

Abstract
We report a case of an infant who developed transient complete heart block following aortic and mitral valve surgery. In the course of his recovery, he developed a variable morphology wide complex rhythm with intermittent narrow complex beats. Review of his initial postoperative electrocardiogram (ECG), which demonstrated a right bundle branch block, helped to clarify the rhythm.
Keywords: bundle branch block, fusion complexes
CASE
A 3‐month‐old male with a history of aortic and mitral valve disease underwent a Ross‐Konno procedure and mitral valve repair. His initial electrocardiogram (ECG) upon returning from the operating room demonstrated a nonsinus atrial rhythm and a right bundle branch block (RBBB) (Fig. 1). During the first postoperative night he developed complete heart block and was AV sequentially paced with temporary atrial and ventricular epicardial wires. On postoperative day 1, an ECG was obtained upon cessation of pacing, which demonstrated a wide complex rhythm with three different QRS morphologies (Fig. 2). What is the etiology of the variable QRS morphology?
Figure 1.
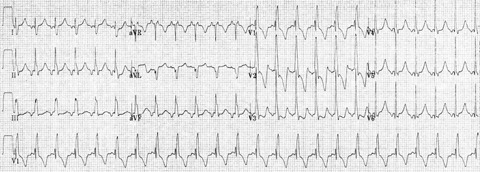
Postoperative ECG demonstrating an atrial rhythm with a right bundle branch block.
Figure 2.
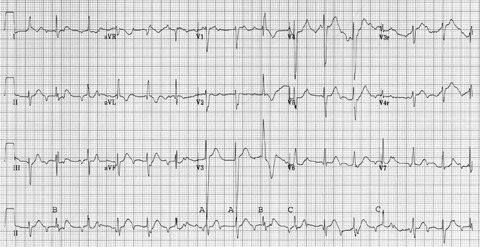
Fifteen‐lead ECG 16 hours postoperatively demonstrating various morphology of QRS complexes. “A,”“B,” and “C” correspond to different ventricular morphologies.
DISCUSSION
The ECG (Fig. 2) reveals evidence of heart block with intermittent AV nodal conduction and three different QRS morphologies. Distortion of many QRS complexes by P waves complicates interpretation of the etiology of the ventricular beats. The atrial cycle length is approximately 380 ms. P waves, which fall within 370 ms of the previous ventricular beat, fail to conduct while P wave greater than 400 ms after a ventricular beat demonstrates AV nodal conduction with a prolonged PR interval. A possibility of retrograde‐ concealed conduction into the AVN could be raised, as the conducted beats demonstrate a prolonged PR interval. The exact level of block cannot be determined from the surface ECG.
A majority of the ventricular beats have a morphology similar to “A,” which are ventricular escape beats with a left bundle branch pattern, with a cycle length of 640 ms. Their relatively narrow morphology and left bundle branch block (LBBP) pattern suggests that they arise from within the Purkinje system on the right side, below the area of block. Sporadically, there are beats transmitted through the AV node with a prolonged PR interval, which demonstrate a RBBB morphology (“B”) similar to the postoperative ECG. Intermittently, there are narrowed beats, which are not similar to either pattern (“C”), representing “normalizing” fusion beats.
Normalization of a bundle branch block due to fusion with a premature ventricular contraction (PVC) from the ventricle ipsilateral to the block has been described. 1 , 2 Similarly, patients with a Wolff‐Parkinson‐White ECG may demonstrate normalization of the QRS morphology if the accessory pathway is located ipsilateral to the bundle branch block. 3 Our patient has a wide complex escape rhythm arising from the right ventricle, as well as a baseline RBBB upon conduction via the AV node. Intermittently, an impulse that traverses the AV node fuses with a ventricular escape beat, producing a narrowing of the QRS complex (Fig. 3) due to ventricular fusion. As would be expected, beats that demonstrate a more significant degree of ventricular fusion, and thus a narrower QRS morphology, tend to have a shorter PR interval. The PR interval of the conducted beats (“B”) measure 210 ms, while the PR intervals of the fused beats (“C”) vary between 150 and 170 ms.
Figure 3.
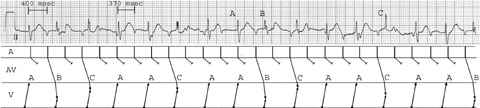
Rhythm strip copied from Figure 2, demonstrating the conduction pattern underlying the variable QRS morphology. Beats A are ventricular escape beats with a LBBB morphology. Beats B are conducted via the AV node and have a similar appearance to the postoperative surface ECG with a RBBB morphology. Beats C represent _normalized fusion beats, and are thus narrower with a shorter PR interval.
On postoperative day 2 the patient demonstrated recovery of AV nodal function with a persistent RBBB. This case demonstrates the critical importance of obtaining an early postoperative ECG in the accurate assessment and management of complex arrhythmias following open heart surgery in children and adults.
The authors have no conflict of interest and there was no financial support for this case report.
This submission is with the full knowledge and approval of the listed coauthors.
REFERENCES
- 1. Schamroth L, Agathangelou N. QRS normalization by ventricular fusion. A study of intraventricular conduction. Pacing Clin Electrophysiol 1981;4:448–451. [DOI] [PubMed] [Google Scholar]
- 2. Witcombe B, Schamroth L. A study in intracardiac conduction. ‘Normalization’ of bundle‐branch block by fusion with ventricular escape beats. Br Heart J 1972;34:213–216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Gersony WM, Ekery DD. Concealed right bundle branch block in the presence of type B ventricular pre‐excitation. Am Heart J 1969;77:668–676. [DOI] [PubMed] [Google Scholar]