

Abstract
Certain types of alopecia, such as traction alopecia, discoid lupus erythematosus, and central centrifugal cicatricial alopecia, occur more commonly in African-American individuals than in those of other ethnicities. Both intrinsic hair qualities and hair care practices play a role. Lower baseline tensile strength, hair density, and growth rates, as well as the use of high-tension hairstyles and chemical relaxers may contribute to alopecia in this group. Alopecia can also occur as a result of discoid lupus erythematosus, which involves chronic lymphocytic infiltration and eventual scarring of the hair follicle. Lichen planopilaris is a less common cause of scarring alopecia that can appear clinically similar to other forms of cicatricial alopecia. Lastly, although not classically associated with hair loss, recent evidence indicates that seborrheic dermatitis may play a role in shedding and alopecia. Recognizing and differentiating these alopecic subtypes clinically and histopathologically is important for prompt diagnosis and treatment. This article is based on a chapter in Ethnic Skin and Hair, and intended as a supplemental article to “Current and Emerging Treatment Strategies for Hair Loss in Women of Color.”
Keywords: Alopecia, Traction alopecia, Seborrheic dermatitis, Lichen planopilaris, Discoid lupus erythematosus
Introduction
Hair loss is a common yet challenging clinical scenario encountered by dermatologists. The underlying cause of hair loss can at times be difficult to pinpoint and can often be even more challenging to treat. This may be particularly true for African-American patients who are affected by certain types of alopecia, such as discoid lupus erythematosus and central centrifugal cicatricial alopecia (CCCA), more commonly than patients of other ethnicities, but many of these conditions still lack an appropriate pathophysiologic description and validated treatment. In fact, compared with their Caucasian, Asian, and Hispanic counterparts, patients of color are the only ethnic group in which alopecia ranks among the top 10 dermatologic conditions (Davis et al., 2012).
For many women, hair is a central feature of appearance and identity. Therefore, loss of hair, even in small amounts, can have a detrimental psychological impact. In a study of androgenetic alopecia, the majority of women reported changing their daily activities and a loss of self-confidence due to hair loss (McMichael, 2003). A recent review of several quality-of-life studies found alopecia in women to be associated with a reduced quality of life and self-esteem along with greater anxiety and depression (Davis and Callendar, 2018). Regardless of ethnic background or mechanism of hair loss, alopecia is likely to significantly affect patients and encourage them to seek dermatologic help. Certain hair loss conditions occur more commonly or almost exclusively in African-American patients and should be familiar to dermatologists.
This article is based on a chapter in Ethnic Skin and Hair and is intended as a supplemental article to “Current and Emerging Treatment Strategies for Hair Loss in Women of Color” (Okereke et al., 2019).
Structural differences of hair between patients of color and Caucasian patients
Structural and biochemical characteristics of hair vary among ethnic groups. The chemical composition of the hair shaft, specifically the keratin and amino acid configurations, is similar across African, Asian, and Caucasian ethnicities (Franbourg et al., 2003, Lawson et al., 2017). African and Caucasian hair are also largely similar with respect to cuticle thickness, shape and size of scale, and cortical cells (Taylor, 2002). With regard to hair pattern (e.g., helical, spiral, straight, and wavy), spiral hair is seen most commonly in African hair, which makes the hair more difficult to comb and increases the risk of breakage due to styling (Khumalo, 2005, Richards et al., 2003).
Under magnification, African hair exhibits many random twists and irregular direction changes (Franbourg et al., 2003, Khumalo, 2005). The African hair follicle is sharply curved, which contributes to the textured, curly appearance of the hair, and is distinct from the ovular follicle in Caucasian individuals and the round shape in Asian persons (Franbourg et al., 2003, Lindelof et al., 1988). This also results in hair growing from the skin at an oblique angle, increasing the risk of conditions such as pseudofolliculitis barbae (Perry et al., 2002).
Studies on hair growth have demonstrated slower rates of growth in African than Caucasian hair (Lewallen et al., 2015). Additionally, the density of hair and total number of hair follicles may be lower in African hair compared with Caucasian hair (Franbourg et al., 2003, Sperling, 1999). Fewer elastic fibers attaching hair follicles to the dermis in African hair compared with Caucasian hair has also been observed (Richards et al., 2003, Taylor, 2002), which may help explain why certain types of alopecia, such as traction alopecia (TA) and CCCA, occur more commonly in African than Caucasian women (Lawson et al., 2017, Ogunleye et al., 2014).
Integral lipids of the hair cuticle (sometimes called the hair barrier) lend hydrophobicity, moisturization, and stiffness to hair, as well as protection from ultraviolet damage (Ji et al., 2013, Lee et al., 2005). Although the composition of various lipids in hair is similar across racial type, African hair appears to contain fewer lipids than Caucasian hair, increasing susceptibility to ultraviolet damage (Ji et al., 2013). Along with reduced tensile strength and less moisture compared with Caucasian hair, these factors provide clarity as to why African hair is more susceptible to breakage (Franbourg et al., 2003).
Traction alopecia: predisposing hair care practices and differential diagnosis
TA is a form of hair loss associated with sustained or repetitive traction on the hair shaft and follicle (Lawson et al., 2017). Most commonly seen in women of African descent, TA results from haircare practices that regularly subject the hair to tight pulling, such as tight ponytails, buns, braids, cornrows, and dreadlocks (Khumalo et al., 2007a, Khumalo et al., 2007b, Lawson et al., 2017). Hair extensions also pose a risk for TA, because they often involve tight braids and sewing or gluing of artificial hair into the braids (Griffin and Lenzy, 2015). The risk of TA significantly increases when traction is applied to chemically treated hair, such as with relaxers or dyes, although the use of shampoo and other hair styling products has not been found to play a role (Khumalo et al., 2007a, Khumalo et al., 2007b, Lawson et al., 2017, Mirmirani and Khumalo, 2014).
TA typically affects the marginal hairline and the hairline anterior and superior to the ears (Lawson et al., 2017); however, TA can affect any location in the hair-bearing scalp. Early in the clinical course, repetitive traction on the scalp leads to perifollicular erythema, which can progress to follicular papules or pustules with continued insult (Mirmirani and Khumalo, 2014). As the condition progresses, affected hair shafts display peripilar casts (i.e., yellow-white enveloping material) that indicates continued traction (Fig. 1; Lawson et al., 2017, Mirmirani and Khumalo, 2014, Tosti et al., 2010). After this stage, hair loss becomes clinically evident. The fringe sign, referring to retained hairs on the frontotemporal hairline, has been recognized as a sensitive and specific sign of hair loss due to TA (Fig. 2; Lawson et al., 2017, Samrao et al., 2011). Another poignant example is seen after the use of wefted hair extensions, in which a band of hairs is sewn, bonded, glued, or clipped in for extended periods. Long-term or repetitive wefting can result in a pattern of TA known as horseshoe alopecia (Fig. 3; Ahdout and Mirmirani, 2012).
Fig. 1.
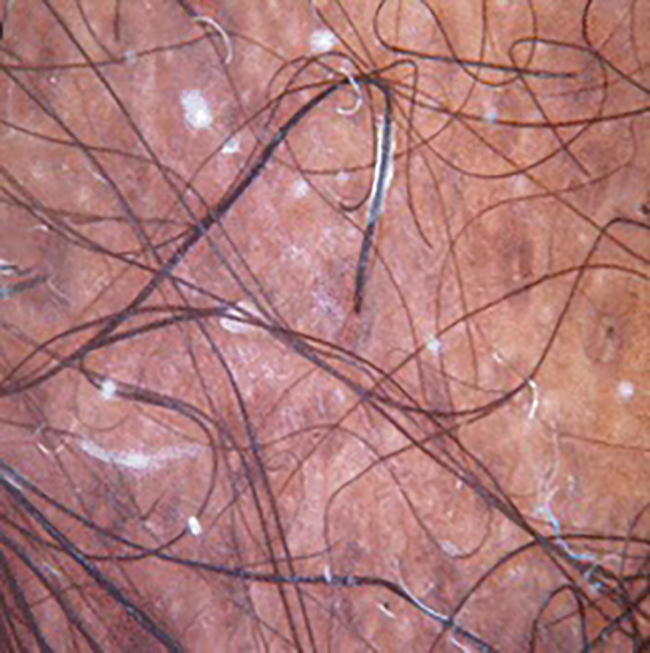
Peripilar casts (Tosti et al., 2010). Dermoscopy of the margin of the patch reveals numerous white hair casts encircling the proximal portion of the hair shafts (60× magnification; Photo reprinted with permission from Wiley Online Library).
Fig. 2.

Fringe sign (Samrao et al., 2011). Traction alopecia involving the frontal and temporal scalp in an African-American patient with concurrent trichorrhexis nodosa (Photo reprinted with permission from Paradi Mirmirani, MD).
Fig. 3.

Horseshoe traction alopecia (Ahdout and Mirmirani, 2012). Alopecia of occipital and temporoparietal scalp corresponds to area where patient used glued-in hair wefts (Photo reprinted with permission from Elsevier).
In cases with unclear clinical presentation or exposure to hair traction, the differential diagnosis includes androgenetic alopecia, telogen effluvium, trichotillomania, and CCCA (Lawson et al., 2017, Samrao et al., 2011). TA of the marginal hairline may also resemble frontal fibrosing alopecia (FFA) and alopecia areata (AA) ophiasis pattern (Heath and Taylor, 2012, Samrao et al., 2011). However, unlike TA, AA and FFA may also involve the eyebrows, body hair, skin, and nails. Whereas the fringe sign of the marginal hairline is considered sensitive and specific for TA, FFA has been associated with the lonely hair sign, and AA has been associated with exclamation point hairs. Other differences are visible under the dermatoscope: follicular markings are observable in AA, but reduced in TA and absent in FFA (Mirmirani and Khumalo, 2014). Perifollicular erythema and scale, as seen in early TA, may also be seen in FFA, but both are usually absent in AA. A definitive diagnosis may necessitate biopsy in these cases (Mirmirani and Khumalo, 2014).
Trichorrhexis nodosa
Trichorrhexis nodosa (TN) is a common hair shaft disorder that stems from the loss of cuticle cells on the hair shaft. Without the protective cuticle, the cortical fibers of the hair shaft become fragile and fray longitudinally (Lawson et al., 2017). Although this type of hair loss may occur in any ethnicity, TN is most common in women of African descent (Haskin et al., 2017). In contrast to the rare congenital form of TN, acquired TN is induced by traumatic hair care practices. Repeated chemical treatment, such as with relaxers, dyes, bleaches, perms, or shampoos, has been implicated in the development of TN. Cysteine, which contributes to hair shaft strength through covalent bonding, is depleted with relaxer use, resulting in a weakened hair cuticle and compromised shaft (Khumalo et al., 2007b, Lawson et al., 2017). In addition to relaxer use, thermal hair tools compromise the cuticle, which ultimately leads to increased fragility and breakage. The cuticle may be further damaged by aggressive hair brushing or combing.
Because TN does not originate within the scalp, a scalp biopsy is of low yield. Instead, the diagnosis is made clinically (Haskin et al., 2017). Repeated trauma to the hair shaft ultimately results in dry, brittle hair with whitish spots along the shaft (Lawson et al., 2017, Miyamoto et al., 2009). These whitish spots (also called nodes) represent the location of fraying and ultimate shaft breakage. Physical examination will reveal broken hairs of varying lengths. Hair fragility can be evaluated by gathering a small group of hairs and tugging on the distal end, resulting in breakage of frail hairs. Under the dermatoscope, the shaft will display numerous areas of swelling, representing the weakening at the nodes. Findings of diminished or absent follicular ostia on the scalp itself signify the presence of a scarring alopecia distinct from TN (Haskin et al., 2017).
Other forms of hair loss in women of color
Seborrheic dermatitis
Seborrheic dermatitis (SD) is a chronic inflammatory condition characterized by erythema, flaking, and pruritus of the scalp, face, and upper chest (Borda and Wikramanayake, 2015). This condition is seen more commonly in patients of African descent, numbering among the top five dermatologic diagnoses in this group (Davis et al., 2012, Lawson et al., 2017). The pathogenesis of SD has been at least partially attributed to colonization of the stratum corneum by Malassezia spp., contributing to chronic, local inflammation of seborrheic areas (Borda and Wikramanayake, 2015, Piérard-Franchimont et al., 2006).
Although hair loss is not a classic finding in SD, some authors have demonstrated a potential association between long-term inflammation in SD and increased telogen shedding (Burns et al., 2010, Piérard-Franchimont et al., 2006, Piérard-Franchimont et al., 2002). Alopecia may not be directly caused by SD but can be a secondary effect of SD caused by SD-related scaly desquamation and/or traumatically induced by scratching due to pruritus. In the authors’ experience, alopecia may be a presenting symptom of underlying uncontrolled SD. SD can also be related to hair breakage (Taylor et al., 2017). When severe, hair breakage associated with SD may be concerning for alopecia.
Clinically, SD of the scalp manifests as mild desquamation or greasy, honey-colored crusts associated with hair loss (Fig. 4). Perifollicular erythema, flaking, scaling, and pruritus may be present, as well as corona seborrheica, which is an erythematous and scaly border of the marginal hairline due to SD (Borda and Wikramanayake, 2015, Pitney et al., 2015). In acute or early stages, histology shows superficial perivascular and perifollicular lymphocytic inflammation with spongiosis and psoriasiform hyperplasia. Chronic SD will demonstrate psoriasiform hyperplasia, parakeratosis, and dilation of surface plexus venules, as seen in psoriasis (Borda and Wikramanayake, 2015).
Fig. 4.

Seborrheic dermatitis. Seborrheic dermatitis associated with scaly hypopigmented and erythematous patches of alopecia across the frontotemporal hairline (Image courtesy of Oma Agbai, MD).
SD must be distinguished from tinea capitis, which may also manifest as scaly patches of hair loss. Dermoscopic examination of alopecic areas due to tinea capitis will display short, broken hairs that appear as black dots. Tinea can be diagnosed with a potassium hydroxide preparation under the microscope or with fungal culture. Psoriasis may also occur on the scalp, but lesions appear as sharply demarcated, thick erythematous plaques with silvery scale. Although the histology of psoriasis and SD is similar, the parakeratosis in psoriasiform lesions is often seen in conjunction with thinning or loss of the granular layer (Borda and Wikramanayake, 2015).
Lichen planopilaris
Lichen planopilaris (LPP) is an inflammatory condition with lymphocytic inflammation of hair follicles leading to scarring alopecia (Errichetti et al., 2018). LPP occurs more commonly in women, although not necessarily in women of color, and often presents between the ages of 30 and 60 years (Cho et al., 2010, Errichetti et al., 2018). LPP is considered a follicular variant of lichen planus, which may be found on the body before, during, or after LPP affects the scalp (Errichetti et al., 2018, Mirmirani et al., 2003).
Clinically, LPP appears as multifocal patches or diffuse hair loss throughout the scalp (Fig. 5). Hairs at lesional margins may show perifollicular erythema and scaling, and follicular markings are often absent (Cho et al., 2010, Mirmirani et al., 2003, Whiting, 2001). Margins of alopecic patches progress outward to create smooth, pale, atrophic polygonal areas of hair loss (Whiting, 2001). The condition often progresses slowly, allowing the remaining hair to conceal affected areas. Symptoms vary by patient, ranging from moderate to severe pruritus, pain, or burning. A positive pull test for anagen hairs can be used to identify active disease (Mirmirani et al., 2003).
Fig. 5.

Lichen planopilaris. Lichen planopilaris in a mature African-American woman (Image courtesy of Oma Agbai, MD).
Clinical variants of LPP-associated alopecia include FFA and Graham-Little-Piccardi-Lassueur syndrome (Fig. 6; Errichetti et al., 2018). LPP and FFA may both display peripilar erythema and white scales. Dermoscopic findings of LPP additionally include keratotic plugs, concentric, elongated blood vessels, violaceous interfollicular areas, and large irregular white dots. Unlike LPP, eyebrows are commonly affected with FFA and may display gray dots under the dermatoscope (Bolduc et al., 2016). Graham-Little-Piccardi-Lassueur syndrome is characterized by patches of scarring alopecia on the scalp in conjunction with non-scarring alopecia of the axillary and pubic areas and follicular papules on the limbs and trunk (Errichetti et al., 2018).
Fig. 6.

Frontal fibrosing alopecia. Overlapping lichen planopilaris and frontal fibrosing alopecia in a mature Asian woman (Image courtesy of Oma Agbai, MD).
Discoid lupus
Discoid lupus erythematosus (DLE) is a chronic variant of cutaneous lupus erythematosus (Whiting, 2001). DLE occurs more commonly in women and patients of color and is one of the most common causes of inflammatory scarring alopecia (Milam et al., 2015, Whiting, 2001). An estimated one-third of patients with DLE will experience cicatricial alopecia (Udompanich et al., 2018).
More than half of patients present with scalp lesions, although DLE also affects the face, ears, and neck (Milam et al., 2015). DLE lesions resemble erythematous plaques with follicular plugging, scale, central hypopigmentation, and epidermal atrophy (Fig. 7; Milam et al., 2015, Udompanich et al., 2018). Sensitivity and pruritus may be present in early lesions (Whiting, 2001). At our clinic, three African American patients with DLE presented with hyperpigmented scaly plaques of the scalp without areas of hypopigmentation (Agbai, clinical observation). Trichoscopy characteristically reveals follicular red dots; branching vessels, large yellow dots, and speckled brown discoloration may also be seen (Udompanich et al., 2018). In late disease, lesions ultimately become atrophic, fibrotic areas with central hypopigmentation and loss of follicular markings (Milam et al., 2015). Irreversible alopecia can result without intervention (Milam et al., 2015, Udompanich et al., 2018).
Fig. 7.

Discoid lupus erythematosus. Hyperpigmented papules within alopecic patch in a middle-aged African-American woman with discoid lupus erythematosus (Image courtesy of Oma Agbai, MD).
Histologically, DLE demonstrates vacuolar interface alteration, mild dyskeratosis, atrophic sebaceous epithelium, and lymphocytic infiltration around follicles, blood vessels, and eccrine glands (Whiting, 2001). Given the often overlapping clinical and histological features, distinguishing hair loss due to DLE or LPP can be difficult. DLE is suggested by the presence of follicular plugging and central hypopigmentation, whereas perifollicular erythema and scale more likely indicate LPP. Excess mucin may be present in both conditions, located perifollicularly in LPP and dermally in DLE. Basement membrane thickening is significant in DLE (Nambudiri et al., 2014). DLE may also resemble folliculitis decalvans and pseudopelade, although differentiation is more challenging once scarring has occurred. In these cases immunofluorescence demonstrating immunoglobulins G or M or complement may aid in the diagnosis of DLE (Whiting, 2001).
Management of trichorrhexis nodosa, seborrheic dermatitis, lichen planopilaris, and discoid lupus erythematosus
Trichorrhexis nodosa
Avoidance of traumatic hair styling practices is paramount in the management of TN. The use of hot combs, curling irons, and flat irons should be limited to temperatures <175 °C, frequency of once a week or less, and on dry hair only (Lawson et al., 2017, Mirmirani, 2010). Similarly, chemical relaxer and dye use should be minimized, especially in combination, because this notably increases the risk of hair breakage. In routine hair care, efforts should be made to reduce friction with the use of conditioners, hair oils, and combs with straight elongated bristles (Lawson et al., 2017).
Seborrheic dermatitis
Because SD is a chronic condition, management involves long-term maintenance aimed at reducing symptoms and clinically visible changes. Topical antifungal and corticosteroid formulations are the cornerstone of maintenance used to counteract excess Malassezia spp. and chronic scalp inflammation. Select antifungal regimens as delineated by Borda and Wikramanayake (2015) include ketoconazole 2% shampoo twice weekly for 4 weeks, then once weekly for maintenance; bifonazole 1% shampoo once daily or every other day; ciclopirox olamine 1.5% shampoo twice weekly for 4 weeks, then once weekly for maintenance; and zinc pyrithione 1% shampoo 2 to 3 times per week. Topical corticosteroids useful in SD include fluocinolone 0.01% solution or shampoo, betamethasone dipropionate 0.05% lotion, and desonide 0.05% lotion or gel. We recommend that women of African descent wash their hair once or twice weekly with the shampoo; more frequent hair washing can lead to excessive drying of the hair shafts and a subsequent increase in hair fragility. Topical pimecrolimus (1% cream) or tacrolimus (0.1% ointment) may be used on affected skin to combat inflammation. Other agents include lithium gluconate or succinate and phototherapy. Large or recalcitrant lesions may require treatment with systemic antifungal agents, including itraconazole or terbinafine (Borda and Wikramanayake, 2015).
Lichen planopilaris
Established management strategies for LPP are based on limited evidence and focus on disease progression and symptom relief (Mirmirani et al., 2003). Although treatment commonly involves use of high-potency topical steroids (e.g., clobetasol propionate), topical corticosteroids and immunomodulators (e.g., pimecrolimus and tacrolimus) are often insufficient as monotherapy (Cho et al., 2010).
Oral corticosteroids have been used to treat LPP after failure of topical therapy (e.g., with prednisone 1 mg/kg/day for 15 days), although this treatment has been associated with high relapse rates (Errichetti et al., 2018). Intralesional corticosteroids can be used to target areas of active disease, such as triamcinolone acetonide suspension 10 mg/ml (Whiting, 2001). The use of azathioprine, antimalarial medications, dapsone, isotretinoin, and cyclosporine has also been described (Mirmirani et al., 2003, Whiting, 2001). One suggested regimen is 200 mg oral hydroxychloroquine, transitioning to cyclosporine (3–5 mg/kg/day) after 2–4 months; however, cyclosporine has been associated with serious adverse effects as well as high relapse rates (Errichetti et al., 2018).
Recent evidence points to mycophenolate mofetil as a safe and effective treatment of recalcitrant LPP (Cho et al., 2010, Errichetti et al., 2018).
Discoid lupus erythematosus
Early intervention in DLE of the scalp is important because affected areas may progress to permanent hair loss. Early DLE may be managed with potent topical, intralesional, and oral corticosteroids. Suggested oral and intralesional regimens include oral prednisone 10–20 mg daily, tapering down over time, as well as intralesional triamcinolone acetonide 10 mg/ml every 4–6 weeks (Whiting, 2001). Topical calcineurin inhibitors are also commonly used and are particularly useful in areas with thinning or atrophy (Udompanich et al., 2018).
Most regimens described in the literature have used low-potency tacrolimus ointment (0.03%–0.1%). A recent study by Milam et al. (2015) demonstrated effectiveness with off-label higher-potency tacrolimus 0.3% lotion. Limited data point to potential benefits from oral antimalarial agents, mycophenolate mofetil, methotrexate, retinoids, dapsone, and thalidomide (Udompanich et al., 2018). Smoking cessation and sunscreen use may prevent formation of new lesions (Udompanich et al., 2018).
Conclusion
Certain types of alopecia, such as traction alopecia, occur at higher rates in African-American women. Both intrinsic hair qualities and hair care practices play a role in certain types of alopecia in this group. Biochemical and morphological differences in the hair shaft and follicle contribute to lower baseline tensile strength, hair density, and growth rates in this group compared with Caucasian patients. Hair styling practices prevalent in this ethnic group, such as the use of high-tension braids, weaves, and cornrows, also play a role in some alopecic subtypes. Alopecia can also occur as a result of DLE, LPP, and less commonly SD. Recognizing and differentiating these alopecic subtypes clinically and histopathologically is important for prompt diagnosis and treatment.
Conflict of Interest
None.
Funding
None.
Study Approval
The authors confirm that any aspect of the work covered in this manuscript that has involved human patients has been conducted with the ethical approval of all relevant bodies.
Footnotes
No human subjects were included in this study. No animals were used in this study.
References
- Ahdout J., Mirmirani P. Weft hair extensions causing a distinctive horseshoe pattern of traction alopecia. J Am Acad Dermatol. 2012;67:e294–e295. doi: 10.1016/j.jaad.2012.07.020. [DOI] [PubMed] [Google Scholar]
- Bolduc C., Sperling L., Shapiro J. Primary cicatricial alopecia: Lymphocytic primary cicatricial alopecias, including chronic cutaneous lupus erythematosus, lichen planopilaris, frontal fibrosing alopecia, and Graham-Little syndrome. J Am Acad Dermatol. 2016;75(6):1081–1099. doi: 10.1016/j.jaad.2014.09.058. [DOI] [PubMed] [Google Scholar]
- Borda L.J., Wikramanayake T.C. Seborrheic dermatitis and dandruff: a comprehensive review. J Clin Invest Dermatol. 2015;3(2):10. doi: 10.13188/2373-1044.1000019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burns T., Breathnach S., Cox N., Griffiths C. 8th ed. Blackwell; Oxford: 2010. Rook’s textbook of dermatology; pp. 2329–2330. [Google Scholar]
- Cho B.K., Sah D., Chwalek J., Rosenborough I., Ochoa B., Chiang C. Efficacy and safety of mycophenolate mofetil for lichen planopilaris. J Am Acad Dermatol. 2010;62(3):393–397. doi: 10.1016/j.jaad.2009.05.018. [DOI] [PubMed] [Google Scholar]
- Davis D.S., Callendar V.D. Review of quality of life studies in women with alopecia. Int J Womens Dermatol. 2018;4(1):18–22. doi: 10.1016/j.ijwd.2017.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis S.A., Narahari S., Feldman S.R., Huang W., Pichardo-Geisinger R.O., McMichael A.J. Top dermatologic conditions in patients of color: an analysis of nationally representative data. J Drugs Dermatol. 2012;11(4):466–473. [PubMed] [Google Scholar]
- Errichetti E., Figini M., Croatto M., Stinco G. Therapeutic management of classic lichen planopilaris: a systematic review. Clin Cosmet Investig Dermatol. 2018;2018(11):91–102. doi: 10.2147/CCID.S137870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franbourg A., Hallegot P., Baltenneck F., Toutain C., Leroy F. Current research on ethnic hair. J Am Acad Dermatol. 2003;48(Suppl 6):S115–S119. doi: 10.1067/mjd.2003.277. [DOI] [PubMed] [Google Scholar]
- Griffin M, Lenzy Y. Contemporary African-American hair care practices [Internet]. 2015 [cited 2018 August 21]. Available from: https://practicaldermatology.com/articles/2015-may/contemporary-african-american-hair-care-practices?c4src=article:infinite-scroll.
- Haskin A., Kwatra S.G., Aguh C. Breaking the cycle of hair breakage: pearls for the management of acquired trichorrhexis nodosa. J Dermatol Treat. 2017;28(4):322–326. doi: 10.1080/09546634.2016.1246704. [DOI] [PubMed] [Google Scholar]
- Heath C.R., Taylor S.C. Alopecia in an ophiasis pattern: traction alopecia versus alopecia areata. Cutis. 2012;89:213–216. [PubMed] [Google Scholar]
- Ji J.H., Park T.S., Lee H.J., Kim Y.D., Pi L.Q., Jin X.H. The ethnic differences of the damage of hair and integral hair lipid after ultra violet radiation. Ann Dermatol. 2013;25:54–60. doi: 10.5021/ad.2013.25.1.54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khumalo NP, African hair morphology: macrostructure to ultrastructure. Int J Dermatol. 2005;Oct;44 Suppl 1:10-2. [DOI] [PubMed]
- Khumalo N.P., Jessop S., Gumedze F., Ehrlich R. Hairdressing and the prevalence of scalp disease in African adults. Br J Dermatol. 2007;157:981–988. doi: 10.1111/j.1365-2133.2007.08146.x. [DOI] [PubMed] [Google Scholar]
- Khumalo N.P., Jessop S., Gumedze F., Ehrlich R. Hairdressing is associated with scalp disease in African schoolchildren. Br J Dermatol. 2007;157(1):106–110. doi: 10.1111/j.1365-2133.2007.07987.x. [DOI] [PubMed] [Google Scholar]
- Lawson C.N., Hollinger J., Sethi S., Rodney I., Sarkar R., Dlova N. Updates in the understanding and treatments of skin & hair disorders in women of color. Int J Womens Dermatol. 2017;3(1 Suppl):S21–S37. doi: 10.1016/j.ijwd.2017.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee W.S., Oh T.H., Chun S.H., Jeon S.Y., Lee E.Y., Lee S. Integral lipid in human hair follicle. J Investig Dermatol Symp Proc. 2005;10(3):234–237. doi: 10.1111/j.0022-202X.2005.10113.x. [DOI] [PubMed] [Google Scholar]
- Lewallen R., Francis S., Fisher B., Richards J., Li J., Dawson T. Hair care practices and structural evaluation of scalp and hair shaft parameters in African American and Caucasian women. J Cosmet Dermatol. 2015;14(3):216–223. doi: 10.1111/jocd.12157. [DOI] [PubMed] [Google Scholar]
- Lindelof B., Forslind B., Hedblad M.A. Kaveus U. Human hair form. Morphology revealed by light and scanning electron microscopy and computer aided three-dimensional reconstruction. Arch Dermatol. 1988;124:1359–1363. [PubMed] [Google Scholar]
- McMichael A.J. Ethnic hair update: past and present. J Am Acad Dermatol. 2003;48(Suppl 6):S127–S133. doi: 10.1067/mjd.2003.278. [DOI] [PubMed] [Google Scholar]
- Milam E.C., Ramachandran S., Franks A.G., Jr. Treatment of scarring alopecia in discoid variant of chronic cutaneous lupus erythematosus with tacrolimus lotion, 0.3% JAMA Dermatol. 2015;151(10):1113–1116. doi: 10.1001/jamadermatol.2015.1349. [DOI] [PubMed] [Google Scholar]
- Mirmirani P. Ceramic flat irons: improper use leading to acquired trichorrhexis nodosa. J Am Acad Dermatol. 2010;62:145–147. doi: 10.1016/j.jaad.2009.01.048. [DOI] [PubMed] [Google Scholar]
- Mirmirani P., Khumalo N.P. Traction alopecia: How to translate study data for public education—closing the KAP gap? Dermatol Clin. 2014;32(2):153–161. doi: 10.1016/j.det.2013.12.003. [DOI] [PubMed] [Google Scholar]
- Mirmirani P., Wiley A., Price V.H. Short course of oral cyclosporine in lichen planopilaris. J Am Acad Dermatol. 2003;49(4):667–671. doi: 10.1067/s0190-9622(03)00873-9. [DOI] [PubMed] [Google Scholar]
- Miyamoto M., Tsuboi R., Oh-I T. Case of acquired trichorrhexis nodosa: scanning electron microscopic observation. J Dermatol. 2009;36(2):109–110. doi: 10.1111/j.1346-8138.2009.00600.x. [DOI] [PubMed] [Google Scholar]
- Nambudiri V.E., Vleugels R.A., Laga A.C., Goldberg L.J. Clinicopathologic lessons in distinguishing cicatricial alopecia: 7 cases of lichen planopilaris misdiagnosed as discoid lupus. J Am Acad Dermatol. 2014;71(4):e135–e138. doi: 10.1016/j.jaad.2014.04.052. [DOI] [PubMed] [Google Scholar]
- Ogunleye T.A., McMichael A., Olsen E.A. Central centrifugal cicatricial alopecia: what has been achieved, current clues for future research. Dermatol Clin. 2014;32(2):173–181. doi: 10.1016/j.det.2013.12.005. [DOI] [PubMed] [Google Scholar]
- Okereke U.R., Simmons A., Callender V.C. Current and emerging treatment strategies for hair loss in women of color. Int J Womens Dermatol. 2019;5(1):37–45. doi: 10.1016/j.ijwd.2018.10.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perry P.K., Cook-Bolden F.E., Rahman Z., Jones E., Taylor S.C. Defining pseudofolliculitis barbae in 2001: a review of the literature and current trends. J Am Acad Dermatol. 2002;46(2 Suppl Understanding):S113–S119. doi: 10.1067/mjd.2002.120789. [DOI] [PubMed] [Google Scholar]
- Piérard-Franchimont C., Goffin V., Henry F., Uhoda I., Braham C., Piérard G.E. Nudging hair shedding by antidandruff shampoos. A comparison of 1% ketoconazole, 1% piroctone olamine and 1% zinc pyrithione formulations. Int J Cosmet Sci. 2002;24:249–256. doi: 10.1046/j.1467-2494.2002.00145.x. [DOI] [PubMed] [Google Scholar]
- Piérard-Franchimont C., Xhauflaire-Uhoda E., Piérard G.E. Revisiting dandruff. Int J Cosmet Sci. 2006;28:311–318. doi: 10.1111/j.1467-2494.2006.00326.x. [DOI] [PubMed] [Google Scholar]
- Pitney L., Weedon D., Pitney M. Is seborrhoeic dermatitis associated with a diffuse, low-grade folliculitis and progressive cicatricial alopecia? Australas J Dermatol. 2015;57(3):e105–e107. doi: 10.1111/ajd.12289. [DOI] [PubMed] [Google Scholar]
- Richards G.M., Oresajo C.O., Halder R.M. Structure and function of ethnic skin and hair. Dermatol Clin. 2003;21(4):595–600. doi: 10.1016/s0733-8635(03)00081-0. [DOI] [PubMed] [Google Scholar]
- Samrao A., Price V.H., Zedek D., Mirmirani P. The, “fringe sign” – a useful clinical finding in traction alopecia of the marginal hair line. Dermatol Online J. 2011;17(11):1. [PubMed] [Google Scholar]
- Sperling L.C. Hair density in African Americans. Arch Dermatol. 1999;135(6):656–658. doi: 10.1001/archderm.135.6.656. [DOI] [PubMed] [Google Scholar]
- Taylor S.C. Skin of color: biology, structure, function, and implications for dermatologic disease. J Am Acad Dermatol. 2002;46(2 Suppl):S41–S62. doi: 10.1067/mjd.2002.120790. [DOI] [PubMed] [Google Scholar]
- Taylor S.C., Barbarosa V., Burgess C., Heath C., McMichael A.J., Ogunleye T. Hair and scalp disorders in adult and pediatric patients with skin of color. Cutis. 2017;100(1):31–35. [PubMed] [Google Scholar]
- Tosti A., Miteva M., Torres F., Vincenzi C., Romanelli P. Hair casts are a dermoscopic clue for the diagnosis of traction. Br J Dermatol. 2010;163(6) doi: 10.1111/j.1365-2133.2010.09979.x. [DOI] [PubMed] [Google Scholar]
- Udompanich S., Chanprapaph K., Suchonwanit P. Hair and scalp changes in cutaneous and systemic lupus erythematosus. Am J Clin Dermatol. 2018;19(5):679–694. doi: 10.1007/s40257-018-0363-8. [DOI] [PubMed] [Google Scholar]
- Whiting D.A. Cicatricial alopecia: clinicopathological findings and treatment. Clin Dermatol. 2001;9(2):211–225. doi: 10.1016/s0738-081x(00)00132-2. [DOI] [PubMed] [Google Scholar]