

Abstract
Background: Sildenafil citrate may have direct cardiac electrophysiological effects, and is possibly responsible for some cardiac events. The aim of our study was to investigate the effects of sildenafil citrate on QT dynamicity properties with a new QT analysis program showing even small changes in ventricular repolarization.
Methods: Twenty‐four‐hour Holter electrocardiographic recordings were used to obtain the data in the predrug phase (1‐hour rest position before drug administration), and in the postdrug phase (1‐hour rest position, which began 60 minutes after 50 mg oral sildenafil citrate administration). With the special QT analysis program (Verda, Reynolds Medical Ltd., UK); mean values of RR, QT, QTo (corrected QT), J (the exponent of correction formula) and S (QT/RR plots slope) parameters together with QT variability indexes (QTVI) were calculated for study phases.
Results: Mean ± SEM values for RR and QT were higher in postdrug phase than in predrug phase (RR: 845 ± 42 ms vs 816 ± 46 ms, P < 0.05; QT: 371 ± 8 ms vs 361 ± 9 ms, P < 0.05). However, sildenafil did not induce any significant change in mean ± SEM values for QTo, J, and S in postdrug phase compared with predrug phase (408 ± 10 ms vs 406 ± 8 ms, 0.474 ± 0.030 vs 0.433 ± 0.025, 0221 ± 0.020 vs 0.198 ± 0.017, respectively; P > 0.05). QTVIs were also not different in each phase (predrug: −0.874 ± 0.071 vs postdrug: −0.997 ± 0.067, P = 0.109).
Conclusions: Fifty milligrams sildenafil does not affect QT dynamicity properties. The cardiac events associated with sildenafil could not be explained with ventricular arrhythmias.
Keywords: sildenafil, QT dynamicity, erectile dysfunction, ventricular arrhythmia
The introduction of sildenafil citrate into clinical practice has opened a new era for the treatment of impotence. 1 , 2 A certain number of patients suffering from erectile dysfunction have coronary heart disease with or without any symptoms. However, erectile dysfunction is also an important health problem in patients with cardiovascular disease. 3 Although sildenafil use is considered safe, some cardiac events have been reported after marketing the drug. 4 , 5 , 6 The cardiac events and the side effects of sildenafil are ascribed to its vasodilatation properties. When used together with nitrates, this vasodilatation effect is augmented and results in significant hypotension; thus, sildenafil is absolutely contraindicated in patients taking any kind of nitrate preparation. 7 Some other possible mechanisms are recently suggested to explain cardiovascular events associated with the use of sildenafil. Phillips et al. 8 demonstrated the vascular sympathetic activation effect of sildenafil, and Piccirillo et al. 9 suggested that these effects on the autonomic cardiovascular functions resulted in some repolarization abnormalities in patients with heart failure and healthy volunteers. In addition to these mechanisms, the data from in vitro animal studies showed that sildenafil might have direct cardiac electrophysiological effects similar to class III antiarrhythmic drugs in high concentrations or any effect on repolarization in clinical doses. 10 , 11 However, the data on the effects of sildenafil on QT interval and QT dynamics in clinical doses are limited in the literature. If sildenafil affects QT dynamics in clinical conditions, its use may render the patients prone to ventricular arrhythmias.
The relationship between serious arrhythmia generation and QT interval was well established. Dynamic QT analysis methods, which measure changes in QT duration and QT rate dependence rather than absolute values, may give more reliable information than QT dispersion calculated directly from surface electrocardiography with questionable reproducibility. 12 This relatively new kind of QT evaluation studies showed that patients having steeper QT/RR slopes (S) were prone to lethal arrhythmias. 13 , 14 It has also been established that patients with long QT syndrome have steeper S during the night than control subjects and class III antiarrhythmic agents cause steeper S in healthy volunteers as well. 15 , 16 However, QT rate dependence is an important parameter, the precise relationship between the QT and the RR data at any time can be defined as QT = QTo (RR/RRo)J; where “QTo” is the extrapolated QT at RRo, and “J” is the exponent of the formula that determines the shape of the QT/RR relation curve. A new dynamic QT analysis program was developed and validated, 17 by which the S together with J parameter of the QT/RR relationship can continuously be calculated in a given time interval. In other words, QT/RR rate dependence together with corrected QT and correction formula parameters can be obtained over even short intervals allowing accurate estimation of ventricular repolarization properties. Thus, the aim of our study was to investigate the effects of sildenafil on QT/RR association using a precise method with a new dynamic QT analysis program in a stable clinical condition.
METHODS
Study Population
Our study population consisted of 20 patients (mean age 52 ± 2 years, range 48‐61 years) having erectile dysfunction and all of the patients were in sinus rhythm. They were suffering from erectile dysfunction (27 ± 7 months, range 7–36 months) for which they were taking sildenafil at an adequate dose of 50 mg. Patients having unstable clinical conditions (i.e., acute coronary syndrome, uncontrolled hypertension), with recent myocardial infarction within 6 months and functional capacity worse than NYHA class II, and with insulin‐dependent diabetes mellitus were not included in the study. The patients taking beta‐adrenergic receptor blockers or antiarrhythmic agents were also excluded from the study owing to their well‐known effects on electrocardiographic intervals and dynamics. They were allowed to receive their routine medications other than nitrate preparations.
Study Design
All patients gave written informed consent, and the departmental ethical committees of our cardiology and urology clinic approved the study protocol. Following at least 8 hours of sleep and after having breakfast free of caffeine‐containing beverages, 24‐hour Holter recordings were initiated between 08:00 and 09:00 a.m. in the hospital. Participants went home and had rest in supine position for 1 hour in their comfortable environment. After this baseline period, they received 50 mg sildenafil citrate (Viagra, Pfizer, Turkey) and continued to rest in supine position 2 hours more. They mobilized to exclusively meet their basic requirements within the first hour after administration of the drug, and drink only plain water during the study period. Patients recorded the exact starting times of each phase of the study based on the Holter recorder clock. Holter recordings were terminated the next morning. The first 1‐hour rest period before drug administration was defined as the predrug phase. Because of the fact that sildenafil reaches its maximum effect within 1 hour, 18 the first 1‐hour period after drug administration was not taken into consideration; thus, the second 1‐hour rest period after drug administration was defined as postdrug phase.
QT Analysis
Electrocardiographic data were obtained with a 3‐channel “LifeCard” recorder (Reynolds Medical Limited, Hertford, UK) and analyzed with a Pathfinder Analyzer (Reynolds Medical Limited) on a personal computer. The remaining parts of the 24‐hour recordings other than the 3‐hour study period (beginning with predrug phase and ending with postdrug phase) were inhibited and the study period was analyzed with the new software called Verda (Version 1.19, Reynolds Medical Limited). The Q and T wave markers of all beats were visually examined, and adjusted if they were not accurate with the joint agreement of two trained cardiologists. However, the details of the analysis were described previously, 17 the main feature of the program is the calculation of RR, QT, QTo, S, J, and correlation coefficients between QT and RR parameters of the QT/RR relationship for whole study period and for a given single period. The program applies a compensation for the RR interval, which is a well‐known phenomenon called a two‐component time lag. 19 , 20 QTo, S, and J exponent are available when the QT and RR correlation remains high (r>0.80). After analyses with the Verda program were completed for the whole study period, the data of pre‐drug and postdrug periods of the study were extracted and averaged. Averaged values were used for statistical comparisons and for the calculation of QT variability index (QTVI) of the study phases with the following formula: QTVI = log10[(QT variance)/(mean QT)2]/[(RR variance)/(mean RR)2]. 21
Statistical Analysis
Results were expressed as mean ± SEM. Wilcoxon signed rank test was used to evaluate differences between the matched data obtained during pre‐ and postdrug phases.
RESULTS
Patient characteristics are shown in Table 1. All participants' study periods were completed between 10:00 a.m. and 01:00 p.m. None of the patients reported any side effect that could be attributable to sildenafil. No serious arrhythmia was noted in the routine Holter electrocardiography examinations, except single supraventricular and ventricular ectopic beats. One patient's data were excluded after routine analysis because of alternating left bundle branch block that might disturb Verda analysis. Three patients' data were lost due to incorrect analysis and saving procedures during the period of learning curve of the program. Consequently, data from 16 patients were available for statistical comparisons (mean age 53 ± 2 years, range 38‐65 years).
Table 1.
Clinical Features of the Patients
| Clinical Characteristics | Percent of All Patients (n = 20) | Percent of Patients with Available Verda Data (n = 16) |
|---|---|---|
| Tobacco use | 60 (12) | 63 (10) |
| Hypercholesterolemia | 35 (7) | 31 (5) |
| Hypertension | 45 (9) | 50 (8) |
| Diabetes mellitus | 30 (6) | 38 (6) |
| Previous CABG | 10 (2) | 13 (2) |
| Previous PCI | 5 (1) | 6 (1) |
| Previous MI | 15 (3) | 19 (3) |
| Heart failure | 15 (3) | 19 (3) |
| Medication | ||
| ACEi or ARB | 50 (10) | 56 (9) |
| Calcium channel blockers | 25 (5) | 25 (4) |
| Aspirin and/or Clopidogrel | 50 (10) | 50 (8) |
| Statins | 25 (5) | 25 (4) |
| Oral antidiabetics | 25 (5) | 31 (5) |
ACEi: Angiotensin converting enzyme inhibitor, ARB: Angiotensin‐II receptor blocker, CABG: Coronary by‐pass surgery, MI: Acute myocardial infarction, PCI: Percutaneous coronary intervention.
Mean values of RR and QT in postdrug phase were slightly but significantly higher than predrug phase (RR: 845 ± 42 vs 816 ± 46, P < 0.05; QT: 371 ± 8 vs 361 ± 9, P < 0.05). In contrast, there was no statistically significant difference in the mean values of the QTo, J, and S between predrug and postdrug phases. The results of the Verda program are shown in Table 2. Similarly, QTVIs of the two study phases did not show any statistical difference (predrug: −0.874 ± 0.071 and postdrug: −0.997 ± 0.067, P = 0.109).
Table 2.
QT Dynamicity Parameters Obtained with the Verda Program (mean ± SEM). Values of RR and QT Were Higher in the Postdrug Phase than the Predrug Phase that Was Thought to Result from Prolonged Supine Position, but QTo and J Together with S of the QT/RR Plots Were Not Different in Each Phase of the Study
| Predrug | Postdrug | Mean Differences | P Value | |
|---|---|---|---|---|
| RR (ms) | 816 ± 46 | 845 ± 42 | 29 ± 16 | 0.041 |
| QT (ms) | 361 ± 9 | 371 ± 8 | 10 ± 2 | 0.005 |
| QTo (ms) | 408 ± 10 | 406 ± 8 | 2 ± 4 | 0.918 |
| J (Exponent) | 0.474 ± 0.030 | 0.433 ± 0.025 | 0.040 ± 0.028 | 0.179 |
| S (Slope) | 0.221 ± 0.020 | 0.198 ± 0.017 | 0.023 ± 0.014 | 0.148 |
DISCUSSION
Our study findings suggested that 50 mg oral sildenafil citrate administration did not cause any alteration in the cardiac repolarization dynamics in the patients with erectile dysfunction. Sildenafil did not change the QT/RR slope together with the corrected QT and J exponent of the correction formula. It did not induce any changes in QTVI as well. These findings support the conclusion that the use of sildenafil is safe for erectile dysfunction, and imply that the cardiac events associated with sildenafil may not be due to ventricular arrhythmias.
Our results are partly in disagreement with a previous work that uniquely investigated the effect of sildenafil QT dynamics and QTVI as a primary target. In their study, Piccirillo et al. 9 suggested that sildenafil induced an increase in both QT/RR slope and QTVI in patients with heart failure, but increased QTVI only in healthy control subjects. The explanation they gave for this kind of effect was that the heart rate increase induced by sildenafil resulted from a sympathetic drive augmentation to the heart rather than direct electrophysiological effects. In contrast, sildenafil did not cause an increase and even caused a decrease in the heart rate and this effect could be explained by prolonged rest position during post‐drug phase in our study in accordance with previous studies. 22 , 23 Also, Agelink et al. 24 did not find any effect of sildenafil on sympathovagal balance (low power/high power of power spectral heart rate variability) of the heart. However, the findings of Piccirillo et al. 9 on the effects of sildenafil on QT interval and QT dispersion are in agreement with the present study and previous work of our institution. 25
It should also be acknowledged that Piccirillo et al. used a 256‐beat segment of continuous electrocardiography recordings to calculate QT/RR slopes without performing any compensation or selection for RR and QT data. In contrast, our data were obtained from the whole 1‐hour period with RR compensation (Fig. 1), which significantly augments the correlation of the QT/RR relationship that was previously demonstrated. 17 In our study, the QT/RR correlation coefficients in the segments used to calculate the slope and the J exponent of QT/RR relationship were at least 0.80. Thus, we compared two more correlated QT/RR slopes of each study phase than Piccirillo et al. did, 9 and we suggest that this feature of our method may make our findings more reliable. In addition, not only we did find any effect of sildenafil on S but we also did not find any effect of sildenafil on the J exponent, another important determinant of QT/RR association. According to our knowledge, this is the first report using such a sensitive method and the one that demonstrates any effect of sildenafil on all aspects of QT dynamics.
Figure 1.
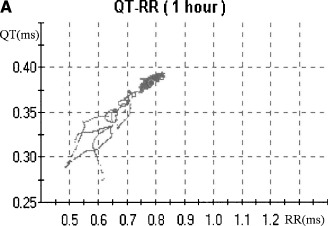
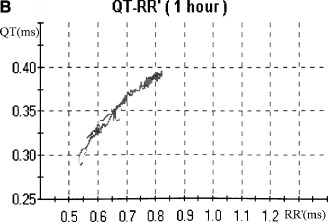
An example of uncompensated (1A) and compensated (1B) QT/RR plots representing QT lag phenomenon. In 1B, QT interval is plotted against the delayed RR interval (RR′), so, the correlation between QT and RR was improved.
The same considerations may be valid for QTVI interpretation. It is a well‐known finding that the variance of RR interval increases with the prolongation of the electrocardiography recording time. 26 This kind of relation may be true for even all intervals of the electrocardiography, so, any index calculated from the mean values and variances of the time intervals of longer recordings of electrocardiography may have more statistical significance than the shorter one. This issue is needed be further emphasized by future research investigating the effect of recording time on QTVI.
Controversies exist about the in vitro effect of sildenafil on cardiac repolarization. Gleen et al. 10 demonstrated that sildenafil prolonged cardiac repolarization the same as the class III antiarrhythmic drugs by blocking the rapid component of delayed rectifier potassium current at about 100‐fold higher concentrations in vitro than at the usual clinical oral dose of 25–100 mg. In contrast, Chiang et al. 11 found that sildenafil did not cause any prolongation of repolarization in therapeutic concentrations and even shortened repolarization by blocking L‐type Ca(2+) current in supra‐therapeutic concentrations. Moreover, dynamic QT analysis methods could detect even small changes of ventricular repolarization induced with single oral dofetilide administration, which is a true class III agent. 16 Thus, our findings imply that sildenafil does not induce any ventricular repolarization abnormalities in clinical conditions.
Our study once again suggests that sildenafil can be used for erectile dysfunction safely. It does not alter cardiac repolarization and this fact may imply that it does not possess any capacity to induce ventricular arrhythmias. These findings are in agreement with large randomized studies that sildenafil was not a cause for serious cardiac effects. 27 However, because some recommendations categorized patients to low, intermediate, and high cardiac risk for sexual activity, 28 care should be taken of patients' risk factors before starting an erectile dysfunction therapy rather than specially sildenafil use.
The dose of sildenafil citrate used may be considered as a limitation of the study. We investigated the effects of 50 mg sildenafil citrate on QT dynamicity but 100 mg or 200 mg may be needed for nonresponders in clinical practice. Although it was thought to be clinically not significant, 25–200 mg oral sildenafil administration causes about 2.1‐fold increases in systemic exposure for a doubling in dose 29 , so the effects of increased doses of sildenafil may be another issue for further researches. Same drawbacks should be kept in mind when sildenafil is coadministered with the drugs that are potent inhibitors of cytochrome P450 3A (e.g., erythromycin) because of the moderate increase in sildenafil plasma level. 30
CONCLUSION
Fifty milligrams of sildenafil citrate does not affect QT rate dependence, corrected QT, and the correction exponent. Our findings provide reliable information regarding this drug's safety. The cardiac events associated with sildenafil could not be explained with ventricular arrhythmias.
Acknowledgments
Acknowledgment: The authors thank Simon Auger and Metehan Firat for their technical assistance.
REFERENCES
- 1. Boolell M, Gepi‐Attee S, Gingell JC, et al Sildenafil, a novel effective oral therapy for male erectile dysfunction. Br J Urol 1996;78: 257–261. [DOI] [PubMed] [Google Scholar]
- 2. Goldstein I, Lue TF, Padma‐Nathan H, et al Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group. N Engl J Med 1998;338: 1397–1404. [DOI] [PubMed] [Google Scholar]
- 3. Feldman HA, Goldstein I, Hatzichristou DG, et al Impotence and its medical and psychosocial correlates: results of the Massachusetts Male Aging Study. J Urol 1994;151: 54–61. [DOI] [PubMed] [Google Scholar]
- 4. Feenstra J, Van Drie‐Pierik RJ, Lacle CF, et al Acute myocardial infarction associated with sildenafil. Lancet 1998;352: 957–958. [DOI] [PubMed] [Google Scholar]
- 5. Hayashi K, Minezaki KK, Narukawa M, et al Atrial fibrillation and continuous hypotension induced by sildenafil in an intermittent WPW syndrome patient. Jpn Heart J 1999;40: 827–830. [DOI] [PubMed] [Google Scholar]
- 6. Cheitlin MD, Hutter AM Jr, Brindis RG, et al Use of sildenafil (Viagra) in patients with cardiovascular disease. Technology and Practice Executive Committee. Circulation 1999;99: 168–177. [DOI] [PubMed] [Google Scholar]
- 7. Cheitlin MD, Hutter AM Jr, Brindis RG, et al ACC/AHA expert consensus document. Use of sildenafil (Viagra) in patients with cardiovascular disease. American College of Cardiology/American Heart Association. J Am Coll Cardiol 1999;33: 273–282. [DOI] [PubMed] [Google Scholar]
- 8. Phillips BG, Kato M, Pesek CA, et al Sympathetic activation by sildenafil. Circulation 2000;102: 3068–3073. [DOI] [PubMed] [Google Scholar]
- 9. Piccirillo G, Nocco M, Lionetti M, et al Effects of sildenafil citrate (Viagra) on cardiac repolarization and on autonomic control in subjects with chronic heart failure. Am Heart J 2002;143: 703–710. [DOI] [PubMed] [Google Scholar]
- 10. Geelen P, Drolet B, Rail J, et al Sildenafil (Viagra) prolongs cardiac repolarization by blocking the rapid component of the delayed rectifier potassium current. Circulation 2000;102: 275–277. [DOI] [PubMed] [Google Scholar]
- 11. Chiang CE, Luk HN, Wang TM, et al Effects of sildenafil on cardiac repolarization. Cardiovasc Res 2002;55: 290–299. [DOI] [PubMed] [Google Scholar]
- 12. Coumel P, Maison‐Blanche P, Badilini F. Dispersion of ventricular repolarization: Reality? Illusion? Significance Circulation 1998;97: 2491–2493. [DOI] [PubMed] [Google Scholar]
- 13. Hintze U, Vach W, Burchardt H, et al DIAMOND Study Group: QT interval dynamics predict mortality in high‐risk patients after myocardial infarction. Scand Cardiovasc J 2002;36: 276–281. [DOI] [PubMed] [Google Scholar]
- 14. Extramiana F, Neyroud N, Huikuri HV, et al QT interval and arrhythmic risk assessment after myocardial infarction. Am J Cardiol 1999;83: 266–269. [DOI] [PubMed] [Google Scholar]
- 15. Neyroud N, Maison‐Blanche P, Denjoy I, et al Diagnostic performance of QT interval variables from 24‐h electrocardiography in the long QT syndrome. Eur Heart J 1998;19: 158–165. [DOI] [PubMed] [Google Scholar]
- 16. Lande G, Maison‐Blanche P, Fayn J, et al Dynamic analysis of dofetilide‐induced changes in ventricular repolarization. Clin Pharmacol Ther 1998;64: 312–321. [DOI] [PubMed] [Google Scholar]
- 17. Lang CC, Flapan AD, Neilson JM. The impact of QT lag compensation on dynamic assessment of ventricular repolarization: Reproducibility and the impact of lead selection. Pacing Clin Electrophysiol 2001;24: 366–373. [DOI] [PubMed] [Google Scholar]
- 18. Milligan PA, Marshall SF, Karlsson MO. A population pharmacokinetic analysis of sildenafil citrate in patients with erectile dysfunction. Br J Clin Pharmacol 2002;53(Suppl. 1):45S–52S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Franz MR, Swerdlow CD, Liem LB, et al Cycle length dependence of human action potential duration in vivo. Effects of single extrastimuli, sudden sustained rate acceleration and deceleration, and different steady‐state frequencies. J Clin Invest 1988;82: 972–979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Lee SD, Dorian P, Geist M, et al Validation of a noninvasive measure of local myocardial repolarization in a conscious human model: Adaptation of repolarization to changes in rate. J Cardiovasc Electrophysiol 1999;10: 1171–1179. [DOI] [PubMed] [Google Scholar]
- 21. Berger RD, Kasper EK, Baughman KL, et al Beat‐to‐beat QT interval variability: Novel evidence for repolarization lability in ischemic and nonischemic dilated cardiomyopathy. Circulation 1997;96: 1557–1565. [DOI] [PubMed] [Google Scholar]
- 22. Jackson G, Benjamin N, Jackson N, et al Effects of sildenafil citrate on human hemodynamics. Am J Cardiol 1999;83: 13C–20C. [DOI] [PubMed] [Google Scholar]
- 23. Arruda‐Olson AM, Mahoney DW, Nehra A, et al Cardiovascular effects of sildenafil during exercise in men with known or probable coronary artery disease: A randomized crossover trial. JAMA 2002;287: 719–925. [DOI] [PubMed] [Google Scholar]
- 24. Agelink MW, Ullrich H, Brockmeyer NH. Sildenafil does not influence autonomic neurocardiac control assessed by standard measurements of heart rate variability. Circulation 2001;104: E145. [PubMed] [Google Scholar]
- 25. Alpaslan M, Onrat E, Samli M, et al Sildenafil citrate does not affect QT intervals and QT dispersion: An important observation for drug safety. Ann Noninvasive Electrocardiol 2003;8: 14–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Heart rate variability: Standards of measurement, physiological interpretation and clinical use . Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996;93: 1043–1065. [PubMed] [Google Scholar]
- 27. Sadovsky R, Miller T, Moskowitz M, et al Three‐year update of sildenafil citrate (Viagra) efficacy and safety. Int J Clin Pract 2001;55: 115–128. [PubMed] [Google Scholar]
- 28. DeBusk R, Drory Y, Goldstein I, et al Management of sexual dysfunction in patients with cardiovascular disease: Recommendations of The Princeton Consensus Panel. Am J Cardiol 2000;86: 175–181. [DOI] [PubMed] [Google Scholar]
- 29. Nichols DJ, Muirhead GJ, Harness JA. Pharmacokinetics of sildenafil after single oral doses in healthy male subjects: Absolute bioavailability, food effects and dose proportionality. Br J Clin Pharmacol 2002;53(Suppl. 1):5S–12S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Muirhead GJ, Faulkner S, Harness JA, et al The effects of steady‐state erythromycin and azithromycin on the pharmacokinetics of sildenafil in healthy volunteers. Br J Clin Pharmacol 2002;53(Suppl. 1):37S–43S. [DOI] [PMC free article] [PubMed] [Google Scholar]