

Madam,
We present this prospective observational pilot study to determine if there is a correlation between inferior vena cava collapsibility index (IVCCI) and intraoperative fluid requirements in patients undergoing elective surgery.
Background: The use of point of care ultrasound in the perioperative arena has recently gained momentum.[1] Studies have shown its application in critical care; however, only a few have investigated specific applications of ultrasonography to alter perioperative care.[2] Inferior vena cava (IVC) collapsibility measured by ultrasound has been used for the assessment of volume status and fluid responsiveness in non-operative hospital settings.[3] Recently, the preoperative measurement of IVC collapsibility was correlated with hypotension after the induction of general anesthesia showing a moderate correlation (r = 0.46) between a drop in mean arterial blood pressure after induction and IVCCI.[4] However, the use of IVC measurements in the preoperative setting has not been investigated to identify hypovolemic elective surgery patients.
Methods: This prospective observational study was performed after IRB approval from the University. Written informed consent was obtained from 55 adult patients undergoing non-emergent surgery who were expected to receive general anesthesia.
In the preoperative holding area, a single window ultrasound evaluation was performed using a Sonosite® X-Porte Ultrasound (Fujifilm Sonosite, Bothell, WA, USA) with 5 MHz-phased array probe while the patient was supine. Subcostal longitudinal views of the IVC in the retrohepatic region were obtained and IVCCI determined as previously described by Zhang et al.[4] The intraoperative course was not protocolized, and anesthetic management was up to the discretion of individual practitioners.
Using previously published data showing a moderate correlation (r = 0.46) for IVCCI and decrease in mean arterial pressure (MAP) after the induction of general anesthesia,[4] a sample size of 45 was calculated to detect an equally strong correlation to fluid administered. A plot of IVCCI and fluid administered intraoperatively calculated as ml kg−1 hr−1 was created using linear regression. Bivariate Pearson correlation was calculated using IBM SPSS version 24 software.
Results: A total of 55 patients were enrolled in the study. Seven patients were excluded from the analysis due to missing data or unobtainable images. Of the 48 included patients, 42 were American Society of Anesthesiologists (ASA) class 1 or 2 and only 4 patients were receiving antihypertensive medications. The IVCCI ranged from 1.9% to 74.1% with a mean CI of 32% [Table 1]. The Pearson correlation (R) for IVCCI to fluid administered intraoperatively was 0.24, with wide variance and poor fit [Figure 1].
Table 1.
Demographic data of patients included in the study
| Age (yrs) | 42±15.9 |
| Weight (kg) | 73.6±14.7 |
| Gender: Male (number/%) | 34/71 |
| Gender: Female (number/%) | 14/29 |
| BMI (kg/m2) | 26.2±5.3 |
| ASA 1 (number) | 10 |
| ASA 2 (number) | 29 |
| ASA 3 (number) | 8 |
| ASA 4 (number) | 1 |
| Cardiac disease (number) | 6* |
| Propofol dose (mg/kg) | 1.87±0.68 |
| Baseline MAP (mmHg) | 91.8±13.9 |
| IVCCI (%) | 32±17 |
*4 with uncontrolled hypertension, 1 patient with CAD/CHF, 1 patient with aortic stenosis
Figure 1.
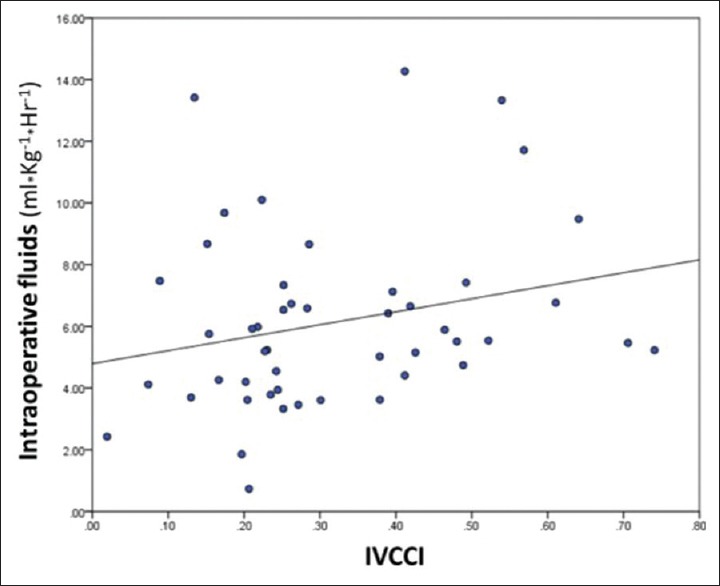
Distribution of IVCCI and amount of fluid administered intraoperatively
Hypotension after induction, defined as a MAP of less than 60 mmHg within 10 minutes of induction, was present in 10 of the 48 patients. Hypotension at any point in the case was present in 26 of the 48 patients with a broad range of duration from 1 to 108 minutes of hypotension. The average IVCCI for those patients who did exhibit hypotension was 33% ±18% (25.7–40.4%) compared to 30.8% ±15% (23.8–37.7%) for those who did not experience intraoperative hypotension (P = 0.60) [Figure 2].
Figure 2.
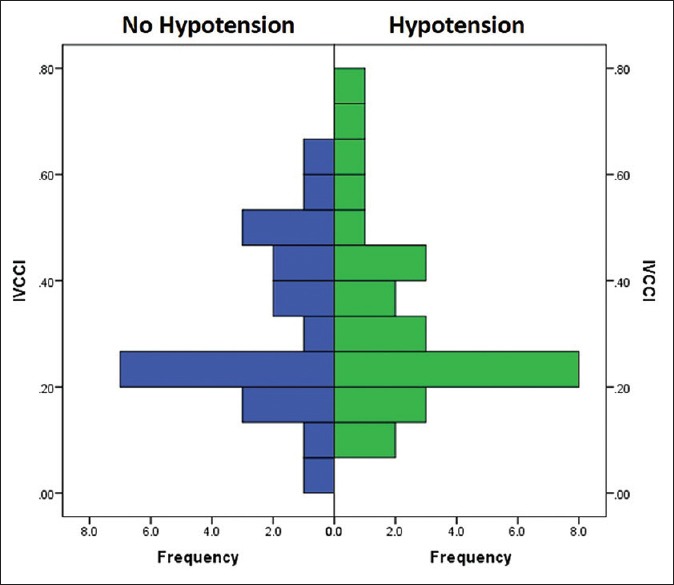
IVCCI comparison of patients who experienced hypotension compared to those that did not
Discussion: This pilot study demonstrated a broad range of preoperative IVCCI in elective surgery patients. The mean IVCCI of 32% in our study had a poor correlation with fluid responsiveness or hypotension. This might indicate that the point of care echocardiography parameters established for critically ill and acutely decompensated patients would not necessarily apply to patients presenting for elective surgery. Although in specific high-risk patients’ perioperative TTE is useful for diagnosis and management,[5] this may need further evaluation as a screening tool preoperatively.[6] When preoperative focused ultrasonography is performed in urgent surgery, it was only able to provide some clinically useful information to change management in sicker (ASA class ≥ 3) and older (Age > 60) patients.[2]
In perioperative patients, a previous study has correlated IVCCI with changes in MAP after induction, which determined our pretest expectation of correlation with intraoperative fluids.[4] In the study by Zhang et al.[4] there was a good correlation between IVCCI and hypotension after induction. However, the relationship between IVCCI does not seem to translate to changes as far as volume requirements intraoperatively and could be due to the static cross-sectional measurement prior to a dynamic intraoperative period. A more effective strategy could entail targeting perioperative ultrasonography to evaluate preoperative hydration in patients who are at increased risk of hemodynamic instability or who present more challenging cases of fluid management. This presents an avenue for further clinical investigation.
In conclusion, the preoperative IVCCI of our general elective surgery population did not correlate with the volume of fluid administered intraoperatively.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Ramsingh D, Gudzenko V, Martin RD. Point-of-care ultrasound: Novel technology to routine perioperative assessment tool. Anesth Analg. 2017;124:709–11. doi: 10.1213/ANE.0000000000001529. [DOI] [PubMed] [Google Scholar]
- 2.Bøtker MT, Vang ML, Grøfte T, Sloth E, Frederiksen CA. Routine pre-operative focused ultrasonography by anesthesiologists in patients undergoing urgent surgical procedures. Acta Anaesthesiol Scand. 2014;58:807–14. doi: 10.1111/aas.12343. [DOI] [PubMed] [Google Scholar]
- 3.Corl KA, George NR, Romanoff J, Levinson AT, Chheng DB, Merchant RC, et al. Inferior vena cava collapsibility detects fluid responsiveness among spontaneously breathing critically-ill patients. J Crit Care. 2017;41:130–7. doi: 10.1016/j.jcrc.2017.05.008. [DOI] [PubMed] [Google Scholar]
- 4.Zhang J, Critchley LA. Inferior Vena Cava Ultrasonography before General Anesthesia Can Predict Hypotension after Induction. Anesthesiology. 2016;124:580–9. doi: 10.1097/ALN.0000000000001002. [DOI] [PubMed] [Google Scholar]
- 5.Kratz T, Steinfeldt T, Exner M, Dell Orto MC, Timmesfeld N, Kratz C, et al. Impact of focused intraoperative transthoracic echocardiography by anesthesiologists on management in hemodynamically unstable high-risk noncardiac surgery patients. J Cardiothorac Vasc Anesth. 2017;31:602–9. doi: 10.1053/j.jvca.2016.11.002. [DOI] [PubMed] [Google Scholar]
- 6.Gui J, Yang Z, Ou B, Xu A, Yang F, Chen Q, et al. Is the Collapsibillity index of the inferior vena cava an accurate predictor for the early detection of intravascular volume change? Shock. 2017 doi: 10.1097/SHK.0000000000000932. doi: 10.1097/SHK.0000000000000932. [DOI] [PubMed] [Google Scholar]