

Abstract
Background: The electrocardiogram (ECG) remains a simple, universally available, and prognostically powerful investigation in heart failure, and acute coronary syndromes. We sought to assess the prognostic utility of clinical, angiographic, and simple ECG parameters in a large cohort of patients undergoing elective cardiac catheterization (CC) for known or suspected coronary artery disease.
Methods: Consecutive consenting patients undergoing CC for coronary disease were enrolled at a single tertiary center. Patient data, drug therapy, catheter reports, and ECG recordings were prospectively recorded in a validated electronic archive. The primary outcome measure was death or nonfatal myocardial infarction (MI) over 1 year or until percutaneous or cardiac surgical intervention. Independent prognostic markers were identified using the Cox proportional hazard model.
Results: A total of 682 individuals were recruited of whom 17(2.5%) died or suffered a nonfatal MI in 1 year. In multivariate analysis QRS duration (ms) (HR 1.03 95% CI 1.01–1.05, P = 0.003), extent of coronary disease (HR 2.01 95% CI 1.24–3.58, P = 0.006), and prolonged corrected QT peak interval in lead I (HR 1.02 95% CI 1.00–1.03, P = 0.044) were independently associated with death or nonfatal MI. Receiver‐operator characteristic (ROC) analysis for the multivariate model against the primary end point yielded an area under the curve of 0.759 (95% CI 0.660–0.858), P < 0.001.
Conclusions: QRS duration and QT peak are independently associated with increased risk of death or nonfatal MI in stable patients attending for coronary angiography.
Keywords: QRS duration, myocardial infarction, electrocardiography, mortality
The 12‐lead ECG is a simple, inexpensive, and widely available diagnostic tool able to provide significant information on both cardiac structure and its electrical properties. Many ECG parameters have been investigated for their potential prognostic value with particular interest centered on abnormalities in depolarization such as QRS prolongation and ECG features associated with altered repolarization.
QRS prolongation denotes delayed propagation of myocardial depolarization that both promotes ventricular arrhythmias and often reflects significant structural cardiac defects. QRS prolongation has been associated with adverse outcome in individuals presenting with acute‐ST‐elevation myocardial infarction, 1 , 2 , 3 non‐ST‐elevation myocardial infarction, 4 and those with evidence of left ventricular dysfunction. 5 , 6 However, the prognostic value of QRS prolongation for patients with stable coronary artery disease without significant left ventricular dysfunction has not been established.
Uncoordinated myocardial repolarization has been demonstrated to provide a substrate for reentry arrhythmia 7 and QT segment prolongation has been associated with adverse outcome for patients with chronic heart failure, 8 following myocardial infarction, 9 in diabetic patients 10 and in apparently normal individuals. 11 At present there is no clear consensus of the correct methodology for detecting repolarization abnormalities in the standard 12‐lead ECG. Although measurement of the entire QT interval provides useful information on total repolarization, difficulties in defining the end of the T wave have provided potential sources of error. This issue can be addressed by the use of the QT peak interval as an alternative measure of repolarization (onset of the Q wave to the maximum amplitude of the T wave; QTp interval).
The aim of this study was to determine the significance of prolonged QRS duration and corrected QT peak in predicting of all‐cause mortality or nonfatal MI in elective patients undergoing coronary angiography for known or suspected coronary artery disease.
METHODS
Patient recruitment and data collection was carried out at the Cardiothoracic Centre, Liverpool (UK), between September 2001 and January 2003. The Royal Liverpool and Broadgreen University hospital ethical committee approved the research protocol. All patients gave informed written consent. Consenting patients attending the cardiology day ward for elective diagnostic cardiac catheterization for known or suspected coronary artery disease and in sinus rhythm were included in the study. We excluded patients with atrial fibrillation, atrial flutter, preexcitation, paced rhythm, and any sustained arrhythmia. Also patients with acute ST‐elevation‐myocardial infarction [STEMI], acute non‐ST‐elevation myocardial infarction [NSTEMI] and cardiogenic shock were excluded. They had a 12‐lead electrocardiogram (ECG) recorded and underwent coronary angiography with left ventricular ejection fraction estimated by invasive ventriculography. Stenoses were deemed significant if the luminal obstruction was greater than 50%. The extent of coronary artery disease was defined as the number of coronary vessels with greater than 50% stenoses. Patients were excluded in the presence of sustained arrhythmia. Patients were followed over 1 year by structured telephone interviews, mailed questionnaires, and hospital case records review. Patient records were linked to the National Strategic Tracing Service (NSTS), which records all‐cause mortality in the UK, to establish the current vital status. Patients were matched to the NSTS based on patient name, National Health Service number, date of birth, gender, and postcode.
Electrocardiographic Analysis
Twelve‐lead electrocardiography was performed in resting supine position, using General Electric Medical Systems at 25 mm/s and 1mv/cm standardization. An experienced cardiologist blinded to the clinical and the outcome data reviewed the admission ECGs of all the patients. ECGs were interpreted using standard criteria 12 and all standard ECG variables including QT peak 13 were recorded. The widest QRS duration in the standard leads was manually measured using hand held calipers. QTp in lead I was corrected for heart rate (HR) using Bazzett's equation. QT peak was measured in lead I in line with standard methodology. 14 , 15 , 16 , 17
Statistical Analysis
Continuous variables were reported as mean ± SD. Categorical variables were summarized as percentages. Associations between clinical, angiographic, electrocardiographic variables, and death or nonfatal myocardial infarction prior to cardiac intervention were determined by a Cox proportional hazards regression model with a forward stepwise approach. Variables offered to the model were age, left ventricular ejection fraction, extent of coronary disease, QRS duration, and HR corrected QT peak. Survival from the time of presentation was estimated by Kaplan‐Meier method. Probability values < 0.05 were considered to indicate statistical significance.
Receiver‐operator characteristic (ROC) analysis was used to assess the prognostic utility of each electrocardiographic variable and the multivariate model including angiographically determined burden of disease. An area under the ROC curve of 0.5 indicates that the test results are no better than those obtained by chance whereas an area of 1.0 denotes a perfectly sensitive and specific test. All none normally distributed data were dichotomized.
End Points
The primary outcome measure was defined as a composite of all‐cause mortality or nonfatal myocardial infarction (MI) over 1 year or until percutaneous or cardiac surgical intervention.
RESULTS
Six hundred eighty‐two consecutive consenting patients attending the Cardiothoracic Centre, Liverpool for elective cardiac catheterization from September 2001 to January 2003 were recruited into the study. They were being investigated for suspected coronary artery disease. 80.7% of the study population had stable coronary disease, 10.4% had had a hospital admission within 2 months for acute coronary syndrome, and 8.9% had valvular heart disease. We had 4.0% of patients with LBBB and 3.4% of patients with RBBB as baseline conduction abnormality. QRS axis was not offered to the Cox model as the a priori hypothesis was to compare age, LV function, extent of coronary disease, QRS duration, and QT peak with outcome. The characteristics of these patients are detailed in Table 1. During the mean follow‐up period of 278 days 17 deaths or nonfatal MI occurred, representing 2.5% of the study population.
Table 1.
Patient Characteristics (n = 682)
| Variable | Mean ± SD |
|---|---|
| Age in years | 60.7(±9.6) |
| Male | 66.5% |
| Prior MI | 33.6% |
| Prior CABG | 4.6% |
| Prior PCI | 6.8% |
| Prior CVA/TIA | 6.8% |
| Aspirin | 80.7% |
| Statin | 70.7% |
| Beta‐blocker | 60.3% |
| ACE inhibitor | 31.3% |
| No. coronary stenosis >50% | 34.1% |
| One vessel disease | 23.5% |
| Two vessel disease | 21.3% |
| Three vessel disease | 21.1 |
| LV ejection fraction | 60.3 ± 12% |
| QRS duration | 97.3 ± 18.2% |
| QT peak lead I(ms) | 342 ± 31.5% |
CABG = coronary artery bypass grafting; CVA = cerebrovascular accident; LV = left ventricle; PCI = percutaneous coronary intervention; TIA = transient ischemic attack.
All Cause Mortality and Nonfatal Myocardial Infarction
The univariate association between a range of ECG markers and outcome was assessed by Cox regression. This analysis yielded QRS duration and HR corrected QT peak interval in lead I as potential independent prognostic indicators. Multivariable Cox regression analysis was then performed to establish that QRS duration and corrected QT peak interval in lead I were associated with death or nonfatal MI independent of the major clinical prognostic markers; age, left ventricular ejection fraction, and angiographic extent of coronary disease. The results of this analysis are given in Table 2. The independent predictors of all cause mortality or nonfatal MI were: QRS duration per ms (HR 1.03 95% CI 1.01–1.05, P = 0.003), extent of coronary disease (HR 2.01 95% CI 1.24–3.58, P = 0.006), and prolonged corrected QT peak interval in lead I per ms (HR 1.02 95% CI 1.00–1.03, P = 0.044). The HR refers to each ms increase for QRS duration above and below 110 ms.
Table 2.
Cox Multivariate Regression Analysis for Death or Nonfatal MI
| Hazard ratio HR | Confidence interval 95% | Significance (P) | |
|---|---|---|---|
| Age (years) | 0.97 | 0.91–1.03 | 0.314 |
| Number of vessels with >50% stenosis | 2.10 | 1.24–3.58 | 0.006 |
| Left ventricular ejection fraction (%) | 1.01 | 0.97–1.06 | 0.472 |
| QRS duration (ms) | 1.03 | 1.01–1.05 | 0.003 |
| QT peak interval in lead I (ms) | 1.02 | 1.00–1.03 | 0.044 |
The Kaplan‐Meier curves estimated survival for patients with QRS durations dichotomized into greater or less than 110 ms are displayed in Figure 1. The QRS durations were dichotomized in steps of 10 ms and the strongest association between QRS duration and adverse outcomes was for the dichotomy above and below 110 ms. The Kaplan‐Meier curves estimated survival for patients with corrected QT peak interval dichotomized into greater or less than the median (341 ms) are displayed in Figure 2.
Figure 1.

Kaplan‐Meier survival curves indicating freedom from death or nonfatal MI for patients with QRS duration < or > 110 ms.
Figure 2.

Kaplan‐Meier curves for freedom from death or MI for patients above or below median QT peak interval (341 ms).
Figure 3 shows the receiver operator curves for each of the independent predictor variables taken alone against death or nonfatal MI.
Figure 3.

Receptor‐operator characteristic curves for extent of coronary disease, QRS duration, and QT Peak interval predicting death or nonfatal MI.
ROC analysis demonstrated a significant area under the curve for QRS duration alone of 0.66 (95% CI 0.50–0.81), P = 0.028 against the composite of all cause mortality/nonfatal MI. Similarly, the ROC characteristic for corrected QT peak interval in lead I against death or nonfatal MI was 0.68 (95% CI 0.58–0.79), P = 0.009, and the ROC characteristic for the extent of coronary disease was 0.67 (95% CI 0.54–0.81), P = 0.014. The ROC characteristic of the Cox regression model including extent of coronary disease, QRS duration, and corrected QT peak interval in lead I was 0.76 (95% CI 0.66–0.86), P < 0.001 (See Fig. 4).
Figure 4.
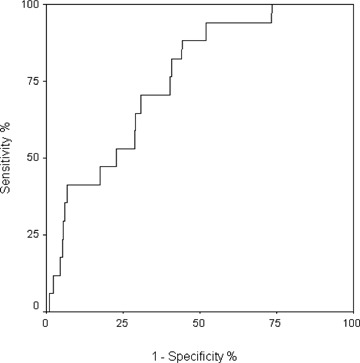
Receiver‐operator characteristic curve for the multivariate regression model including extent of coronary disease, QRS duration, and QT peak interval predicting death or nonfatal MI.
DISCUSSION
In this study, QRS duration and rate‐corrected QT peak were associated with death or nonfatal MI independent of age, significant coronary artery disease, and left ventricular ejection fraction, factors that have previously been demonstrated to be powerful predictors of adverse outcome in this patient group. 18 Our findings also corroborate with and extend previous studies that have demonstrated the prognostic power of these ECG parameters in other patient populations which included patients suffering from acute STEMI, NSTEMI, and those with evidence of left ventricular dysfunction.
QRS Interval and Survival
The slowed and heterogeneous conduction within increased mass of ventricular myocardium observed in the presence of a prolonged QRS duration will lead to an increased likelihood of reentrant ventricular arrhythmia. 19 Inducibility of sustained ventricular tachycardia has been shown to be easier in patients with wide QRS complexes 20 and a recent study demonstrated that prolonged QRS duration on surface ECG is a strong independent predictor of sustained monomorphic ventricular tachycardia. 21 It is therefore possible that the association between QRS duration and mortality in this study may be secondary to an association with arrhythmic death, although we did not clarify the mode of death in this study. Previous studies have also shown prolonged QRS duration to be an important predictive variable for sudden death in survivors of myocardial infarction 22 with individuals with increased QRS duration more likely to have evidence of increased left ventricular mass, 23 myocardial fibrosis, 23 larger areas of myocardial necrosis, 24 and ischemic involvement of the conduction tissue. 25 In our study, approximately a third of subjects had suffered a previous MI and for these individuals a prolonged QRS duration may indicate more significant infarction‐related myocardial impairment likely to place them at greater risk of future adverse events.
Prolonged QRS duration is due to delayed ventricular electrical activation that may result in mechanical dyssynchrony 26 with impairment of hemodynamic performance and mitral regurgitation. 27 Although left ventricular function was controlled by multivariate analysis in this study, it remains possible that subtle alterations in contractile function through dyssynchrony could be implicated in promoting adverse outcome. Previous studies have demonstrated that acute ischemia provokes widening of the QRS complex during exercise 28 and temporary balloon occlusion of coronary arteries during percutaneous coronary intervention. 29 Though QRS duration under unstressed conditions is not a marker for ischemia, post‐MI studies have shown an association between QRS prolongation and subsequent reinfarction suggesting that this ECG marker may be an indicator of vulnerable myocardium. 3
QT Peak Interval and Survival
The adverse prognostic power of a prolonged QTc interval has been demonstrated in the majority of population‐based trials 30 , 31 with conflicting results likely to represent imprecision in measurement of QTc interval. Prolongation of the QTc interval has been demonstrated to be associated with aging, arterial hypertension, underlying coronary artery disease, and ECG‐estimated left ventricular mass in previous studies. 32 It is likely that the prognostic importance of prolongation of the corrected QTp interval in this study probably reflects structural cardiac abnormalities that promote adverse events particularly related to cardiac arrhythmia. The QTc interval is also determined by cardiac autonomic activity 33 with a prolonged QTc interval associated with sudden cardiac death in diabetic patients with abnormal autonomic function. 34
Limitations
The major limitation of this study is relatively small number of primary endpoint events occurring during the initial 1‐year follow‐up. In addition, follow‐up of this cohort of patients at 5 years, at present underway, should provide for a more detailed assessment of the associations discussed.
CONCLUSION
QRS duration and corrected QT peak demonstrated a significant association with mortality or nonfatal myocardial infarction independent of age, LV function, and extent of coronary artery disease among stable patients attending for coronary angiography.
Funding: none
Conflict of interest: none
REFERENCES
- 1. Go AS, Barron HV, Rundle AC, et al Bundle‐branch block and in‐hospital mortality in acute myocardial infraction. National registry of myocardial infarction 2 investigators. Ann Intern Med 1998;129:690–697. [DOI] [PubMed] [Google Scholar]
- 2. Melgarejo‐Moreno A, Galcera‐Tomas J, Garcia‐Alberola A, et al Incidence, clinical characteristics, and prognostic significance of right bundle‐branch block in acute myocardial infraction. Circulation 1997;96:1139–1144. [DOI] [PubMed] [Google Scholar]
- 3. Bauer A, Watanabe MA, Barthel P, et al QRS duration and late mortality in unselected post‐infarction patients of the revascularization era. Eur Heart J 2006;27:427–433. [DOI] [PubMed] [Google Scholar]
- 4. Brilakis E, Mavrogiorgos N, Kopecky S, et al Usefulness of QRS duration in the absence of bundle branch block as an early predictor of survival in non‐ST elevation myocardial infarction. Am J Cardiol 2002;89:1013–1018. [DOI] [PubMed] [Google Scholar]
- 5. Silvet H, Amin J, Padmanabhan S, et al Prognostic implications of prolonged QRS duration in patients with moderate and severe left ventricular systolic impairment. Am J Cardiol 2001;88:182–185. [DOI] [PubMed] [Google Scholar]
- 6. Iuliano S, Fisher S, Karasik P, et al Department of veterans affairs survival trial of antiarrhythmic therapy in patients with congestive heart failure. Am Heart J 2002;143:1085–1091. [DOI] [PubMed] [Google Scholar]
- 7. Han J, Moe GK. Non‐uniform recovery of excitable tissue in ventricular muscle. Circulation Research 1964;14:14. [DOI] [PubMed] [Google Scholar]
- 8. Vrtovec B, Delgado R, Zewail A, et al Prolonged QTc interval and high B‐type natriuretic peptide levels together predict mortality in patients with advanced heart failure. Circulation 2003;107:1764–1769. [DOI] [PubMed] [Google Scholar]
- 9. Peters RW, Byington RP, Barker A, et al Prognostic value of prolonged ventricular repolarization following myocardial infarction: The BHAT experience: The BHAT study group. J Clin Epidemiol 1990;43:167–172. [DOI] [PubMed] [Google Scholar]
- 10. Rossing P, Breum L, Major‐Pedersen A, et al Prolonged QTc interval predicts mortality in patients with type I diabetes mellitus. Diabet Med 2001;18:199–205. [DOI] [PubMed] [Google Scholar]
- 11. Schouten EG, Dekker JM, Meppelink P, et al QT interval prolongation predicts cardiovascular mortality in an apparently healthy population. Circulation 1991;84:1516–1523. [DOI] [PubMed] [Google Scholar]
- 12. Wagner GS. Interpretation of the normal electrocardiogram In Wagner GS. (ed.): Marriott's Practical Electrocardiography, 9th Edition, New Delhi , India . Williams & Wilkins B.I.Waverly, 1994, pp. 37–57. [Google Scholar]
- 13. Saveileva I, Yap YG, Guo X, et al Comparative reproducibility of QT, QT peak, and T peak T intervals in normal subjects, patients with myocardial infarction, and with hypertensive cardiomyopathy. Pacing Clin Electrophysiol 1998;21:2376–2381. [DOI] [PubMed] [Google Scholar]
- 14. Wong KYK, Lim PO, Wong SY, et al Does a prolonged QT peak identify left ventricular hypertrophy in hypertension? Int J Cardiol 2003;89:179–186. [DOI] [PubMed] [Google Scholar]
- 15. Velavan P, Wong KY, Ball JB. Evaluation of a novel technique to detect left ventricular hypertrophy on the surface electrocardiogram QT peak. Circulation 2004;110 (Suppl):III–580. [Google Scholar]
- 16. Wong KYK, McSwiggan S, Kennedy NSJ, et al QT peak prolongation may reflect inducible myocardial ischaemia. Heart 2005;91 (Suppl. I):A47. [Google Scholar]
- 17. Wong KYK, MacWalter RS, Douglas D, et al Long QT peak measured from a single ECG lead predicts cardiac death and all‐cause mortality. Heart 2006;92 (Suppl. II):A77. [Google Scholar]
- 18. Mock MB, Ringqvist I, Fisher LD, et al Survival of medically treated patients in the Coronary Artery Surgery Study (CASS) registry. Circulation 1982;66:562–568. [DOI] [PubMed] [Google Scholar]
- 19. Watanabe MA, Fenton FH, Evans SJ, et al Mechanisms for discordant alternans. J Cardiovasc Electrophysiol 2001;12:196–206. [DOI] [PubMed] [Google Scholar]
- 20. Brembilla‐Perrot B. Correlation between inducibility of sustained ventricular tachycardia and QRS duration. Eur Heart J 1994;15:26–31. [DOI] [PubMed] [Google Scholar]
- 21. Horwich T, Lee S, Saxon L. Usefulness of QRS prolongation in predicting risk of inducible monomorphic ventricular tachycardia in patients referred for electrophysiologic studies. Am J Cardiol 2003;92:804–809. [DOI] [PubMed] [Google Scholar]
- 22. Jordeans L, Tavernier R. and the MIRRACLE Investigators . Determinants of sudden death after discharge from hospital for myocardial infarction in the thrombolytic era. Eur Heart J 2000;22:1214–1225. [DOI] [PubMed] [Google Scholar]
- 23. Okin PM, Roman MJ, Devereux RB, et al Electrocardiographic identification of increased left ventricular mass by simple voltage‐duration products. J Am Coll Cardiol 1995;25:417–423. [DOI] [PubMed] [Google Scholar]
- 24. Rabkin SW. Relationship of various QRS indices to SGOT levels in acute anterior myocardial infarction. Acta Cardiol 1977;32:295–303. [PubMed] [Google Scholar]
- 25. Sherisan DJ, Culling W, Penny WJ. Electrophysiological disturbances associated with acute myocardial infarction. Eur Heart J 1986;7:Suppl. B:11–18. [DOI] [PubMed] [Google Scholar]
- 26. Kass DA, Chen CH, Curry C, et al Improved left ventricular mechanics from acute VDD pacing in patients with dilated cardiomyopathy and ventricular conduction delay. Circulation 1999;99:1567–1573. [DOI] [PubMed] [Google Scholar]
- 27. Bramlet DA, Morris KG, Coleman RE, et al Effect of rate‐dependent left bundle branch block on global and regional left ventricular function. Circulation 1983;67:1059–1065. [DOI] [PubMed] [Google Scholar]
- 28. Michaelides A, Ryan JM, VanFossen D, et al Exercise induced QRS prolongation in patients with coronary artery disease: A marker of myocardial ischaemia. Am Heart J 1993;126:1320–1325. [DOI] [PubMed] [Google Scholar]
- 29. Cantor AA, Goldfarb B, Ilia R. QRS prolongation: A sensitive marker of ischemia during percutaneous transluminal angioplasty. Catheter Cardiovasc Interventions 2000;50:177–183. [DOI] [PubMed] [Google Scholar]
- 30. Goldberg RJ, Bengtson J, Chen ZY, et al Duration of the QT interval and total and cardiovascular mortality in healthy persons (The Framingham Heart Study experience). Am J Cardiol 1991;67:55–58. [DOI] [PubMed] [Google Scholar]
- 31. Bednar MM, Harrigan EP, Anziano RJ, et al The QT interval. Prog Cardiovasc Dis 2001;43:1–45. [DOI] [PubMed] [Google Scholar]
- 32. Rautaharju PM, Manolio TA, Psaty BM, et al for the cardiovascular Health Study Collaborative Research Group . Correlates of QT prolongation in older adults (the Cardiovascular Health Study). Am J Cardiol 1994;73:999–1002. [DOI] [PubMed] [Google Scholar]
- 33. Rosen MR, Jeck CD, Steinberg SF. Autonomic modulation of cellular repolarization and of the electrocardiographic QT interval. J Cardiovasc Electrophysiol 1992;3:487–499. [Google Scholar]
- 34. Ewing DJ, Neilsson JM. QT interval length and diabetic autonomic neuropathy. Diabet. Med 1990;7:23–26. [DOI] [PubMed] [Google Scholar]