

Abstract
Background
Endometriosis is defined as a chronic inflammatory disease. Recent studies have shown that increased coagulation parameters including fibrinogen and platelets are associated with endometriosis. The objective of this study was to determine the levels of inflammatory markers and coagulation parameters and their correlations in women with endometriomas compared to those with benign ovarian cysts or normal pelvic anatomy.
Methods
Between June 2015 and June 2017, a total of 548 women who underwent laparoscopic/laparotomic surgery for ovarian endometriomas (OMA group, n = 226), non-endometriosis benign ovarian cysts (Cyst group, n = 210) and tubal reanastomosis (Control group, n = 112) were recruited in this study. Inflammatory markers including c-reactive protein (CRP), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and coagulation parameters including platelet count, thrombin time (TT), prothrombin time (PT), activated partial thromboplastin time, and plasma fibrinogen as well as CA-125 were determined.
Results
Compared with Cyst group and Control group, TT and PT in OMA group were significantly shorter and plasma fibrinogen levels were significantly higher (P < 0.05). Moreover, the levels of plasma fibrinogen were positively correlated with CRP, NLR and PLR (P < 0.05). In addition, the confidence intervals for the area under the curve (AUC) for CA-125 × fibrinogen were significantly higher than those for CA-125 (0.904–0.952 vs. 0.899–0.949) in the diagnosis of endometrioma.
Conclusions
These results indicate that women with endometriomas demonstrate a hypercoagulable status due to the inflammatory nature of endometriosis. The combined determination for CA-125 and fibrinogen demonstrate a higher area under the curve than the single detection of CA-125 in those with endometriomas compared to these with benign ovarian cysts.
Trial registration
This study was approved by the Human Ethics Committee of the Women’s Hospital, School of Medicine, Zhejiang University (No.20170174) and all women provided written informed consent.
Keywords: Endometriosis, Fibrinogen, Inflammation, Coagulation, Ovarian cyst
Background
Endometriosis, defined as the presence of functional endometrial tissue outside the uterine cavity, is considered to be a chronic inflammatory disease, which is related to the increase of pro-inflammatory cytokines and chemokines [1]. The inflammatory process of endometriosis is associated with increased levels of activated macrophages secreted cytokines in the endometriotic lesions and peritoneal fluid (PF), which provides a local microenvironment suitable for the growth and maintenance of endometriosis. The expression levels of interleukin (IL)-1β, IL-6 and tumor necrosis factor (TNF)-α in lesion, endometriotic cyst fluid, and PF have been demonstrated to be increased in women with endometriosis [2–5]. The ratio of neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) in the peripheral blood of women with endometriosis also increased [6–8]. Moreover, the levels of cytokines [5], free iron, reactive oxygen species [9], matrix metalloproteinases (MMPs) [10], activins [11], and even plasminogen activated system components [12] have also been shown to be elevated in women with ovarian endometriomas compared with other benign ovarian cysts. These different inflammatory and coagulation mediators may identify pathways activated or associated with the development and progression of endometriosis [13].
It has been shown that women with endometriosis appear to be in a hypercoagulable and hyperfibrinolytic status because platelets aggregate in endometriotic lesions [14]. In women with endometriosis, platelet counts (PLT) and plasma fibrinogen levels increase [15, 16], thrombin time (TT) [15] and activated partial thromboplastin time (APTT) decrease [15, 17], while prothrombin time (PT) remains at normal level. Moreover, tissue factor (TF, coagulation factor III) is also increased in the endometriotic lesions and PF in women with endometriosis [14, 18]. TF binds to coagulation factor VIIa, activates coagulation factors IX and X, and induces thrombin formation. Fibrinolysis is a response to elevated levels of coagulation factors and promotes the levels of urokinase-plasminogen activator (u-PA) and plasminogen activator inhibitors (PAIs) in the eutopic endometrium and PF [19, 20].
Inflammatory processes can initiate and promote coagulation, increasing the risk of bleeding, microvascular thrombosis and organ dysfunction [21]. In the coagulation cascade reaction, activated platelets and TF bind to coagulation factors and thrombin to induce inflammation [22, 23]. Activated fibrinogen can also induce thrombin generation, which further activates chemokine production and macrophage adhesion [24].
In this study, we aimed to determine the correlations between coagulation parameters (TT, PT, APTT, and PLT), inflammatory biomarkers [C-reactive protein (CRP), NLR and PLR], compare the differences between patients with endometriomas and patients with non-ovarian endometriosis cysts and without ovarian cysts, and to explore how these parameters can be used as auxiliary biomarkers for diagnosis.
Methods
Patients
This study was approved by the Ethics Committee of the Women’s Hospital, Zhejiang University School of Medicine (No.20170174) in accordance with the Declaration of Helsiniki, and we obtained the written informed consent of each participant in this study.
Before the implementation of this study, we used formulas for mismatched case-control studies (α = 0.05, β = 0.1) to determine the size of samples. According to the cut-off of fibrinogen at 2.8 g/L for the diagnosis of endometriomas reported by Chmaj-Wierzchowska et al. [16], P1 and P2 were 0.83 and 0.64 in our small sample test, and the size of samples was at least 111. As a results, a total of 548 women who underwent laparoscopic/laparotomic surgery for ovarian endometriomas (OMA group, n = 226), non-endometriosis benign ovarian cysts (Cyst group, n = 210) and tubal anastomosis (Control group, n = 112) at the Women’s Hospital affiliated to Zhejiang University School of Medicine from June 2015 and June 2017 were recruited in this study. In OMA group, endometriosis was graded according to the Revised American Fertility Society Scoring (rAFS) system (III = 91, IV = 135) [25]. Of the 226 women with endometriosis, 128 (56.6%) women had dysmenorrhea. In Cyst group, 117 (55.7%) women had ovarian mature teratomas, 21 (10.0%) benign ovarian serous tumors, 24 (11.4%) benign ovarian mucinous tumors, 33 (15.7%) simple cysts, 8 (3.8%) follicular cysts, 5 (2.4%) paroophoritic cysts and 2 (1.0%) corpus luteum cysts. In Control group, all women underwent tubal anastomosis because of the requirement of fertility after tubal ligation.
The patients’ demographic and clinical data such as age, gravidity, parity, body mass index (BMI), dysmenorrhea, pelvic pain, and cyst size were extracted and recorded from patients’ original electronic medical record. Due to the lack of women in secretory phase at admission, only women in proliferative phase were included in the study. All patients had no history of hypertension, diabetes, liver and kidney dysfunction, leiomyoma, adenomyosis, and coagulation disorder. No steroid hormone or anticoagulation therapy was given 6 months before surgery.
Blood assays
Before surgery, all of patients had routine peripheral blood tests including complete blood count, serum biochemistry, coagulation profile, and tumor markers. The neutrophil count, lymphocyte count and PLT were determined using an automatic classification analyzer (Beckman, Coulter LH750). CRP levels were measured with an automatic blood analyzer (Abbott, Architect C16000). Levels of APTT, PT, TT and fibrinogen were determined with an automatic blood coagulation analyzer (STAGO, Evolution ISTA-R-IV, Germany). The levels of serum cancer antigen (CA) 125 were measured by chemiluminescence with an endocrine detector (Roche, COBAS800, France).
Statistical analysis
Statistical Package for the Social Sciences Statistics v22.0 were used for data analysis. Continuous data were presented as mean ± standard error of the mean (SEM). The comparison of the distribution of continuous data among the three groups was performed with Kruskal–Wallis H test. Mann–Whitney U and χ2 tests were used to compare the medians and frequencies among the groups. Spearman analysis was conducted to determine the correlation among the measured parameters. The optimal cut-off values of the parameters differentiating endometriomas were evaluated with the receiver operating characteristic (ROC) curve analysis. Then, the area under the curve (AUC) was calculated and the sensitivity and specificity of each parameter were determined. P values of less than 0.05 (P < 0.05) is considered to have statistical significance.
Results
Patients’ characteristics
There were no statistical differences with regard to age, body weight, height or BMI between OMA, Cyst and Control groups (P > 0.05). Compared with the Cyst and Control groups, the gravidity and parity were significantly lower, and the incidence of dysmenorrhea was significantly higher in the OMA group (P < 0.05). No statistical difference in the size of ovarian cysts between the OMA and Cyst groups was observed (P > 0.05, Table 1).
Table 1.
Patients’ characteristics
| Variable | OMA group | Cyst group | Control group |
|---|---|---|---|
| (n = 226) | (n = 210) | (n = 112) | |
| Age (year) & | 35.7 ± 0.4 | 35.9 ± 0.4 | 35.8 ± 0.5 |
| Height (cm) & | 159.2 ± 0.3 | 159.1 ± 0.3 | 158.2 ± 0.3 |
| Body weight (kg) & | 57.4 ± 0.5 | 56.6 ± 0.5 | 57.1 ± 0.6 |
| Body mass index& | 22.6 ± 0.2 | 22.3 ± 0.2 | 22.8 ± 0.2 |
| Gravidity&& | 2 (0–5) | 2 (0–5)* | 3 (1–5)***# |
| Parity&& | 1 (0–2) | 1 (0–2)* | 2 (1–2)***# |
| Dysmenorrhea, n (%) | 128 (56.6) | 26 (12.4) *** | 8 (7.1)*** |
| Cyst size (cm) & | 6.2 ± 0.1 | 6.0 ± 0.2 | – |
OMA group, women with ovarian endometriomas; Cyst group, women with non-endometriosis benign ovarian cysts; Control group, women undergoing tubal anastomosis; * P < 0.05 (compared with OMA group); *** P < 0.0001 (compared with OMA group); # P < 0.0001 (compared with Cyst group); & mean ± SEM; && median [Range (5–95%)]
Comparisons of levels of coagulation parameters and inflammatory markers between groups
The mean (± SEM) levels of CRP (mg/L) were significantly higher in the OMA group (1.38 ± 0.11) than those in the Cyst group (0.86 ± 0.08, P < 0.01) and Control group (0.72 ± 0.15, P < 0.0001, Fig. 1a). Moreover, the levels of NLR and PLR were significantly higher in the OMA group (2.56 ± 0.07 and 146.4 ± 2.8) than those in the Cyst group (2.34 ± 0.07 and 137.7 ± 3.4, P < 0.05; Fig. 1b, c). Furthermore, the levels of PLT (10^9/L) and plasma fibrinogen (g/L) were also significantly higher in the OMA group (239.8 ± 3.6 and 3.29 ± 0.04) than those in the Cyst group (228.4 ± 4.0 and 2.93 ± 0.03, P < 0.05) and the Control group (220.0 ± 5.4 and 2.88 ± 0.05, P < 0.05; Fig. 1d, h). However, the time of TT (s) and PT (s) were significantly shorter in the OMA group (15.42 ± 0.04 and 12.69 ± 0.04) than those in the Cyst group (15.68 ± 0.05 and 13.00 ± 0.04, P < 0.05) and the Control group(15.78 ± 0.06 and 12.99 ± 0.06, P < 0.05; Fig. 1E–1F). No significant differences with regard to CRP, PLT, fibrinogen, TT or PT between the Cyst and Control groups were found (P > 0.05). There were no statistical differences in the APTT between groups (P > 0.05, Fig. 1g).
Fig. 1.

Levels of inflammatory biomarkers and coagulation parameters in groups. a-c, Inflammatory biomarkers of CRP (a), NLR (b) and PLR (c) were measured among groups. d-i, Coagulation parameters of PLT (d), TT (e), PT (f), APTT (g) and fibrinogen (h), as well as cancer antigen CA-125 (i) were measured among groups. OMA group, women with ovarian endometriomas; Cyst group, women with non-endometriosis benign ovarian cysts; Control group, women undergoing tubal anastomosis; CRP, C-reactive protein; NLR, neutrophil-to-lymphocyte ratio; PLR; platelet-to-lymphocyte ratio; PLT, platelet count; TT, thrombin time; PT, prothrombin time; APTT, activated partial thromboplastin time;  OMA group;
OMA group;  Cyst group;
Cyst group;  Control group* P < 0.05; ** P < 0.01; *** P < 0.0001
Control group* P < 0.05; ** P < 0.01; *** P < 0.0001
Spearman analysis showed that fibrinogen was positively correlated with CRP (r = 0.56, P < 0.0001; Fig. 2a), NLR (r = 0.11, P < 0.01; Fig. 2b), and PLR (r = 0.10, P < 0.05; Fig. 2c). PLT was positively correlated with CRP (r = 0.16, P < 0.01; Fig. 2d) but not significantly correlated with NLR (P = 0.45; Fig. 2e). Fibrinogen and PLT demonstrated a significantly positive correlation (r = 0.20, P < 0.0001; Fig. 2f). Moreover, fibrinogen (r = − 0.41, P < 0.0001; r = − 0.37, P < 0.0001 respectively) and PLT (r = − 0.10, P < 0.05; r = − 0.19, P < 0.0001, respectively) were negatively correlated with TT and PT but not significantly correlated with APTT (P > 0.05).
Fig. 2.

Correlations of coagulation parameters and inflammatory biomarkers. a-c, The correlations of fibrinogen with CRP (a), NLR (b) and PLR (c) were tested using Spearmen analysis. d-f, The correlations of PLT with CRP(d), NLR (e) and fibrinogen (f) were tested using Spearmen analysis. CRP, C-reactive protein; NLR, neutrophil-to-lymphocyte ratio; PLR; platelet-to-lymphocyte ratio; PLT, platelet count
Coagulation parameters and inflammatory biomarkers in women with ovarian endometriosis
In the OMA group, no significant correlation between coagulation parameters or inflammatory markers and dysmenorrhea, cyst size or endometriosis stage was found (Table 2). However, the levels of PLT in women with endometriosis who had severe pelvic adhesions were significant higher when compared with women with endometriosis who had mild or no pelvic adhesions (P < 0.05; Table 2). In addition, the time of TT, PT and APTT were shorted, and the levels of fibrinogen were higher in women with endometriosis who had severe pelvic adhesions as compared with women with endometriosis who had mild or no pelvic adhesions, but the differences did not reach statistical significance (P > 0.05; Table 2).
Table 2.
Coagulation parameters and inflammatory biomarkers in women with ovarian endometriosis
| Variables | CRP | NLR | PLR | PLT | TT | PT | APTT | Fb |
|---|---|---|---|---|---|---|---|---|
| Dysmenorrhea | ||||||||
| Yes (n = 128) | 1.46 ± 0.01 | 2.60 ± 0.10 | 148.7 ± 3.9 | 242.3 ± 4.9 | 15.45 ± 0.05 | 12.72 ± 0.05 | 35.86 ± 0.27 | 3.32 ± 0.05 |
| No (n = 98) | 1.27 ± 0.02 | 2.50 ± 0.10 | 143.3 ± 3.8 | 236.5 ± 5.2 | 15.37 ± 0.06 | 12.65 ± 0.06 | 35.11 ± 0.28 | 3.25 ± 0.05 |
| Cyst size, cm | ||||||||
| < = 5 cm (n = 66) | 1.32 ± 0.02 | 2.66 ± 0.14 | 153.2 ± 5.8 | 237.3 ± 7.3 | 15.48 ± 0.08 | 12.71 ± 0.07 | 35.06 ± 0.34 | 3.29 ± 0.07 |
| > 5 cm (n = 160) | 1.40 ± 0.01 | 2.52 ± 0.08 | 143.5 ± 3.1 | 240.8 ± 4.0 | 15.39 ± 0.04 | 12.68 ± 0.05 | 35.73 ± 0.23 | 3.29 ± 0.04 |
| Stage | ||||||||
| III (n = 91) | 1.22 ± 0.02 | 2.58 ± 0.10 | 145.6 ± 4.5 | 243.8 ± 5.4 | 15.38 ± 0.06 | 12.64 ± 0.06 | 35.68 ± 0.30 | 3.24 ± 0.05 |
| IV (n = 135) | 1.48 ± 0.01 | 2.54 ± 0.09 | 146.9 ± 3.5 | 237.1 ± 4.7 | 15.44 ± 0.05 | 12.72 ± 0.05 | 35.44 ± 0.26 | 3.32 ± 0.06 |
| Pelvic adhesions# | ||||||||
| Yes (n = 204) | 1.38 ± 0.01 | 2.52 ± 0.07 | 147.7 ± 3.0 | 242.6 ± 3.8* | 15.41 ± 0.04 | 12.68 ± 0.04 | 35.51 ± 0.20 | 3.29 ± 0.04 |
| N0 (n = 22) | 1.37 ± 0.10 | 2.90 ± 0.32 | 134.2 ± 6.8 | 214.0 ± 10.0 | 15.51 ± 0.13 | 12.76 ± 0.14 | 35.77 ± 0.71 | 3.25 ± 0.11 |
CRP C-reactive-protein (mg/L); NLR Neutrophil to lymphocyte ratio; PLR Platelet to lymphocyte ratio, PLT Platelet count (10^9/L), TT thrombin time (s); PT (s), Prothrombin time, APTT Activated partial thromboplastin time (s), Fb Fibrinogen (g/L). #, Endometriosis women with severe pelvic adhesions; * P < 0.05 (compared with no severe pelvic adhesions)
Diagnostic value of CA-125, coagulation and inflammatory parameters in ovarian endometrioma
The levels of CA-125 in OMA group were significantly higher than those in Cyst group (80.0 ± 7.1 vs. 19.2 ± 0.8; P < 0.0001; Fig. 1i), with a cut-off value at 30.75 IU/mL. The AUC of CA-125 was 0.924 (95% confidence interval: 0.899–0.949) with sensitivity and specificity reaching 82.3 and 90.0%, respectively (Table 3). The optimal cut-off points for inflammatory markers, coagulation parameters, and the combined marker (plus CA-125) for determining endometriosis were evaluated by ROC analysis (Table 3). The results also showed that the sensitivity and specificity of using any of these factors alone for diagnosis of endometrioma were lower than those of CA-125. For fibrinogen, the cut-off value was 3.09 g/L with a validity power at 0.9998 (P1 = 0.63, P2 = 0.28, β = 0.0002) in present study. However, the combination of CA-125 and fibrinogen showed the highest AUC of 0.928 (0.904–0.952) with sensitivity of 0.898 and specificity of 0.829 (Fig. 3). The diagnostic effects of TT or PT combined with CA-125 were also better than that of CA-125 alone. (Table 3).
Table 3.
The diagnostic value of CA-125, coagulation and inflammatory parameters in ovarian endometrioma
| Parameters | AUC (95% CI) | Sensitivity (%) | Specificity (%) | Cutoff value |
|---|---|---|---|---|
| CA-125 (IU/mL) | 0.924 (0.899–0.949) | 82.3 | 90.0 | 30.75 |
| CRP (mg/L) | 0.630 (0.578–0.682) | 78.8 | 40.1 | 0.35 |
| NLR | 0.575 (0.522–0.629) | 77 | 39.5 | 1.88 |
| PLR | 0.584 (0.530–0.638) | 65.9 | 51.4 | 128.3 |
| PLT (10^9/L) | 0.557 (0.503–0.611) | 41.2 | 69.5 | 253.5 |
| TT (s) | 0.613 (0.560–0.665) | 69.5 | 49.1 | 15.35 |
| PT (s) | 0.643 (0.592–0.695) | 56.7 | 65 | 12.85 |
| APTT (s) | 0.546 (0.492–0.600) | 33.3 | 76.1 | 37.45 |
| Fibrinogen (g/L) | 0.692 (0.643–0.741) | 63.3 | 67.1 | 3.09 |
| CA-125 * CRP (IU*mg/mL*L) | 0.832 (0.794–0.869) | 69.5 | 82.6 | 24.17 |
| CA-125 * NLR (IU/mL) | 0.899 (0.870–0.927) | 84.1 | 81.0 | 60.06 |
| CA-125 * PLR (IU/mL) | 0.907 (0.879–0.935) | 88.1 | 80.0 | 3383.16 |
| CA-125 * PLT (IU*10^9/mL*L) | 0.909 (0.882–0.937) | 80.1 | 87.6 | 6695.85 |
| CA-125 / TT (IU*s/mL) | 0.926 (0.902–0.951) | 85.0 | 88.1 | 1.84 |
| CA-125 / PT (IU*s/mL) | 0.927 (0.903–0.952) | 87.2 | 85.7 | 2.06 |
| CA-125 / APTT (IU*s/mL) | 0.924 (0.899–0.949) | 88.1 | 84.3 | 0.75 |
| CA-125*Fibrinogen(IU*g/mL*L) | 0.928 (0.904–0.952) | 89.8 | 82.9 | 73.77 |
AUC area under the curve, CRP C-reactive protein, NLR neutrophil-to-lymphocyte ratio, PLR platelet-to-lymphocyte ratio, PLT platelet count, TT thrombin time, PT prothrombin time, APTT activated partial thromboplastin time
Fig. 3.
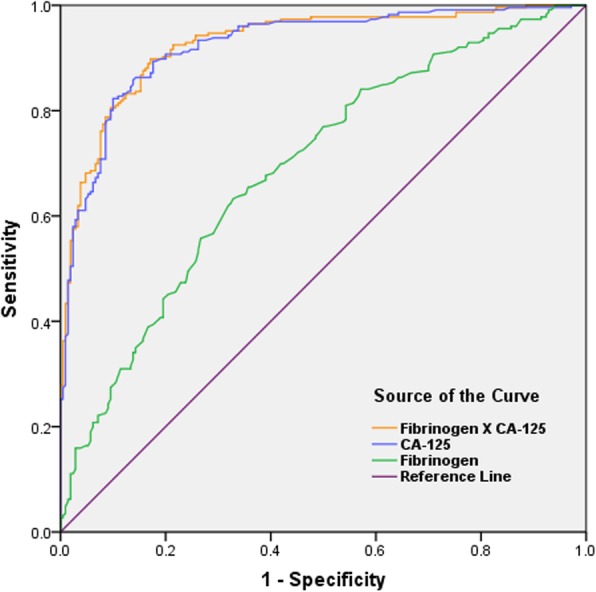
Receiver–operating characteristic curves of CA-125, fibrinogen, and the combined marker for the diagnosis of endometriomas
Discussion
Women with ovarian endometriomas demonstrated a hypercoagulable and inflammatory status, based on increased levels of CRP, PLT, and fibrinogen as well as shortened TT and PT.
Evidence shows that systemic inflammation activates the coagulation system in response to TF-mediated thrombin generation [26]. TF can be secreted by activated monocytes and endothelial and polymorphonuclear cells, which are regulated by TNF-α, IL-1β, and lipopolysaccharide [27–29]. Ding et al. have [14] reported that TF concentrations are significantly elevated in primary endometriotic stromal cells. TF binds to circulating factor VIIa to mediate the activation of factors IX and X and generates thrombin [30]. It has been reported in endometriotic stromal cells, thrombin and proteinase-activated receptor (PAR)-1 agonist induce IL-6 and IL-8 secretion and cell proliferation [23]. Thrombin also can binds to another type of PAR expressed in endometriotic stromal cells, PAR-2, mediating the production of chemokines and cytokines such as IL-8, monocyte chemotactic protein-1, MMP-2, and cyclooxygenase-2 [22].
Studies have reported that inflammatory also induces fibrinolysis activation in endometriosis. Plasmin, an active enzyme, can degrade various extracellular matrix proteins and activate MMPs [31]. The eutopic endometrium of women with ovarian endometriosis has been shown to express high levels of MMP-3, which can hydrolyze and inactivate PAI-1, regulating cell-associated plasmin activities [32]. Higher levels of PAI-1 and tissue inhibitor of metalloproteinase-1 in ovarian endometriomas prevent endometriotic cysts from invading surrounding ovarian tissues [33, 34]. Meanwhile, activated plasmin may induce expression of proinflammatory cytokines such as IL-1α, IL-1β, TNF-α, and TF [28]. Inflammatory changes and activated fibrinolytic systems in women with endometriomas may play an important role in the development and progression of endometriosis.
Fibrinogen influences thrombin formation, platelet aggregation, blood rheology and blood viscosity. Fibrinogen levels are elevated in a variety of diseases such as diabetes and nephrotic diseases, and are associated with an increased risk of cardiovascular disease [35, 36]. Fibrinogen is closely associated with hypercoagulation. Kurata et al. [37] reported that TT, APTT, and PT were all significantly shortened in canines injected with fibrinogen. In the present study, the levels of plasma fibrinogen were significantly higher in women with ovarian endometriomas than those in women with non-endometriosis benign ovarian cysts and those in women without ovarian cysts. These results are in agreement with those of previous reports [15, 16]. We also found that TT and PT were significantly shortened in patients with endometrioma, but there was no difference in APTT. In coagulation cascade, the procoagulation factor, PT, measures the extrinsic coagulation pathway. PT is most sensitive to factor VII (FVII) levels as the latter exhibits a short half-life [38]. Given PT is initiated by TF, our findings correspond to previous studies that have reported the elevation of TF in endometriotic lesions and PF in women with endometriosis [14, 18]. However, Paola et al. [17] demonstrated shortened APTT and constant TT, whereas Guo et al. [15] reported shortened TT and APTT and constant PT in women with endometriosis. These different results may be attributed to the different sample sizes, conditions and techniques applied between the studies, considering that blood assays are highly dependent on the combination of reagents and instruments. For coagulation parameters, specific reagents and different manufacturers usually lead to variable results [38]. Obviously, the coagulation function of women with endometriosis needs further study.
CA-125 is a marker and often used in the diagnosis of endometriomas. Some studies reported that NLR as an adjunct to CA-125 is a useful diagnostic marker [6, 7]. However, some studies refute this claim because NLR has not yet been fully investigated and is not suitable as a diagnostic tool for advanced endometriosis [39, 40]. In our study, we demonstrated that the coagulation factors TT, PT, and fibrinogen were more reliable as complementary auxiliary markers of CA-125 for identifying ovarian endometrioma from non-endometriosis benign ovarian cysts. Obviously, the discrepancies among the studies can be attributed to the differences in sample size, experimental measurement methods, and instruments used.
The primary limitation of our study is its retrospective design. All the recruited women were in proliferative phase of menstrual cycle. The coagulation stability in women with endometriosis remains unknown while coagulation status is usually unaffected by menstrual cycle in healthy women [41]. Moreover, only women with advanced endometriosis (stages III–IV) were included in the study. Therefore, the coagulation function and its influence on inflammation in women with early-stage endometriosis are still uncertain.
A combined influence of inflammatory response and hypercoagulation status may exist in advanced stages of endometriosis. At present, the treatment of endometriosis often focuses on anti-inflammatory control. Modulation of the coagulation pathway in endometriosis may provide another potential treatment option. Studies have reported inhibition of inflammation by blocking formation of TF-PAR-2 and the TF-VIIa signaling pathway [42]. In a mouse model of endometriosis, a chimeric immunoconjugate molecule specifically targeting endothelial TF in ectopic implants has been shown to obliterate the endometriotic implant by vascular disruption without reducing fertility [43]. Guo et al. [44] reported that targeting P-selectin-mediated platelet adhesion can reduce the size of endometriotic lesions, improving general hyperalgesia and resulting in reduction of macrophage infiltration and fibrotic tissue content. Thus, in order to determine whether abnormal coagulation parameters contribute to the diagnosis and treatment of endometriosis, a more detailed study of large samples is needed.
In conclusion, our findings suggest that women with ovarian endometriomas demonstrate a hypercoagulable status potentially attributable to the inflammatory nature of endometrioma. Plasma fibrinogen is an auxiliary marker of serum CA-125 in the diagnosis of endometriosis.
Acknowledgements
None.
Consent to publication
Not applicable.
Abbreviations
- APTT
Activated partial thromboplastin time
- AUC
Area under the curve
- BMI
Body mass index
- CA
Cancer antigen
- CRP
C-reactive protein
- IL
Interleukin
- MMP
Matrix metalloproteinase
- NLR
Neutrophil-to-lymphocyte ratio
- PAIs
Plasminogen activator inhibitors
- PAR
Proteinase-activated receptor
- PF
Peritoneal fluid
- PLR
Platelet-to-lymphocyte ratio
- PLT
Platelet count
- PT
Prothrombin time
- ROC
Receiver operating characteristic
- SEM
Standard error of the mean
- TF
Tissue factor
- TNF
Tumor necrosis factor
- TT
Thrombin time
- uPA
urokinase plasminogen activator
Authors’ contributions
SD: Data Collection, Manuscript writing; QL: Data collection, Manuscript writing; TZ: Data collection; TL: Data analysis; LZ: Data analysis; JW: Data analysis, Manuscript writing; XZ: Project development, Manuscript editing. All authors have read and approved the manuscript in its current state.
Funding
This work was supported by National Key R&D Program of China (2017YFC1001202), The National Natural Science Foundation of China (81471433, 81671429), and Key Medical Science (Innovation) Project of Zhejiang Province. The funders had no role in the design of the study, in the collection, analysis, and interpretation of the data, or in the writing or approval of the manuscript.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
This study is approved by the Human Ethics Committee of the Women’s Hospital, School of Medicine, Zhejiang University (No.20170174) and all women provided written informed consent.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Shaojie Ding and Qiao Lin contributed equally to this work.
Contributor Information
Shaojie Ding, Email: dsjd12345@zju.edu.cn.
Qiao Lin, Email: 88279871@qq.com.
Tianhong Zhu, Email: 21518279@zju.edu.cn.
Tiantian Li, Email: 11718248@zju.edu.cn.
Libo Zhu, Email: 5514027@zju.edu.cn.
Jianzhang Wang, Email: jianzhang.wang@zju.edu.cn.
Xinmei Zhang, Email: zhangxinm@zju.edu.cn.
References
- 1.Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. Fertil Steril. 2012;98(3):511–519. doi: 10.1016/j.fertnstert.2012.06.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sikora J, Mielczarek-Palacz A, Kondera-Anasz Z. Imbalance in cytokines from interleukin-1 family - role in pathogenesis of endometriosis. Am J Reprod Immunol. 2012;68(2):138–145. doi: 10.1111/j.1600-0897.2012.01147.x. [DOI] [PubMed] [Google Scholar]
- 3.Wickiewicz D, Chrobak A, Gmyrek GB, Halbersztadt A, Gabrys MS, Goluda M, et al. Diagnostic accuracy of interleukin-6 levels in peritoneal fluid for detection of endometriosis. Arch Gynecol Obstet. 2013;288(4):805–814. doi: 10.1007/s00404-013-2828-6. [DOI] [PubMed] [Google Scholar]
- 4.Birt JA, Nabli H, Stilley JA, Windham EA, Frazier SR, Sharpe-Timms KL. Elevated peritoneal fluid TNF-alpha incites ovarian early growth response factor 1 expression and downstream protease mediators: a correlation with ovulatory dysfunction in endometriosis. Reprod Sci. 2013;20(5):514–523. doi: 10.1177/1933719113477479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Velasco I, Acien P, Campos A, Acien MI, Ruiz-Macia E. Interleukin-6 and other soluble factors in peritoneal fluid and endometriomas and their relation to pain and aromatase expression. J Reprod Immunol. 2010;84(2):199–205. doi: 10.1016/j.jri.2009.11.004. [DOI] [PubMed] [Google Scholar]
- 6.Tokmak A, Yildirim G, Oztas E, Akar S, Erkenekli K, Gulsen P, et al. Use of neutrophil-to-lymphocyte ratio combined with CA-125 to distinguish Endometriomas from other benign ovarian cysts. Reprod Sci. 2016;23(6):795–802. doi: 10.1177/1933719115620494. [DOI] [PubMed] [Google Scholar]
- 7.Cho S, Cho H, Nam A, Kim HY, Choi YS, Park KH, et al. Neutrophil-to-lymphocyte ratio as an adjunct to CA-125 for the diagnosis of endometriosis. Fertil Steril. 2008;90(6):2073–2079. doi: 10.1016/j.fertnstert.2008.03.061. [DOI] [PubMed] [Google Scholar]
- 8.Yang H, Zhu L, Wang S, Lang J, Xu T. Noninvasive diagnosis of moderate to severe endometriosis: the platelet-lymphocyte ratio cannot be a neoadjuvant biomarker for serum cancer antigen 125. J Minim Invasive Gynecol. 2015;22(3):373–377. doi: 10.1016/j.jmig.2013.06.003. [DOI] [PubMed] [Google Scholar]
- 9.Yamaguchi K, Mandai M, Toyokuni S, Hamanishi J, Higuchi T, Takakura K, et al. Contents of endometriotic cysts, especially the high concentration of free iron, are a possible cause of carcinogenesis in the cysts through the iron-induced persistent oxidative stress. Clin Cancer Res : Official J Am Assoc Cancer Res. 2008;14(1):32–40. doi: 10.1158/1078-0432.CCR-07-1614. [DOI] [PubMed] [Google Scholar]
- 10.Mizumoto H, Saito T, Ashihara K, Nishimura M, Takehara M, Tanaka R, et al. Expression of matrix metalloproteinases in ovarian endometriomas: immunohistochemical study and enzyme immunoassay. Life Sci. 2002;71(3):259–273. doi: 10.1016/S0024-3205(02)01641-7. [DOI] [PubMed] [Google Scholar]
- 11.Reis FM, Di Blasio AM, Florio P, Ambrosini G, Di Loreto C, Petraglia F. Evidence for local production of inhibin a and activin a in patients with ovarian endometriosis. Fertil Steril. 2001;75(2):367–373. doi: 10.1016/S0015-0282(00)01720-9. [DOI] [PubMed] [Google Scholar]
- 12.Boss EA, Massuger LF, Thomas CM, Geurts-Moespot A, van Schaik JH, Boonstra H, et al. Clinical value of components of the plasminogen activation system in ovarian cyst fluid. Anticancer Res. 2002;22(1A):275–282. [PubMed] [Google Scholar]
- 13.Sanchez AM, Vigano P, Somigliana E, Panina-Bordignon P, Vercellini P, Candiani M. The distinguishing cellular and molecular features of the endometriotic ovarian cyst: from pathophysiology to the potential endometrioma-mediated damage to the ovary. Hum Reprod Update. 2014;20(2):217–230. doi: 10.1093/humupd/dmt053. [DOI] [PubMed] [Google Scholar]
- 14.Ding D, Liu X, Duan J, Guo SW. Platelets are an unindicted culprit in the development of endometriosis: clinical and experimental evidence. Hum Reprod. 2015;30(4):812–832. doi: 10.1093/humrep/dev025. [DOI] [PubMed] [Google Scholar]
- 15.Wu Q, Ding D, Liu X, Guo SW. Evidence for a Hypercoagulable state in women with ovarian Endometriomas. Reprod Sci. 2015;22(9):1107–1114. doi: 10.1177/1933719115572478. [DOI] [PubMed] [Google Scholar]
- 16.Chmaj-Wierzchowska K, Kampioni M, Wilczak M, Sajdak S, Opala T. Novel markers in the diagnostics of endometriomas: Urocortin, ghrelin, and leptin or leukocytes, fibrinogen, and CA-125? Taiwan J Obstet Gynecol. 2015;54(2):126–130. doi: 10.1016/j.tjog.2014.08.004. [DOI] [PubMed] [Google Scholar]
- 17.Vigano P, Ottolina J, Sarais V, Rebonato G, Somigliana E, Candiani M. Coagulation status in women with endometriosis. Reprod Sci. 2017;1933719117718273. [DOI] [PubMed]
- 18.Lin M, Weng H, Wang X, Zhou B, Yu P, Wang Y. The role of tissue factor and protease-activated receptor 2 in endometriosis. Am J Reprod Immunol. 2012;68(3):251–257. doi: 10.1111/j.1600-0897.2012.01152.x. [DOI] [PubMed] [Google Scholar]
- 19.Bruse C, Bergqvist A, Carlstrom K, Fianu-Jonasson A, Lecander I, Astedt B. Fibrinolytic factors in endometriotic tissue, endometrium, peritoneal fluid, and plasma from women with endometriosis and in endometrium and peritoneal fluid from healthy women. Fertil Steril. 1998;70(5):821–826. doi: 10.1016/S0015-0282(98)00285-4. [DOI] [PubMed] [Google Scholar]
- 20.Gilabert-Estelles J, Ramon LA, Espana F, Gilabert J, Vila V, Reganon E, et al. Expression of angiogenic factors in endometriosis: relationship to fibrinolytic and metalloproteinase systems. Hum Reprod. 2007;22(8):2120–2127. doi: 10.1093/humrep/dem149. [DOI] [PubMed] [Google Scholar]
- 21.Levi M, van der Poll T. Coagulation and sepsis. Thromb Res. 2017;149:38–44. doi: 10.1016/j.thromres.2016.11.007. [DOI] [PubMed] [Google Scholar]
- 22.Hirota Y, Osuga Y, Hirata T, Harada M, Morimoto C, Yoshino O, et al. Activation of protease-activated receptor 2 stimulates proliferation and interleukin (IL)-6 and IL-8 secretion of endometriotic stromal cells. Hum Reprod. 2005;20(12):3547–3553. doi: 10.1093/humrep/dei255. [DOI] [PubMed] [Google Scholar]
- 23.Hirota Y, Osuga Y, Hirata T, Yoshino O, Koga K, Harada M, et al. Possible involvement of thrombin/protease-activated receptor 1 system in the pathogenesis of endometriosis. J Clin Endocrinol Metab. 2005;90(6):3673–3679. doi: 10.1210/jc.2004-0493. [DOI] [PubMed] [Google Scholar]
- 24.Szaba FM, Smiley ST. Roles for thrombin and fibrin(ogen) in cytokine/chemokine production and macrophage adhesion in vivo. Blood. 2002;99(3):1053–1059. doi: 10.1182/blood.V99.3.1053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertility and sterility. 1997;67(5):817–21. [DOI] [PubMed]
- 26.Levi M, Keller TT, van Gorp E, ten Cate H. Infection and inflammation and the coagulation system. Cardiovasc Res. 2003;60(1):26–39. doi: 10.1016/S0008-6363(02)00857-X. [DOI] [PubMed] [Google Scholar]
- 27.Parry GC, Mackman N. Transcriptional regulation of tissue factor expression in human endothelial cells. Arterioscler Thromb Vasc Biol. 1995;15(5):612–621. doi: 10.1161/01.ATV.15.5.612. [DOI] [PubMed] [Google Scholar]
- 28.Syrovets T, Jendrach M, Rohwedder A, Schule A, Simmet T. Plasmin-induced expression of cytokines and tissue factor in human monocytes involves AP-1 and IKKbeta-mediated NF-kappaB activation. Blood. 2001;97(12):3941–3950. doi: 10.1182/blood.V97.12.3941. [DOI] [PubMed] [Google Scholar]
- 29.Rauch U, Bonderman D, Bohrmann B, Badimon JJ, Himber J, Riederer MA, et al. Transfer of tissue factor from leukocytes to platelets is mediated by CD15 and tissue factor. Blood. 2000;96(1):170–175. doi: 10.1182/blood.V96.1.170. [DOI] [PubMed] [Google Scholar]
- 30.Eilertsen KE, Osterud B. Tissue factor: (patho)physiology and cellular biology. Blood Coagul Fibrinolysis : Int J Haemost Thromb. 2004;15(7):521–538. doi: 10.1097/00001721-200410000-00001. [DOI] [PubMed] [Google Scholar]
- 31.Murphy G, Knauper V, Atkinson S, Gavrilovic J, Edwards D. Cellular mechanisms for focal proteolysis and the regulation of the microenvironment. Fibrinolysis Proteol. 2000;14(2–3):165–174. doi: 10.1054/fipr.2000.0068. [DOI] [Google Scholar]
- 32.Ugwu F, Lemmens G, Collen D, Lijnen HR. Modulation of cell-associated plasminogen activation by stromelysin-1 (MMP-3) Thromb Haemost. 1999;82(3):1127–1131. doi: 10.1055/s-0037-1614341. [DOI] [PubMed] [Google Scholar]
- 33.Gilabert-Estelles J, Estelles A, Gilabert J, Castello R, Espana F, Falco C, et al. Expression of several components of the plasminogen activator and matrix metalloproteinase systems in endometriosis. Hum Reprod. 2003;18(7):1516–1522. doi: 10.1093/humrep/deg300. [DOI] [PubMed] [Google Scholar]
- 34.Ramon L, Gilabert-Estelles J, Castello R, Gilabert J, Espana F, Romeu A, et al. mRNA analysis of several components of the plasminogen activator and matrix metalloproteinase systems in endometriosis using a real-time quantitative RT-PCR assay. Hum Reprod. 2005;20(1):272–278. doi: 10.1093/humrep/deh571. [DOI] [PubMed] [Google Scholar]
- 35.Zhao Y, Zhang J, Zhang J, Wu J. Diabetes mellitus is associated with shortened activated partial thromboplastin time and increased fibrinogen values. PLoS One. 2011;6(1):e16470. doi: 10.1371/journal.pone.0016470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Zwaginga JJ, Koomans HA, Sixma JJ, Rabelink TJ. Thrombus formation and platelet-vessel wall interaction in the nephrotic syndrome under flow conditions. J Clin Invest. 1994;93(1):204–211. doi: 10.1172/JCI116947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kurata M, Sasayama Y, Yamasaki N, Kitazawa I, Hamada Y, Horii I. Mechanism for shortening PT and APTT in dogs and rats--effect of fibrinogen on PT and APTT. J Toxicol Sci. 2003;28(5):439–443. doi: 10.2131/jts.28.439. [DOI] [PubMed] [Google Scholar]
- 38.Ng VL. Prothrombin time and partial thromboplastin time assay considerations. Clin Lab Med. 2009;29(2):253–263. doi: 10.1016/j.cll.2009.05.002. [DOI] [PubMed] [Google Scholar]
- 39.Yavuzcan A, Caglar M, Ustun Y, Dilbaz S, Ozdemir I, Yildiz E, et al. Evaluation of mean platelet volume, neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in advanced stage endometriosis with endometrioma. J Turk Ger Gynecol Association. 2013;14(4):210–215. doi: 10.5152/jtgga.2013.55452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kim SK, Park JY, Jee BC, Suh CS, Kim SH. Association of the neutrophil-to-lymphocyte ratio and CA-125 with the endometriosis score. Clin Exp Repro Med. 2014;41(4):151–157. doi: 10.5653/cerm.2014.41.4.151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Tchaikovski SN, Thomassen MC, Costa SD, Bremme K, Rosing J. Changes in haemostatic parameters during the menstrual cycle and subsequent use of drospirenone-containing oral contraceptives. Thromb Res. 2014;134(5):1032–1037. doi: 10.1016/j.thromres.2014.09.008. [DOI] [PubMed] [Google Scholar]
- 42.Ahamed J, Versteeg HH, Kerver M, Chen VM, Mueller BM, Hogg PJ, et al. Disulfide isomerization switches tissue factor from coagulation to cell signaling. Proc Natl Acad Sci U S A. 2006;103(38):13932–13937. doi: 10.1073/pnas.0606411103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Krikun G, Hu Z, Osteen K, Bruner-Tran KL, Schatz F, Taylor HS, et al. The immunoconjugate "icon" targets aberrantly expressed endothelial tissue factor causing regression of endometriosis. Am J Pathol. 2010;176(2):1050–1056. doi: 10.2353/ajpath.2010.090757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Guo SW, Ding D, Geng JG, Wang L, Liu X. P-selectin as a potential therapeutic target for endometriosis. Fertil Steril. 2015;103(4):990–1000. doi: 10.1016/j.fertnstert.2015.01.001. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.