 (16%) | NSD |
| Angina reason for stopping | 263 (5.7%) | 51 (9.3%) | 0.001 | 32 (5.7%) | NSD |
| Exercise induced ST depression | 761 (16%) | 73 (13%) | <0.001 | 73 (13%) | 0.02 |
| Exercise‐induced ischemia | 1394 (30%) | 262 (46%) | <0.001 | 180 (32%) | NSD |
| Maximal heart rate | 139.3 ± 24.3 | 124.1 ± 23.6 | <0.001 | 130.6 ± 13.2 | <0.001 |
| Borg score | 17.2 ± 2.5 | 17.0 ± 2.4 | NSD | 17.3 ± 2.6 | NSD |
| METs | 8.6 ± 3.5 | 6.4 ± 3.4 | <0.001 | 6.9 ± 3.7 | <0.001 |
| Max SBP | 180.3 ± 28.6 | 171.0 ± 31.5 | <0.001 | 174.0 ± 30.2 | <0.001 |
| EIVA only | 255 (5.5%) | 54 (10%) | <0.001 | 32 (5.7%) | NSD |
| EIVA and rest PVCs | 57 (1.2%) | 18 (3%) | <0.001 | 10 (1.8%) | NSD |
Statistical comparisons between survivors and those with CV death and then between survivors and all other deaths; Exercise‐induced ischemia = angina and/or ST depression.
In the Cox Hazard multivariate analysis shown in Table 3, both EIVA and the combination of resting PVCs with EIVA were independent predictors of mortality after considering age, clinical, resting, and exercise test variables. PVCs occurring only at rest were significantly associated with CV death when considered univariately with age but were not when the other arrhythmia groups were considered. Whereas the hazard ratio was 1.6 for patients with EIVA (P < 0.003), the hazard ratio for both EIVA and resting PVCs was 2.7 (P < 0.0001). Because of this result, the patients were classified as without PVCs, with PVCs only at rest, with EIVA only, and with both EIVA and rest PVCs (Table 4).
Table 3.
Multivariate Analysis of Predictors of Cardiovascular Death
| Variable | Hazard Ratio | P Value |
|---|---|---|
| Age (years) | 1.03 (1.02–1.04) | <0.001 |
| Exercise capacity (Mets) | 0.90 (0.87–0.93) | <0.001 |
| Cardiovascular disease | 1.9 (1.6–2.3) | <0.001 |
| Maximum heart rate | 0.99 (0.98–1.0) | 0.002 |
| Resting ST‐segment depression | 1.4 (1.2–1.7) | <0.001 |
| ECG LVH with ST depression | 2.0 (1.5–2.7) | <0.001 |
| Diabetes | 1.3 (1.03–1.7) | 0.03 |
| History of hypertension | 1.4 (1.2–1.7) | <0.001 |
| EIVA only (n = 341) | 1.6 (1.1–2.1) | 0.002 |
| EIVA w/ rest (n = 85) | 2.7 (1.7–4.3) | <0.001 |
Pulmonary disease, resting heart rate, currently smoking, and exercise‐induced ischemia were entered into the model but not chosen.
Table 4.
Demographics of Patients According to Arrhythmia Classification
| Variable | EIVA Only | Rest Only | EIVA w/rest PVCs | P Value |
|---|---|---|---|---|
| Total | 341 | 126 | 85 | |
| Age | 63 ± 10 | 63 ± 10 | 64 ± 10 | NSD |
| BMI | 28 ± 4 | 29 ± 5 | 27 ± 6 | 0.04 |
| Medical history | ||||
| Cardiovascular disease | 147 (43%) | 53 (42%) | 30 (35%) | <0.001 |
| CHF | 21 (6.2%) | 5 (3.9%) | 6 (7.1%) | <0.005 |
| MI | 84 (24.3%) | 33 (26%) | 21 (25%) | NSD |
| HBP | 174 (51%) | 69 (55%) | 42 (49%) | NSD |
| Smoking | 75 (22%) | 37 (29%) | 28 (33%) | <0.001 |
| Diabetes | 29 (8.5%) | 14 (11%) | 7 (8.2%) | <0.001 |
| Medications | ||||
| Calcium channel blocker | 107 (31%) | 42 (33%) | 28 (33%) | NSD |
| Beta‐blocker | 66 (19%) | 19 (15%) | 18 (1.2%) | <0.001 |
| Nitrates | 84 (25%) | 32 (25%) | 19 (22%) | NSD |
| Antihypertensives | 94 (28%) | 29 (23%) | 24 (28%) | NSD |
| Anti‐arrhythmic | 9 (2.6%) | 4 (3.2%) | 5 (5.9%) | NSD |
| Clinical Findings | ||||
| Q wave | 75 (22%) | 30 (24%) | 11 (13%) | <0.001 |
| Resting ST‐segment | 49 (14%) | 19 (15%) | 14 (16%) | NSD |
| ST‐inclusive LVH | 23 (6.7%) | 6 (4.8%) | 8 (9.4%) | <0.001 |
| Resting HR | 75 ± 15 | 81 ± 14 | 84 ± 15 | <0.001 |
| Resting SBP | 138 ± 21 | 134 ± 20 | 137 ± 21 | NSD |
| Resting DBP | 82 ± 13 | 81 ± 12 | 82 ± 11 | NSD |
| Exercise Test Findings | ||||
| Angina occurred | 77 (23%) | 19 (15%) | 14 (16.5%) | <0.001 |
| Abnormal ST depression | 113 (33%) | 31 (25%) | 23 (27%) | <0.001 |
| Exercise‐induced ischemia | 146 (43%) | 40 (32%) | 30 (35%) | <0.001 |
| METs | 7.7 ± 3.3 | 7.5 ± 3.0 | 7.0 ± 3.3 | NSD |
| Maximum heart rate | 136 ± 23 | 138 ± 20 | 136 ± 22 | NSD |
| Maximum SBP | 181 ± 27 | 178 ± 27 | 176 ± 27 | NSD |
| Maximum DBP | 86 ± 16 | 86 ± 16 | 89 ± 13 | NSD |
| Annual CV mortality | 1.8% | 2.3% | 3.2% | ‐ |
Statistical comparisons among all three groups; exercise‐induced ischemia = angina and/or ST depression.
Patients with both EIVA and rest PVCs had an increased CV mortality of 3.2%, which was significantly higher than in patients with EIVA only (P < 0.001). Of the 126 patients with rest PVCs only, there were 18 CV deaths during the follow‐up period, which represented an annualized mortality of 2.3% (Fig. 1).
Figure 1.
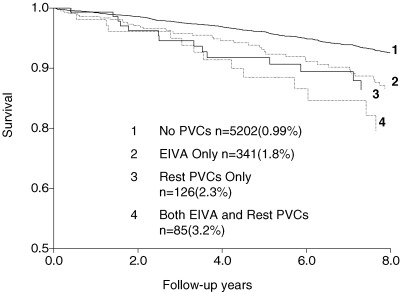
Kaplan–Meier survival curves for the patient groups: 1—no PVCs, 2—rest PVCs only, 3—exercise PVCs only, and 4—both rest and exercise PVCs. The numbers in the parentheses are the annual mortalities.
DISCUSSION
Previous studies suggest that the prevalence of EIVA increases in older populations 2 , 5 , 6 and in those with CV disease, 2 , 4 , 17 and our findings are consistent with these. Some studies suggest that EIVA may result from exercise‐induced ischemia since the prevalence of EIVA increases in those with ischemia; 5 , 18 however, other studies refute these results. 6 , 8 , 10 , 19 , 20 In our population, ischemia was more prevalent in patients with EIVA.
The significance of resting PVCs in apparently healthy patients is somewhat controversial; while many studies have found a favorable prognosis, 21 , 22 , 23 others have found increased risk of CV events. 24 , 25 Resting PVCs only in our population have been associated with CV death even when age adjusted and we assume that PVCs at any time are associated with increased risk whether during rest or exercise.
Some studies have shown that EIVA are not strong predictors of mortality following recovery from myocardial infarction 8 , 20 and in patients with coronary artery disease. 6 , 7 , 18 , 26 However, other studies of patients with known or suspected heart disease demonstrate that PVCs during exercise are associated with increased mortality. 3 , 4 , 5 In a very large sample of CAD patients, EIVA during recovery were the strongest predictor of death. 27
Inconsistency in study design is largely responsible for the discrepancies in these previous studies and perhaps gender differences. 28 Our data were coded in terms of whether EIVA were occasional or frequent in nature, but we did not precisely quantify the PVC rate at rest or during exercise or recovery and therefore we could not determine the rate of increase with exercise. Future investigators should examine how the morphology and exact quantification of EIVA affects prognosis.
CONCLUSION
Exercise‐induced ventricular arrhythmias are associated with an increased risk of cardiovascular death. While other patterns could not be evaluated, patients with both rest PVCs and EIVA are at highest risk. These findings support the need for additional research to direct the clinician by further stratifying the risk.
For the clinician, our study demonstrates that EIVA carry an increased risk independent of disease and other test responses. Until future studies help in stratification and treatment, all the physician can do is tell patients the truth. EIVA are not to be ignored and should lead to additional testing, risk factor modification, and/or closer follow‐up. Our study has resolved any controversy of the risk of EIVA in patients seen in a typical medical center exercise lab.
REFERENCES
- 1. Gibbons RJ, Balady GJ, Beasley JW, et al ACC/AHA guidelines for exercise testing: A report of the American College of Cardiology/American Heart Association Task force on Practice Guidelines. J Am Coll Cardiol 1997;30: 260–311 (updated Circulation. 2002 Oct 1;106(14):1883–1892).DOI: 10.1016/S0735-1097(97)00150-2 [DOI] [PubMed] [Google Scholar]
- 2. McHenry PL, Fisch C, Jordan JW, et al Cardiac arrhythmias observed during maximal treadmill exercise testing in clinically normal men. Am J Cardiol 1972;29: 331–336.DOI: 10.1016/0002-9149(72)90527-9 [DOI] [PubMed] [Google Scholar]
- 3. Udall JA, Ellestad MH. Predictive implications of ventricular premature contractions associated with treadmill stress testing. Circulation 1977;56: 985–989. [DOI] [PubMed] [Google Scholar]
- 4. Califf RM, McKinnes RA, McNeer R, et al Prognostic value of ventricular arrhythmias associated with treadmill testing in patients studied with cardiac catheterization for suspected ischemic heart disease. J Am Coll Cardiol 1983;2: 1060–1067. [DOI] [PubMed] [Google Scholar]
- 5. Marieb MA, Beller GA, Gibson RS, et al Clinical relevance of exercise‐induced ventricular arrhythmias in suspected coronary artery disease. Am J Cardiol 1990;66: 172–178.DOI: 10.1016/0002-9149(90)90583-M [DOI] [PubMed] [Google Scholar]
- 6. Schweikert RA, Pashkow FJ, Snader CE, et al Association of exercise‐induced ventricular ectopic activity with thallium myocardial perfusion and angiographic coronary artery disease in stable, low‐risk populations. Am J Cardiol 1999;83: 530–534.DOI: 10.1016/S0002-9149(98)00908-4 [DOI] [PubMed] [Google Scholar]
- 7. Sami M, Chaitman B, Fisher L, et al Significance of exercise‐induced ventricular arrhythmia in stable coronary artery disease: A coronary artery surgery study project. Am J Cardiol 1984;54: 1182–1188. [DOI] [PubMed] [Google Scholar]
- 8. Casella G, Pavesi PC, Sangiorgio P, et al Exercise‐induced ventricular arrhythmias in patients with healed myocardial infarction. Int J Cardiol 1993;40: 229–235. [DOI] [PubMed] [Google Scholar]
- 9. Jouven X, Zureik M, Desnos M, et al Long‐term outcome in asymptomatic men with exercise‐induced premature ventricular depolarizations. N Engl J Med 2000;343: 826–833.DOI: 10.1056/NEJM200009213431201 [DOI] [PubMed] [Google Scholar]
- 10. Busby MJ, Shefrin EA, Fleg JL. Prevalence and long‐term significance of exercise‐induced frequent or repetitive ventricular ectopic beats in apparently healthy volunteers. J Am Coll Cardiol 1989;14: 1659–1659. [DOI] [PubMed] [Google Scholar]
- 11. Froelicher VF, Thomas MM, Pillow C, et al Epidemiologic study of asymptomatic men screened by maximal treadmill testing for latent coronary artery disease. Am J Cardiol 1974;34: 770–776.DOI: 10.1016/0002-9149(74)90694-8 [DOI] [PubMed] [Google Scholar]
- 12. Partington S, Myers J, Cho S, et al Prevalence and prognostic value of exercise‐induced ventricular arrhythmias. Am Heart J 2003;145(1):139–146.DOI: 10.1067/mhj.2003.60 [DOI] [PubMed] [Google Scholar]
- 13. Froelicher VF, Shiu P. Exercise test interpretation system. Physicians and Computers 1996;14: 40–44. [Google Scholar]
- 14. Myers J, Buchanan N, Walsh D, et al A comparison of the ramp versus standard exercise protocols. J Am Coll Cardiol 1991;17: 1334–1342. [DOI] [PubMed] [Google Scholar]
- 15. Myers J, Do D, Herbert W, et al A nomogram to predict exercise capacity from a specific activity questionnaire and clinical data. Am J Cardiol 1994;73: 591–596.DOI: 10.1016/0002-9149(94)90340-9 [DOI] [PubMed] [Google Scholar]
- 16. Lachterman B, Lehmann KG, Abrahamson D, et al Recovery only ST‐segment depression and the predictive accuracy of the exercise test. Ann Intern Med 1990;112(1):11–16. [DOI] [PubMed] [Google Scholar]
- 17. Faris JV, McHenry PL, Jordan JW, et al Prevalence and reproducibility of exercise‐induced ventricular arrhythmias during maximal exercise testing in normal men. Am J Cardiol 1976;37: 617–622.DOI: 10.1016/0002-9149(76)90404-5 [DOI] [PubMed] [Google Scholar]
- 18. Weiner DA, Levine SR, Klein MD, et al Ventricular arrhythmias during exercise testing: Mechanism, response to coronary bypass surgery, and prognostic significance. Am J Cardiol 1984;53: 1553–1557.DOI: 10.1016/0002-9149(84)90578-2 [DOI] [PubMed] [Google Scholar]
- 19. McHenry PL, Morris SN, Kavalier M, et al Comparative study of exercise‐induced ventricular arrhythmias in normal subjects and patients with documented coronary artery disease. Am J Cardiol 1976;37: 609–616.DOI: 10.1016/0002-9149(76)90403-3 [DOI] [PubMed] [Google Scholar]
- 20. DeBusk RF, Davidson DM, Houston N, et al Serial ambulatory electrocardiography and treadmill exercise testing after uncomplicated myocardial infarction. Am J Cardiol 1980;45: 547–554. [DOI] [PubMed] [Google Scholar]
- 21. Kennedy HL, Whitlock JA, Sprague MK, et al Long‐term follow‐up of asymptomatic healthy subjects with frequent and complex ventricular ectopy. N Engl J Med 1985;312: 193. [DOI] [PubMed] [Google Scholar]
- 22. Elkon KB, Swerdlow TA, Myburgh DP. Persistent ventricular ectopic beats. A long‐term study. S Afr Med J 1977;52: 564. [PubMed] [Google Scholar]
- 23. Rodstein M, Wolloch L, Gubner RS. Mortality study of the significance of extrasystoles in an insured population. Circulation 1971;44: 617. [DOI] [PubMed] [Google Scholar]
- 24. Moss AJ. Clinical significance of ventricular arrhythmias in patients with and without coronary artery disease. Prog Cardiovasc Dis 1980;23: 33DOI: 10.1016/0033-0620(80)90004-3 [DOI] [PubMed] [Google Scholar]
- 25. Bikkina M, Larson MG, Levy D. Prognostic implications of asymptomatic ventricular arrhythmias: The Framingham heart study. Ann Intern Med 1992;117: 990. [DOI] [PubMed] [Google Scholar]
- 26. Nair CK, Thomson W, Aronow WS, et al Prognostic significance of exercise‐induced complex ventricular arrhythmias in coronary artery disease with normal and abnormal left ventricular ejection fraction. Am J Cardiol 1984;54: 1136–1138. [DOI] [PubMed] [Google Scholar]
- 27. Frolkis JP, Pothier CE, Blackstone EH, et al Frequent ventricular ectopy after exercise as a predictor of death. N Engl J Med 2003;348(9):781–790.DOI: 10.1056/NEJMoa022353 [DOI] [PubMed] [Google Scholar]
- 28. Bikkina M, Larson M, Levy D. Prognostic implications of asymptomatic ventricular arrhythmias: The Framingham heart study. Ann Intern Med 1992;117: 990–996. [DOI] [PubMed] [Google Scholar]