

Abstract
There are a significant number of students on maintenance medications for chronic diseases or with diagnoses that may result in medical emergencies requiring administration of medications in school. With passing of legislation in all 50 states allowing self-administration of emergency medications for allergic reactions and asthma, the landscape of medication use in schools is changing. These changes have raised questions about the need for legislation or policy development relating to self-carrying and self-administration of medications for other disease states, undesignated stock of emergency medications, and administration of medications by non-medical personnel. Medication administration in the school setting has become a complex issue, and this review will discuss current legislation related to medication use in schools and provide best practices for administering medications to children and adolescents while at school.
Keywords: drug therapy, pediatrics, school health services, schools, self-administration
Introduction
There are over 73 million children living in the United States, and approximately 19% of them have special health care needs, requiring prescription medications or other specialized therapies for “chronic medical, behavioral, or developmental conditions.”1,2 Medical advancements are allowing children with chronic diseases to live longer and with a higher quality of life. These advances, combined with the implementation of state and federal laws, now allow many of them to be present in classrooms with their peers. With the increase in the number of students with chronic diseases and complex medical histories, there is an increasing need to administer medications in school.
Traditionally, the role of providing direct care to students, including administering medications and assisting with acute medical problems, has fallen to the school nurse.3 Unfortunately, budget cuts have caused many schools to forgo staffing of full-time school nurses who are able to provide care for students with medical needs. Even when nurses or other trained professionals are present at the school, there are instances when time is of the essence to provide lifesaving treatments, and administration of medication without the assistance of trained health care professionals may be required. Many states have instituted regulations allowing other school staff members to administer medications after professionally guided training has been completed.4
As of October 2014, all 50 states and the District of Columbia have laws or statutes allowing students with a diagnosis of asthma or life-threatening allergic reactions to possess and self-administer emergency medication.5 While these laws have helped to advance the care and safety of children with asthma and allergies while at school, these are not the only disease states that may require medication administration throughout the day or in emergencies to help prevent serious complications or even death. Chronic conditions such as epilepsy, diabetes, and cystic fibrosis, or situations such as opioid overdose may also require that medication be given at school. Medication administration in the school setting has become a complex issue. This review will discuss examples of conditions where medication use in school is necessary and outline best practices for administering medication to students.
Asthma
According to data from the CDC, as of 2016 more than 6 million children in the United States had a diagnosis of asthma. Roughly 87% of them were between 5 and 18 years of age and would presumably be attending school. The CDC data showed that over 3.2 million children had at least 1 documented asthma attack in 2016. In the same year, 209 deaths of children were attributed to asthma diagnoses.6 Complications and deaths from asthma can be prevented with proper administration of asthma controller medications, early recognition of asthma attacks paired with prompt administration of inhaled, short-acting bronchodilators.
On the basis of current recommendations from the Global Initiative for Asthma Report, children with persistent asthma may be prescribed an inhaled corticosteroid with or without a long-acting beta-agonist and/or a leukotriene receptor antagonist as controller medications.7 These medications can typically be given at home by scheduling them before and/or after school. However, some school districts have started to include controller medications (e.g., inhaled corticosteroids) on students' asthma action plans for administration during the school day to improve adherence.8 The CDC reported that although 55% of children with asthma are prescribed controller medications, only 25% use them regularly as prescribed, while 68% reported regularly using their rescue medication.9 This presents a potential opportunity for schools to impact the adherence and health of their students with asthma, as studies in large school districts have demonstrated that for some children, school-based, supervised inhaled corticosteroid therapy can help improve asthma control.10
A joint statement of health and school-based organizations recommended that schools implement comprehensive plans for asthma management. The group recommended that schools develop ways to address environmental triggers of asthma that children can be exposed to at school. The statement also advocated for asthma action plans for each student with asthma, education for school staff, development of emergency protocols, and the ability for students to self-administer their short-acting bronchodilator medication.11 An asthma exacerbation can occur at any time owing to potential exposure to triggers such as respiratory infections, pollution, allergens such as dust and pollen, exercise/stress, or cold air.12 Triggers may vary from child to child, but every asthmatic child has specific triggers for his or her asthma and should receive education about them.13 In addition to the student and his/her parents or guardians, school health staff should be familiar with the child's triggers and symptoms of acute asthma to identify acute episodes and determine when additional medical assistance is needed. The variety of asthma triggers and potential severity of the triggered response make it necessary for students with asthma to have a short-acting bronchodilator readily available to them at all times.7,14
In 2004, Congress passed the Asthmatic Schoolchildren's Treatment and Health Management Act (Public Law 108-377). This act provided incentives for states that required schools to allow students with a previous diagnosis of asthma or severe allergy to self-administer medications for urgent situations related to asthma or anaphylaxis.15 Since that time, all 50 states and the District of Columbia have instituted laws that allow children to carry their short-acting bronchodilator while in school.16 However, individual state law specifics can vary resulting in a lack of consistency in school policies allowing students to self-carry their medications. The AAP and American Lung Association recommend allowing responsible, age-appropriate students to carry a short-acting bronchodilator with them at school.16,17 Readiness to self-carry should be assessed by the child's health care provider. The importance of a collaborative decision between the school nurse, the provider, and the patient's family about the appropriateness of self-carrying and self-administration for an individual student cannot be overstated.16,17 Not all students will exhibit the level of responsibility necessary to be candidates for self-carry and/or self-administration. Children who are mature enough to self-carry must be able to understand and recognize the signs and symptoms of an asthma exacerbation, understand and comply with school policies for self-carry/self-administration, as well as demonstrate proper technique when using their inhalers.11,16,17 The school's self-carry/self-administration policy should address the need for students to make school staff aware when an inhaler is used for rescue, to ensure that the situation can be appropriately monitored in case additional intervention is necessary.17 Even when a student is approved for self-carrying, parents/guardians should still provide an additional inhaler that can be kept in a secure location at the school in case the child forgets or loses his or her inhaler.
To optimize asthma management at school, it is imperative that students have reliable access to rescue medications. Even with progress being made in terms of students' ability to self-carry and self-administer short-acting bronchodilators, there are still significant barriers for many students when it comes to accessing rescue medication. A school-based, asthma medication study of elementary school students in Alabama demonstrated that less than 15% of students had albuterol readily available at school despite having policies in place that permitted students to possess short-acting bronchodilators.18 While the data were collected in 2005 and may not accurately reflect the status of albuterol access in schools today, it is consistent with the results of a survey from the United Kingdom that reported 86% of students with asthma had at some point been without an inhaler at school.19 School health staff may run into difficulties with obtaining medication from parents, students forgetting or losing their inhaler, or the inhaler running out or expiring. Other issues such as lack of insurance, limited finances to pay for a second inhaler for school, or difficulty obtaining a prescription owing to lack of a primary care physician or site of asthma care may also be contributing factors.18–20 Regardless of the cause, if a student does not have access to his/her inhaler during an asthma attack and a parent cannot quickly bring it to school, the school health staff are left no choice but to contact emergency services. These issues highlight the importance of legislation allowing, or preferably requiring, implementation of stock inhaler programs in schools.
A stock bronchodilator inhaler (e.g., albuterol) is a school-owned inhaler that is used with individual or disposable spacers, so it can be used for multiple students.18,21 Stock bronchodilator inhalers provide a back-up option for children who do not have access to a personal inhaler, regardless of the reason. It allows for rapid intervention during acute asthma episodes to prevent the need for escalation in care, which may allow children to remain in school.18 Data collected from a large school district in Arizona showed that in the year a stock inhaler program was implemented, the stock inhaler was used by 55 students for 222 separate events. The authors also reported a 20% decrease in 911 calls and 40% decrease in emergency medical service transports during the implementation year compared to the year prior to implementation. Nurses indicated that they were comfortable using the stock inhaler and felt they had better outcomes for their students but voiced concern that they may be open to liability if a stock inhaler was used in an emergency situation without a documented physician diagnosis. In addition, they reported use of the stock bronchodilator inhaler for school staff as well as for some non-emergent situations such as prior to exercise when a student had lost or forgotten his/her inhaler.21 All of these issues should be considered when developing stock rescue inhaler programs and policies. Ability to develop and implement stock bronchodilator inhaler programs in schools may vary by state due to differences in laws and legislation.
To encourage and support the development of progressive asthma and stock inhaler policies in schools, the School-Based Asthma Management Program Act, HR 4662, was introduced in the House of Representatives in March 2016. The proposed bill intended to expand the criteria for federal asthma grant preference set forth in the School Access to Emergency Epinephrine Act to include stocking and staff administration of asthma rescue medications and development of school-based asthma management programs.22 This bill was endorsed by the American Academy of Allergy, Asthma and Immunology, the American Academy of Pediatrics, and the National Association of School Nurses; however, the bill did not pass before the conclusion of the 114th Congress.22,23 A similar bill, HR 2285, was introduced in the House on May 2, 2017. Known as the School-Based Respiratory Health Management Act, this bill sought to increase the preference given to states meeting the specified criteria when awarding allergy and reversible lower airway disorder–related grants. Additional preference would have been given to states that required schools to stock allergy and reversible lower airway disorder rescue medications (at a minimum, short-acting bronchodilators), allow trained school staff to administer those rescue medications to any student reasonably believed to have allergies or a reversible lower airway disorder, and have a comprehensive school-based allergy and reversible lower airway disorder management program in place.24 While this bill garnered a significant amount of support, including 40 cosponsors, it failed to pass before the conclusion of the 115th Congress. It is anticipated that similar federal legislation will be introduced in the 116th Congress; however, several states already have laws or guidelines allowing schools to stock bronchodilators for children with asthma. As shown in Figure 1, 15 states currently have stock bronchodilator laws or guidelines in place.25 While lack of a state law does not prevent schools from implementing a stock bronchodilator inhaler program, state laws can provide standards for schools that are developing these programs and can address the issue of liability by indemnifying school staff for good faith use.21,25 Advocacy on the part of parents, physicians, school health staff, and other medical professionals may facilitate passage of similar laws in the remaining states. In the interim, the American Lung Association has developed a model policy on stock bronchodilators that can aid schools in developing their own stock inhaler policies and protocols.26
Figure 1.
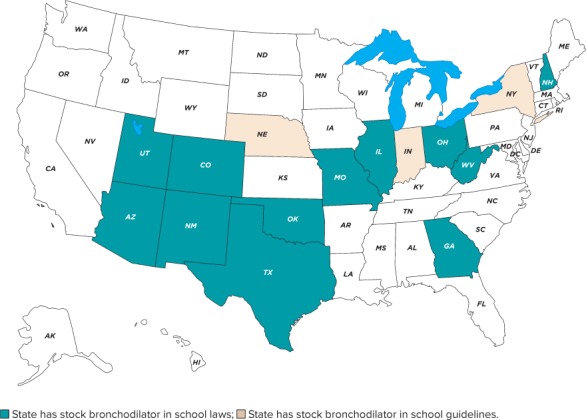
American Lung Association and Allergy and Asthma Network: state map of stock bronchodilator in school laws and guidelines.
Best practices for asthma medication use in schools should consist of appropriate medication access, administration, and documentation policies, guidance or training of school staff, and guidelines for emergency medication use and management. Schools should have guidelines and practices that permit appropriate access to rescue medication from school staff for younger children and allow older, responsible children to self-carry and administer their rescue medications. The self-carry/self-administration policy should require that students report any use of an inhaler for rescue to school staff to allow them to appropriately monitor the situation and intervene if needed.17 In addition, schools should have a stock inhaler program that permits use of a stock bronchodilator for students or school staff when it is deemed necessary.16 All asthmatic children attending school should have an asthma action plan on file with the school and should be familiar with what it entails.7,14 The asthma action plan should include signs and symptoms to be aware of, appropriate treatment steps, documentation of readiness to self-carry an inhaler, and emergency contact numbers.7,12,27 For those children who may benefit from supervised inhaled corticosteroid therapy, this should also be included in the asthma action plan. Schools should have guidelines on chronic medication use, including needed documentation, training of school staff, and a process for consistent communication between health care providers, students and their families, and school staff. There are numerous resources available to assist schools with developing and implementing these best practices. For example, the American Lung Association has developed a program called the Asthma-Friendly School Initiative. This program can help schools develop and maintain an asthma-friendly environment at school for students and the community.28 Information on this and other resources for schools (e.g., action plan templates and model policies) can be found in the Table.
Table.
Additional Internet Resources
AAAAI, American Academy of Allergy, Asthma & Immunology; NASN, National Association of School Nurses
Table.
Additional Internet Resources (cont.)
AAAAI, American Academy of Allergy, Asthma & Immunology; NASN, National Association of School Nurses
Anaphylaxis
Anaphylaxis, “a severe, potentially fatal, systemic allergic reaction,” most commonly results from exposure to certain foods, insect stings, latex, medications, or immunotherapy. 30, 31 Contact with the allergen sets off a profound, IgE-mediated systemic reaction that can result in symptoms from multiple organ systems including the integumentary (e.g., urticaria, flushing, angioedema), respiratory (e.g., laryngeal edema, bronchospasm), gastrointestinal (e.g., nausea, vomiting, abdominal pain), and cardiovascular systems (e.g., tachycardia, hypotension).30 First-line treatment is the immediate administration of intramuscular epinephrine injection.31 Delays in the administration of this lifesaving medication can have fatal consequences.
When anaphylactic reactions occur in school, it is essential for students or staff to have ready access to epinephrine auto-injectors. The Asthmatic Schoolchildren's Treatment and Health Management Act of 2004 prompted the passing of laws protecting the students' right to possess and self-administer anaphylactic medications in all states. Despite these laws, many students remained at significant risk because approximately 24% of anaphylactic reactions in schools occur in children with no documented history of allergy.32
To maximize access to lifesaving medication for all children having anaphylactic reactions in school or while involved in school activities, the School Access to Emergency Epinephrine Act was passed in 2013. This law provided incentives for states that enacted legislation allowing trained school staff to stock epinephrine and administer it to any student of the school reasonably believed to be having an anaphylactic reaction.33 While all states now have legislation addressing the issue of an undesignated stock of epinephrine, the map in Figure 2 shows that most states allow schools to stock epinephrine, but do not require them to do so.34 Therefore, it is not guaranteed that individual schools have a stock of undesignated epinephrine available or an anaphylaxis action plan in place.
Figure 2.
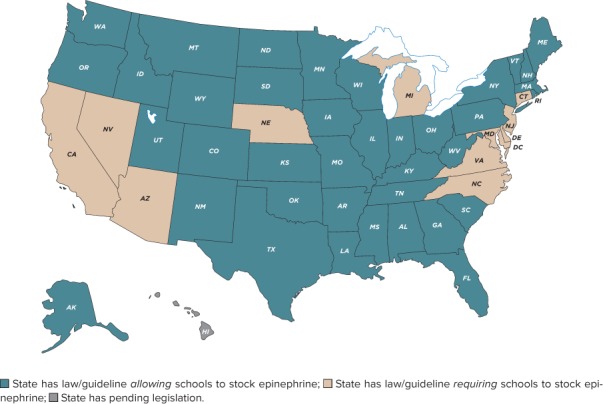
Food Allergy Research and Education (FARE): school access to epinephrine map.
There are lifesaving implications when schools take appropriate steps to prepare for anaphylactic emergencies. Best practices for managing anaphylaxis in school include having an anaphylaxis action plan in place, a ready-to-administer supply of epinephrine, and staff appropriately trained to recognize the early signs of anaphylaxis and administer the appropriate dose of epinephrine when needed. Schools should stock undesignated epinephrine auto-injectors and train staff to recognize and respond to anaphylaxis when it occurs. The school should maintain a supply of both the 0.15-mg and 0.3-mg auto-injectors if appropriate, based on the size of the students, visitors, and staff who may be present. When using epinephrine auto-injectors for anaphylaxis, the recommended dose is 0.15 mg for a child who is 15 to 30 kg (33–66 lb) and 0.3 mg for an adult or a child > 30 kg (> 66 lb).35 The school's anaphylaxis action plan should clearly indicate the appropriate dose of epinephrine that should be administered. In addition to the weight-based dosing, some states and many schools also include age or grade cutoffs to provide additional guidance. For example, in the Toolkit for the Administration of Epinephrine and Albuterol/Levalbuterol in the School Setting from the Georgia Department of Public Health, the recommendation is as follows: “For students in second grade or below or if less than 66 lbs, use white label epi-pen jr 0.15 mg. For adults and students in third grade or above or if more than 66 lbs use yellow label epi-pen 0.3 mg.”36 Students with a previous diagnosis of anaphylaxis or severe allergy should have an individualized anaphylaxis action plan on file with the school. The anaphylaxis action plan should include signs and symptoms to watch for, history related to previous anaphylactic reactions or concomitant respiratory conditions (e.g., asthma), appropriate treatment steps, documentation of ability to self-carry an epinephrine auto-injector and inhaled bronchodilator (if child also has asthma), designation of an adult who can administer the medication if the child is severely symptomatic or otherwise unable to self-administer, and emergency contact information.37–39 There are numerous resources available to assist with implementation of these best practices. Although there are several anaphylaxis emergency action plan templates available from professional allergy and anaphylaxis organizations, there are significant variations in the included content and treatment recommendations.37–39 To provide a more comprehensive and standard approach, the AAP developed a universal allergy and anaphylaxis emergency plan and offers it as a tool for health care providers and school health professionals to use when preparing anaphylaxis action plans for use in school.38,39 In addition, some manufacturers of epinephrine auto-injectors have developed programs that may provide free auto-injectors, training devices, and staff training materials for schools. Links to some of these resources can be found in the Table.
Seizures and Epilepsy
A significant number of children who suffer from seizure disorders such as epilepsy are unable to achieve complete seizure control with maintenance medications, and are therefore at risk of having a breakthrough seizure episode while in school or attending a school event.46 An anticonvulsant or abortive medication is recommended for seizures lasting longer than 5 minutes in most children, but may be recommended as soon as seizure activity begins in others.47 The longer the seizure is allowed to continue, the more difficult it will be to break, and the more likely it is to progress to refractory status epilepticus.48 Therefore, the sooner an abortive medication, such as a benzodiazepine, is given the better the expected outcome.
There are unique considerations to keep in mind when choosing the appropriate benzodiazepine for inclusion in a student's seizure response plan. One of the medications used most frequently for seizure cessation is diazepam rectal gel. While it is premeasured, easy to administer, and very effective, it may not be ideal for a school setting. It requires partially undressing the child and inserting the tip of the syringe into the rectum for administration. In a school setting, nurses or school staff may be reluctant to administer the medication when privacy is unattainable or other children are present.49,50 Additionally, school staff members may feel uncomfortable performing what may be considered an invasive and very personal procedure on a child.50 The laws regarding who may administer rectal medication in schools vary by state.
For instance, in California, non-medical school staff volunteers may administer rectal diazepam when providing emergency medical assistance after receiving training from a physician, physician assistant, credentialed school nurse, registered nurse, or a certified public health nurse.51 Other states, such as Alabama, will not allow any staff members other than the school nurse to administer rectal medication, which can be an issue, particularly when nurses may not be on site at all times.52 In these instances, it may be preferable to use other routes of administration. Some possibilities include buccal administration of midazolam oral solution, buccal administration of clonazepam orally disintegrating tablets, or intranasal administration of injectable midazolam via a mucosal atomization device.53–55
Students and their families should work with the primary care provider or neurologist and the school nurse to design a seizure action plan that is acceptable to the student and can be legally and reasonably accommodated by the school. The seizure action plan should include seizure triggers or warning signs, the seizure type and a description of the child's seizure activity, the typical length and frequency of seizures, the child's response after a seizure, a list of the child's daily seizure medications, whether or not the child has a vagus nerve stimulator, and an emergency seizure protocol.56,57 The emergency seizure protocol should define a seizure emergency and specify any first aid that should be provided, who should be contacted (e.g., nurse, emergency medical services), magnet use for children with a vagus nerve stimulator, and any medication that should be given, including the dose, frequency, and who will administer the medication.56,57 Sample plans and links to other resources can be found in the Table.
The issue of stocking undesignated benzodiazepines in schools has not yet become a topic of discussion, but there are situations where it may be beneficial. An individualized seizure action plan and medication supply is always preferred for students with a previously diagnosed seizure disorder; however, their parents may have difficulty obtaining sufficient supplies of diazepam rectal gel to keep separate supplies at all the necessary locations (e.g., home, school, and daycare) or there may be delays replacing the supply once it is used or expired. In the event that the student's individual supply is expired or unavailable, having an undesignated stock of diazepam rectal gel that could be used may be invaluable, particularly for schools in rural areas, where response times of first responders may be longer. While stocking controlled medications in schools would be more complex, the benefit of having benzodiazepines available to abort seizures is significant and would therefore be worthwhile to consider.
Cystic Fibrosis
While many of the policies and laws addressing medication administration at school have centered on disease states that require acute or emergent intervention, there are some complex childhood diseases that require access to select chronic and preventive therapies throughout the school day. The chronic management of one such disease, cystic fibrosis (CF), may include non-pharmacologic therapies, medications, nutrition modification, or other accommodations while in school.
Cystic fibrosis is a chronic, progressive disease caused by inherited mutations in the cystic fibrosis transmembrane conductance regulator, or CFTR, gene.61 The CFTR gene encodes the CFTR protein, a chloride channel responsible for maintaining an appropriate balance of fluid and electrolytes in various tissues throughout the body, including but not limited to the lungs, sweat glands, pancreas, gastrointestinal tract, and reproductive system.62,63 In patients with CF, an absent or dysfunctional CFTR prevents the normal movement of electrolytes into and out of the epithelial cells, leading to the production and build-up of thick mucus in the affected organs, significantly affecting their function.61,62
There are over 30,000 people with CF living in the United States, and just under half of them are children. Most patients with CF are diagnosed by 2 years of age or even earlier, since many CF mutations can now be identified on the newborn screen.62 Early detection allows initiation of appropriate and targeted management to slow disease progression and prevent complications before they occur. While there is still no cure for this disease, earlier detection and strict adherence to medication regimens and respiratory therapies allow CF patients to live much longer than previous expectations.62–64 According to the Cystic Fibrosis Foundation's patient registry annual report, the median life expectancy for an infant born in 2017 and diagnosed with CF is roughly 46 years.64
There are a significant number of maintenance medications that children with CF require on a daily basis to minimize progression of the disease and optimize function of the organ systems affected.62,63,65 Airway clearance using chest physical therapy, a flutter device, or a vest is also a key component of maintenance therapy and may be needed during school hours in some children.62,63,65 Not all medications should be used in the school setting; however, there are select acute and chronic medications that should be accessible by children with CF. Medication access in schools for children with CF should consist of those necessary for acute situations or emergencies as well as some chronic medications necessary for appropriate nutrition (e.g., pancreatic enzymes). Children with CF may benefit from inhaled beta-2 agonists if they have a component of airway hyperresponsiveness and may experience bronchospasm.65 Oral pancreatic enzyme replacements should be taken before all meals and snacks, including those throughout the school day, to improve digestion and absorption of nutrients.63,66–69 If school policy allows, it is preferable to allow students who are mature enough to administer their own enzymes. Most children with CF have been taking enzymes for many years and are able to take them on their own. It is one way that even young children can independently participate in their care.63,67 As with asthma, guidelines for the self-carrying and administration of medication for CF can vary from school to school, and the ability to self-carry should be determined on the basis of communication between the family, school, and health care provider. In addition, children with CF generally require high-calorie meals and snacks that include foods high in protein and fat, to compensate for some of the malabsorption. As such, availability to higher-calorie foods, such as whole milk, should be permitted for children with this condition. Communication between the child's family, health care provider, and school is key in assuring availability and access to needs specific to a child with CF.
In addition to medication access and nutritional accommodations for students with CF, there are other aspects of life with CF that may affect them at school and should be considered. Coughing is common in people with CF and it is helpful in clearing mucus from the lungs, so it should not be discouraged. In addition, exercise is important to strengthen respiratory muscles and clear mucus from the lungs.66,67 Although they may tire more easily than their peers, students with CF should be encouraged to exercise and participate in physical education.63,66,67 However, they are also at high risk of dehydration and electrolyte imbalance, due to excessive salt loss through perspiration.67 During strenuous exercise or during hot weather, patients with CF may require salty snacks or salt supplements in addition to maintaining adequate hydration by drinking every 20 to 30 minutes.63,66,67 It is essential that school staff be educated about these needs, and that students be granted permission to have the necessary drinks and snacks, even when outside of normally scheduled times. Additionally, since many children with CF have malabsorption of nutrients, they should be provided additional bathroom access owing to the potential for more frequent bowel movements.
Given the various accommodations needed to ensure students with CF can meet their health care needs without impacting their ability to learn, best practices for medication use and health maintenance of CF in school should also be multifaceted. Frequent communication between the student's family, school health staff, and health care professionals is imperative. A 504 plan or an individualized education plan (also known as an individualized education program or IEP) should be developed prior to the start of school.63,70 The appropriate plan will be chosen depending on the types of accommodations needed by the student, and whether the student qualifies for those accommodations under Section 504 of the Rehabilitation Act of 1973, for 504 plans, or the Individuals with Disabilities Education Act (IDEA), for IEPs. The selected plan should clearly address the student's medications, nutritional needs, airway clearance therapy, exercise guidelines, and other necessary accommodations including infection control precautions, bathroom privileges, etc.63,70 While a 504 plan can address these types of accommodations, it cannot address any educational accommodations that may be necessary. A student with CF may qualify for an IEP and educational accommodations under the “other health impairment” qualification of the IDEA if the disease or its consequences impact his/her ability to learn.63,71 Cystic fibrosis often impacts a student's ability to learn owing to decreased stamina from the disease, interruptions to learning for medication administration, missed class time for medical appointments, frequent exacerbations, and/or prolonged hospitalizations when the student may be out of school for an extended period of time.63,70 Proactively putting an IEP in place that outlines a plan for getting necessary homework or tutoring during prolonged absences, as well as addressing accommodations like audio or videotaped classes or exceptions to attendance policies, can prevent unnecessary delays and difficulties when exacerbations or hospitalizations do occur.63,70 Links for information on IEP and 504 plans as well as additional resources for families are provided in the Table.
Diabetes Mellitus
According to the 2017 National Diabetes Statistics Report, nearly 18,000 children with type 1 diabetes and over 5000 children with type 2 diabetes are diagnosed each year.73 The management of diabetes involves dietary restrictions, physical activity, and medication management. Unlike other chronic disease states, diabetes requires medication to be given during the day, along with testing of blood glucose levels while in school. The proper management of a child's blood glucose level is important in preventing short-term complications such as hypoglycemia and hyperglycemia, as well as the long-term complications of nephropathy, neuropathy, and retinopathy.
Diabetes is considered a disability, and children are protected from discrimination in school under the Americans with Disabilities Act, the Rehabilitation Act of 1973, and the Individuals with Disabilities Education Act.74 These regulations require schools to make accommodations for children with diabetes to allow them to participate in all school activities. However, in some states only health care professionals can assist students in the administration of insulin, while many do allow non–health care professionals to administer emergency glucagon.75
Diabetes management in the school setting can be challenging because it involves children in various developmental stages. Children < 5 years of age are at a developmental stage where recognition of symptoms of hypoglycemia and ability to manage their diabetes may be challenging. Children at this age can still be involved with their care, for example, by choosing which finger to use for glucose testing as well as their insulin injection site.74 At the elementary school level, the ability for children to manage their diabetes care will vary based on their maturity level and when they were diagnosed with diabetes. First and foremost, children must be willing to participate in and/or provide their own care.74,76 Schoolchildren should be allowed to self-administer their insulin under supervision if deemed appropriate by their parents, the school nurse, and the diabetes care provider. Middle-school and high-school students who show the maturity and knowledge of their diabetes should also be encouraged to self-manage their diabetes in school.74 A note from the diabetes care provider outlining the child's ability to self-administer or self-manage his or her diabetes while at school should be included in the Diabetes Medical Management Plan (DMMP). Parents or caregivers should provide the school with all the supplies needed to manage their child's diabetes, including but not limited to insulin, needles, syringes, glucose tablets, glucagon, sharps container, and glucose monitor. In addition, children who are capable of self-managing should be allowed to carry these supplies with them while in school.
According to the recommendations from the American Diabetes Association, all children with diabetes should have a DMMP on file with their school.74 The DMMP should include all routine and emergency care and provide the school with the roles and responsibilities of all the participants.77 At a minimum, the DMMP should include specifics on the following: blood glucose monitoring, insulin administration, meal time considerations, symptoms of hypoglycemia/hyperglycemia, checking for ketones if applicable, physical activity limitations, and emergency plans and contacts.74 Some schools may elect to or are required to use an Individualized Health Care Plan (IHP) and/or an Emergency Care Plan. The IHP and/or Emergency Care Plan should be based on the DMMP. Of note, some children may also need a 504 Plan or IEP on file with the school when further services, aids, or modifications are needed to make sure children with diabetes have access to all school activities without impacting their ability to learn.77
The AAP recommends that all schools have a minimum of 1 full-time school nurse to help with medical management of children in the school setting.3 Unfortunately, some schools are not able to have a full-time school nurse on staff or may need more than 1 school nurse on staff to meet the needs of the students. As a result, other school professionals may be called upon to help manage a child's diabetes. Many professional organizations have developed resources to help schools with comprehensive staff training in diabetes care. These resources, as well as additional resources for families, can be found in the Table.
Opioid Overdose/Drug Abuse
In recent years, there has been a significant increase in the number of fatalities involving opioid pain relievers or illicit opiates such as heroin. The Substance Abuse and Mental Health Services Administration National Survey on Drug Use and Health in 2015 reported that there were 2.2 million current illicit drug users between the ages of 12 and 17 years. Of those, 276,000 reported misusing pain relievers within the past month.83 In the 2017 Monitoring the Future study, roughly 1 in 50 high-school seniors reported non-medical use of hydrocodone/acetaminophen and 1 in 37 reported non-medical use of extended-release oxycodone within the last year.84 When opioids are used in high doses or for non-medical reasons, the risk of severe respiratory depression increases significantly. If not reversed, severe opioid-induced respiratory depression can lead to respiratory arrest and may be fatal. With the significant number of school-age and adolescent children using illicit drugs or medications for non-medical reasons, it is essential that schools be prepared to encounter and respond to students with opioid overdose or respiratory depression.
One of the strategies for preventing fatalities from opioid overdose is the rapid administration of naloxone.85 Historically, naloxone injection was given to reverse the respiratory depressive effects associated with opioid overdose. This required emergency medical personnel to be present to supply and administer naloxone; however, fatalities from opioid overdose have occurred while waiting for first responders to arrive. Two recent additions to the market, the naloxone auto-injector and naloxone hydrochloride nasal spray, are specifically designed for ease of administration and would be considerably easier for non-medical personnel to administer during an emergency. One dose of naloxone nasal spray should be given immediately, by spraying into 1 nostril, and emergency services should be contacted. If the child does not respond, or the respiratory depression returns, additional doses may be given every 2 to 3 minutes in alternating nostrils.86 This simple intervention may reverse respiratory depression, at least temporarily, thus buying time until emergency personnel arrive. The availability of these new, simpler alternatives may significantly reduce fatalities related to opioid overdose, particularly in rural areas where access to medical care may be limited. In some states or school districts, there are restrictions in place that allow only the school nurse to administer injections; however, the nurse may not be on-site full-time or may be split between different schools in the district. Naloxone nasal spray may be ideal in those situations.
In an effort to combat the opioid crisis, the Clinton Foundation and Adapt Pharma have joined together in the Clinton Health Matters Initiative that offers a free carton of naloxone nasal spray to every public high school in the United States.87 In addition, the National Association of School Nurses have been given a grant to develop and disseminate educational materials to school nurses, students, and their families.87 Opioid abuse has the potential to go unrecognized until a significant overdose occurs. Having school staff trained to recognize the early signs of opioid toxicity and having naloxone available in the school will very likely save numerous lives. Information on obtaining naloxone for your school and other educational materials is available in the Table.
Over-the-counter Products
The use of over-the-counter (OTC) medications, including dietary supplements, may be a challenge for schools, owing to the lack of a prescribed indication, dose, route, frequency, or duration for a given child. However, ease of access to treatment with OTC medications can result in symptomatic improvement, which may help enable learning and decrease disruption in the classroom. Additionally, most OTC products, when used appropriately, are relatively safe with regard to adverse drug effects. One problem with OTC medication use in the school setting involves difficulty in obtaining physician permission or orders for short-term use. Liability is another significant concern that schools face when offering to use OTC medications in students. The safety of students and security of medication supplies are important issues that also need to be evaluated. When considering the use of OTC products in their students, school personnel should consider risk versus benefit for each child.17
As with many medication-use policies in schools, the use of OTC medications in this setting can vary, based on state or school district-specific standards. For example, some schools hold the same policies for both OTC and prescription medications, while others permit the use of OTC medications for students with parental permission alone (i.e., no physician order needed). It is recommended that schools or school districts have medication-use policies specific to both OTC and prescription medications.
There are a number of best practices to consider when developing and implementing OTC medication policies in schools. The AAP recommends that schools develop standing protocols or orders with the school district's medical director that permit a 1-time verbal permission by parents for select OTC medications such as acetaminophen.17 The use of OTC products in schools should be limited to those that are necessary to treat acute issues such as pain, fever, and allergies. Over-the-counter multivitamins or dietary supplements that may otherwise be given outside of school hours should not be permitted, unless they are deemed medically necessary as documented in writing by the child's physician. Schools should maintain an updated medication list for students, whenever possible, that can be used to screen for possible drug-drug interactions with OTC medications.17 The AAP also recommends that schools require a physician/prescriber order for the use of OTC cough/cold medication in children younger than 6 years of age owing to data demonstrating lack of efficacy and greater risk versus benefit of these medications in this age population.17 The duration of OTC medication use in school should be for the shortest duration possible. If more than a 1-time administration is permitted, school policy should specify a limited duration of use for OTC medications. Finally, in the event that a child needs to receive an OTC medication for an extended period, schools should require a physician/prescriber order for proper oversight and instruction.17
General Recommendations for Best Practices
The AAP Council on School Health developed guidance recommendations for the administration of medications in the school setting in 2009, which were also endorsed by the American School Health Association.17 In addition, the AAP has issued guidance specific to medical emergencies and the management of food allergies in schools92,93 Many of these recommendations are addressed in the following best practice recommendations.
In general, medication-use practices and policies in schools can vary by school, district, and state. Universally, however, school policies should focus on optimizing the safety and health of children while taking into account the challenge of limited resources for the provision of health services in schools. Organizations such as the National Association of School Nurses recommend that school districts develop policies and procedures that “focus on safe and efficient medication administration” for prescription and non-prescription medications as well as medications being used off-label.94 Off-label medication use, although common in pediatric care, is an area that has raised additional concern and discussion amongst school health staff owing to concerns for safety and the risk of liability. The variety and number of medications seen in schools have increased over time. School district policies and regulations should be routinely updated to reflect the changes and trends in pediatric health care in order to support continuity of care between health care provider, caregiver, and the school community.17,94
School Health Staff. The presence of a full-time licensed registered nurse in each school is highly encouraged; however, the limited financial resources in school districts can hinder the ability to provide this. It is important to provide comprehensive and ongoing training for all school staff, outlining the signs and symptoms of common pediatric emergencies, the location of both individual student action plans and general school emergency action plans, and the school's policies pertaining to emergency medication administration. Using untrained school staff to administer medications in schools can increase both risk and liability. Thus, if unlicensed staff members are to be delegated the task of medication administration in schools, the AAP, American Nurses Association, and National Association of School Nurses recommend that they be trained and supervised by a registered nurse.17 These individuals, referred to as unlicensed assistive personnel (UAP), should have the “knowledge, skills, and composure” to administer medications or assist with other routine health duties under the guidance of a licensed registered nurse.17 It is preferred that UAP who will be assigned medication-related tasks be members of the school health staff (e.g., health aid/assistant); however, non-medical school staff members (e.g., teachers) may also be chosen.17 The school nurse is responsible for selecting and training UAP. Delegation of duties as well as training and assessment of UAP is an ongoing process and should be completed by the school nurse at multiple times throughout the year. Delegation of nursing responsibilities such as medication administration should follow outlined school policies and local and/or state practice regulations. Continuing education and training is recommended for all members of the school health staff.17 Such education and training can be offered through state school nurse organizations as well as through universities and affiliated nursing schools.
Use of a 504 Plan. To help ensure that appropriate medication administration is provided in the correct manner no matter who is administering the medication, it is recommended that a 504 plan be developed. Section 504 is part of the Rehabilitation Act of 1973 that allows students with disabilities to have access to the same education as peers without disabilities. A 504 plan is used as a blueprint for services or accommodations needed in the learning environment to meet the needs of the child. Students qualify for protection under Section 504 if they have a physical or mental impairment that substantially limits 1 or more major life activities (e.g., breathing, walking, learning). A physical or mental impairment is defined as any physiological disorder or condition that affects 1 or more of the body systems including respiratory, neurological, or cardiovascular. Students are evaluated to determine if they meet the requirements of Section 504. Once they are deemed eligible, students can continue to receive services as long as they continue to meet the qualifications outlined in Section 504. If a child meets eligibility requirements, a 504 plan is developed by a team of individuals familiar with the student and 504 plans. The child's parent or guardian, general and special education teachers, and principal are key participants, and it is recommended that they take part in the process. The student's physician may also be asked to be involved to provide recommendations or documentation of the disability. There are no specific requirements for what must be included in a 504 plan, but a plan should include specific accommodations needed (e.g., ability to self-administer medications, emergency medication administration), who will provide those services, and who will implement the plan. While the rules may vary by state, 504 plans are typically revised yearly, and the student is reevaluated for eligibility every 3 years.95
Use of an IEP. To ensure that the school meets the health and educational needs for each child, it is recommended that IEPs be developed prior to the start of the school year for students who qualify.70 The IDEA is a law that ensures students with disabilities have access to a free and appropriate public education as well as any special education or other services necessary to meet their needs.96 IEPs are used to clearly identify services or accommodations that are needed in the learning environment to remove barriers to a student's education.97 The IDEA requires schools to develop IEPs for all students who qualify as having a disability. Under IDEA, a child is considered to have a disability if he/she has “an intellectual disability, a hearing impairment (including deafness), a speech or language impairment, a visual impairment (including blindness), a serious emotional disturbance, an orthopedic impairment, autism, traumatic brain injury, another health impairment, a specific learning disability, deaf-blindness, or multiple disabilities” and “by reason thereof need special education and related services.”71 Students must be evaluated to determine if they meet the requirements of IDEA before an IEP can be developed.
While this law does apply most often to students with specific learning disabilities, it also applies to and protects students who require educational accommodations or other services as a result of any of the other disability categories, one of which is “other health impairments” (OHIs). In fact, of over 6 million students served under the IDEA in 2016, 15.4% qualified as having a disability based on OHIs.98 According to IDEA, a student meets the definition of OHI if he/she has “limited strength, vitality, or alertness, including a heightened alertness to environmental stimuli, that results in limited alertness with respect to the educational environment, that is due to chronic or acute health problems such as asthma, attention deficit disorder or attention deficit hyperactivity disorder, diabetes, epilepsy, a heart condition, hemophilia, lead poisoning, leukemia, nephritis, rheumatic fever, sickle cell anemia, and Tourette syndrome and adversely affects a child's educational performance.”71 The list of conditions is not all inclusive and other acute and chronic conditions, such as CF, may qualify a student for an IEP under the OHI clause.70
If a child is evaluated and determined to meet eligibility requirements, an IEP is developed by a team made up of the child's parent or guardian, general and special education teachers, an individual who can interpret the child's evaluation results, a member of a public agency who is “qualified to provide or supervise the provision of specially designed instruction” to meet the needs of a child with a disability, any individuals with special knowledge of the student's needs, and the student if appropriate.99 For students who qualify for IDEA for OHIs, it may be helpful for a member of the child's health care team or primary care provider to participate in the IEP meeting or submit written documentation of the child's medical needs, particularly those that will impact the child during the school day and/or interfere with learning.70 The IEP must include and address the child's current academic and functional performance, annual education goals and how progress will be tracked, the type and timing of special educational or related services the child will receive, other accommodations or modifications that need to be made, participation in standardized tests, and inclusion in general education classes and school activities.100 IEPs must be reviewed at least annually, and the student must be reevaluated every 3 years to ensure that he/she still qualifies for an IEP.
Secure Storage of Medications. Security and storage of medication is fundamental when providing health care services in the school setting. Medications for use in school should be in the original containers with an accurate, up-to-date prescription label. These medications should be kept in a secure location and at an appropriate temperature based on medication instructions (e.g., cabinet, refrigerator). Medications that are classified as controlled substances, such as amphetamines, must be stored by using double-lock security. Medications need to be not only safe and secure, but also accessible for school health staff during school hours and activities. At the start of the school year, members of the school health staff should provide guidance to caregivers regarding required documentation and medication supply preparation (e.g., reminders to obtain refills, make sure supply has prescription label). At the end of a given school year, medication supplies should be returned to caregivers or disposed of in accordance with laws and regulations. Documentation that should be on file for students who require medications during the school day include an up-to-date medication list, up-to-date list of allergies, current weight, health action plans (e.g., asthma action plan, 504 plan), documentation of permission for self-administration (when applicable), physician order documents, and parent/caregiver consent forms. Documentation of medication administration should be completed in real-time and spot-checked regularly.17
Off-site Activities and Medication Use (e.g., Field Trips). Medication use on field trips can be a challenging task for school staff. Currently, there is no specific guidance in the literature with regard to medication administration and storage during school field trips. In general, a school's medication-use policies would apply similarly when it comes to administering medications during a school field trip. Secure storage of medications in such a situation may be challenging and should be addressed in each school policy whenever possible. To help minimize the need for transporting medication supplies and reduce the risk of loss, whenever medically appropriate, medications should be administered prior to and/or after a given field trip. Medications that must be carried for a field trip should be in the original container with a prescription label providing accurate instructions for use. Additionally, appropriate documentation (e.g., current medication list, action plans) should accompany children and be completed when doses are administered.
Self-Carrying and Self-Administration of Medications. Self-administered medications include those that are needed for urgent or emergency use and do not require refrigeration or secure storage. Controlled substances should not be self-administered or carried by children in school. Children who are expected to carry and self-administer selected medications should be old enough to be capable of such responsibility and should be trained in appropriate administration and use. Determining whether a child is capable of such responsibilities should be done collaboratively between parent/caregiver, prescriber, and school health staff. Each assessment should evaluate the child's knowledge of the medical condition, medication administration technique, and understanding of appropriate steps to notify or alert school staff for health-related assistance. Doses self-administered by younger children (e.g., elementary school) should be reported to school health staff for documentation and determination if additional health assessment or assistance is needed.17 Medications carried by children for self-administration should not be left unattended, but should be on their person at all times, including during off-campus school activities such as field trips. Also, designated school staff (e.g., teachers) may carry medications to provide assistance in administration, if policies and regulations permit such practices.
Partnering with Schools and Students' Caregivers. Given the variety and number of items needed to prepare for medication use in the school setting, it is essential that those in the health care and school communities provide support to caregivers. School health staff can help caregivers prepare for medication use in school through informational sessions and provision of documents prior to the start of school as well as with intermittent reminders, in case children start medications during the school year. Clinicians, including pharmacists, in the primary care setting and specialty clinics should also provide support and guidance to caregivers regarding medication use in the school setting before each new school year and whenever a new therapy is started. This can include evaluation of the school's documentation requirements (such as physician orders, letter for medication use), reminders of medication refills for both home and school supplies, and providing any prescriptions necessary to maintain an adequate supply of medication at school.
Conclusions
Whether addressing a student's health and medication needs associated with a chronic condition or an emergency situation, it is apparent that thoughtful preparation and communication between the school, the student's family, and primary care/specialty providers are essential to optimize care of the student.
The development of medication policies addressing self-carrying of medication, self-administration of medications by students, administration of medication by school staff, and keeping of undesignated stock of emergent medications is a key step in improving medication administration and emergency response in schools. These policies should be routinely updated to reflect current legislation and practice changes.
Although the disease states addressed in this review (e.g., asthma, diabetes, anaphylaxis) are all vastly different, it is considered best practice in all cases to develop a written plan for medication and disease management at school and file it with the school nurse to allow for any necessary preparation or staff education that is required. Physicians should work with school-age patients, their families and school to develop individual action plans for daily and emergency care associated with preexisting diagnoses (e.g., asthma, seizures).
Among the most ardent advocates for their children, parents can also play a significant role in making schools safer for them. Parents or caregivers of all students can contact the school office to see what medication policies and emergency action plans are currently in place. Their inquiries may prompt school administrators to develop medication policies for prescription, emergency, and OTC medications as well as protocols for medical emergencies (e.g., anaphylaxis, opioid overdose) if they have not already done so. They can also petition school administrators or school nurses to develop policies allowing non-designated stock of medications, such as albuterol, epinephrine, and naloxone, to be stored within the school.
Lack of proper planning, development of appropriate policies, clear delineation of responsibilities, and thorough staff education can lead to confusion and inefficiency during emergencies. The resulting time lost can be life-altering for those involved and can even mean the difference between life and death. It is time for school administrators, health care professionals, and families to come together and proactively address medication and health issues in our schools. It is only with collaboration and ongoing advocacy that advances can be made to improve the health of our students.
ABBREVIATIONS
- CF
cystic fibrosis
- CFTR
cystic fibrosis transmembrane conductance regulator
- DMMP
diabetes medical management plan
- IDEA
Individuals with Disabilities Education Act
- IEP
individualized education program
- IHP
individualized health care plan
- OHI
other health impairment
- OTC
over-the-counter
- UAP
unlicensed assistive personnel
Footnotes
Disclosure The authors declare no conflicts or financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employment, gifts, and honoraria.
REFERENCES
- 1.Child and Adolescent Health Measurement Initiative 2016–2017 National Survey of Children's Health (NSCH) data query. Data Resource Center for Child and Adolescent Health supported by Cooperative Agreement U59MC27866 from the US Department of Health and Human Services, Health Resources and Services Administration's Maternal and Child Health Bureau (HRSA MCHB). www.childhealthdata.org Accessed January 11, 2019.
- 2.US Department of Health and Human Services, Health Resources and Services Administration, Maternal and Child Health Bureau Child Health USA 2014. Rockville, MD: US Dept of Health and Human Services; 2015. www.mchb.hrsa.gov/chusa14 Accessed May 16, 2016. [Google Scholar]
- 3.American Academy of Pediatrics, Council on School Health Role of the school nurse in providing school health services. Pediatrics. 2008;121(5):1052–1056. doi: 10.1542/peds.2008-0382. [DOI] [PubMed] [Google Scholar]
- 4.State School Health Policy Database: Administration of Medications [Internet] Alexandria, VA: National Association of State Boards of Education, Center for Safe and Healthy Schools; Dec, 2013. (1998-) www.nasbe.org/healthy_schools/hs/bytopics.php?topicid=4110 Accessed May 4, 2016. [Google Scholar]
- 5.Allergy and Asthma Network Breathe: It's the Law. Vienna, VA: Allergy and Asthma Network; 2014. www.allergyasthmanetwork.org/advocacy/current-issues/medications-school Accessed May 16, 2016. [Google Scholar]
- 6.Centers for Disease Control and Prevention Most Recent Asthma Data. Atlanta, GA: Centers for Disease Control and Prevention; 2016. www.cdc.gov/asthma/most_recent_data.htm Accessed July 13, 2018. [Google Scholar]
- 7.Global Initiative for Asthma Global Strategy for Asthma Management and Prevention, 2018. Global Initiative for Asthma; 2019. https://ginasthma.org/wp-content/uploads/2019/06/GINA-2019-main-report-June-2019-wms.pdf Accessed September 22, 2019. [Google Scholar]
- 8.The New York City Department of Education Asthma Medication Administration Form. New York, NY: The New York City Department of Education; 2017. schools.nyc.gov/NR/rdonlyres/100F9F6C-2220-4D5A-BBC0-D5C58FA20B4B/0/AsthmaMAF4212017.pdf Accessed December 10, 2017. [Google Scholar]
- 9.Centers for Disease Control and Prevention Asthma in Children: Working Together to Get It Under Control. Atlanta, GA: Centers for Disease Control and Prevention; 2018. www.cdc.gov/vitalsigns/childhood-asthma Accessed January 21, 2019. [Google Scholar]
- 10.Gerald LB, McClure LA, Mangan JM et al. Increasing adherence to inhaled steroids among schoolchildren: a randomized, controlled trial of school-based supervised asthma therapy. Pediatrics. 2009;123(2):466–474. doi: 10.1542/peds.2008-0499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.American Lung Association Joint Statement on Improving Asthma Management in Schools. Chicago, IL: American Lung Association; 2013. www.lung.org/assets/documents/asthma/joint-statement-improve-asthma-mgmt-schools.pdf Accessed May 2, 2017. [Google Scholar]
- 12.American Academy of Allergy, Asthma & Immunology Asthma Triggers and Management. Milwaukee, WI: American Academy of Allergy, Asthma & Immunology; 2017. www.aaaai.org/conditions-and-treatments/library/asthma-library/asthma-triggers-and-management Accessed May 2, 2017. [Google Scholar]
- 13.American Academy of Allergy, Asthma & Immunology Asthma Symptoms, Diagnosis, Management & Treatment. Milwaukee, WI: American Academy of Allergy, Asthma & Immunology; 2017. www.aaaai.org/conditions-and-treatments/asthma Accessed March 10, 2017. [Google Scholar]
- 14.National Institutes of Health, National Asthma Education and Prevention Program Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Institutes of Health, National Heart, Lung and Blood Institute; 2007. [Google Scholar]
- 15.Asthmatic Schoolchildren's Treatment and Health Management Act of 2004. Oct 30, 2004. Pub L 108-377, 118 Stat 2202–2205. May 12, 2017 [Internet]
- 16.American Lung Association Improving Access to Asthma Medications in Schools. Chicago, IL: American Lung Association; 2014. www.lung.org/assets/documents/asthma/improving-access-to-asthma.pdf Accessed March 10, 2017. [Google Scholar]
- 17.American Academy of Pediatrics Council on School Health Policy statement: guidance for the administration of medication in school. Pediatrics. 2009;124(4):1244–1251. doi: 10.1542/peds.2009-1953. [DOI] [PubMed] [Google Scholar]
- 18.Gerald JK, Stroupe N, McClure LA et al. Availability of asthma quick relief medication in five Alabama school systems. Pediatr Allergy Immunol Pulmonol. 2012;25(1):11–16. doi: 10.1089/ped.2011.0118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Department of Health Guidance on the Use of Emergency Salbutamol Inhalers in Schools. Whitehall, London: Department of Health; 2015. www.gov.uk/government/uploads/system/uploads/attachment_data/file/416468/emergency_inhalers_in_schools.pdf Accessed: February 3, 2018. [Google Scholar]
- 20.Flores G, Snowden-Bridon C, Torres S et al. Urban minority children with asthma: substantial morbidity, compromised quality and access to specialists, and the importance of poverty and specialty care. J Asthma. 2009;46(4):392–398. doi: 10.1080/02770900802712971. [DOI] [PubMed] [Google Scholar]
- 21.Gerald LB, Disney J, Gerald JK et al. Implementation and evaluation of a stock albuterol program for students with asthma. Ann Am Thorac Soc. 2016;13(2):295–296. doi: 10.1513/AnnalsATS.201510-683LE. [DOI] [PubMed] [Google Scholar]
- 22.United States, Congress, House Committee on Energy and Commerce. School-Based Asthma Management Program Act. 114th Cong, 2nd Sess, HR 4662. March 2, 2016. May 4, 2017 [Internet]
- 23.Allergy and Asthma Network Support HR 4662: School-Based Asthma Management Program Act. Vienna, VA: Allergy and Asthma Network; www.allergyasthmanetwork.org/cms/wp-content/uploads/2015/01/Advocate-Issue-Brief-School-Based-Asthma-Mgmt-Program.pdf Accessed May 24, 2017. [Google Scholar]
- 24.United States, Congress, House Committee on Energy and Commerce. School-Based Respiratory Health Management Act. 115th Cong, 1st Sess, HR 2285. May 2, 2017. May 24, 2017 [Internet]
- 25.American Lung Association Asthma Medications in School. Chicago, IL: American Lung Association; 2018. www.lung.org/lung-health-and-diseases/lung-disease-lookup/asthma/living-with-asthma/creating-asthma-friendly-environments/asthma-medication-in-schools.html Accessed January 29, 2018. [Google Scholar]
- 26.American Lung Association Model Policy on Stock Bronchodilators. Chicago, IL: American Lung Association; 2018. www.lung.org/assets/documents/asthma/model-policy-for-school.pdf Accessed January 29, 2018. [Google Scholar]
- 27.American Academy of Allergy, Asthma & Immunology Asthma Action Plan. Milwaukee, WI: American Academy of Allergy, Asthma & Immunology; 2017. www.aaaai.org/Aaaai/media/MediaLibrary/PDF%20Documents/Libraries/NEW-WEBSITE-LOGO-asthma-action-plan_HI.pdf Accessed May 26, 2017. [Google Scholar]
- 28.American Lung Association Asthma-Friendly Schools Initiative. Chicago, IL: American Lung Association; 2007. www.lung.org/lung-health-and-diseases/lung-disease-lookup/asthma/asthma-education-advocacy/asthma-friendly-schools-initiative Accessed August 9, 2016. [Google Scholar]
- 29.American Academy of Allergy, Asthma & Immunology School Tools: Allergy & Asthma Resources for Families, Clinicians and School Nurses. Milwaukee, WI: American Academy of Allergy, Asthma & Immunology; 2016. www.aaaai.org/conditions-and-treatments/library/school-tools Accessed August 9, 2016. [Google Scholar]
- 30.Sampson HA, Muffoz-Furlong A, Campbell RL et al. Second symposium on the definition and management of anaphylaxis: summary report—Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network Symposium. J Allergy Clin Immunol. 2006;117(2):391–397. doi: 10.1016/j.jaci.2005.12.1303. [DOI] [PubMed] [Google Scholar]
- 31.Lieberman P, Nicklas RA, Oppenheimer J et al. The diagnosis and management of anaphylaxis practice parameter: 2010 update. J Allergy Clin Immunol. 2010;126(3):477–480.e42. doi: 10.1016/j.jaci.2010.06.022. [DOI] [PubMed] [Google Scholar]
- 32.McIntyre CL, Sheetz AH, Carroll CR, Young MC. Administration of epinephrine for life-threatening allergic reactions in school settings. Pediatrics. 2005;116(5):1134–1140. doi: 10.1542/peds.2004-1475. [DOI] [PubMed] [Google Scholar]
- 33.United States, Congress, Senate Committee on Health, Education, Labor and Pensions. School Access to Emergency Epinephrine Act. 113th Cong, 1st Sess, S 1503. September 12, 2013. May 12, 2016 [Internet]
- 34.Food Allergy Research and Education Inc. School Access to Epinephrine Map. McLean, VA: Food Allergy Research and Education Inc; 2016. www.foodallergy.org/advocacy/epinephrine/map Accessed May 25, 2017. [Google Scholar]
- 35.IBM Micromedex Drugdex [Internet] Greenwood Village, CO: IBM Watson Health; 2018. Epinephrine. Cited January 21, 2019. www.micromedexsolutions.com Accessed January 21, 2019. [Google Scholar]
- 36.Georgia Department of Public Health Toolkit for the Administration of Epinephrine and Albuterol/Levalbuterol in the School Setting. Atlanta, GA: Georgia Dept of Public Health; 2016. dph.georgia.gov/sites/dph.georgia.gov/files/ToolkitforAdministrationofEpinephrine%20and%20AlbuterolandLevalbuterolinSchoolSetting%28Final%209_3_2015%29%281%29%281%29.pdf Accessed January 10, 2019. [Google Scholar]
- 37.American Academy of Allergy, Asthma & Immunology Anaphylaxis Emergency Action Plan. Milwaukee, WI: American Academy of Allergy, Asthma & Immunology; 2017. www.aaaai.org/Aaaai/media/MediaLibrary/PDF%20Documents/Libraries/Anaphylaxis-Emergency-Action-Plan.pdf Accessed May 26, 2017. [Google Scholar]
- 38.American Academy of Pediatrics Allergy and Anaphylaxis Emergency Plan. Itasca, IL: American Academy of Pediatrics; 2017. www.aap.org/en-us/Documents/AAP_Allergy_and_Anaphylaxis_Emergency_Plan.pdf Accessed January 24, 2018. [Google Scholar]
- 39.Wang J, Sicherer SH, AAP Section on Allergy and Immunology Guidance on completing a written allergy and anaphylaxis emergency plan. Pediatrics. 2017;139(3) doi: 10.1542/peds.2016-4005. e20164005. doi: 10.1542/peds.2016-4005. pediatrics.aappublications.org/content/pediatrics/early/2017/02/09/peds.2016-4005.full.pdf Accessed January 24, 2018. [DOI] [PubMed] [Google Scholar]
- 40.Mylan Get Schooled in Anaphylaxis: Resource Library. Canonsburg, PA: Mylan; 2017. www.anaphylaxis101.com/en/resource-library Accessed May 26, 2017. [Google Scholar]
- 41.National Association of School Nurses Food Allergies and Anaphylaxis. Silver Spring, MD: National Association of School Nurses; 2017. www.nasn.org/nasn/nasn-resources/practice-topics/food-allergies Accessed May 26, 2017. [Google Scholar]
- 42.Food Allergy & Anaphylaxis Connection Team (FAACT) Education for School Personnel. West Chester, OH: Food Allergy & Anaphylaxis Connection Team; 2017. www.foodallergyawareness.org/education/for_school_personnel-3/for_school_personnel-3 Accessed May 28, 2017. [Google Scholar]
- 43.National Association of School Nurses Epinephrine Policies, Protocols, and Reporting. Silver Spring, MD: National Association of School Nurses; 2017. www.nasn.org/nasn/nasn-resources/models-samples/epinephrine Accessed May 26, 2017. [Google Scholar]
- 44.Centers for Disease Control and Prevention Voluntary Guidelines for Managing Food Allergy in Schools and Early Care and Education Programs. Washington, DC: US Dept of Health and Human Services; 2013. www.cdc.gov/healthyyouth/foodallergies/pdf/13_243135_a_food_allergy_web_508.pdf Accessed May 26, 2017. [Google Scholar]
- 45.Mylan Inc. Epipen4schools. Canonsburg, PA: Mylan Inc; 2016. www.epipen4schools.com Accessed May 12, 2016. [Google Scholar]
- 46.Brodie MJ, Barry SJ, Bamagous GA et al. Patterns of treatment response in newly diagnosed epilepsy. Neurology. 2012;78(20):1548–1554. doi: 10.1212/WNL.0b013e3182563b19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Glauser T, Shinnar S, Gloss D et al. Evidence based guideline: treatment of convulsive status epilepticus in children and adults: report of the guideline committee of the American Epilepsy Society. Epilepsy Curr. 2016;16(1):48–61. doi: 10.5698/1535-7597-16.1.48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Eriksson K, Metsaranta P, Huhtala H et al. Treatment delay and the risk of prolonged status epilepticus. Neurology. 2005;65(8):1316–1318. doi: 10.1212/01.wnl.0000180959.31355.92. [DOI] [PubMed] [Google Scholar]
- 49.Terry D, Paolicchi J, Karn M. Acceptance of the use of diazepam rectal gel in school and day care settings. J Child Neurol. 2007;22(9):1135–1138. doi: 10.1177/0883073807306254. [DOI] [PubMed] [Google Scholar]
- 50.O'Dell C, O'Hara K. School nurses' experience with administration of rectal diazepam gel for seizures. J Sch Nurs. 2007;23(3):166–169. doi: 10.1177/10598405070230030701. [DOI] [PubMed] [Google Scholar]
- 51.California Department of Education Antiseizure Medication Law FAQs. Sacramento, CA: California Dept of Education; 2017. www.cde.ca.gov/ls/he/hn/sb161faq.asp Accessed March 2, 2018. [Google Scholar]
- 52.Alabama Board of Nursing Administrative Code Chapter 610-X-7 Standards of Nursing Practice; Specific Settings. Montgomery, AL: Alabama Board of Nursing; 2018. www.abn.alabama.gov/laws/#tab-code Accessed March 3, 2018. [Google Scholar]
- 53.Scott RC, Besag FM, Neville BG. Buccal midazolam and rectal diazepam for treatment of prolonged seizures in childhood and adolescence: a randomised trial. Lancet. 1999;353(9153):623–626. doi: 10.1016/S0140-6736(98)06425-3. [DOI] [PubMed] [Google Scholar]
- 54.Troester MM, Hastriter EV, Ng YT. Dissolving oral clonazepam wafers in the acute treatment of prolonged seizures. J Child Neurol. 2010;25(12):1468–1472. doi: 10.1177/0883073810368312. [DOI] [PubMed] [Google Scholar]
- 55.Hartman AL, Devore CDL, AAP and the Section on Neurology et al. Rescue medicine for epilepsy in education settings. Pediatrics. 2016;137(1) doi: 10.1542/peds.2015-3876. e20153876. doi:10.1542/peds.2015-3876. [DOI] [PubMed] [Google Scholar]
- 56.Epilepsy Foundation Seizure Response Plans 101. Landover, MD: Epilepsy Foundation; 2017. www.epilepsy.com/get-help/managing-your-epilepsy/seizure-response-plans-101 Accessed June 3, 2017. [Google Scholar]
- 57.Epilepsy Foundation Seizure Action Plan. Landover, MD: Epilepsy Foundation; 2014. www.epilepsy.com/sites/core/files/atoms/files/SeizureActionPlan_School.pdf Accessed March 3, 2018. [Google Scholar]
- 58.healthychildren.org Children With Epilepsy at School. Elk Grove Village, IL: American Academy of Pediatrics; 2015. www.healthychildren.org/English/health-issues/conditions/head-neck-nervous-system/Pages/Children-with-Epilepsy-at-School.aspx Accessed June 3, 2017. [Google Scholar]
- 59.Epilepsy Foundation Your Child at School and Child Care. Landover, MD: Epilepsy Foundation; 2014. www.epilepsy.com/learn/seizures-youth/about-kids/your-child-school-and-child-care Accessed June 3, 2017. [Google Scholar]
- 60.Martenz D, Cramp L. The Keto Diet at School: A Sample Letter to Your Child's Teachers [Internet] New York: Demos Health Publishing; www.demoshealth.com/w/the-keto-diet-at-school-a-sample-letter-to-your-childs-teachers Accessed June 3, 2017. [Google Scholar]
- 61.Boyle MP, De Boeck K. A new era in the treatment of cystic fibrosis: correction of the underlying CFTR defect. Lancet Respir Med. 2013;1(2):158–163. doi: 10.1016/S2213-2600(12)70057-7. [DOI] [PubMed] [Google Scholar]
- 62.Cystic Fibrosis Foundation About Cystic Fibrosis. Bethesda, MD: Cystic Fibrosis Foundation; 2016. www.cff.org/What-is-CF/About-Cystic-Fibrosis Accessed May 31, 2017. [Google Scholar]
- 63.Cystic Fibrosis Research Inc. Cystic Fibrosis in the Classroom. Palo Alto, CA: Cystic Fibrosis Research Inc; 2014. www.cfri.org/pdf/cfintheclassroom.pdf Accessed May 22, 2017. [Google Scholar]
- 64.Cystic Fibrosis Foundation Cystic Fibrosis Foundation Patient Registry: 2017 Annual Data Report. Bethesda, MD: Cystic Fibrosis Foundation; 2018. www.cff.org/Research/Researcher-Resources/Patient-Registry/2017-Patient-Registry-Annual-Data-Report.pdf Accessed January 16, 2019. [Google Scholar]
- 65.Mogayzel PJ, Naureckas ET, the Pulmonary Clinical Practice Guidelines Committee et al. Cystic fibrosis pulmonary guidelines: chronic medication for maintenance of lung health. Am J Respir Crit Care Med. 2013;187(7):680–689. doi: 10.1164/rccm.201207-1160oe. [DOI] [PubMed] [Google Scholar]
- 66.Cystic Fibrosis Foundation A Teacher's Guide to CF. Bethesda, MD: Cystic Fibrosis Foundation; 2006. www.cff.org/Life-With-CF/Daily-Life/CF-and-School/For-Teachers/A-Teacher-s-Guide-to-CF Accessed May 22, 2017. [Google Scholar]
- 67.Cystic Fibrosis Foundation School, Enzymes, and Sports: Nutrition for the Child With Cystic Fibrosis. Bethesda, MD: Cystic Fibrosis Foundation; 2006. www.childrenshospitalofillinois.org/pdfs/specialty-services/cf/cf-at-school/School-Enzymes-and-Sports.pdf Accessed May 22, 2017. [Google Scholar]
- 68.Cystic Fibrosis Foundation Nutrition: Pancreatic Enzyme Replacement in People With Cystic Fibrosis. Bethesda, MD: Cystic Fibrosis Foundation; 2006. www.cff.org/PDF-Archive/Pancreatic-Enzyme-Replacement.pdf Accessed June 3, 2017. [Google Scholar]
- 69.Cystic Fibrosis Foundation Pancreatic Enzymes Clinical Care Guidelines: Executive Summary. Bethesda, MD: Cystic Fibrosis Foundation; 2016. https://www.cff.org/Care/Clinical-Care-Guidelines/Nutrition-and-GI-Clinical-Care-Guidelines/Pancreatic-Enzymes-Clinical-Care-Guidelines Accessed June 3, 2017. [Google Scholar]
- 70.Cystic Fibrosis Foundation Day-to-Day: School and CF. Bethesda, MD: Cystic Fibrosis Foundation; www.cff.org/Life-With-CF/Caring-for-a-Child-With-CF/Working-with-Your-Childs-School/Formalizing-Special-Accomodations-Using-IEP-504-Plans.pdf Accessed May 22, 2017. [Google Scholar]
- 71.US Department of Education, Office of Special Education Programs Individuals With Disabilities Education Act, Sec 300.8 Child with a Disability. Washington, DC: US Dept of Education; sites.ed.gov/idea/regs/b/a/300.8 Accessed January 19, 2019. [Google Scholar]
- 72.Cystic Fibrosis Australia CF Smart, Cystic Fibrosis Education Program: A Guide to Cystic Fibrosis for Primary School Teachers. Cystic Fibrosis Australia; 2014. cfsmart.files.wordpress.com/2014/02/cff035i-booklet-cf-for-primary-school-teacherssingles_web-2.pdf Accessed May 29, 2017. [Google Scholar]
- 73.Centers for Disease Control and Prevention National Diabetes Statistics Report, 2017: Estimates of Diabetes and Its Burden in the United States. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; 2017. www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf Accessed September 7, 2018. [Google Scholar]
- 74.American Diabetes Association Diabetes care in the school setting: a position statement of the American Diabetes Association. Diabetes Care. 2015;38(10):1958–1963. doi: 10.2337/dc15-1418. [DOI] [PubMed] [Google Scholar]
- 75.American Diabetes Association State Laws, Regulations and Policies for School Diabetes Care. Arlington, VA: American Diabetes Association; 2014. www.diabetes.org/living-with-diabetes/parents-and-kids/diabetes-care-at-school/legal-protections/school-laws-and-policies Accessed March 4, 2018. [Google Scholar]
- 76.Siminerio LM, Albanese-O'Neill A, Chiang JL et al. Care of young children with diabetes in the child care setting: a position statement of the American Diabetes Association. Diabetes Care. 2014;37(10):2834–2842. doi: 10.2337/dc14-1676. [DOI] [PubMed] [Google Scholar]
- 77.American Association of Diabetes Educators Management of children with diabetes in the school setting: AADE position statement. Diabetes Educ. 2016;34(3):439–443. doi: 10.1177/0145721708317873. www.diabeteseducator.org/docs/default-source/practice/practice-resources/position-statements/diabetes-in-the-school-setting-position-statement_final.pdf Accessed: June 6, 2017. [DOI] [PubMed] [Google Scholar]
- 78.National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases Helping the Student With Diabetes Succeed: A Guide for School Personnel. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2016. www.niddk.nih.gov/health-information/health-communication-programs/ndep/health-care-professionals/school-guide/Pages/publicationdetail.aspx Accessed August 9, 2016. [Google Scholar]
- 79.American Diabetes Association Safe at School. Arlington, VA: American Diabetes Association; 2017. www.diabetes.org/living-with-diabetes/parents-and-kids/diabetes-care-at-school Accessed May 1, 2017. [Google Scholar]
- 80.Juvenile Diabetes Research Foundation T1D Resources and Support. New York, NY: Juvenile Diabetes Research Foundation; 2019. www.jdrf.org/t1d-resources Accessed January 22, 2019. [Google Scholar]
- 81.Diabetes at School. West Chester, OH: Children with Diabetes; 2015. Children with Diabetes. www.childrenwith-diabetes.com Accessed May 2, 2017. [Google Scholar]
- 82.Centers for Disease Control and Prevention Managing Diabetes at School Playbook. Atlanta, GA: Centers for Disease Control and Prevention; 2016. www.cdc.gov/features/diabetesinschool Accessed August 9, 2016. [Google Scholar]
- 83.Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration Key Substance Use and Mental Health Indicators in the United States: Results From the 2015 National Survey on Drug Use and Health. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration; 2016. HHS Pub No. SMA 16-4984, NSDUH Series H-51. www.sam-hsa.gov/data/sites/default/files/NSDUH-FFR1-2015Rev1/NSDUH-FFR1-2015Rev1/NSDUH-FFR1-2015Rev1/NSDUH-National%20Findings-REVISED-2015.pdf Accessed May 4, 2017. [Google Scholar]
- 84.Johnston LD, Miech RA, O'Malley PM Monitoring the Future National Survey Results on Drug Use, 1975–2017: Overview, Key Findings on Adolescent Drug Use. Ann Arbor, MI: Institute for Social Research, The University of Michigan; 2018. www.monitoringthefuture.org/pubs/monographs/mtf-overview2017.pdf Accessed January 19, 2019. [Google Scholar]
- 85.Substance Abuse and Mental Health Services Administration (SAMHSA) SAMHSA Opioid Overdose Prevention Toolkit. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2016. HHS Pub No. 16-1472. store.samhsa.gov/shin/content/SMA16-4742/SMA16-4742.pdf Accessed May 22, 2017. [Google Scholar]
- 86.Adapt Pharma Inc. Narcan® (Naloxone HCl) Nasal Spray Prescribing Information. Radnor, PA: Adapt Pharma Inc; 2017. www.narcan.com/pdf/NARCAN-Prescribing-Information.pdf Accessed March 4, 2018. [Google Scholar]
- 87.Adapt Pharma Inc. Adapt Pharma to Offer all U.S. High Schools a Free Narcan® Nasal Spray and Fund School-Based Opioid Overdose Education. 2016 Jan 25; May 22, 2016 [Internet]. www.adaptpharma.com/press-releases Accessed May 26, 2017.
- 88.Adapt Pharma Inc. Free Narcan® Nasal Spray High School Program Order and Terms and Conditions. Radnor, PA: Adapt Pharma Inc; 2017. www.narcan.com/pdf/NARCAN-for-High-Schools.pdf Accessed May 26, 2017. [Google Scholar]
- 89.National Association of School Nurses Naloxone in School: Resources. Silver Spring, MD: National Association of School Nurses; 2016. www.pathlms.com/nasn/courses/3353/documents/3966 Accessed May 26, 2017. [DOI] [PubMed] [Google Scholar]
- 90.National Association of School Nurses Naloxone in Schools Toolkit. Silver Spring, MD: National Association of School Nurses; 2016. www.pathlms.com/nasn/courses/3353/documents/3969 Accessed June 2, 2017. [DOI] [PubMed] [Google Scholar]
- 91.National Association of School Nurses Narcan® Administration Protocol. Silver Spring, MD: National Association of School Nurses; 2016. www.pathlms.com/nasn/courses/3353/documents/3969 Accessed June 2, 2017. [Google Scholar]
- 92.American Academy of Pediatrics (AAP) Council on School Health Medical emergencies occurring at school. Pediatrics. 2008;122(4):887–894. doi: 10.1542/peds.2008-2171. [DOI] [PubMed] [Google Scholar]
- 93.Sicherer SH, Mahr T, AAP and the Section on Allergy and Immunology et al. Management of food allergy in the school setting. Pediatrics. 2010;126(6):1232–1239. doi: 10.1542/peds.2010-2575. [DOI] [PubMed] [Google Scholar]
- 94.National Association of School Nurses Medication Administration in the School Setting: Position Statement. Silver Spring, MD: National Association of School Nurses; 2012. www.nasn.org/PolicyAdvocacy/PositionPapersandReports/NASNPositionStatementsFullView/tabid/462/ArticleId/86/Medication-Administration-in-the-School-Setting-Amended-January-2012 Accessed August 4, 2016. [Google Scholar]
- 95.US Department of Education Protecting Students With Disabilities: Frequently Asked Questions About Section 504 and the Education of Children with Disabilities. Washington, DC: US Dept of Education; 2015. www2.ed.gov/about/offices/list/ocr/504faq.html Updated October 16, 2015. Accessed December 9, 2017. [Google Scholar]
- 96.US Department of Education, Office of Special Education Programs About IDEA. Washington, DC: US Dept of Education; sites.ed.gov/idea/about-idea Accessed January 21, 2019. [Google Scholar]
- 97.Lee AM. Understood.org: Accommodations: What they are and how they work [Internet] New York: Understood.org USA LLC; www.understood.org/en/learning-attention-issues/treatments-approaches/educational-strategies/accommodations-what-they-are-and-how-they-work Accessed January 21, 2019. [Google Scholar]
- 98.US Department of Education, Office of Special Education Programs 2018 Annual Report to Congress on the Individuals With Disabilities Education Act: IDEA Parts B and C. Washington, DC: US Dept of Education; 2018. sites.ed.gov/idea/2018-annual-report-to-congress-on-the-individuals-with-disabilities-education-act/#Ages-6-12-Part-B Accessed January 21, 2019. [Google Scholar]
- 99.US Department of Education, Office of Special Education Programs IDEA Sec.300.321(a) Washington, DC: US Dept of Education; sites.ed.gov/idea/regs/b/d/300.321/a Accessed January 21, 2019. [Google Scholar]
- 100.US Department of Education, Office of Special Education Programs IDEA Sec.300.320 Definition of Individualized Education Program. Washington, DC: US Dept of Education; sites.ed.gov/idea/regs/b/d/300.320 Accessed January 21, 2019. [Google Scholar]