

Abstract
Aims
The aim of the study was to analyze the value of a completely new fuzzy logic–based detection algorithm (FA) in comparison with arrhythmia classification algorithms used in existing ICDs in order to demonstrate whether the rate of inappropriate therapies can be reduced.
Methods
On the basis of the RR intervals database containing arrhythmia events and controls recordings from the ICD memory a diagnostic algorithm was developed and tested by a computer program. This algorithm uses the same input signals as existing ICDs: RR interval as the primary input variable and two variables derived from it, onset and stability. However, it uses 15 fuzzy rules instead of fixed thresholds used in existing devices. The algorithm considers 6 diagnostic categories: (1) VF (ventricular fibrillation), (2) VT (ventricular tachycardia), (3) ST (sinus tachycardia), (4) DAI (artifacts and heart rhythm irregularities including extrasystoles and T‐wave oversensing‐TWOS), (5) ATF (atrial and supraventricular tachycardia or fibrillation), and 96) NT (sinus rhythm). This algorithm was tested on 172 RR recordings from different ICDs in the follow‐up of 135 patients.
Results
All diagnostic categories of the algorithm were present in the analyzed recordings: VF (n = 35), VT (n = 48), ST (n = 14), DAI (n = 32), ATF (n = 18), NT (n = 25). Thirty‐eight patients (31.4%) in the studied group received inappropriate ICD therapies. In all these cases the final diagnosis of the algorithm was correct (19 cases of artifacts, 11 of atrial fibrillation and 8 of ST) and fuzzy rules algorithm implementation would have withheld unnecessary therapies. Incidence of inappropriate therapies: 3 vs. 38 (the proposed algorithm vs. ICD diagnosis, respectively) differed significantly (p < 0.05). VT/VF were detected correctly in both groups. Sensitivity and specificity were calculated: 100%, 97.8%, and 100%, 72.9% respectively for FA and tested ICDs recordings (p < 0.05).
Conclusions
Diagnostic performance of the proposed fuzzy logic based algorithm seems to be promising and its implementation could diminish ICDs inappropriate therapies. We found FA usefulness in correct diagnosis of sinus tachycardia, atrial fibrillation and artifacts in comparison with tested ICDs.
Keywords: implantable cardioverter‐defibrillator(ICD), inappropriate ICD therapies, supraventricular versus ventricular tachycardia discrimination algorithms, fuzzy logic
INTRODUCTION
There is a powerful device in the prevention of sudden cardiac death (SCD): an implantable cardioverter‐defibrillator (ICD). The results of many primary and secondary prevention trials1, 2, 3, 4, 5 caused rapid growth in cardiovascular implantable electronic devices (CIED) implantations so the rate of related complications increases as well. The defibrillators existing on the market tend to apply more therapies than necessary on the basis of the rule: “safety first.” The unnecessary shocks, due to false VF or VT detection, deplete the battery power, shorten the longevity of the device which requires premature reimplantation. These discharges are painful for the patient and may influence patients psychosocial well being, may result in psychiatric sequel6, 7 and proarrhythmia.8 In some cases inappropriate therapies (IT) may cause death.9 The fear of IT delivery during exercise withholds the patients from daily and sport activities.10
Therefore, reduction of the ICDs IT is a crucial issue for this therapy of life‐threatening arrhythmias. The most important detection criterion used by ICD is the length of RR intervals. It means that the arrhythmia is detected if a certain number of consecutive intervals are shorter than the preprogrammed value. All ICDs meet additional criteria like sudden onset and stability to differentiate between atrial and ventricular arrhythmias. Dual‐chamber devices (DDD) compare the atrial and ventricular rhythm. Superior from the theoretical point of view11, 12, 13, 14, 15, 16 do not present higher specificity for SVT tachycardias over single‐chamber (VVI) ICDs in avoiding IT in some studies.1
The contemporary tachyarrhythmia detection algorithms of VVI and DDD ICDs are based on the timing (high rate‐only criterion) and the morphology of cardiac signals (characteristics of the electrogram to differentiate SVT and ventricular tachycardias). The latter algorithm compare a series of ventricular complexes during sinus rhythm, obtaining a patient specific template and if detected QRS morphology which is similar to the template, the rhythm is regarded as SVT.17 It may result in inappropriate detection of VT in the presence of aberrancy during SVTs (rate‐related and/or ischemia) or by changes in basic cardiac cycle morphology. The RR interval information, when used alone, offers highest sensitivity detection of true VT/VF but lower sensitivity.
In the case of a single‐chamber defibrillator, up to 40% of delivered therapies are inappropriate.17 However, single‐chamber ICDs represent more than half of implants.
The aim of this study is to test the diagnostic value of the newly created fuzzy logic–based algorithm for ICDs (FA) and to demonstrate if IT occurrence can be reduced with this detection algorithm. The overview of this methodology in general is also available on the Website.18
The ICD unnecessary therapy remains a very appropriate problem for the fuzzy logic approach. The fuzzy logic19, 20 is a mathematical theory developed in order to apply imprecise rules of human thinking in a precise way to problems having no ordinary mathematical models or good algorithmic solutions. The fuzzy logic is based on two main concepts: fuzzy set and linguistic variable.19, 20 A fuzzy set is characterized by a membership function, which can have any value between (and including) 0 and 1. This function assigns a membership value (also called degree of membership) to every investigated phenomenon, for example, the heart rate (HR). The membership functions of adjacent sets may overlap, and HR values may belong partly to one fuzzy set and partly to another. Every membership function establishes a quantitative link between a linguistic variable (and a fuzzy set associated with it) and an ordinary measurable quantity. There are three basic logical operators applied to fuzzy sets: AND, OR, and NOT. These three operators can also be implemented in other ways, for example, AND and OR can be implemented as a product and a sum of the grades of membership, respectively. To apply the fuzzy logic to a particular problem, we have to define a suitable set of the fuzzy rules. These rules are defined in terms of linguistic variables and usually come from human experience. A typical rule has the form
IF ((A is a) AND (B is b)) OR ((C is c) AND (D is d)) THEN (E is e), where A, B, C, D, and E are linguistic variables (with appropriate fuzzy sets associated with them) and a, b, c, d, and e are values of these variables.
To apply fuzzy logic to a particular problem, one has to define the input and output variables, the fuzzy sets and the fuzzy rules. If the fuzzy sets and the rules are not obvious, an optimization procedure may be used. The shapes of the membership functions and the set of fuzzy rules have to be optimized using an optimization algorithm and the training set of RR recordings for which correct diagnoses are known.
The fuzzy logic can be used for automatic control of a physical process, decision making, classification or diagnosis, etc. A typical structure of a fuzzy logic–based diagnostic or control algorithm is shown in Figure 1.
Figure 1.
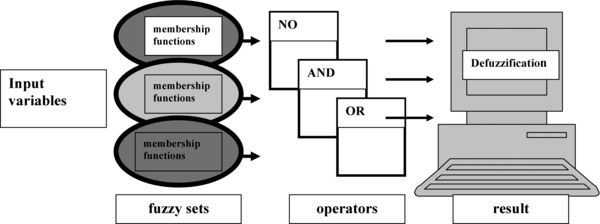
The structure of a fuzzy logic–based diagnostic algorithm.
MATERIAL AND METHODS
From a data base containing RR interval series (8000–10,000 intervals) of the arrhythmia events and controls, stored in the ICD memory and archived on PC during systematic control visits of 135 consecutive patients, 172 recordings were analyzed. The inclusion criteria were: full data availability, that is, RR interval series with simultaneous IEGM (intracardiac electrogram) prints in case of arrhythmia event and clinical data (symptoms reported by a patient). The episodes of ICD intervention and controls were analyzed and qualified by two cardiologists (M.L., A.P.).
Study group characteristics (etiology and indications for implantation): age 57 ± 28 years, 75% males, 15% implanted for primary prevention, 85% for secondary prevention, 58% had coronary artery disease (CAD), 15% nonischemic dilated cardiomyopathy (DCM), 15% hypertrophic cardiomyopathy (HCM), 12% other causes.
Follow‐up took 3–126 months (mean 64).
The following rhythm classification was made by two cardiologists in six diagnostic categories (the proposed algorithm considers the same six diagnostic categories):
Category 1: VF, ventricular fibrillation
Category 2: VT, ventricular tachycardia
Category 3: ST, sinus tachycardia
Category 4: DAI, detection of artifacts and irregularities, including extrasystoles and T‐wave oversensing (TWOS)
Category 5: ATF, atrial, and SVT or atrial fibrillation
Category 6: NT, no tachycardia or sinus rhythm
A heart rate more than 132 bpm, which was an arbitrary lower limit of ventricular tachychardia, suggested by a medical expert, was applied to VT category.
RR recordings came from VVI devices (Medtronic, Biotronik) and were obtained in our institution—The National Institute of Cardiology, Warsaw, Poland.
FUZZY LOGIC METHODS
In the first phase of the study (pilot group n = 132), a training data set of 74 recordings of events with well‐confirmed diagnoses was built up, followed by the validation set of 58 recordings. All details of pilot group study: the algorithm creation (FA) and validation are described and available on the website.18, 21
In the second phase of the study 172 more different RR recordings were tested by the created algorithm and evaluated for the statistical analysis in this study.
In our project, the FA result can have any value between 0 and 1, and not only either 0 or 1 as in classical two‐valued logic. Every fuzzy rule translates a rule expressed in a natural language into a mathematical relationship which allows to calculate some output quantity for the given values of some input quantities.
In terms of the fuzzy set theory, we have three input variables and defined six output fuzzy sets corresponding to six output diagnostic categories. The output is in the form of six numbers having values between 0 and 1, assigned to six diagnostic categories. The highest value (highest degree of membership) indicates the most probable diagnosis. The diagnosis is updated after every new RR interval.
Sensitivity and specificity of the proposed algorithm and ICD diagnosis were calculated on the basis of the widely accepted criteria (equations are given in the appendix).
Incidence of inappropriate therapies was analyzed and compared (the FA implementation vs ICD diagnosis, respectively). This study was approved by the National Institute of Cardiology Ethical Committee on Human Research, Warsaw, Poland. The informed consent was obtained after the nature and possible consequences of this study were explained to every patient. This study protocol complies with the Declaration of Helsinki.
The results were analyzed by using SPSS/PC+ statistical software. Quantitative variables were compared by the Student's t‐test. Fisher's test was used when indicated (comparison of incidence of inappropriate therapies and specificity of tested algorithms). Statistical significance was set at a probability (P) value P < 0.05.
RESULTS
All diagnostic categories of the FA were present in the analyzed recordings: VF (n = 35), VT (n = 48), ST (n = 14), DAI (n = 32), ATF (n = 18). The examples of RR analysis by a computer program based on the FA before and following ICD discharge due to VF and artifacts are presented in Tables 1 and 2. These tables are the parts of original printouts from PC programme incorporating FA. A result has any value between (an including) 0 and 1. This result indicates probability of a complex phenomenon such a heart rhythm classification. Probability between and including 0.8 and 1 (arbitrary decided) indicates positive result for the diagnosis of the certain kind of the heart rhythm. If the value of final diagnosis exceeds 1 (like in the given examples sometimes) it means it equals 1, this discrepancy comes from mathematical method of calculation. These two examples in the form of tables of true VF and artifacts explain the way of diagnosis creation. The entire analysis of certain episode consists of all diagnoses corresponding to each time point (column 1). In both examples, ca. 9000 RR values (time points) were analyzed. The columns 2–7 represent six diagnostic categories of FA, the columns 8–10 depicts three input variables (interval, onset, instability).
Table 1.
The Result of RR Analysis by a Computer Program Based on the Fuzzy Detection Algorithm before and Following ICD Discharge due to VF
| Time point | VF | VT | ST | DAI | AT | NT | Interval | Onset | Instability | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 0 | 0 | 0 | 0 | 0 | 1 | 848 | 0 | 0 | |
| 2 | 0 | 0 | 0 | 0 | 0 | 1 | 832 | 0 | 16 | |
| 3 | 0 | 0 | 0 | 0 | 0 | 1 | 828 | −16 | 20 | |
| (Not continuous) | ||||||||||
| 9046 | 1.049 | 0.03568 | 0 | 0 | 0 | 0 | 207 | −160 | 23 | |
| 9047 | 0.6819 | 0 | 0 | 0.0009859 | 0.4308 | 0 | 113 | −160 | 117 | |
| 9048 | 0.3016 | 0 | 0 | 0 | 0.7406 | 0 | 211 | −160 | 98 | |
| 9049 | 0.3677 | 0 | 0 | 0 | 0.6868 | 0 | 203 | −160 | 98 | |
| 9050 | 0.1005 | 0 | 0 | 0.05733 | 0.8589 | 0 | 254 | −160 | 141 | |
| 9051 | 0.1566 | 0 | 0 | 0.07731 | 0.7922 | 0 | 219 | −160 | 141 | |
| 9052 | 0.8726 | 0.01465 | 0 | 0 | 0.146 | 0 | 230 | −160 | 51 | |
| 9053 | 0 | 0 | 0 | 0.03716 | 0.9628 | 0 | 434 | −160 | 230 | |
| ⇒ | 9054 | 0.948 | 0.0229 | 0 | 0 | 0.07713 | 0 | 230 | −160 | 43 |
| ⇒ | 9055 | 0.9502 | 0.01902 | 0 | 0 | 0.08134 | 0 | 207 | −160 | 43 |
| ⇒ | 9056 | 0.9579 | 0.01896 | 0 | 0 | 0.07188 | 0 | 219 | −160 | 43 |
| ⇒ | 9057 | 1.045 | 0.03885 | 0 | 0 | 0 | 0 | 227 | −160 | 23 |
| ⇒ | 9058 | 1.049 | 0.0353 | 0 | 0 | 0 | 0 | 211 | −160 | 23 |
| ⇒ | 9059 | 1.052 | 0.04484 | 0 | 0 | 0 | 0 | 227 | −160 | 20 |
| ⇒ | 9060 | 1.06 | 0.05136 | 0 | 0 | 0 | 0 | 227 | −160 | 16 |
| ⇒ | 9061 | 1.066 | 0.04625 | 0 | 0 | 0 | 0 | 215 | −160 | 16 |
| ⇒ | 9062 | 1.056 | 0.0412 | 0 | 0 | 0 | 0 | 207 | −160 | 20 |
| ⇒ | 9063 | 1.048 | 0.03611 | 0 | 0 | 0 | 0 | 203 | −160 | 23 |
| ⇒ | 9064 | 1.023 | 0.03391 | 0 | 0 | 0.006271 | 0 | 234 | −160 | 31 |
| ⇒ | 9065 | 1.031 | 0.02715 | 0 | 0 | 0.005647 | 0 | 223 | −160 | 31 |
| ⇒ | 9066 | 1.032 | 0.02595 | 0 | 0 | 0.005615 | 0 | 219 | −160 | 31 |
| 9067 | 0 | 0 | 0 | 0 | 0 | 1 | 859 | −160 | 656 | |
| 9068 | 0 | 0 | 0 | 0 | 0 | 1 | 895 | −160 | 676 | |
This patient is presented in Figure 2. Right arrows (lower left) mark detection of VF in the first column.
Table 2.
The Result of RR Analysis by a Computer Program Based on the Fuzzy Detection Algorithm before and Following Inappropriate ICD Discharge
| Time point | VF | VT | ST | DAI | ATF | NT | Interval | Onset | Instability | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 0 | 0 | 0 | 0 | 0 | 1 | 793 | 0 | 0 | |
| 2 | 0 | 0 | 0 | 0 | 0 | 1 | 805 | 0 | 12 | |
| (Not continuous) | ||||||||||
| 7203 | 0 | 0 | 0 | 0 | 0 | 1 | 852 | 0 | 20 | |
| 7204 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 250 | −4 | 613 |
| 7205 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 258 | −586 | 602 |
| 7206 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 74 | −586 | 777 |
| 7207 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 168 | −586 | 777 |
| 7208 | 0.1919 | 0 | 0 | ⇒ | 0.8099 | 0.03021 | 0 | 156 | −586 | 184 |
| 7209 | 0.2398 | 0 | 0 | ⇒ | 0.7676 | 0.03257 | 0 | 125 | −586 | 184 |
| 7210 | 1.021 | 0 | 0 | 0 | 0.1431 | 0 | 141 | −586 | 94 | |
| 7211 | 0.9845 | 0 | 0 | 0 | 0.08731 | 0 | 191 | −586 | 66 | |
| 7212 | 1.019 | 0 | 0 | 0 | 0.1117 | 0 | 137 | −586 | 66 | |
| 7213 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 332 | −586 | 207 |
| 7214 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 117 | −586 | 215 |
| 7215 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 191 | −586 | 215 |
| 7216 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 188 | −586 | 215 |
| 7217 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 129 | −586 | 215 |
| 7218 | 0.5052 | 0 | 0 | 0.3962 | 0.1828 | 0 | 242 | −586 | 125 | |
| 7219 | 0.2688 | 0 | 0 | 0.6152 | 0.1608 | 0 | 270 | −586 | 141 | |
| 7220 | 0.5715 | 0 | 0 | 0.4188 | 0.1049 | 0 | 180 | −586 | 141 | |
| 7221 | 0.6523 | 0 | 0 | 0.3559 | 0.1005 | 0 | 152 | −586 | 141 | |
| 7222 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 125 | −586 | 344 |
| 7223 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 125 | −586 | 344 |
| 7224 | 0 | 0 | 0 | ⇒ | 1 | 0 | 0 | 39 | −586 | 430 |
| 7225 | 0 | 0 | 0 | 0 | 0 | 1 | 898 | −586 | 859 | |
Intervention was caused by device oversensing (lead insulation disruption and extracardiac noise resulting in misdiagnosis of VF by ICD). This patient is presented in Figure 3. Right arrows mark detection of artifacts in the fifth column.
In the Table 1 time points numbered 9054–9066 indicate VF diagnosis in the 2nd column. In the Table 2, time points numbered 7204–7209 and 7213–7217, and 7222–7224 indicate DAI diagnosis in the 5th column. This is correct FA diagnosis instead of the false ICD diagnosis (VF).
Corresponding to Table 1, the ICD IEGM and ICD RR pattern before and following ICD appropriate discharge due to VF is presented in Figure 2. Corresponding to Table 2, the ICD IEGM and ICD RR pattern before and following ICD inappropriate discharge due to oversensing = artifacts (lead insulation disruption and misdiagnosis of VF by ICD) is presented in Figure 3.
Figure 2.
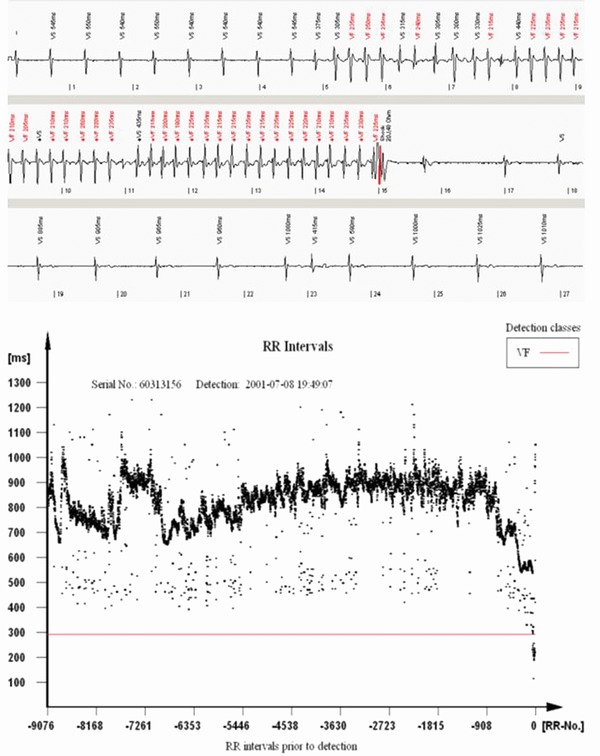
ICD‐stored electrogram and RR pattern before and following ICD appropriate discharge due to VF.
Figure 3.
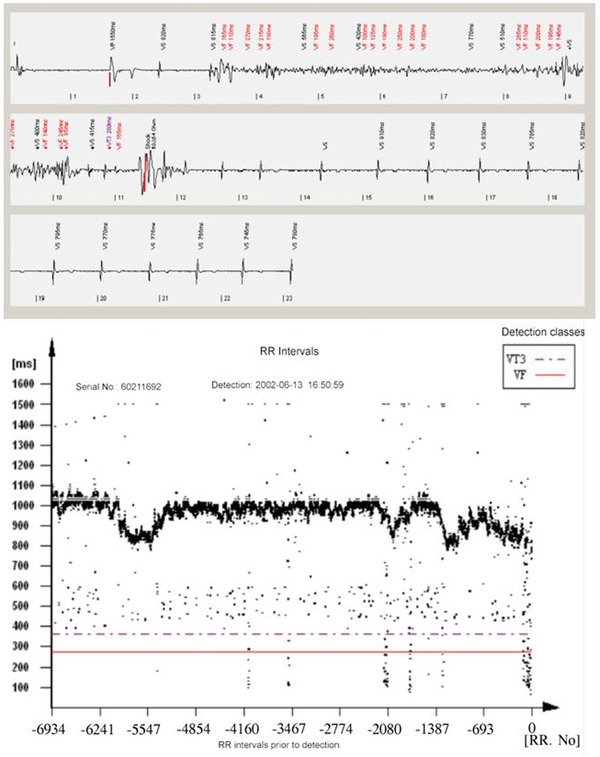
ICD‐stored electrogram and RR pattern before and following ICD inappropriate discharge due to oversensing (lead insulation disruption and misdiagnosis of VF by ICD).
A crucial proof of the effectiveness of the life‐threatening arrhythmias therapy is the correct detection of VT/VF category: both FA and ICD detected the VF in all above cases. The summary of the events analysis for tested ICDs: for 172 recordings 121 shocks were delivered by ICD: 38 of 121 (31.4%) shocks were completely unjustified: 8 for ST, 19 for DAI (including TWOS), 11 for ATF. The FA diagnosis failed three times in the analyzed group. In 1 case fast VT was recognized as VF (a FA driven ICD would deliver one unjustified shock instead of an ATP attempt), in two cases VT was diagnosed instead of ST (a FA driven ICD would deliver two more unjustified shocks).
Sensitivity and specificity of the FA algorithm calculated on the basis of the results presented above: 100% and 97.8%, respectively for the entire group. This was compared with calculated sensitivity and specificity of the tested ICD diagnosis in the same group: 100% and 72.9%. Specificity differed significantly (P < 0.05). Incidence of inappropriate therapies: 3 versus 38 (the simulation of the FA results vs. ICD diagnosis in “real life,” respectively) differed significantly (P < 0.05).
DISCUSSION
Our study evaluated the diagnostic value of the new developed fuzzy logic–based classification algorithm for the heart rhythm and found it effective in recognition of ventricular and SVT arrhythmias. However, in clinical practice the high sensitivity (i.e., correct VT and VF diagnosis) is accompanied by lower specificity (i.e., inappropriate treatment of SVT rhythms like ST, atrial fibrillation or artifacts).22, 23 This widely known fact is concordant with our results. We found moderate specificity of the tested ICDs (72.9%) in “real life” in studied group. This specificity is caused by the ICD technical detection characteristic and the device programming as well (the attending physician related). Specificity of the FA is high (97.8%) for a rate only detection algorithm without others features like the template. It gives hope for its future practical implementations. Specificity could probably be even better. The FA diagnostic errors require explanation: in two cases of VT detection instead of ST there are no beginnings of tachycardia recordings (long lasting episode of ST, longer than RR ICD's internal memory capacity), so the onset criterion could not have been applied. If it would have been possible in these cases, the diagnosis should be correct. In the third case, very fast VT is an example of the arrhythmia appropriate for ATP therapy instead of shock.24 However, this RR data and ICD programming come from the period before publishing Pain Free Study results in 2004, so programming fast VT (FVT) detection zone with the first therapy as an ATP sequence during or before charging could terminate FVT successfully without shock.25, 26
The inappropriate therapies incidence in our study—31.4% is concordant with median value presented in other investigations.26
The single‐chamber devices only were chosen for this study due to the fact that VVI‐ICD remain a majority (or at least half) of implantations.27 and that differentiation between VT and SVT is a more difficult diagnostic challenge for the single‐chamber ICDs without atrial channel information.
The most important finding of our study seems to be a proof that our fuzzy logic–based algorithm has comparable specificity with those implemented in DDD devices in different studies (39%, 64%, 89%, 91%, 92%, and 97%) although they should be superior to VVI from the theoretical point of view.13, 14, 15, 28, 29, 30, 31
The correct diagnosis of life‐threatening arrhythmias has to be made rapidly, within a few seconds from the beginning of the event, especially in the case of VF, as it can provoke a fatal outcome if not treated. Our algorithm meets these requirements. It is computationally very simple. An integrated circuit which implements the FA has been designed.32 Therefore, we believe that this algorithm is suitable as an additional detection feature for ICDs and may significantly improve the accuracy of arrhythmia detection.
The FA implementation is valid not only for shock reduction but also for ATPs. In the presented material for 121 shocks, 68 were preceded by ATP programming (in VT zone at the discretion of the physician). The correct diagnosis of AFib, ST or artefacts would withhold the ATP therapy in all those cases on the basis of the rule: “no detection = no therapy.”
The proposed algorithm once tested in ICD and while proven to be sufficient, can be added to those existing in clinical practice in order to avoid inappropriate therapies. This research on the optimization of the existing ICD therapy and future development of the device seems to be promising. To our knowledge this is the first attempt of the fuzzy logic implementation for this purpose. Some other studies were performed with different techniques33, 34 or the fuzzy logic–based different methodology.35, 36 The ICD is still a basic option for sudden cardiac death prevention but its inappropriate therapy is still not resolved issue for many years.35 The Internet data transfer opens potential application of the presented heart rhythm classification methodology in Holter ECG monitoring, implantable loop recorders and telemedicine. This study is new ECG‐based technique in the diagnosis and treatment of cardiac patients.
STUDY LIMITATIONS
An important limitation of our study is a relatively small number of recordings with atrial flutter, this situations are often associated with a high rate of inappropriate shocks.37 The single‐chamber devices only were chosen for this study due to the fact explained in the methods section, this could be regarded as an important limitation of the study. The template‐based algorithms could work together with the proposed FA. We did not had the opportunity to compare it because the tested ICDs in this study did not have the template function. The problem of discrepancy between two or three different algorithms including FA and the decision to override the other has to be explained in the future. We did not analyze it.
CONCLUSIONS
A fuzzy logic–based control algorithm for the ICD has been developed. Our study proved ability of this algorithm to decrease occurrence of inappropriate therapies without reducing sensitivity to the life‐threatening arrhythmias. We found FA usefulness in the correct diagnosis of ST, atrial fibrillation, and artefacts in comparison with the tested ICDs. We would welcome a future evaluation of the proposed algorithm in different populations. The computer program implementing the described above algorithm is accessible on the Website (http://defib.imio.pw.edu.pl).
The following equations were used for the calculation of sensitivity (i.e., appropriate ventricular arrhythmia = VT/VF diagnosis) and specificity (i.e., appropriate inhibition of therapy in case of appropriate diagnosis of supraventricular arrhythmia = SVT or other episodes not diagnosed as VT/VF):
| (1) |
| (2) |
This study was supported by a Polish Ministry of Science and Informatics Grant (No 3P05C 009 23) and performed in these institutions listed above
REFERENCES
- 1. Epstein AE. An update on implantable cardioverter‐defibrillator guidelines. Curr Opin Cardiol 2004;19:23–252. [DOI] [PubMed] [Google Scholar]
- 2. Oseroff O, Retyk E, Bochoeyer A. Subanalyses of secondary prevention implantable cardioverter‐defibrillator trials; antiarrhythmic versus implantable defibrillators (AVID), Canadian Implantable Defibrillator Study (CIDS), and Cardiac Arrest Study Hamburg(CASH). Curr Opin Cardiol 2004;19:26–30. [DOI] [PubMed] [Google Scholar]
- 3. Bardy GH, Lee KL, Mark DB, et al. Sudden cardiac death in heart failure trial (SCD‐heft) investigators. amiodarone or an implantable cardioverter‐defibrillator for congestive heart failure. N Eng J Med 2005;352(3):225–237. [DOI] [PubMed] [Google Scholar]
- 4. Moss AJ, Greenberg H, Case RB, et al. Multicenter automatic defibrillator implantation trial‐ii (madit‐ii) research group. long‐term clinical course of patients after termination of ventricular tachyarrhythmia by an implanted defibrillator. Circulation 2004;110(25):3760–3765. [DOI] [PubMed] [Google Scholar]
- 5. Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. A report of the american college of cardiology/american heart association task force and the european society of cardiology committee for practice guidelines (writing committee to develop guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death). developed in collaboration with the european hearth rhythm association and the heart rhythm society. Eur Heart J 2006;27(17):2099–2140. [DOI] [PubMed] [Google Scholar]
- 6. Sears SF, Burns JL, Handberg E, et al. Young at heart: Understanding the unique psychosocial adjustment of young implantable cardioverter defibrillators recipients. PACE 2001;24:1113–1117. [DOI] [PubMed] [Google Scholar]
- 7. Wójcicka M, Lewandowski M, Smolis‐Bąk E, et al. Psychological and clinical problems in youg adultes with implantable cardioverter‐defibrillators. Polish Heart J 2008;66,10:1050–1060. [PubMed] [Google Scholar]
- 8. Gradaus R, Block M, Brachmann J, et al. Mortality, morbidity and complications in 3344 patients with implantable cardioverter–defibrillators: Results from the German ICD registry EURID. Pacing Clin Electrophysiol 2003;26:1511–1514. [DOI] [PubMed] [Google Scholar]
- 9. Messali A, Thomas O, Chauvin M, et al. Death due to an implantable cardioverter defibrillator. J Cardiovasc Electrophysiol 2004;15:953–956. [DOI] [PubMed] [Google Scholar]
- 10. Van Ittersum M, De Greef M, van Gelder W, et al. Fear of exercise and health‐related quality implantable cardioverter defibrillator. Int J Rehabil Res 2003;26:117–122. [DOI] [PubMed] [Google Scholar]
- 11. Deisenhofer I, Kolb C, Ndrepepa G, et al. Do current dual chamber cardioverter defibrillators have advantages over conventional single chamber cardioverter defibrillators in reducing innapropriate therapies. A randomised, prospective study. J Cardiovasc Electrophysiol 2001;12(2):134–142. [DOI] [PubMed] [Google Scholar]
- 12. Sonne K, Phennig A, Bhandari AK, et al. Dual vs. single chamber ICDs : Equal incidence of inappropriate discharge in supraventricular events give rise to look closer. PACE 2001;24:489–491.11341087 [Google Scholar]
- 13. Wilkoff BL, Cook JR, Epstein AE, et al. Dual Chamber and VVI Implantable Defibrillator Trial Investigators. Dual chamber pacing or ventricular backup pacing in patients with an implantable defibrillator: The Dual Chamber and VVI Implantable defibrillator (DAVID) trial. JAMA 2002;288(24):315–323. [DOI] [PubMed] [Google Scholar]
- 14. Diemberger I, Martignani C, Biffi M. et al. Arrhythmia discrimination by physician and defibrillator: importance of atrial channel. Int J Cardiol 2012;154(20):134–140. [DOI] [PubMed] [Google Scholar]
- 15. Sinha AM, Stelbrink C, Schuchert A, et al. Clinical experience with a new detection algorithm for differentiation of supraventricular from ventricular tachycardia in a dual‐chamber defibrillator. J Cardiovasc Electrophysiol 2004;15(6):646–652. [DOI] [PubMed] [Google Scholar]
- 16. Kouakam C. Kacet S, Hazard JR, et al. Performance of a dual‐chamber implantable defibrillator algorithm for discrimination of ventricular from supra ventricular tachycardia. Europace 2004;6(1);32–34. [DOI] [PubMed] [Google Scholar]
- 17. Aliot E, Nitzsche R, Ripart A. Arrhythmia detection by dual‐chamber implantable cardioverter defibrillators. A review of current algorithms. Europace 2004;6:273–286. [DOI] [PubMed] [Google Scholar]
- 18.Fuzzy logic. Available at http://en.wikipedia.org/wiki/fuzzy_logic. Accessed August 29, 2013.
- 19. Zadeh LA. Information and Control, Vol. 8, 338–353, Academic Press, N. York, 1965. [Google Scholar]
- 20. Bárdossy A, Duckstein L. Fuzzy Rule‐Based Modeling with Applications to Geophysical, Biological and Engineering Systems, CRC Press, Boca Raton, FL, USA, 1995. [Google Scholar]
- 21. Kuźmicz W, Lewandowski M. Available at: http://defib.imio.pw.edu.pl, 2006. Accessed August 28, 2013.
- 22. Klein G, Gillberg JM, Tang A, et al. Improving svt discrimination in single‐chamber ICDs: A new electrogram morphology‐based algorithm. J Cardiovasc Electrophysiol 2006;17:1310–1319. [DOI] [PubMed] [Google Scholar]
- 23. Gillberg J. Detection of cardiac tachyarrhythmias in implantable devices. J Electrocardiol 2007;40:S123–S128. [DOI] [PubMed] [Google Scholar]
- 24. Wathen MS, Sweeney MO, Degroot PJ, et al. Shock reduction using antitachycardia pacing for spontaneous rapid ventricular tachycardia in patients with coronary artery disease Circulation 2001;104:796–801. [DOI] [PubMed] [Google Scholar]
- 25. Wathen MS, Sweeney MO, Degroot PJ, et al. Prospective randomized multicenter trial of empiric antitachycardia pacing versus shocks for spontaneous rapid ventricular tachycardia in patients with implantable cardioverter‐defibrillators: Pacing fast ventricular tachycardia reduces shocks therapies (painfree rx ii) trial results. Circulation 2004;110:2591–2596. [DOI] [PubMed] [Google Scholar]
- 26. Auricchio A, Meijer A, Kurita T, et al. Safety, efficacy, and performance of a new discrimination algorithms to reduce inappropriate and unnecessary shocks: The PainFree SST clinical study design. Europace 2011:139100:1484–1493. [DOI] [PubMed] [Google Scholar]
- 27. Wilkoff BL, Ousdigian KT, Sterns LD, et al. A comparison of empiric to physician‐tailored programming of implantable cardioverter‐defibrillator. Results from the prospective randomized multicenter empiric trial. J Am Coll Cardiol 2006;48:No 2;330–339. [DOI] [PubMed] [Google Scholar]
- 28. Lee MA, Corbisiero R, Nabert DR, et al. Clinical results of an advanced SVT detection enhancement algorithm. Pacing Clin Electrophysiol 2005;28(10):1032–1040. [DOI] [PubMed] [Google Scholar]
- 29. Corbisiero R, Lee MA, Nabert DR, et al. Performance of a New single‐chmaber ICD algorithm: Discrimination of supraventricular from ventricular tachycardia. Based on vector timing and correlation. Europace 2006;8(12):1057–1061. [DOI] [PubMed] [Google Scholar]
- 30. Gold MR, Shorofsky SR, Thompson JA, et al. Advanced rhythm discrimination for implantable cardioverter‐defibrillator using vector timing and correlation. J Cardiovasc Electrophysiol 2002;13(11):1092–1097. [DOI] [PubMed] [Google Scholar]
- 31. Shome S, Li D, Thompson J, McCabe A. Improving contemporary algorithms for implantable cardioverter‐defibrillator function. J Electrocardiol 2010;43(6):503–508. [DOI] [PubMed] [Google Scholar]
- 32. Bardossy A, Blinowska A, Jaworski Z, et al. Application of fuzzy logic to pacemaker control. Biocyber Biomed Eng 2003;23:5–6. [Google Scholar]
- 33. Kamousi B, Lin B, Al‐Ahmad A, et al. A covariance‐based algorithm; A novel technique w for rhythm discrimination. Eng. Med. Biol. 2008,20–25. [DOI] [PubMed] [Google Scholar]
- 34. Rojo‐Álvarez JL, García‐Alberola A, Arenalmaíz A, et al. Automatic discrimination between supraventricular and ventricular tachycardia using a multilayer perceptron in implantable cardioverter defibrillators. PACE 2002;25:1599–1604. [DOI] [PubMed] [Google Scholar]
- 35. Usher J, Campbell D, Vohra J, et al. Fuzzy logic‐controlled classifier for use in implantable cardioverter defibrillators. Pacing Clin Electroph 1999;22:183–6. [DOI] [PubMed] [Google Scholar]
- 36. Yeh YC, Wang WJ, Chiou CW. Heartbeat case determiantion using fuzzy logic method on ECG signals international. J Fuzzy Syst 11(4):250–261, 2009. [Google Scholar]
- 37. Theuns DA, Klootwijk AP, Goedhart D, et al. Prevention of inappropriate therapy in implantable cardioverter‐defibrillators: Results of a prospective, randomized study of tachyarrhythmia detection algorithms. J Am Coll Cardiol 2004;44(12):2362–7. [DOI] [PubMed] [Google Scholar]