

Abstract
There is a lack of population-based surveys on oral health in Jilin province. Accordingly, this study aimed to understand the oral health status of 12-year-old children in Jilin province, China, to demonstrate the prevalence of oral health–related diseases, as well as to identify the associated risk factors.
From February to April 2017, a cross-sectional investigation was conducted among 2324 children aged 12 years from 63 public schools of 9 regions in Jilin province, China. A questionnaire of World Health Organization (WHO) was conducted to ascertain the potential risk factors associated with oral diseases. The 3 examiners, who received theoretical and clinical training before the investigation, underwent clinical examinations to assess dental caries, dental fluorosis, presence of calculus, and gingival bleeding. Furthermore, the mean decayed-missing-filled tooth (DMFT), the rate of pit and fissure closure, education level of patients, brushing habits, and sugar consumption were also evaluated. All data analyses were conducted using SPSS version 19.0.
A total of 2324 twelve-year-old children from 9 regions in Jilin-China were examined from February to April 2017. The prevalence of dental caries, dental fluorosis, calculus, and gingival bleeding reached 40.8%%, 21.8%, 47.93%, and 48.88%, respectively; the mean DMFT was 0.8787. The proportion of DMFT was 83.7% for decayed teeth, 0.2% for missing teeth, and 16.1% for filling teeth. The prevalence of pit and fissure closure was 10%.
Educational level of parents was negatively correlated with the prevalence of oral diseases, whereas sugar consumption was positively associated with dental caries prevalent in children. We also found that there was no association between brushing habits and dental caries in children aged 12 years in Jilin Province.
Keywords: children, dental caries, epidemiological, oral health
1. Introduction
Oral health–related diseases (e.g., dental caries, gingival bleeding, calculus, fluorosis, and oral mucositis) have been affecting humans for a long time.[1–7] Thus far, about 3.9 billion people have been affected all over the word.[8] Oral health–related diseases are a greater economic burden on citizens and also impose a huge burden on the healthcare system of government.[9] Currently, the national strategy for healthcare has been shifting gradually to prevention-orientated care, and oral health care should also follow this lead and shift from a treatment-orientated care to a prevention-orientated care.[10,11] Thus, investigation in representational groups is the first step to prevent oral health–related diseases. This study aimed to conduct an epidemiological survey on oral health conditions in a representative population of 12-year-old children to verify the prevalence of oral diseases, as well as to determine its associated risk factors in Jilin province of China.
2. Ethical approval
Ethical approval for the study was obtained from the Jilin University Stomatological Hospital. Informed consent to examine the children was obtained from parents, and assent was obtained from children before examination.
3. Methods
3.1. Survey subjects and regions
A total of 2324 twelve-year-old children were taken as the subjects in 2017. The questionnaire survey was conducted with collective self-answer questionnaire according to Sun et al,[12] and the survey data were analyzed with SPSS19.0 statistical software. Nine regions (Fig. 1) in the Jilin province of China, including Changchun, Yanji, Huadian, Baishan, Siping, Meihekou, Baicheng, Nong’an, and Changling, were taken as the survey regions.
Figure 1.
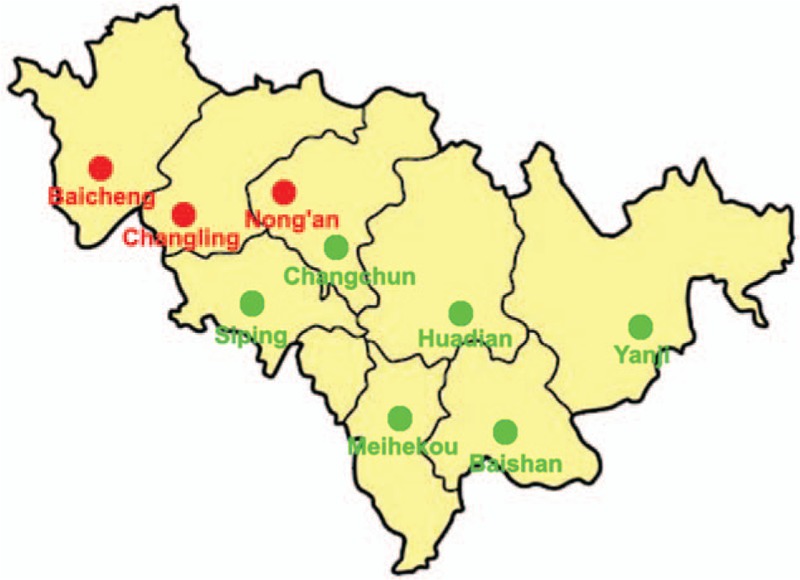
Nine regions were surveyed in Jilin province, China. Red dots and green dots represent high-fluoride regions and non–high-fluoride regions, respectively.
3.2. Survey items and methodology
Unified inspection instruments were employed in the investigation, including plane oral mirror, Community Periodontal Index probe, and instruments disc (Zhejiang Beikang Medical Technology Co, Ltd, Hangzhou, China). Checklist design, survey methods, and standards were all consistent with the basic method of WHO oral health survey (5th edition).[13] Dental caries, gingival bleeding, and the presence of calculus and fluorosis were investigated. In addition, average caries, the rate of pit and fissure closure education background of patients, brushing habits, and sugar consumption were evaluated as well.
3.3. Quality control
The Kappa values of standard consistency test were generally >0.81. During the investigation, 5% of the respondents were randomly sampled for review, and the Kappa values were overall >0.81.
3.4. Statistical analysis
EpiData 3.1 software (The EpiData Association, Odense, Denmark) was adopted to create data table files, double-track input of the same data, and build a database. After logical checking, the data were analyzed with SPSS19.0 software (IBM SPSS, IBM Corp, Armonk, NY). The classification data were expressed by the number of cases (percentage), and the Pearson χ2 test was performed for comparison between groups. Chi-square test was performed to compare the dental fluorosis rate and periodontal condition between various groups and the relevant factors. Nonparametric test was performed to assess the mean difference between different groups. The statistical test level α was set to 0.05.
4. Results
4.1. Dental caries and decayed-missing-filled tooth
In the present study, a total of 2324 twelve-year-old children were surveyed, of whom 948 were found to have dental caries, and the prevalence of dental caries reached 40.8% (Table 1). The prevalence of calculus and gingival bleeding reached 47.93% and 48.88%, respectively. The mean decayed-missing-filled tooth (DMFT) was 0.8787, and the proportion of DMFT was 83.7% for decayed teeth, 0.2% for missing teeth, and 16.1% for filling teeth. The average caries of permanent teeth was 0.865. The pit and fissure closure rate was 10%. The details are shown in the Figures 2 to 4.
Table 1.
The prevalence of oral health-related diseases in 12-year-old children.
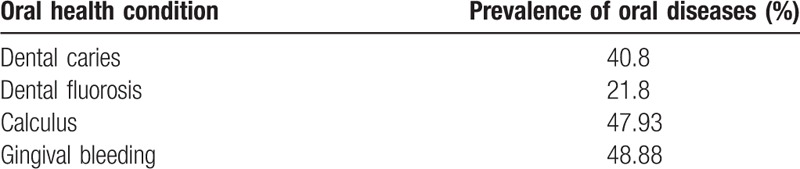
Figure 2.
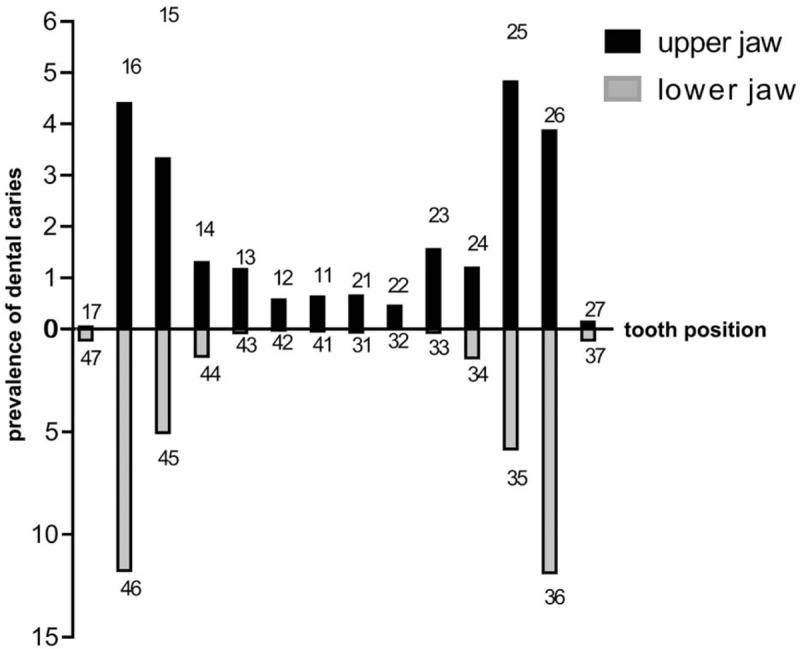
The prevalence of dental caries in the upper and lower jaws.
Figure 4.
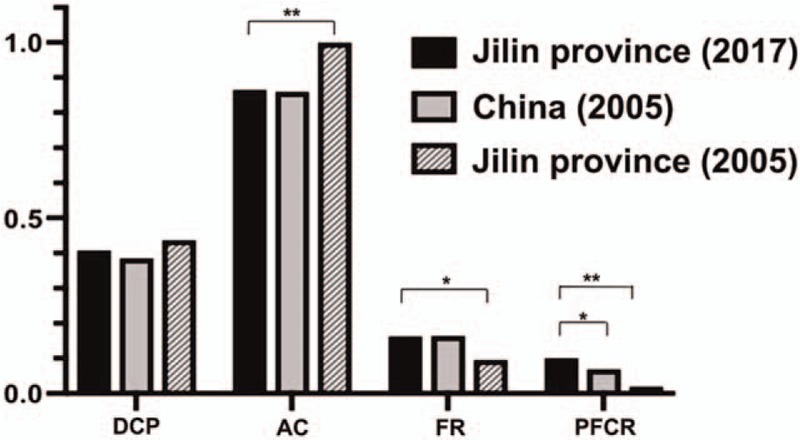
Comparison of dental caries prevalence (DCP), average caries (AC), filling rate (FR), and pit and fissure closure rate (PFCR) between 2017 and 2005 in Jilin Province, and comparison of caries incidence, average caries, filling rate, and pit and fissure closure rate between Jilin Province and China in 2017. ∗P < .05, and ∗∗P < .01.
Figure 3.
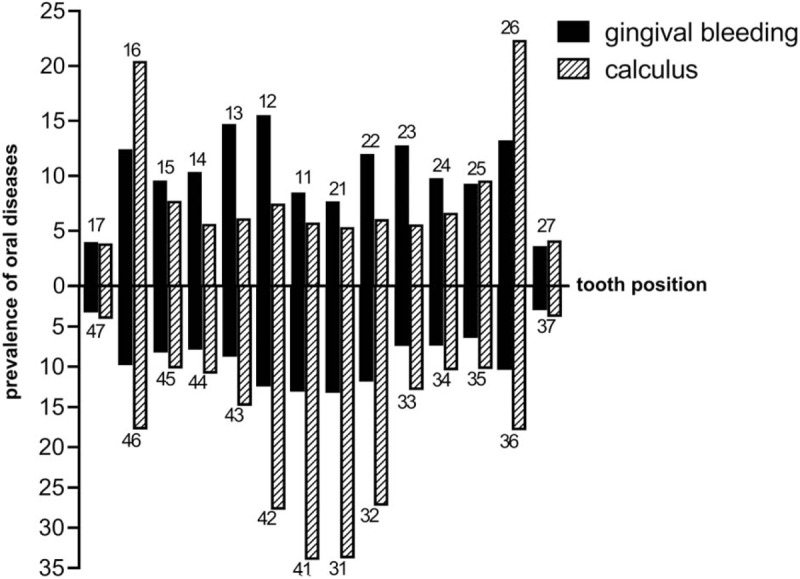
The prevalence of calculus and gingival bleeding in the upper and lower jaws.
4.2. Dental fluorosis
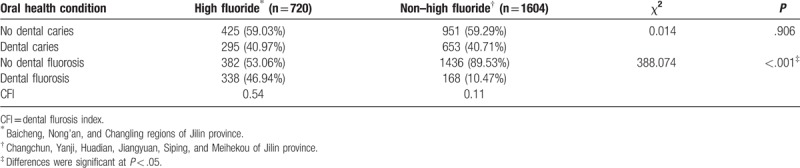
We used Dean index,[13] recommended by WHO, to calculate the prevalence of dental fluorosis.[14] The prevalence of dental fluorosis was 21.8% in Jilin, and the incidence of dental fluorosis in high-fluoride (46.9%) and that of non–high-fluoride (10.47%) regions of Jilin province were compared (Table 2).
Table 2.
The prevalence of oral diseases in high-fluoride and non–high-fluoride regions in Jilin province, China.
4.3. The relationship between education level of patients, brushing habits, sugar consumption, and dental caries
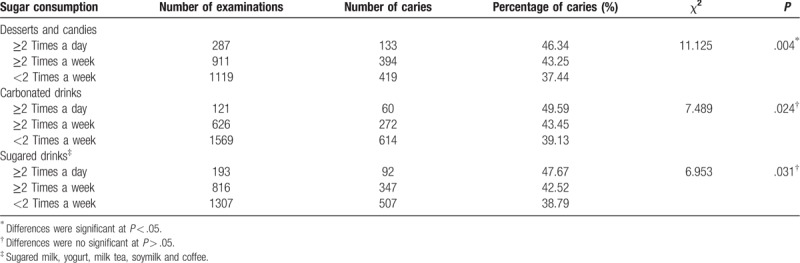
The incidence of dental caries was inversely correlated with the educational background of parents (P < .05) (Table 3). Sugar consumption (e.g., desserts and candies) can induce dental caries (P < .05), whereas no statistical significance of carbonated drinks and sugared drinks could cause dental caries (P > .05) (Table 4). In addition, brushing could induce dental caries without statistical significance (P > .05) Table 5).
Table 3.
Caries prevalence in different family factors.
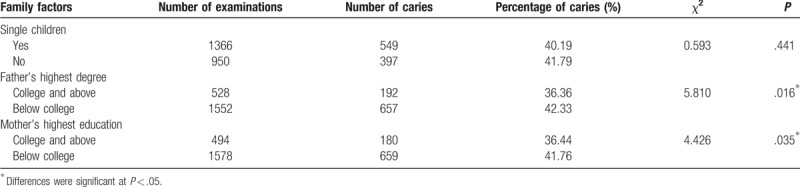
Table 4.
Caries prevalence in different brush habits.

Table 5.
The caries rate of 12-year-old children corresponding to various sweets.
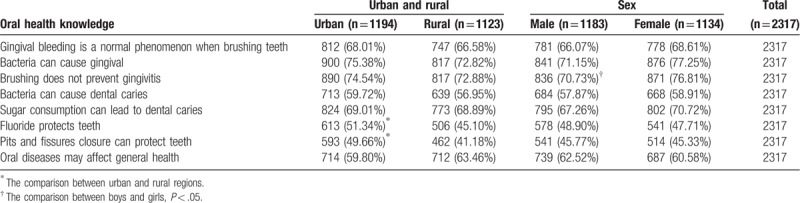
4.4. The awareness of oral health knowledge in 12-year-old children
Children knowing that pit and fissure closure can prevent dental caries in the urban were higher than the rural in Jilin province (P < .05), and those knowing that brushing can prevent gingivitis in boys were lower than that in girls (P < .05).
Among the children, 68.9% know that sugar consumption can cause dental caries, 45.5% know that pit and fissure closure can prevent dental caries, and 61.5% know that fluoride can prevent dental caries (Table 6).
Table 6.
The awareness of oral health knowledge in the population.
5. Discussion
It is essential to know exactly about oral health conditions of population, as an attempt to make prevention strategies, to determine medical requires, and to assess the periodical effect of public oral health strategies on addressing these troubles.[15–19] To the best of our knowledge, last information on dental caries in Jilin was surveyed in 2005, and these data do not represent the latest situation. Thus, there was a lack of prevalence data on oral diseases in the Jilin-China, especially in children. Thus, this report aims to report the prevalence of oral health–related diseases and to determine the risk factors affecting oral health, as an attempt to make prevention strategies.
The oral health knowledge and behavior of 12-year-old children can reflect the situation that students acquire oral health knowledge and nurture oral health habits. Accordingly, 12-year-old children are a crucial population in WHO oral epidemiological sampling survey.[5,13,20] In addition, all permanent teeth, which except third molars, have erupted in aged 12. This age was applied for monitoring of disease trends globally.[21]
Dental caries is a common oral disease in childhood. In this study, the prevalence of dental caries was 40.8%, which is similar to 40% prevalence described in Tamil Nadu, India,[22] but still high than those of Nigeria (13.9%),[23] Kashmir (25%),[24] and Sudan (30.5%).[25] Numerous factors, including sample size, dietary behaviors, brushing habits, and cultural difference, could induce these different prevalence figures.
For the DMFT, we identified a DMFT mean of 0.8787. This value was lower than those of other countries, including 1.4 in São Paulo,[26] 2.04 in Brazil,[27] and 1.6 in Quito, capital of Ecuador.[5]
For the dental fluorosis, fluoride, defined as a chemical compound, is critical to prevent and control dental caries.[4] The mineralized tissues of the teeth was directly affected by dental fluorosis.[28] The mean prevalence of dental fluorosis was 21.8% in the Jilin province, higher than the rates reported from China (13.4%) among 12-year-old children in recent epidemiological survey.[29] Dental fluorosis prevalence in high fluoride of Jilin was 46.94%, which was extremely higher than the global averages.[30] We believe that the high incidence of dental fluorosis may be associated with the high fluoride content in Jilin Province. Literature reported that increasing fluoride in drinking water is a rapid and feasible way to avoid dental caries,[31] and we think this is part of the reason why the incidence of dental caries in Jilin province(40.8%) is lower than those in other developing countries(Quito-Ecuador, 78%[5]; Riyadh-Saudi Arabia, 64.98%[32]; Kulasekharam-India, 77%[33]).
Given calculus and gingival bleeding, we compared the prevalence of calculus and gingival bleeding among 12-year-old boys and girls in Jilin Province. It was observed that boys had a higher incidence than did girls. We believe that the reason for the poor periodontal condition of boys may be correlated with less carefully brushing their teeth in boy population. Therefore, parents should focus on the effect of children's tooth brushing.
Given the rate of pit and fissure closure, the rate of pit and fissure closure was 10%, which was higher than that in China with lower prevalence of dental caries in 2005 (6.9%). We believe that active pit and fissure closure can effectively prevent dental caries and attribute these positive results to the oral health education and free pit and fissure closure carried out in Jilin province abiding by China's National Policy in recent years.
For the sugar consumption, we found that desserts and candies are an important risk factor for dental caries, whereas carbonated drinks and sugared drinks without risk for dental caries were found; Peres et al[34] agreed the viewpoint that sugar consumption may lead to dental caries.
Literatures suggested that tooth brushing can effectively prevent oral disease in children.[35–37] However, other studies have shown no correlation between prevalence and tooth brushing.[38,39] Although the reason for this uncorrelation was unclear, it was considered that life habits (e.g., sleep, snacking[39]) influenced the prevalence of dental caries. In the present survey, dental caries experience was similar between tooth brushing and nontooth brushing children. We considered that it is to some extent related to the incorrect way children brush their teeth, as well as due to majority children do not understand the concept that tooth brushing can prevent dental caries. Accordingly, oral health professionals should strengthen propagation and education of the dental health knowledge and assist parents to improve their tooth brushing habits.
In addition, Sun et al[2] suggested the later children start brushing their teeth, the greater their dental caries prevalence will be gained at the age of 5, and provided evidence of higher dental caries prevalence with each passing year tooth brushing is delayed. However, our findings revealed that <9% children in Jilin province had started tooth brushing before the age of 5 years. At present, early tooth brushing is obviously not the societal norm,[2] and our results are consistent with the current situation in China. As a result, this is the reason why the dental caries prevalence of children in Jilin Province is high. Further studies are needed to access the risk indicators confirmed as significantly associated with dental caries.
For oral mucositis, it is a frequent infection among immunocompromised patients,[40] and causes pain, dysphagia, xerostomia, and lastly septicemia.[1,2,41] It affects functions such as speaking, eating, dental, and drinking.[41,42] Oral mucositis always requires systemic analgesics, physical therapy, psychological therapy, oral care, and adjunctive medications.[43] Regretfully, we did not investigate the oral mucositis prevalence of children in the present study. However, it is still an important risk indicator for oral diseases.
6. Conclusion
Educational level of parents was negatively correlated with the prevalence of oral diseases, whereas sugar consumption was positively associated with dental caries prevalent in children. We also found that there was no association between brushing habits and dental caries in 12-year-old children in Jilin Province. In addition, the prevalence of dental fluorosis in high fluoride of Jilin remained higher than global averages. Oral health strategies, including oral health service utilization, effect of brushing teeth, and levels of water fluoride, are required to optimize for Jilin province of China.
Author contributions
Data curation: Hong Zhang, Xiaoxuan Liu.
Investigation: Chong Chen, Rui Wang.
Methodology: Fenglan Zhang.
Project administration: Xiaoxuan Liu.
Validation: Zhimin Zhang.
Writing – original draft: Aobo Du, Hong Zhang.
Writing – review and editing: Zhimin Zhang, Rui Wang.
Footnotes
Abbreviations: DMFT = decayed-missing-filled tooth, WHO = World Health Organization.
How to cite this article: Du A, Zhang H, Chen C, Zhang F, Liu X, Zhang Z, Wang R. Oral health of 12-year-old children in Jilin province, China: a population-based epidemiological survey. Medicine. 2019;98:51(e18463).
AD and HZ contributed equally to this work.
The authors have no conflicts of interest to disclose.
References
- [1].Rodrigues CF, Henriques M. Oral mucositis caused by Candida glabrata biofilms: failure of the concomitant use of fluconazole and ascorbic acid. Ther Adv Infect Dis 2017;4:10–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Nemes J, Jenei A, Marton I. Oral mucositis as the most common complication of childhood cancer therapy. Review of the literature. Orv Hetil 2018;159:495–502. [DOI] [PubMed] [Google Scholar]
- [3].Wojcik D, Krzewska A, Szalewski L, et al. Dental caries and vitamin D3 in children with growth hormone deficiency: a STROBE compliant study. Medicine (Baltimore) 2018;97:e9811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Dalledone M, Cunha AS, Ramazzotto LA, et al. Estrogen receptor gene is associated with dental fluorosis in Brazilian children. Clin Oral Investig 2019;23:3565–70. [DOI] [PubMed] [Google Scholar]
- [5].Michel-Crosato E, Raggio DP, Coloma-Valverde ANJ, et al. Oral health of 12-year-old children in Quito, Ecuador: a population-based epidemiological survey. BMC Oral Health 2019;19:184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Navarro Azevedo de Azeredo F, Silva Guimaraes L, Azeredo AAL, et al. Global prevalence of dental caries in athletes with intellectual disabilities: an epidemiological systematic review and meta-analysis. Spec Care Dentist 2019;39:114–24. [DOI] [PubMed] [Google Scholar]
- [7].Pham TAV, Nguyen PA. Factors related to dental caries in 10-year-old Vietnamese schoolchildren. Int Dent J 2019;69:214–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Marcenes W, Kassebaum NJ, Bernabe E, et al. Global burden of oral conditions in 1990-2010: a systematic analysis. J Dent Res 2013;92:592–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Cheng ML, Xu MR, Xie YY, et al. Utilisation of oral health services and economic burden of oral diseases in China. Chin J Dent Res 2018;21:275–84. [DOI] [PubMed] [Google Scholar]
- [10].Liu J, Zhang SS, Zheng SG, et al. Oral health status and oral health care model in China. Chin J Dent Res 2016;19:207–15. [DOI] [PubMed] [Google Scholar]
- [11].Zhou X, Xu X, Li J, et al. Oral health in China: from vision to action. Int J Oral Sci 2018;10:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Sun HY, Jiang H, Du MQ, et al. The prevalence and associated factors of periodontal disease among 35 to 44-year-old Chinese adults in the 4th National Oral Health Survey. Chin J Dent Res 2018;21:241–7. [DOI] [PubMed] [Google Scholar]
- [13].World Health Organization. Oral Health Surveys: Basic Methods. World Health Organization; 2013. [Google Scholar]
- [14].Lima IFP, Nobrega DF, Cericato GO, et al. Prevalence of dental fluorosis in regions supplied with non-fluoridated water in the Brazilian territory: a systematic review and meta-analysis. Cien Saude Colet 2019;24:2909–22. [DOI] [PubMed] [Google Scholar]
- [15].Burt BA. How useful are cross-sectional data from surveys of dental caries? Community Dent Oral Epidemiol 1997;25:36–41. [DOI] [PubMed] [Google Scholar]
- [16].Bonecker M, Cleaton-Jones P. Trends in dental caries in Latin American and Caribbean 5-6- and 11-13-year-old children: a systematic review. Community Dent Oral Epidemiol 2003;31:152–7. [DOI] [PubMed] [Google Scholar]
- [17].Roncalli AG, Silva NN, Nascimento AC, et al. Relevant methodological issues from the SBBrasil 2010 Project for national health surveys. Cad Saude Publica 2012;28: suppl: s40–57. [DOI] [PubMed] [Google Scholar]
- [18].Cleaton-Jones P, Fatti P, Bonecker M. Dental caries trends in 5- to 6-year-old and 11- to 13-year-old children in three UNICEF designated regions--Sub Saharan Africa, Middle East and North Africa, Latin America and Caribbean: 1970–2004. Int Dent J 2006;56:294–300. [DOI] [PubMed] [Google Scholar]
- [19].Gimenez T, Bispo BA, Souza DP, et al. Does the decline in caries prevalence of Latin American and Caribbean children continue in the new century? Evidence from systematic review with meta-analysis. PLoS One 2016;11:e0164903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Ishii T, Yoshida S. Oral health surveys--basic methods--fundamental and practical problems of oral health surveys by WHO [in Japanese]. Shikai Tenbo 1978;51:762–72. [PubMed] [Google Scholar]
- [21].2003;Peterson PE, Baez RJ. World Health Organization. Oral health surveys: basic methods. 92:154864–9. [Google Scholar]
- [22].Prabu JJ, Saravanan S. Impact of dental caries and dental fluorosis on the quality of life on 12 year old children in Tamil Nadu, India. Chettinad Health City Med J 2013;2:74–9. [Google Scholar]
- [23].Sofowora C, Nasir W, Oginni A, et al. Dental caries in 12 year old suburban Nigerian school children. Afr Health Sci 2006;6:145–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Tasneem S, Sultan S, Gowhar O, et al. Prevalence of dental caries among 12 year old school children in Kashmir, India-a crosssectional study. Int J Contemp Med Res 2016;3:2156–9. [Google Scholar]
- [25].Nurelhuda NM, Trovik TA, Ali RW, et al. Oral health status of 12-year-old school children in Khartoum state, the Sudan; a school-based survey. BMC Oral Health 2009;9:15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Sousa Mda L, Rando-Meirelles MP, Torres LH, et al. Dental caries and treatment needs in adolescents from the state of Sao Paulo, Brazil. Rev Saude Publica 2013;47: suppl 3: 50–8. [DOI] [PubMed] [Google Scholar]
- [27].Freire Mdo C, Reis SC, Figueiredo N, et al. Individual and contextual determinants of dental caries in Brazilian 12-year-olds in 2010. Rev Saude Publica 2013;47: suppl 3: 40–9. [DOI] [PubMed] [Google Scholar]
- [28].Majumdar KK. Health impact of supplying safe drinking water containing fluoride below permissible level on flourosis patients in a fluoride-endemic rural area of West Bengal. Indian J Public Health 2011;55:303–8. [DOI] [PubMed] [Google Scholar]
- [29].Yan Z, Dongru C, Qinghui Z, et al. Epidemiology and Risk Indicators of Dental Fluorosis in 12-Year-Old Children in China. The 18th Annual Conference of Stomatological Preventive Medicine. Chinese Society of Stomatology; 2018. [Google Scholar]
- [30].Iheozor-Ejiofor Z, Worthington HV, Walsh T, et al. Water fluoridation for the prevention of dental caries. Cochrane Database Syst Rev 2015;CD010856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Tenuta LM, Cury JA. Fluoride: its role in dentistry. Braz Oral Res 2010;24: suppl 1: 9–17. [DOI] [PubMed] [Google Scholar]
- [32].Al-Rafee MA, AlShammery AR, AlRumikan AS, et al. A comparison of dental caries in urban and rural children of the Riyadh Region of Saudi Arabia. Front Public Health 2019;7:195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Joshi N, Rajesh R, Sunitha M. Prevalence of dental caries among school children in Kulasekharam village: a correlated prevalence survey. J Indian Soc Pedod Prev Dent 2005;3:138–40. [DOI] [PubMed] [Google Scholar]
- [34].Peres MA, Sheiham A, Liu P, et al. Sugar consumption and changes in dental caries from childhood to adolescence. J Dent Res 2016;95:388–94. [DOI] [PubMed] [Google Scholar]
- [35].Boustedt K, Dahlgren J, Twetman S, et al. Tooth brushing habits and prevalence of early childhood caries: a prospective cohort study. Eur Arch Paediatr Dent 2019;[Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- [36].ElSalhy M, Honkala S, Soderling E, et al. Relationship between daily habits, Streptococcus mutans, and caries among schoolboys. J Dent 2013;41:1000–6. [DOI] [PubMed] [Google Scholar]
- [37].Sun X, Bernabe E, Liu X, et al. Early life factors and dental caries in 5-year-old children in China. J Dent 2017;64:73–9. [DOI] [PubMed] [Google Scholar]
- [38].Guido JA, Martinez Mier EA, Soto A, et al. Caries prevalence and its association with brushing habits, water availability, and the intake of sugared beverages. Int J Paediatr Dent 2011;21:432–40. [DOI] [PubMed] [Google Scholar]
- [39].Nishide S, Yoshihara T, Hongou H, et al. Daily life habits associated with eveningness lead to a higher prevalence of dental caries in children. J Dent Sci 2019;14:302–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Pasqualotto AC, Nedel WL, Machado TS, et al. Risk factors and outcome for nosocomial breakthrough candidaemia. J Infection 2006;52:216–22. [DOI] [PubMed] [Google Scholar]
- [41].Markiewicz M, Dzierzak-Mietla M, Frankiewicz A, et al. Treating oral mucositis with a supersaturated calcium phosphate rinse: comparison with control in patients undergoing allogeneic hematopoietic stem cell transplantation. Support Care Cancer 2012;20:2223–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Riley P, McCabe MG, Glenny AM. Oral cryotherapy for preventing oral mucositis in patients receiving cancer treatment. JAMA Oncol 2016;2:1365–6. [DOI] [PubMed] [Google Scholar]
- [43].Scully C, Sonis S, Diz PD. Oral mucositis. Oral Dis 2006;12:229–41. [DOI] [PubMed] [Google Scholar]