

Abstract
Background:
This study was conducted to evaluate the clinical outcomes of the acromioclavicular joint (ACJ) fixation with hook plate (HP) and continuous loop double endobutton fixation (CLDE) in the treatment of acute ACJ dislocation.
Methods:
This retrospective study was conducted on eight patients with HP and nine patients with CLDE fixations for acute ACJ dislocations. The subjects were evaluated by various criteria, including disabilities of the Arm, Shoulder, and Hand (DASH), American Shoulder and Elbow Surgeons Standardized Shoulder Assessment (ASES), University of California, Los Angeles (UCLA) shoulder rating scale, Shoulder Constant score, Simple Shoulder Test (SST), and coracoclavicular (CC) distance.
Results:
The differences between the mean scores of the visual analog scale for pain, DASH, ASES, UCLA shoulder rating scale, and Shoulder Constant, and SST were statistically significant in favor of the CLDE group. Mean difference of CC distance was 8.6±0.9 mm in the HP group; however, it was 11.6±1.2 mm in the CLDE group. The operation time was shorter in the HP fixation, compared to that in the CLDE fixation (51±13.3 versus 105±9.7 min; P<0.001 and P=0.008). There were six concomitant subacromial erosions and osteoarthritis in the ACJ of the HP group.
Conclusion:
The CLDE fixation was reported with better clinical outcomes than HP fixation; however, it was a technically demanding procedure. The HP maintained the CC distance better than CLDE with a technically easy application. The HP requires a second surgery for the removal and development of subacromial erosion and osteoarthritis of the ACJ that can be regarded as major concerns.
Key Words: Acromioclavicular dislocation, Closed-loop, Double endobutton, Hook plate
Introduction
The acromioclavicular joint (ACJ) represents the link between the clavicle and scapula that is responsible for the synchronized dynamics of the shoulder girdle (1). The ACJ dislocation with a prevalence of 9-12% is a common shoulder girdle injury in active young adults (1, 2). The ACJ dislocation is associated with acromioclavicular (AC) and coracoclavicular (CC) ligaments injuries. Rockwood classified ACJ dislocations into types I to VI based on the amounts of horizontal and vertical displacement of the lateral clavicle and CC distance (3).
Results of biomechanical studies have demonstrated the importance of anatomical reconstruction of the AC and CC ligaments in cases of unstable ACJ injuries. The change in the anatomical orientation of the scapula in unstable ACJ dislocations may lead to scapular dyskinesis in 70% of the patients who were treated with nonsurgical methods. Moreover, 45% of patients may present with sick scapula syndrome, including scapular malposition, inferior medial scapular winging, coracoid tenderness, and scapular dyskinesis. Scapular dyskinesis changes the dynamics of the rotator cuff that can predispose to chronic shoulder pain (4-7).
Nonoperative treatments have been generally accepted as the gold standard of treatment in Rockwood I and II lesions; however, the treatment of grade III is controversial and individualized. The ACJ dislocations grades IV-VI generally require operative treatment. There is no gold standard treatment for ACJ dislocations type III and more severe types. According to the literature, there are nonhomogeneous comparative studies between the treatments of ACJ dislocations type III and more severe types (8-23).
The aim of this study was to compare the clinical and radiographic results of acute Rockwood type III and more severe ACJ dislocations treated with either rigid trans-articular hook plate (HP) or non-rigid extra-articular with continuous loop double endobutton (CLDE) fixations. Hypothesis of this study was that the clinical results of HP and CLDE CC fixations for acute ACJ dislocations revealed equal functional and radiographic outcomes.
Materials and Methods
In this retrospective study, young athlete patients with ACJ dislocation candidates for surgery were treated with CLDE or HP fixations between March 2013 and March 2017. The CLDE or HP fixations were offered and performed on 22 physically active high-demand adult subjects due to Rockwood type III and IV ACJ dislocations. A total of 20 patients were estimated based on Minitab statistical software (version 13), according to a previous study with a power of 80% and 0.7 sigma (22). The subjects with previous shoulder injury or surgery, congenital deformity in the upper limb, neuromuscular disorder, and Rockwood type I and II ACJ dislocations were excluded from the present study.
The lesions were the results of road traffic accidents in 12 patients (54.5%) and falling on the affected shoulder in 10 patients (45.5%). The ACJ dislocations were evaluated by a standard anteroposterior radiograph of the shoulder and Zanca view. At the final follow-up, the vertical distance between the inferior border of the clavicle and superior border of the coracoid (i.e., CC distance) was measured in millimeter (mm) in both groups. Increase in CC distance by 50-100% and higher than 100% with respect to the contralateral side was considered as subluxation and redislocation, respectively. All the patients had a minimum of 6 months follow-up. This study was approved by the Ethics Committee of Urmia University of Medical Sciences, Urmia, Iran.
A total of 12 patients (11 males and 1 female) with the mean age of 37±12.2 years underwent CLDE CC fixations. The mean follow-up period was reported as 19.8±8.8 months (follow-up period range: 6-36 months). In the present study, the open technique was used as described by Struh (5). An auxiliary No. 5 Ethibond suture (Ethicon®) replicating the course of the trapezoid ligament was tied. The AC capsule and deltotrapezial fascia were imbricated to augment the endobutton construct.
In one of the patients, reduction immediately lost after the surgery due to fracture at the base of the coracoid. The subject was treated with an HP and evaluated in the HP group. At the final follow-up, ACJ was redislocated in two patients due to the displacement of the clavicular and coracoid buttons [Figure 1]. The patients declined further surgery; therefore, these three subjects were excluded, and finally nine patients remained in this group.
Figure 1.

Redislocation of acromioclavicular joint due to the failure of continuous loop double endobutton fixation at the clavicular button
In this study, 11 cases (10 males and one female) with the mean age of 38.1±14.7 years were treated with HP CC fixation. One patient was transferred from the CLDE group to this group. The mean follow-up period was 23.8±12.9 months (follow-up period range: 6-38 months). The fixation failed in one patient with morbid obesity, and he declined further surgery [Figure 2].
Figure 2.
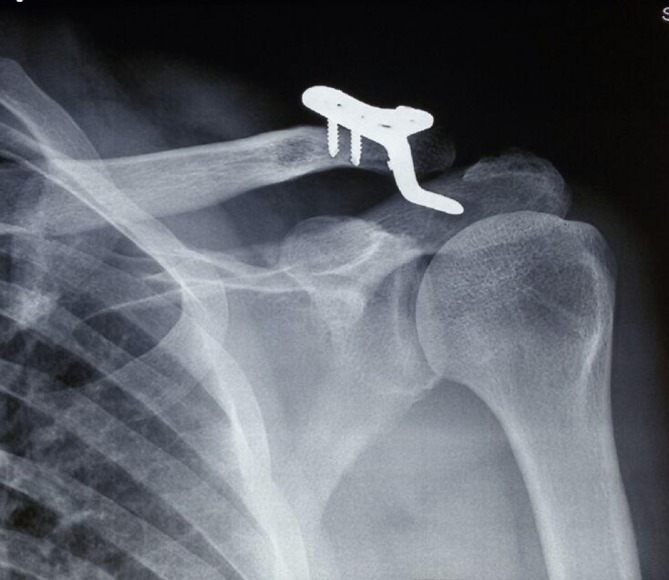
Redislocation of acromioclavicular joint with hook plate
One patient was lost during the follow-up, and one subject declined to remove the HP. It was offered to remove the HPs at 3 months postsurgery; however, due to patients’ preferences, HPs were removed in 10.7±4.8 months in eight cases. The subjects were evaluated after the HP removal within a period of 2 months on average. This group consisted of eight patients. Presence of subacromial erosion, osteoarthritis, and other probable adverse effects of HP was evaluated in this group.
Table 1 tabulates the characteristics of the two groups of patients. There was no significant difference between age, gender, Rockwood type of ACJ dislocation, shoulder side (e.g., right or left), and interval between the injury, surgery, and follow-up. A significant difference was observed between the mean values of operation time in the two groups (P=0.008). The patients were subjectively evaluated using the visual analog scale (VAS) for pain (0: no pain, 10: worst possible pain), disabilities of the Arm, Shoulder, and Hand (DASH) score (0: no disability, 100: disabled), and American Shoulder and Elbow Surgeons Standardized Shoulder Assessment (ASES) (100: best score, 0: worst score).
Table 1.
Characteristics of eight patients with hook plate coracoclavicular fixation and nine subjects with continuous loop double endobutton coracoclavicular fixation
| Variable | Hook plate (n=8) | Continuous loop double endobutton (n=9) | P-value (test) |
|---|---|---|---|
| Age (year) | 39.6±16.2 | 37.3±12.02 | 0.6 (Man-Whitney U test) |
| Gender | 7 males/1 female | 8 males/1 female | 0.2 (Fisher’s exact test) |
| Rockwood type of acromioclavicular joint dislocation | 7 cases with type III/1 case with type IV | 8 cases with type III/case with type IV | 0.8 (Fisher’s exact test) |
| Side | 6 right/2 left | 4 right/5 left | 0.2 (Fisher’s exact test) |
| Interval between injury and surgery (day) | 8.2±3.9 | 9.05±3.6 | 0.6 (Man-Whitney U test) |
| Operation time (min) | 51±13.2 | 105±9.7 | 0.008 (Man-Whitney U test) |
| Follow-up (month) | 19.8±8.8 | 23.8±19.2 | 0.08 (Man-Whitney U test) |
In addition, the patients were subjectively and objectively evaluated with the University of California, Los Angeles (UCLA) shoulder rating scale (score range: 0-35; Good/Excellent > 27, Fair/Poor < 27), Shoulder Constant score (100: no pain, 0: maximum pain), and Simple Shoulder Test (SST) (12: best score, 0: worst score). The mean CC distances (mm) between the two groups were compared at the latest follow-up. This study was conducted under the supervision of the Ethics Committee of Urmia University of Medical Sciences with the code of 96-09-63-3041. Written consent was obtained from all the patients, and the subjects were free to participate.
Frequency and percentage were used to characterize the qualitative variables; however, the mean±standard deviation and range of variations were employed for quantitative variables. To conduct inferential analysis, Fisher’s exact test was utilized to compare the qualitative variables, and the nonparametric Mann-Whitney U test was applied for quantitative variables. P-value less than 1% was considered statistically significant.
Results
As earlier noted, 3 (27%) out of 11 and 1 (9%) out of 11 patients in the CLDE and HP groups failed the surgery, respectively; therefore, they were excluded from the study. Table 2 tabulates the mean scores of the instruments in both groups. The differences between the mean VAS scores of pain, DASH, ASES, UCLA shoulder rating scale, Shoulder Constant, and SST were statistically significant in favor of the CLDE group. Mean difference of CC distance was in favor of HP fixation. In the HP group, 6 (75%) out of 8 patients had concomitant subacromial erosions and osteoarthritis of the ACJ [Figure 3].
Table 2.
Scores of the different shoulder functional instruments of eight patients with hook plate and nine subjects with continuous loop double endobutton fixations
| Variable |
Hook plate
(n=8) |
Continuous loop double endobutton
(n=9) |
P-value
(Man-Whitney U test) |
|---|---|---|---|
| VAS score (0: no pain, 10: worst possible pain) |
7.6±9.5 | 3.2±8.9 | 0.001 (Man-Whitney U test) |
| DASH score (0: no disability, 100: disabled) |
73.1±22.1 | 39.4±11.02 | 0.008 (Man-Whitney U test) |
| ASES (100: best score, 0: worst score) |
47.9±27.4 | 87.6±10.4 | 0.007 (Man-Whitney U test) |
| UCLA shoulder rating scale (score range: 0-35; Good/Excellent > 27, Fair/Poor < 27) |
21±7.03 | 32.2±1.4 | 0.006 (Man-Whitney U test) |
| Shoulder Constant score (100: no pain, 0: maximum pain) |
55±22.9 | 91.7±5.9 | 0.004 (Man-Whitney U test) |
| Simple Shoulder Test (12: best score, 0: worst score) |
5.3±3.2 | 10.5±1.45 | 0.006 (Man-Whitney U test) |
| Coracoclavicular distance (mm) | 8.6±0.9 | 11.6±1.2 | < 0.001 (Man-Whitney U test) |
VAS: Visual Analog Scale
DASH: Disabilities of the Arm, Shoulder, and Hand
ASES: American Shoulder and Elbow Surgeons Standardized Shoulder Assessment
UCLA: University of California, Los Angeles
Figure 3.

Subacromial erosion and osteoarthritis of acromioclavicular joint; removal of hook plate 13 months after fixation
Discussion
In acute ACJ dislocation, the AC and CC ligaments still have the potential to be healed; therefore, surgical techniques aimed to align the ends of the torn ligaments to facilitate tissue healing. There are many different types of rigid trans-articular and nonrigid extra-articular fixations. In the past, wires and threaded pins were frequently used for the temporary trans-articular fixation of the ACJ. However, pin migration or breakage, pin-site infection, fixation failure, and recurrent instability after pin removal were major concerns about these conventional therapies.
Bosworth screw was also used to stabilize ACJ extra-articularly; however, it may be associated with coracoid fracture, erosion on the clavicle, and loosening of screw. Extra-articular stabilization between coracoid and clavicle with cerclage using heavy sutures or high-strength synthetic materials induced a sawing effect on clavicle due to the rotation of the clavicle. On the other hand, sutures may fail due to knot slippage and suture breakage (1, 8, 12, 21).
In recent years, the two modern techniques commonly used for Rockwood type III and more severe ACJ dislocations are rigid trans-articular CC fixation with HP and nonrigid extra-articular fixation using a suspensory loop with flip buttons. Each technique has its own advantages and disadvantages. The suspensory loop may be either a tightrope (i.e., single or double), continuous loop with either a single, double or triple endobuttons, synthetic ligament, multistrand titanium cable, and absorbable polydioxansulfate (PDS) sling (1, 4, 5, 8-11, 17, 18, 20).
In the present study, HP was used for rigid trans-articular CC fixation. The HP fixation has a simple and easy technique; however, there are several concerns that HP may lead to shoulder pain and dysfunction. The HP may crowd and violate the subacromial space and produce impingement syndrome with rotator cuff injury, subacromial osteolysis, osteoarthritis of the ACJ, implant failure, and CC ossification (12-14). In this regard, a second operation is recommended to remove the adverse effects of HP on ligamentous healing.
Removal of HP improves the shoulder functional scores (9, 12, 16). In a study carried out by Chen et al., HPs were removed 8 to12 months after the surgery. Among the patients in the aforementioned study, 10 (30.3%) and 6 (18.1%) cases had subacromial osteolysis and osteoarthritis of ACJ, respectively (12). In the present study, 6 (75%) out of the 8 subjects showed subacromial osteolysis and osteoarthritis of the ACJ that can be a major concern similar to other studies (15, 21).
In the present study, CLDE was used for nonrigid extra-articular CC fixation. The CLDE eliminates the problem of knot breakage and slippage that may occur in suture-button techniques. The CLDE has a double strength of the native tendon. However, it is a technically complex and demanding task requiring longer operation time. It requires accurate drilling on the clavicle and at the base of coracoid. Large or misdirected drill holes can produce fracture through clavicle and coracoids (4, 5). In the present study, 3 (27%) out of 11 patients had reduction loss and failed surgery.
The literature provides a plethora of heterogeneous comparative studies between nonrigid extra-articular and rigid trans-articular CC fixations for ACJ dislocations with contradictory outcomes. Majority of the studies are retrospective with a relatively low number of subjects and short-term follow-up that can pool the acute and chronic ACJ dislocations, as well as different types of Rockwood classification for ACJ dislocation together (4, 19). The authors have used minimally invasive, arthroscopic, and open surgical techniques (7, 10, 19). In some studies, patients with radiographically displaced and redislocated ACJ were not excluded from the final evaluation and the inferential analysis (7, 11, 15). In a study conducted by Cai et al., HPs were not removed at final evaluation (11).
In another study performed by Metzlaff et al., no significant clinical difference was observed between HP and minimally invasive reconstruction of suspensory loop with two flip buttons (19). Eschler et al. compared HP fixation with absorbable PDS sling in ACJ dislocations. In the aforementioned study, there was no significant difference in the functional outcomes of both groups; however, HP restored CC distance more accurately than PDS sling (15).
In a retrospective multicenter study, Natera-Cisneros et al. compared arthroscopy-assisted tightrope fixation with HP fixation for acute high-grade ACJ dislocations. Patients with nonrigid fixations had a better quality of life; nevertheless, 12 (60%) out of 20 patients with tightrope achieved anatomic ACJ reduction. In the aforementioned study, HPs were removed 3.98 months (on average) after the surgery; however, 7 (63.63%) out of 11 patients achieved anatomic ACJ reduction (7).
In a systematic review and meta-analysis, Arirachakaran et al. compared the clinical outcomes and complications of the loop suspensory fixation devices, including tightrope, synthetic ligament or absorbable PDS sling, with hook plate fixation for the treatment of acute ACJ injury. They found that in a short-term period, loop suspensory fixation had higher postoperative Constant-Murley score and lower postoperative pain level; however, loop suspensory fixation showed higher complication rates (8).
In a prospective randomized study carried out by Cai et al., HP fixation was compared with tightrope fixation in Rockwood type III ACJ dislocations. In one year of follow-up, there was no significant difference between Constant-Murley scores of the two groups. The difference between VAS scores was in favor of the tightrope group. Both groups achieved reasonable and satisfactory clinical and radiological outcomes. Moreover, 3 (10%) out of 30 patients with tightrope fixations had complete ACJ redislocations. The HP was not removed during the study (11).
In the present study, similar to other researches, nonrigid extra-articular CLDE CC fixation exhibited better clinical outcomes, compared to rigid fixation with HP (in a short-term period). However, it was a technically demanding procedure with longer operation time and higher rate of failure. The HP maintained the CC distance better, and its application was more feasible. The HP needs a second surgery for the removal and development of subacromial erosion and osteoarthritis of the ACJ that is considered one of its major concerns.
One of the limitations of the present study was low sample size due to the low incidence of ACJ dislocation. Contaminant reconstruction of ligament with the CLDE or HP techniques was useful and requires further evaluation in future studies. However, in this study, patient follow-up was performed after HP discharge, and all the complications were honestly recorded. The present study was a short-term retrospective single-center study with a small number of patients. It is suggested to carry out further multicenter studies with a larger number of subjects, longer follow-ups, as well as randomized and prospective design.
Conflicts of Interest:
The authors declare that there is no conflict of interest.
Ethical Issues:
This study was approved by the Ethics Committee of Urmia University of Medical Sciences.
Acknowledgements
This study was financially supported by Clinical Research Development Unit of Urmia University of Medical Sciences, Urmia, Iran.
References
- 1.Teodoro RL, Nishimi AY, Pascarelli L, Bongiovanni RR, Velasco MA, Dobashi ET. Surgical treatment of acromioclavicular dislocation using the endobutton. Acta Ortop Bras. 2017;25(3):81–4. doi: 10.1590/1413-785220172503166657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Domos P, Sim F, Dunne M, White A. Current practice in the management of Rockwood type III acromioclavicular joint dislocations-National survey. J Orthop Surg (Hong Kong) 2017;25(2):2309499017717868. doi: 10.1177/2309499017717868. [DOI] [PubMed] [Google Scholar]
- 3.Rockwood CA Jr. Injuries to the acromioclavicular joint. In: Rockwood CA Jr, Williams GR, Young DC., editors. Rockwood & Green’s fractures in adults. 4th ed. Philadelphia: Lippincott-Raven Publishers; 1996. [Google Scholar]
- 4.Struhl S, Wolfson TS. Continuous loop double endobutton reconstruction for acromioclavicular joint dislocation. Am J Sports Med. 2015;43(10):2437–44. doi: 10.1177/0363546515596409. [DOI] [PubMed] [Google Scholar]
- 5.Struhl S. Double endobutton technique for repair of complete acromioclavicular joint dislocations. Techniq Shoulder Elbow Surg. 2007;8(4):175–9. [Google Scholar]
- 6.Murena L, Vulcano E, Ratti C, Cecconello L, Rolla PR, Surace MF. Arthroscopic treatment of acute acromioclavicular joint dislocation with double flip button. Knee Surg Sports Traumatol Arthrosc. 2009;17(12):1511–5. doi: 10.1007/s00167-009-0838-5. [DOI] [PubMed] [Google Scholar]
- 7.Natera-Cisneros L, Sarasquete-Reiriz J, Escolà-Benet A, Rodriguez-Miralles J. Acute high-grade acromioclavicular joint injuries treatment: arthroscopic non-rigid coracoclavicular fixation provides better quality of life outcomes than hook plate ORIF. Orthop Traumatol Surg Res. 2016;102(1):31–9. doi: 10.1016/j.otsr.2015.10.007. [DOI] [PubMed] [Google Scholar]
- 8.Arirachakaran A, Boonard M, Piyapittayanun P, Kanchanatawan W, Chaijenkij K, Prommahachai A, et al. Post-operative outcomes and complications of suspensory loop fixation device versus hook plate in acute unstable acromioclavicular joint dislocation: a systematic review and meta-analysis. J Orthop Traumatol. 2017;18(4):293–304. doi: 10.1007/s10195-017-0451-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Athar MS, Ashwood N, Arealis G, Hamlet M, Salt E. Acromioclavicular joint disruptions: A comparison of two surgical approaches ‘hook’ and ‘rope’. J Orthop Surg (Hong Kong) 2018;26(1):2309499017749984. doi: 10.1177/2309499017749984. [DOI] [PubMed] [Google Scholar]
- 10.Bin Abd Razak HR, Yeo EN, Yeo W, Lie TD. Short-term outcomes of arthroscopic TightRope® fixation are better than hook plate fixation in acute unstable acromioclavicular joint dislocations. Eur J Orthop Surg Traumatol. 2017;28(5):869–75. doi: 10.1007/s00590-017-2095-5. [DOI] [PubMed] [Google Scholar]
- 11.Cai L, Wang T, Lu D, Hu W, Hong J, Chen H. Comparison of the tight rope technique and clavicular hook plate for the treatment of Rockwood type III acromioclavicular Joint Dislocation. J Invest Surg. 2017;31(3):226–33. doi: 10.1080/08941939.2017.1305022. [DOI] [PubMed] [Google Scholar]
- 12.Chen CH, Dong QR, Zhou RK, Zhen HQ, Jiao YJ. Effects of hook plate on shoulder function after treatment of acromioclavicular joint dislocation. Int J Clin Exp Med. 2014;7(9):2564–70. [PMC free article] [PubMed] [Google Scholar]
- 13.De Baets T, Truijen J, Driesen R, Pittevils T. The treatment of acromioclavicular joint dislocation Tossy grade III with a clavicle hook plate. Acta Orthop Belg. 2004;70(6):515–9. [PubMed] [Google Scholar]
- 14.Ding M, Ni J, Hu J, Song D. Rare complication of clavicular hook plate: clavicle fracture at the medial end of the plate. J Shoulder Elbow Surg. 2011;20(7):18–20. doi: 10.1016/j.jse.2011.06.005. [DOI] [PubMed] [Google Scholar]
- 15.Eschler A, Gradl G, Gierer P, Mittlmeier T, Beck M. Results after AC joint repair with the hook plate. Arch Orthop Trauma Surg. 2012;132(1):33–9. doi: 10.1007/s00402-011-1399-x. [DOI] [PubMed] [Google Scholar]
- 16.Gao YS, Zhang YL, Ai ZS, Sun YQ, Zhang CQ, Zhang W. Transarticular fixation by hook plate versus coracoclavicular stabilization by single multistrand titanium cable for acute Rockwood grade-V acromioclavicular joint dislocation: a case-control study. BMC Musculoskelet Disord. 2015;16(1):360. doi: 10.1186/s12891-015-0820-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lu D, Wang T, Chen H, Sun LJ. A comparison of double Endobutton and triple Endobutton techniques for acute acromioclavicular joint dislocation. Orthop Traumatol Surg Res. 2016;102(7):891–5. doi: 10.1016/j.otsr.2016.07.003. [DOI] [PubMed] [Google Scholar]
- 18.Lim YW. Triple endobutton technique in acromioclavicular joint reduction and reconstruction. Ann Acad Med Singapore. 2008;37(4):294–9. [PubMed] [Google Scholar]
- 19.Metzlaff S, Rosslenbroich S, Forkel PH, Schliemann B, Arshad H, Raschke M, et al. Surgical treatment of acute acromioclavicular joint dislocations: hook plate versus minimally invasive reconstruction. Knee Surg Sports Traumatol Arthrosc. 2016;24(6):1972–8. doi: 10.1007/s00167-014-3294-9. [DOI] [PubMed] [Google Scholar]
- 20.Wei HF, Chen YF, Zeng BF, Zhang CQ, Chai YM, Wang HM, et al. Triple endobuttton technique for the treatment of acute complete acromioclavicular joint dislocations: preliminary results. Int Orthop. 2011;35(4):555–9. doi: 10.1007/s00264-010-1057-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yoon JP, Lee BJ, Nam SJ, Chung SW, Jeong WJ, Min WK, et al. Comparison of results between hook plate fixation and ligament reconstruction for acute unstable acromioclavicular joint dislocation. Clin Orthop Surg. 2015;7(1):97–103. doi: 10.4055/cios.2015.7.1.97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zhang L, Zhou X, Qi J, Zeng Y, Zhang S, Liu G, et al. Modified closed-loop double-endobutton technique for repair of Rockwood type III acromioclavicular dislocation. Exp Ther Med. 2018;15(1):940–8. doi: 10.3892/etm.2017.5487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhang J, Ying Z, Wang Y. surgery for acromioclavicular dislocation: factors affecting functional recovery. Am Surg. 2017;83(12):1427–32. doi: 10.1177/000313481708301231. [DOI] [PubMed] [Google Scholar]