

Abstract
Background:
Ultrasound guidance has dramatically improved the accuracy of nerve localization, and various adjuvants prolong the block and extend analgesia.
Aims:
This study aimed to evaluate the effects of dexmedetomidine added to 0.5% bupivacaine on the onset and duration of motor and sensory blockade and the duration of analgesia.
Settings and Design:
This is a prospective, randomized double-blind, study.
Materials and Methods:
Sixty adult patients aged 20–60 years of either sex undergoing orthopedic procedures on the forearm were randomly allocated into two groups of thirty each: Group BS (bupivacaine + saline) and Group BD (bupivacaine + dexmedetomidine). All patients were administered subclavian perivascular brachial plexus block under ultrasound guidance. Group BS: Patients in this group were administered 20-mL 0.5% bupivacaine + 0.75-mL saline. Group BD: Patients in this group were administered 20-mL 0.5% bupivacaine + 0.75-mL dexmedetomidine (75 μg).
Statistical Analysis:
Statistical analysis was performed with IBM SPSS software Version 21.0. Quantitative data were expressed as mean ± standard deviation. Independent sample t-test was used for comparisons between the two groups. P < 0.05 was considered statistically significant.
Results:
Demographic data and surgical characteristics were similar in both groups. The onset times for sensory and motor blocks were statistically significantly shorter in Group BD compared to Group BS (P < 0.01), whereas the duration of blocks and analgesia were statistically significantly longer (P < 0.01) in Group BD.
Conclusion:
The addition of dexmedetomidine to 0.5% bupivacaine for supraclavicular brachial plexus block shortens the onset time and prolongs both the duration of the block and analgesia.
Keywords: Bupivacaine, dexmedetomidine, subclavian perivascular brachial plexus, ultrasound
INTRODUCTION
Local anesthetic nerve blocks provide excellent operative conditions and good analgesia with a low incidence of complications.[1] Of all the techniques used for nerve localization, ultrasound guidance has gained immense popularity as it has been shown to be more precise and accurate with the added advantage of the need to use lesser volumes of local anesthetic agents in extremity blocks.
Extremity blocks using long-acting local anesthetics such as bupivacaine are helpful for extended postoperative pain relief, but the duration of sensory block may not be sufficient, and postoperative opioids may still be needed. The recent past has seen increasing focus on the clinical application of α2 adrenoceptor agonists in anesthesia due to their sedative-, analgesic-, and anesthetic-sparing effects.[2] Clonidine, an α2 adrenoceptor agonist, has been shown to prolong the duration of peripheral nerve blocks.[3,4,5] Dexmedetomidine is a more selective α2 adrenoceptor agonist, and its α2 selectivity is eight times more than that of clonidine, making it a much more effective sedative and analgesic agent.[6]
The safety and efficacy of dexmedetomidine has been shown in various studies which included its use as an adjuvant in Bier's block and central neuraxial blocks including intrathecal and epidural administration.[7,8,9,10] Two studies[11,12] have reported an increased duration of sensory blockade and analgesia, with dexmedetomidine as an adjuvant to local anesthetics for peripheral nerve blocks.
Previous studies have shown that dexmedetomidine 100 μg effectively prolongs brachial plexus block and also reduces onset time. Using ultrasound guidance with Enhanced Needle Visualization (ENV) software (SonoSite, Inc. WA, USA), we sought to evaluate whether using a lower dose of dexmedetomidine (75 μg) and lower volume of local anesthetic (20 mL) would be effective.
In this study, we evaluated the effect of adding dexmedetomidine to bupivacaine for ultrasound-guided subclavian perivascular brachial plexus block.
Our primary end points were the onset time of sensory block (OTSB), onset set of motor block (OTMB), duration of sensory block (DSB), and duration of motor block (DMB).
MATERIALS AND METHODS
After institutional ethical committee's approval and written informed consent, sixty American Society of Anesthesiologists Physical Status I–II patients of either sex, aged 20–60 years, scheduled for bony orthopedic procedures on the forearm and hand under ultrasound-guided subclavian perivascular brachial plexus block, were enrolled in a prospective, double-blind, controlled trial.
Exclusion criteria: Patients receiving adrenoceptor agonists or antagonists and anticoagulants; those with a history of bleeding disorders; those with a history of cardiac, respiratory, hepatic, or renal failure; and pregnant women.
Using computer-generated random numbers, the patients were randomly allocated to two groups of thirty each:
Group BS: Received 20 mL of 0.5% bupivacaine + 1.5 mL of 0.9% saline
Group BD: Received 20 mL of 0.5% bupivacaine +1.5 mL (75 μg) of dexmedetomidine.
On arrival in the operating room, standard monitoring was established, and baseline heart rate (HR), blood pressure, and oxygen saturation were recorded. The patients were not premedicated before the block. Intravenous access was secured on the upper extremity contralateral to the one on which the block was to be performed. With the patient in supine position and the head turned away from the side to be blocked, the area of the proposed block site and around was disinfected with chlorhexidine solution (chlorhexidine gluconate solution 2.5% v/v equivalent to chlorhexidine gluconate 0.5% w/v ethyl alcohol I. P. 70%).
Ultrasound imaging was performed using a Sonosite M-Turbo (Sonosite Inc. Bothell, WA, USA) with a High Frequency Linear (HFL), 38 mm, 13-6 MHz, transducer [Figure 1]. After sterile preparation of the area, a scout scanning was done using sterile gel, and the subclavian perivascular brachial plexus was identified by the characteristic bunch-of-grapes appearance.
Figure 1.

HFL 38 probe (left) Sonosite M-turbo with Enhanced Needle Visualization software (right)
The local anesthetic with normal saline or with dexmedetomidine was prepared in a sterile bowl by an anesthetist not involved in the study. The operator performing the block was blinded to the composition of the injectate, and he was the one who recorded the sensory and motor tests to evaluate block success and duration.
After preparation of the area, a skin wheal was raised using 2 mL of 1% lidocaine at the intended site of block performance. Under direct sonographic visualization, a 22G 50-mm short beveled Stimuplex® needle (B. Braun) was advanced in plane with transducer, with the subclavian perivascular brachial plexus in a short axis. Sonosite ENV™ software was used to facilitate the visualization of the needle.
Once the subclavian artery and brachial plexus were visible as they passed over the first rib, an in-plane technique was used with lateral needle entry, allowing the whole of the needle to be kept in continuous view, and 25 mL of the solution was deposited in aliquots of 5 mL (after careful negative aspiration following every 5 mL to avoid intravascular injection) accurately around the plexus. Following this, 5 mL of 0.25% bupivacaine was used to block the intercostobrachial nerve.
The sensory block (four nerves) was assessed by pinprick test using a 3-point scale: 0 = normal sensation, 1 = loss of sensation of pinprick (analgesia), and 2 = loss of sensation of touch (anesthesia). The motor block was assessed by thumb abduction (radial nerve), thumb adduction (ulnar nerve), thumb opposition (median nerve), and flexion at elbow (musculocutaneous nerve). The motor block was also graded on a 3-point scale according to the modified Bromage scale as follows: 0 = normal motor function, 1 = reduced motor strength but able to move fingers, and 2 = complete motor block.
The sensory and motor blocks were evaluated every 3 min till their onset and then every 30 min after surgery, until they had resolved.
The onset time for sensory block was defined as the time interval between the end of total local anesthetic administration and complete sensory block (a score of 2 for all nerves). The duration of sensory block was defined as the time interval between the end of local anesthetic administration and complete resolution of anesthesia on all nerves (a score of “0”). The onset time for motor block was defined as the time interval between the total local anesthetic administration and complete motor block (a score of “2”). The duration of motor block was defined as the time interval between the end of local anesthetic administration and the recovery of complete motor function of the hand and forearm (score “0”).
HR, systolic arterial blood pressure, and diastolic arterial blood pressure were recorded at 0, 5, 10, 15, 30, 45, 60, 90, 120, 150, and 180 min. Hypotension was defined as decrease in arterial pressure to <20% relative to baseline and bradycardia as a HR <50 bpm. Pain was assessed using the Visual Analog Scale (0–10). The nursing staff were advised to administer intramuscular injection of diclofenac sodium 75 mg (rescue analgesia) when the Visual Analog Score >4. The time between the end of the local anesthetic administration and the first analgesic request was recorded as the duration of analgesia.
Statistical analysis
Statistical analysis was performed with IBM SPSS software Version 21.0 (SPSS Inc., Chicago, IL, USA). Statistical power for the motor and sensory block durations between the two groups at α=0.05 was calculated to be 99.99%. The descriptive statistics of the data give the information about number of patients (n) and minimum, maximum, mean, and standard deviation (SD) values of the variables under study. Quantitative data were expressed as mean ± SD [Table 1]. Independent sample ttest was used for comparisons between the two groups. P < 0.05 was considered statistically significant.
Table 1.
Descriptive statistics of the data set
| Descriptive statistics | ||||
|---|---|---|---|---|
| Variable | n | Minimum | Maximum | Mean±SD |
| BD-age (years) | 30 | 25.00 | 60.00 | 41.57±11.25 |
| BD-height (cm) | 30 | 140.00 | 175.00 | 165.03±7.41 |
| BD-weight (kg) | 30 | 58.00 | 80.00 | 68.83±5.38 |
| BD-OTSB | 30 | 9.00 | 12.00 | 10.10±1.47 |
| BD-OTMB | 30 | 12.00 | 15.00 | 13.10±1.47 |
| BD-DSB | 30 | 690.00 | 830.00 | 769.50±36.87 |
| BD-DMB | 30 | 650.00 | 800.00 | 719.17±44.26 |
| BD-DA | 30 | 800.00 | 930.00 | 869.33±31.18 |
| BS-age (years) | 30 | 22.00 | 59.00 | 39.77±10.89 |
| BS-height (cm) | 30 | 150.00 | 178.00 | 165.67±6.83 |
| BS-weight (kg) | 30 | 63.00 | 80.00 | 70.47±4.29 |
| BS-OTSB | 30 | 9.00 | 15.00 | 12.70±1.88 |
| BS-OTMB | 30 | 12.00 | 18.00 | 15.60±1.83 |
| BS-DSB | 30 | 560.00 | 700.00 | 619.33±35.10 |
| BS-DMB | 30 | 480.00 | 640.00 | 561.00±40.71 |
| BS-DA | 30 | 680.00 | 820.00 | 738.50±38.40 |
BS=Bupivacaine-saline, BD=Bupivacaine-dexmedetomidine, OTSB=Onset time of sensory block, OTMB=Onset time of motor block, DSB=Duration of sensory block, DMB=Duration of motor block, DA=Duration of analgesia, SD=Standard deviation
RESULTS
The demographic and surgical data were similar in each group [Table 2]. The sensory and motor block onset times were statistically significantly shorter in Group BD compared to Group BS (P < 0.01).
Table 2.
Demographic and surgical data
| Group BS (n=30) (SD) | Group BD (n=30) (SD) | P | |
|---|---|---|---|
| Age (years) | 39.77±10.89 | 41.57±11.25 | 0.531(NS) |
| Height (cm) | 165.67±6.83 | 165.03±7.41 | 0.732(NS) |
| Weight (kg) | 70.47±4.23 | 68.83±5.38 | 0.199(NS) |
| Gender (M/F) | 22/8 | 21/9 | |
| Duration of surgery (minutes) | 154.33±17.11 | 153.33±14.46 | 0.808(NS) |
| Type of surgeries | |||
| #Middle 1/3rd of humerus | 6 | 8 | 0.5416(NS) |
| #Lower end of humerus | 11 | 9 | 0.5839(NS) |
| # Both bones forearm | 9 | 8 | 0.7745(NS) |
| #Olecranon | 4 | 5 | 0.7177(NS) |
Note: NS=Not significant, BS=Bupivacaine-saline, BD=Bupivacaine-dexmedetomidine, SD=Standard deviation
The sensory and motor blockade durations were longer in Group BD than in Group BS (P < 0.01). The duration of analgesia was statistically significantly longer in Group BD than in Group BS (P < 0.01) [Table 3].
Table 3.
Onset times of sensory and motor blocks and duration of analgesia (n=30)
| X̄±SD | t-statistic | P | ||
|---|---|---|---|---|
| Group BS | Group BD | |||
| OTSB (min) | 12.7±1.88 | 10.1±1.47 | 5.970 | 1.53e-07 |
| OTMB (min) | 15.6±1.83 | 13.1±1.47 | 5.831 | 2.58e-07 |
| DSB (min) | 619.33±35.10 | 769.5±36.87 | 16.157 | 0.001 |
| DMB (min) | 561.00±40.71 | 719.17±44.26 | 14.406 | 0.001 |
| DA (min) | 738.5±7.01 | 869.33±31.18 | 14.188 | 0.001 |
BS=Bupivacaine–saline, BD=Bupivacaine–dexmedetomidine, SD=Standard deviation, OTSB=Onset time of sensory block, OTMB=Onset time of motor block, DSB=Duration of sensory block, DMB=Duration of motor block, DA=Duration of analgesia
The mean onset time for sensory and motor blocks in Group BD was 10.1 ± 1.47 and 13.1 ± 1.47 min, respectively. The mean onset time for sensory and motor blocks in Group BS was 12.7 ± 1.88 and 15.6 ± 1.83 min, respectively.
The mean duration for sensory and motor blocks in Group BD was 769.5 ± 36.87 and 719.17 ± 44.26 min, respectively. For Group BS, the mean durations were 619.33 ± 35.10 and 561.00 ± 40.71 min, respectively. The mean duration of analgesia for Group BD was 869.33 ± 31.18 min, whereas it was 738.5 ± 7.01 min for Group BS [Figure 2].
Figure 2.
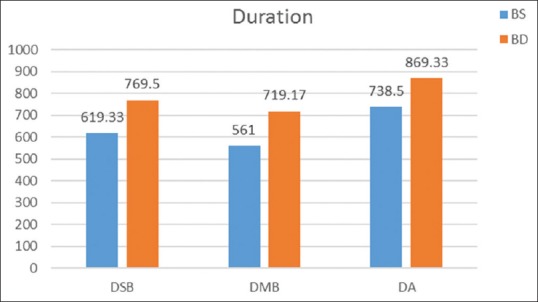
Comparison of duration of sensory block and motor block and duration of analgesia. The difference between the two groups for these parameters was statistically significant (P < 0.001)
Systolic blood pressure levels in Group BD at 10, 15, 30, 45, 60, 90, 120, 150, and 180 min were statistically significantly lower than those in Group BS (P < 0.05). Diastolic blood pressure levels in Group BD at 30, 45, 60, 90, 120, 150, and 180 min were significantly lower than those in Group BS (P < 0.05) [Figure 3]. HR levels in Group BD were statistically significantly lower than those in Group BS (P < 0.05), but the HR was never lower than 50 bpm (bradycardia) at all the time points of measurements [Figure 4]. This was probably because we used only 75 μg of dexmedetomidine perineurally compared to 100 μg in other studies.[13] No side effects – nausea, vomiting, and hypotension – were observed in either group.
Figure 3.
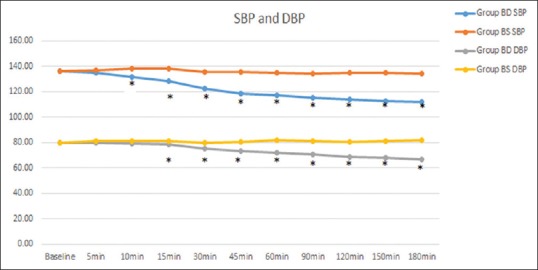
Mean systolic and diastolic arterial pressures for the Groups BS (bupivacaine + saline) and BD (bupivacaine + dexmedetomidine). Asterisks indicate the time points of a statistically significant difference (P < 0.05) when the groups were compared
Figure 4.
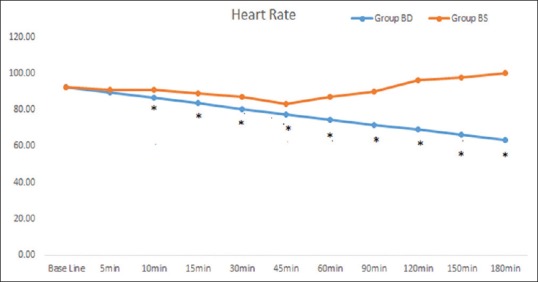
Mean heart rate values in the groups BS (bupivacaine + saline) and BD (bupivacaine + dexmedetomidine). Asterisks indicate the time points of a statistically significant difference (P < 0.05) when the groups were compared
DISCUSSION
The clinical evidence for the use of dexmedetomidine as an adjuvant to local anesthetic for peripheral nerve blocks was first published by Brummett et al. in several animal studies.[14,15,16,17] Under nerve stimulation guidance, Esmaoglu et al. used 40 mL of local anesthetic plus 100 μg of dexmedetomidine for axillary brachial plexus block.
Today, ultrasound guidance is the “gold standard” in peripheral regional anesthesia, enabling a reduction in local anesthetic dosage.[18,19] Ultrasound has brought about a revolution in terms of accuracy, predictability, and success rates. Although neurostimulation remains a useful technique, ultrasound guidance has dramatically improved nerve localization and offers several advantages. Although the requirement of a sound anatomical and theoretical knowledge is important, the use of ENV software incorporated in the newer ultrasound machines has maximized the success and efficacy of the technique. ENV (SonoSite, Inc. WA, USA) is a software that intensifies the brightness of the needle during ultrasound-guided procedures [Figure 5]. Therefore, to reflect the current clinical standard in this field, we used ultrasound guidance with ENV and low volume of local anesthetic along with a lower dose of dexmedetomidine compared with previous studies.
Figure 5.
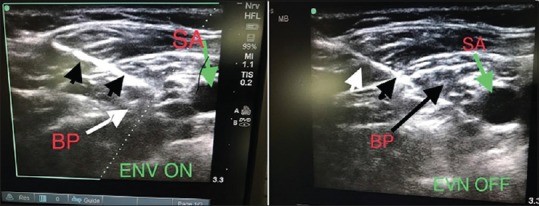
Enhanced Needle Visualization On and Off. SA: Subclavian Artery; BP: Brachial plexus: Green arrow: Subclavian artery; White and black arrow heads: Needle; White and black arrow: Brachial plexus
Dexmedetomidine is a potent α2 adrenoceptor agonist approximately eight times more selective toward the α2 adrenoceptor than clonidine,[6] thus decreasing the unwanted side effects of α1 receptors. α2 adrenergic receptor agonists mediate analgesia and sedation by mechanisms which are not fully understood but are likely to be multifactorial. Peripherally, α2 agonists produce analgesia by reducing the release of norepinephrine and causing α2 receptor-independent inhibitory effects on nerve fiber action potentials. Centrally, they produce analgesia and sedation by inhibition of substanceP release in the nociceptive pathway at the level of the dorsal root neuron and by the activation of α2 adrenoceptors in the locus coeruleus.[20] It has been shown that blockade of the hyperpolarization-activated cation current (Ih current) prolongs the duration of analgesia when dexmedetomidine is used as an adjuvant for nerve blocks.[15] As the Ih current is important to restore the nerve back to the resting potential, blockade of this current by dexmedetomidine will result in prolonged hyperpolarization, thereby hindering it to produce a new action potential. Prolonged hyperpolarization from blockade of the Ih current seems to be more distinct in the unmyelinated C fibers (pain) than in A α fibers (motor). Therefore, blocking the Ih current may have a more pronounced effect on pain than on motor response.[21]
CONCLUSION
We conclude that combining ultrasound guidance for plexus location and using dexmedetomidine as an adjuvant to bupivacaine allows the use of lower volume of bupivacaine and lesser dose of dexmedetomidine yet providing a shorter onset time and prolonged duration of the block.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We convey our sincere thanks to Mr. Goutham for helping us with the statistical analysis of the compiled data for the study.
REFERENCES
- 1.Cowlishaw PJ, Scott DM, Barrington MJ. The role of regional anaesthesia techniques in the management of acute pain. Anaesth Intensive Care. 2012;40:33–45. doi: 10.1177/0310057X1204000105. [DOI] [PubMed] [Google Scholar]
- 2.Flacke JW, Bloor BC, Flacke WE, Wong D, Dazza S, Stead SW, et al. Reduced narcotic requirement by clonidine with improved hemodynamic and adrenergic stability in patients undergoing coronary bypass surgery. Anesthesiology. 1987;67:11–9. doi: 10.1097/00000542-198707000-00003. [DOI] [PubMed] [Google Scholar]
- 3.Murphy DB, McCartney CJ, Chan VW. Novel analgesic adjuncts for brachial plexus block: A systematic review. Anesth Analg. 2000;90:1122–8. doi: 10.1097/00000539-200005000-00023. [DOI] [PubMed] [Google Scholar]
- 4.Singelyn FJ, Gouverneur JM, Robert A. A minimum dose of clonidine added to mepivacaine prolongs the duration of anesthesia and analgesia after axillary brachial plexus block. Anesth Analg. 1996;83:1046–50. doi: 10.1097/00000539-199611000-00025. [DOI] [PubMed] [Google Scholar]
- 5.Duma A, Urbanek B, Sitzwohl C, Kreiger A, Zimpfer M, Kapral S. Clonidine as an adjuvant to local anaesthetic axillary brachial plexus block: A randomized, controlled study. Br J Anaesth. 2005;94:112–6. doi: 10.1093/bja/aei009. [DOI] [PubMed] [Google Scholar]
- 6.Virtanen R, Savola JM, Saano V, Nyman L. Characterization of the selectivity, specificity and potency of medetomidine as an alpha 2-adrenoceptor agonist. Eur J Pharmacol. 1988;150:9–14. doi: 10.1016/0014-2999(88)90744-3. [DOI] [PubMed] [Google Scholar]
- 7.Memiş D, Turan A, Karamanlioǧlu B, Pamukçu Z, Kurt I. Adding dexmedetomidine to lidocaine for intravenous regional anesthesia. Anesth Analg. 2004;98:835–40. doi: 10.1213/01.ane.0000100680.77978.66. [DOI] [PubMed] [Google Scholar]
- 8.Abodedir MA. Adding clonidine or dexmedetomidine to lidocaine during Bier's block: A comparative study. J M Sci. 2008;8:660–4. [Google Scholar]
- 9.Esmaoglu A, Mizrak A, Akin A, Turk Y, Boyaci A. Addition of dexmedetomidine to lidocaine for intravenous regional anaesthesia. Eur J Anaesthesiol. 2005;22:447–51. doi: 10.1017/s0265021505000761. [DOI] [PubMed] [Google Scholar]
- 10.Kanazi GE, Aouad MT, Jabbour-Khoury SI, Al Jazzar MD, Alameddine MM, Al-Yaman R, et al. Effect of low-dose dexmedetomidine or clonidine on the characteristics of bupivacaine spinal block. Acta Anesthesiol Scand. 2006;50:222–7. doi: 10.1111/j.1399-6576.2006.00919.x. [DOI] [PubMed] [Google Scholar]
- 11.Esmaoglu A, Yegenoglu F, Akin A, Turk CY. Dexmedetomidine added to levobupivacaine prolongs axillary brachial plexus block. Anesth Analg. 2010;111:1548–51. doi: 10.1213/ANE.0b013e3181fa3095. [DOI] [PubMed] [Google Scholar]
- 12.Obayah GM, Refaie A, Aboushanab O, Ibraheem N, Abdelazees M. Addition of dexmedetomidine to bupivacaine for greater palatine nerve block prolongs postoperative analgesia after cleft palate repair. Eur J Anaesthesiol. 2010;27:280–4. doi: 10.1097/EJA.0b013e3283347c15. [DOI] [PubMed] [Google Scholar]
- 13.Bhana N, Goa KL, McClellan KJ. Dexmedetomidine. Drugs. 2000;59:263–8. doi: 10.2165/00003495-200059020-00012. [DOI] [PubMed] [Google Scholar]
- 14.Brummett CM, Amodeo FS, Janda AM, Padda AK, Lydic R. Perineural dexmedetomidine provides an increased duration of analgesia to a thermal stimulus when compared with a systemic control in a rat sciatic nerve block. Reg Anesth Pain Med. 2010;35:427–31. doi: 10.1097/AAP.0b013e3181ef4cf0. [DOI] [PubMed] [Google Scholar]
- 15.Brummett CM, Hong EK, Janda AM, Amodeo FS, Lydic R. Perineural dexmedetomidine added to ropivacaine for sciatic nerve block in rats prolongs the duration of analgesia by blocking the hyperpolarization-activated cation current. Anesthesiology. 2011;115:836–43. doi: 10.1097/ALN.0b013e318221fcc9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Brummett CM, Norat MA, Palmisano JM, Lydic R. Perineural administration of dexmedetomidine in combination with bupivacaine enhances sensory and motor blockade in sciatic nerve block without inducing neurotoxicity in rat. Anesthesiology. 2008;109:502–11. doi: 10.1097/ALN.0b013e318182c26b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Brummett CM, Padda AK, Amodeo FS, Welch KB, Lydic R. Perineural dexmedetomidine added to ropivacaine causes a dose-dependent increase in the duration of thermal antinociception in sciatic nerve block in rat. Anesthesiology. 2009;111:1111–9. doi: 10.1097/ALN.0b013e3181bbcc26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Marhofer P, Harrop-Griffiths W, Kettner SC, Kirchmair L. Fifteen years of ultrasound guidance in regional anaesthesia: Part 1. Br J Anaesth. 2010;104:538–46. doi: 10.1093/bja/aeq069. [DOI] [PubMed] [Google Scholar]
- 19.Marhofer P, Harrop-Griffiths W, Willschke H, Kirchmair L. Fifteen years of ultrasound guidance in regional anaesthesia: Part 2-recent developments in block techniques. Br J Anaesth. 2010;104:673–83. doi: 10.1093/bja/aeq086. [DOI] [PubMed] [Google Scholar]
- 20.Guo TZ, Jiang JY, Buttermann AE, Maze M. Dexmedetomidine injection into the locus coeruleus produces antinociception. Anesthesiology. 1996;84:873–81. doi: 10.1097/00000542-199604000-00015. [DOI] [PubMed] [Google Scholar]
- 21.Lönnqvist PA. Alpha-2 adrenoceptor agonists as adjuncts to peripheral nerve blocks in children – Is there a mechanism of action and should we use them? Paediatr Anaesth. 2012;22:421–4. doi: 10.1111/j.1460-9592.2012.03821.x. [DOI] [PubMed] [Google Scholar]