

Abstract
Holter electrocardiogram recording revealed symptomatic prolonged ventricular standstill lasting for about two minutes which terminated without any external cardiopulmonary resuscitation.
Ann Noninvasive Electrocardiol 2012;17(1):61–62
Keywords: first degree AV block, left bundle branch block, ventricular arrest, CPR, pacemaker
CASE REPORT
Atrioventricular (AV) block of high degree is well described in literature 1 and is considered class 1 indication for permanent pacemaker implantation irrespective of symptoms. 2 Usually it requires urgent medical assistance and external cardiopulmonary resuscitation (CPR) for survival in prolonged ventricular asystole. Surviving such an event with self termination and without any medical assistance is quite rare and rarely mentioned in the literature. We report a 60‐year‐old healthy man who came to the outdoor patient department with a history of occasional dizziness for the past year. His physical examination revealed no significant abnormalities. The pulse was regular and supine blood pressure was 130/70 mmHg. The complete blood cell count, routine electrolyte, and renal biochemical tests were within normal limits. 12‐lead electrocardiogram (Figure 1) showed sinus rhythm, right axis deviation, first degree AV block with complete left bundle branch block. Echocardiogram revealed structurally normal heart. Twenty‐four hour Holter monitoring was performed with Zymed 3100 device (Zymed, Andover, MA, USA) which revealed (Figure 2) symptomatic ventricular arrest for one minute and fifty‐one seconds, which began at 8:32:10 a.m. after a premature beat and ended with single ventricle complex at 8:34:01 a.m. followed by scattered idioventricular beats; it took two minutes and three seconds before baseline rhythm was restored. According to the patient, at that time he felt dizziness and lay down, and was fine after some time. As there was no witness to the event so the mechanism of self‐termination is unexplained. The patient was successfully treated with St. Jude DDD permanent pacemaker (St. Jude Medical, St. Paul, MN. USA) and is on asymptomatic follow‐up since last year. Criley et al. 3 and Neimann et al. 4 have mentioned a few patients who successfully resuscitated by repeated coughing and termed it cough‐induced CPR. Although the mechanism of self‐resuscitation is not clear in our case, surviving such a prolonged event of ventricular standstill is a miracle in itself. It certainly throws light on the possibility of various mechanisms of self‐resuscitation which need to be explored.
Figure 1.
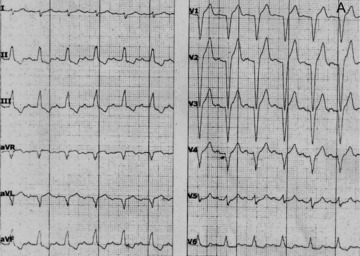
12‐lead electrocardiogram demonstrating normal sinus rhythm, right axis deviation, first degree AV block and complete left bundle branch block.
Figure 2.

Holter strip showing normal sinus activity with ventricular arrest lasting for about two minutes terminating with scattered idioventricular beats.
CONCLUSION
Our case demonstrates the unique example of self‐resuscitation after having prolonged ventricular arrest which was recorded on Holter monitoring.
REFERENCES
- 1. Peter L, Robert OB, Douglas PZ, et al Braunwald's Heart Disease—A Text book of cardiovascular medicine. Philadelphia, Saunders, 2008.
- 2. Gabriel G, Cheitlin MD, Conill A, et al ACC/AHA guidelines for implantation of cardiac pacemakers and antiarrhythmia devices: Executive summary. Circulation 1998;97:1325–1335. [DOI] [PubMed] [Google Scholar]
- 3. Criley JM, Blaufuss AH, Kissel CL. Cough‐induced cardiac compression: Self administered form of cardiopulmonary resuscitation. JAMA 1976;236:1246–1250. [PubMed] [Google Scholar]
- 4. Niemann JT, Roshorough J, Hausknecht M, et al Cough‐CPR. Documentation of systemic perfusion in man and in an experimental model: A “window” to the Mechanism of blood flow in external CPR. Crit Care Med 1980;8:141–146. [DOI] [PubMed] [Google Scholar]