

Abstract
Background:
Selenium (Se) is considered as an antioxidant trace element involved in key activities in human metabolism. Recent investigations indicate that Se plays a pivotal role in human health. Se supplementation considered as an intervention is both cost-effective and simple-to-use that may play an important role in the prevention of cardiometabolic risk factors (CRFs), inflammatory, and antioxidant markers.
Methods:
This paper is a protocol study on systematic review of probable effects of Se supplementation on CRFs, inflammatory, and antioxidant markers. The aim was to achieve three international databases available related to the current publications including, PubMed, ISI/WOS, and Scopus. We attempted to search for randomized clinical trials (RCT) and cross-over trials pertaining to human subjects without any restriction on language and time. In addition, there was no limitation on the age of participants. For RCTs were included all studies in different target groups comprising diabetic patients, patients with polycystic ovarian syndrome, obese subjects, or even healthy controls. To investigate the effect of Se, we included all studies which Se is used either as single therapy or as combination therapy. All studies associated with articles and meta-analyses would be evaluated to review their references.
Conclusions:
The current study contained numerous outcomes. The result of this study can be led to make reliable scientific evidence on the probable effects of Se supplementation on CRFs, inflammatory factors, and antioxidant factors. In addition to these findings, other technical documents developed for a systematic review can be used for future studies.
Keywords: Antioxidant markers, cardiometabolic risk factors, inflammatory markers, selenium, supplementation, systematic review
Introduction
Selenium (Se) is considered as an antioxidant trace element involved in key metabolic activities through selenoprotein enzyme as essential factors to protect against oxidative damage and regulate immune system process.[1,2,3] In addition to this mechanism, there are many studies that investigate Se may have other health benefits unrelated to its enzymatic functions.[1] Se is considered as an essential micronutrient in human metabolism. Recent evidence suggests that this element plays a pivotal role in human health.[3,4]
Se supplementation can be considered as a cost-effective and simple-to-use inorganic element due to its antioxidant and anti-inflammatory effects and based on the results of recent studies plays a key role in the prevention of cancer and cardiovascular disease and supporting patients after surgery.[3,4]
The results of studies suggest that Se may have therapeutic effects for patients who suffer from inflammatory disease or even infectious diseases such as human immunodeficiency virus/acquired immunodeficiency syndrome.[5] Se, alone or in conjunction with other micronutrients plays an effective role in improving treatment outcomes at a patient's risk of cancers.[6,7]
With an increase in reactive oxygen species and low endogenous antioxidative capacity, Se supplementation may result in a reduction of mortality in patients with severe sepsis.[2,6] Se supplementation improved the clinical outcome in patients with systemic inflammatory response syndrome who exposed to severe oxidative stress.[2,5]
Considering the association of cardiometabolic risk factors (CRFs) with Se, most of the studies reveal that diabetes patients have increased oxidative stress together with decreased Se concentrations.[3] In this regard, some evidence in type 2 diabetes patients suggested the association of Se supplementation with adverse effects on blood glucose homeostasis, even in cases plasma Se concentration is raised from deficient status to the optimal concentration of antioxidant activity.[3] In another investigation, there was a significant positive correlation between dietary Se intake and diabetes, that emphasize its findings are yet inconclusive.[8,9]
Both metabolic syndrome (MetS) and CRFs have emerged as a and the major public health problem that is approaching epidemic globally.[10,11,12] The findings of studies showed that the plasma Se level correlated positively with MetS, waist circumference, plasma glucose, and triglyceride (TG) concentration. Thus, more studies are needed to investigate the role of Se supplementation yet.[11,13,14,15]
Various strategies have been proposed to prevent CRFs and MetS. With respect to the need for prevention and control program, one study suggested that the protective role of Se supplementation must be investigated in more details.
In spite of the priority of the problem, there is an evident gap in the related literature review on these topics or proposed controversial topics.[8,9,16] Considering the importance of exploring different aspects of phenomenon, the present study aimed to provide the approaches and the details considered in the development of the protocol for a comprehensive systematic review on the assessment of Se supplementation on CRFs, inflammatory, and antioxidant markers.
Methods
The present study aimed to follow the PRISMA-P guidelines.[17,18]
Objectives
This study is considered as a systematic review addressed probable effects of Se supplementation on CRFs, inflammatory, and antioxidant markers. The study is based on the current-related publications in the international databases available [Figure 1].
Figure 1.
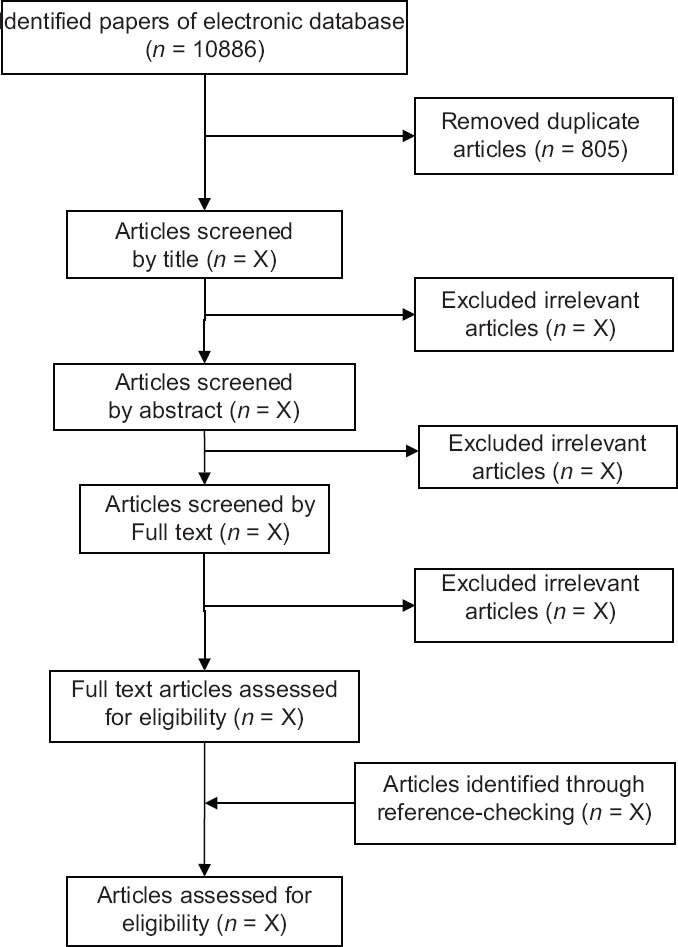
Papers search and review flowchart for selection of primary study
Intervention
To investigate the effect of Se, we included all studies which Se is applied as supplement (either as single therapy or as combination therapy with other drugs or micronutrients).
Outcomes
Effect of Se supplementation will be assessed through evaluation indices:
Metabolic risk factors including lipid profile, (total cholesterol, TG, high-density lipoprotein [HDL], low-density lipoprotein [LDL], very LDL), MetS, hypertension (systolic/diastolic blood pressure), glycemic indices (fasting plasma glucose, hemoglobin A1c, homeostatic model assessment-insulin resistance (IR), quantitative insulin sensitivity check index, fasting blood sugar), and anthropometric measures (weight, waist circumference, body mass index, body fat, and waist to hip)
Antioxidant markers, including oxidative stress index, antioxidant potency composite indices, total antioxidant capacity, antioxidant enzymes (superoxide dismutases, glutathione peroxidases, catalase), total antioxidant plasma
Inflammatory markers such as C-reactive protein and interleukins, tumor necrosis factor-α.
Study subject
We attempted to search for randomized clinical trials (RCT) and crossover trails pertaining to human subjects with no limitation as regards age groups. In this regard, population of the study contained more diabetic patients, patients with polycystic ovarian syndrome (PCOS) and obese subjects than healthy controls.
Eligibility criteria
We included all RCT and cross-over trails which control group received the placebo, irrespective of date and language. For RCTs, where there was no interaction with Se consumption and access to the study objectives, all studies in different target groups comprising diabetic patients, PCOS subjects, obese subjects, or even healthy individuals were included. To investigate of the role of Se, we included all studies which Se is used either as single therapy or as combination therapy. All studies would be included which Se prescribed for therapeutic procedures (such as anti-angiogenic and anti-metastatic agents for cancer treatment).
All studies associated with articles and meta-analyses would be evaluated to review their references.
If there were more than one paper that were extracted by one specific study, the most complete reported data were only considered by one paper. We also excluded article with a duplicate citation and those, based on data refinement results are non-relevant.
There was no time limit on the study, the duration of Se supplementation, language of documents, or time of publication.
Search strategy
To identify the probable effects of Se supplementation on CRFs, inflammatory, and antioxidant factors, we searched through systematic search strategy three international databases including, PubMed, ISI/WOS, and Scopus for published scientific papers and peer review studies. The search terms were developed concentrating on MetS, cardiometabolic syndrome, IR Syndrome, oxidative stress and lipid profile, inflammatory factors, antioxidant factors, and Se supplementation. We searched for RCT and crossover trials, human subject, and without any restriction on language and time. Furthermore, there was no limitation as regards age groups. Searches conducted on January 1, 2016 [Table 1].
Table 1.
Search strategy
| PubMed | |
|---|---|
| ((“Oxidative Stress”[Mesh] OR “lipid profile”[Mesh] OR”Glucose Homeostasis”[Mesh] OR “Metabolic Syndrome X”[Mesh] OR “cardiometabolic syndrome” [Title/Abstract] OR “insulin Resistance Syndrome” [Title/Abstract]) OR “Metabolic X Syndrome” [Title/Abstract] OR “Dysmetabolic Syndrome” [Title/Abstract] OR “Cardiovascular Syndromes, Metabolic” [Title/Abstract] OR “Diabetes Mellitus, Type 2”[Mesh] OR “obesity” [Mesh] OR “ abdominal obesity” [Mesh] OR “inflamantion” [Mesh] OR “inflamantory factors” [ Title/Abstract] OR “antioxidant” [Mesh]) AND (“Se”[Mesh] OR “se” [Title/Abstract])) | |
| Scopus | |
| (((TITLE-ABS-KEY (Se) OR TITLE-ABS-KEY (“Se”)) AND ((TITLE-ABS-KEY (“Metabolic Syndrome”) OR TITLE-ABS-KEY (cardiometabolic) OR TITLE-ABS-KEY (“ Cardiovascular Syndromes” OR TITLE-ABS-KEY (“Diabetes Mellitus”) OR TITLE-ABS-KEY (“Type 2 Diabetes”) OR TITLE-ABS-KEY (cardiovascular) OR TITLE-ABS-KEY (“Syndrome X”) OR TITLE-ABS-KEY (“Insulin Resistance “) OR (TITLE-ABS-KEY (“glucose homeostasis”) OR TITLE-ABS-KEY (“Homeostasis of Glucose”) OR TITLE-ABS-KEY (“Lipid profile “) OR TITLE-ABS-KEY (“lipid panel”) OR TITLE-ABS-KEY (“Lipid_profile”) OR TITLE-ABS-KEY (“Oxidative Stress”) OR TITLE-ABS-KEY (“inflamantion”) OR TITLE-ABS-KEY (“inflamantory factors”) OR TITLE-ABS-KEY (“antioxidant))) | |
| ISI/WOS | |
| TOPIC: (Se) OR TOPIC: (se) (TOPIC: (“Metabolic Syndrome”) OR TOPIC: (“Mets”) OR TOPIC:(“Dysmetabolic Syndrome”) OR TOPIC: (“Cardiovascular Syndromes”) OR TOPIC: (“Insulin Resistance Syndrome”) OR TOPIC: (“Cardiometabolic”) OR TOPIC: (“Diabetes Mellitus”) OR TOPIC: (“Type 2 Diabetes”) OR TOPIC: (“Syndrome X”) OR TOPIC: (“glucose homeostasis”) OR TOPIC: (“Homeostasis of Glucose”) OR TOPIC: (“Lipid profile”) OR TOPIC: (“lipid panel”) OR TOPIC: (“Lipid-profile”) OR TOPIC: (“Oxidative Stress”) OR TOPIC: (“inflamantion”) OR TOPIC: (“inflamtory factors “) OR TOPIC: (“antioxidant”)) Timespan=All years AND Indexes=SCI-EXPANDED, SSCI, CPCI-S, CPCI-SSH Timespan=All years | |
ISI/WOS=Institute for scientific information/web of science
Other resources
Other sources will be searched to identify related grey literature and reference lists of the relevant primary studies as well as the related key journals for additional publication.
Data management
The bibliographic information of searched studies would be saved in Endnote software for further reference management. Through three steps of data refinement, including titles, abstracts and full texts review, all of the processes followed by two independent experts. Possible disagreements can be resolved by discussion or consensus.
Quality assessment and data extraction
The quality assessment and data extraction of eligible remained papers would be conducted independently by two independent research experts and probable discrepancy between them would be resolved through referencing the third expert opinion. We followed the CONSORT 2010 Statement including a 25-item checklist and study design, sampling strategy, measurement quality analyzed, and then interpreted for quality assessment.[19] We used Cohen's kappa statistic to assess agreement between the results of the quality assessment of two experts.
Data were collected according to a standard protocol and citation was extracted based on studied groups including type of study, study subjects, publication year, sample size, dose of supplementation, chemical source of Se, intervention group, control group, mean age of participants, outcome, intervention duration, follow-up duration, measurement interval, result, effect size.
Statistical analysis and data synthesis
The effect of Se supplementation on CRFs, inflammatory, and antioxidant factors can be assessed as mean difference based on changes at the level of outcomes. This value is used to calculate the difference in mean value from baseline values by subtracting the final mean from the baseline value for placebo interventions and treatments. The following equation can be used to calculate the standard deviation (SD):
([n−1] × [SD12/SD22]/[2n−1])
Data were expressed as the median and convert range to mean, and SD was applied by Hozo's formula.[20] We calculated the value of Cohen'sd and the effect size correlation, rYl, using the means and SDs of two groups (treatment and control):
Cohen's d = M1–M2/spooled
Spooled = √([s12+s22]/2)
rYl = d/√(d2+4)
Effect size before and after experimental studies can be calculated by the following equation:
Effect size E = E/S(Δ)* S(Δ)
E/S(Δ) = √AB/N
For studies that express the results in the form of a mean ± SEM, the following formula is used to convert those to mean ± SD (SD = SEM* sqrt [N]).
If the Q-statistic for heterogeneity was significant at the level of 0.1, random-effect model would be used.[21] In other cases, the fixed-effect model can be used.[22] The degree of heterogeneity quantify with I2 statistics represented an estimate of the total variation across studies that can be attributed to heterogeneity.[23] Thus, I2 values of 25%, 50%, and 75% were considered to correspond to low, medium, and high levels of heterogeneity, respectively. Possible sources of heterogeneity were explored by sensitivity analysis.
The statistical analysis was carried out using STATA software, version 10 (Stata Statistical Software: Release 10. College Station, TX: StataCorp. LP).[24] A P ≤ 0.05 is considered to be statistically significant.
Meta-regression
The impact of influencing factors was analyzed using a random-effect meta-regression. According to the result of heterogeneity among the studies, at the next step corresponding models would be followed.[25,26] Forest plot is also used to present schematic representation of the result of the meta-analysis. Publication bias was estimated by Egger's test.
Publication bias
Publication bias was estimated by Egger's test.
Ethical considerations
The present study was approved by the Ethical Committee of Alborz University of Medical Sciences. All presented studies in our reviews will be cited in all the future reports and relevant publications. Therefore, whenever we require more information about a certain study, we will contact the corresponding author to obtain necessary information.
Discussion/Deliverables
The current study contained numerous outcomes. The result of this study can be led to make reliable scientific evidence on the probable effects of Se supplementation on CRFs, inflammatory, and antioxidant markers. In addition to the findings, other technical documents developed for a systematic review can be used for future studies. The results of this study can be used to answer the research questions and, in addition, to identify the gaps from required evidences that is essential for health policymakers. These results have been considered as the most valuable source to determine the future plans for complementary research.
There are large controversies about the effects and correlation of Se on CRFs and component of MetS, which may be attributed to differences in designing and reporting the studies or even lack of a special focus on the association between Se and MetS, and complex nature of MetS.
Some supported evidence emphasized that the plasma Se level correlated positively with MetS, waist circumference, plasma glucose, and TG concentration.[14,15]
However, there were many confirmed findings demonstrated that MetS has no correlation with serum Se. These findings have also been generalized in factors, including hypertension, highly elevated fasting serum TG levels, and lower levels of serum HDL cholesterol that are associated with components of MetS.[15]
Undoubtedly, decisions on the priority, feasibility, granting, conducting, and evaluation of health programs require the accurate information to engage the policymakers and other stakeholders.[16] In addition to data quality importance and data availability, the strategies and the techniques of data presentation in papers must be paid more attention to details.[27]
Considering the previous attempts, the present study has several achievements. This study presents scientific evidence to depict association between Se supplementation on CRFs, inflammatory disorders, and antioxidant markers.
The related data sources available are searched using the most comprehensive database and more efficient systematic approaches of searching. As the main limitation, the validity and applicability of our results in a systematic review depend on the precision and quality of the primary studies that are included. As another considerable point, probably heterogeneity of searched results limits the generalization of our findings. We must select the best approaches for addressing differences in study design and population that may play as a main source of controversies in the analysis. In addition to the complex and multifactorial nature of MetS, different definitions can be used for this disorder.
Conclusions
According to our knowledge, this is the first comprehensive systematic review of association between Se supplementation on CRFs, inflammatory, and antioxidant markers. Results can be useful for better health policy and planning with more studies in this field. These also can be used for the future of complementary analysis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We would like to thank all our research team for their participation in research and support of the project.
References
- 1.Ryan-Harshman M, Aldoori W. The relevance of se to immunity, cancer, and infectious/inflammatory diseases. Can J Diet Pract Res. 2005;66:98. doi: 10.3148/66.2.2005.98. [DOI] [PubMed] [Google Scholar]
- 2.Razavi M, Jamilian M, Kashan ZF, Heidar Z, Mohseni M, Ghandi Y, et al. Selenium supplementation and the effects on reproductive outcomes, biomarkers of inflammation, and oxidative stress in women with polycystic ovary syndrome. Horm Metab Res. 2016;48:185–90. doi: 10.1055/s-0035-1559604. [DOI] [PubMed] [Google Scholar]
- 3.Faghihi T, Radfar M, Barmal M, Amini P, Qorbani M, Abdollahi M, et al. A randomized, placebo-controlled trial of se supplementation in patients with type 2 diabetes: Effects on glucose homeostasis, oxidative stress, and lipid profile. Am J Ther. 2014;21:491–5. doi: 10.1097/MJT.0b013e318269175f. [DOI] [PubMed] [Google Scholar]
- 4.Spallholz JE, Boylan LM, Larsen HS. Advances in understanding selenium's role in the immune system. Ann N Y Acad Sci. 1990;587:123–39. doi: 10.1111/j.1749-6632.1990.tb00140.x. [DOI] [PubMed] [Google Scholar]
- 5.Duntas LH. Selenium and inflammation: Underlying anti-inflammatory mechanisms. Horm Metab Res. 2009;41:443–7. doi: 10.1055/s-0029-1220724. [DOI] [PubMed] [Google Scholar]
- 6.Bjelakovic G, Nikolova D, Gluud C. Antioxidant supplements and mortality. Curr Opin Clin Nutr Metab Care. 2014;17:40–4. doi: 10.1097/MCO.0000000000000009. [DOI] [PubMed] [Google Scholar]
- 7.Bjelakovic G, Nikolova D, Gluud LL, Simonetti RG, Gluud C. Antioxidant supplements for prevention of mortality in healthy participants and patients with various diseases. Sao Paulo Med J. 2015;133:164–5. doi: 10.1590/1516-3180.20151332T1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wei J, Zeng C, Gong QY, Yang HB, Li XX, Lei GH, et al. The association between dietary selenium intake and diabetes: A cross-sectional study among middle-aged and older adults. Nutr J. 2015;14:18. doi: 10.1186/s12937-015-0007-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lu CW, Chang HH, Yang KC, Kuo CS, Lee LT, Huang KC. High serum Se levels are associated with increased risk for diabetes mellitus independent of central obesity and insulin resistance. BMJ Open Diabetes Res Care. 2016;4:1–7. doi: 10.1136/bmjdrc-2016-000253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cheng TO. Metabolic syndrome in China. Circulation. 2004;109:e180. doi: 10.1161/01.CIR.0000124882.83145.E6. [DOI] [PubMed] [Google Scholar]
- 11.McCullough AJ. Epidemiology of the metabolic syndrome in the USA. J Dig Dis. 2011;12:333–40. doi: 10.1111/j.1751-2980.2010.00469.x. [DOI] [PubMed] [Google Scholar]
- 12.Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2005;365:1415–28. doi: 10.1016/S0140-6736(05)66378-7. [DOI] [PubMed] [Google Scholar]
- 13.Reaven G. Metabolic syndrome: Pathophysiology and implications for management of cardiovascular disease. Circulation. 2002;106:286–8. doi: 10.1161/01.cir.0000019884.36724.d9. [DOI] [PubMed] [Google Scholar]
- 14.Vidović B, Dorđević B, Milovanović S, Škrivanj S, Pavlović Z, Stefanović A, et al. Selenium, zinc, and copper plasma levels in patients with schizophrenia: Relationship with metabolic risk factors. Biol Trace Elem Res. 2013;156:22–8. doi: 10.1007/s12011-013-9842-1. [DOI] [PubMed] [Google Scholar]
- 15.Obeid O, Elfakhani M, Hlais S, Iskandar M, Batal M, Mouneimne Y, et al. Plasma copper, zinc, and selenium levels and correlates with metabolic syndrome components of lebanese adults. Biol Trace Elem Res. 2008;123:58–65. doi: 10.1007/s12011-008-8112-0. [DOI] [PubMed] [Google Scholar]
- 16.Heinrich CJ. Evidence-based policy and performance management: Challenges and prospects in two parallel movements. Am Rev Publ Adm. 2007;37:255–77. [Google Scholar]
- 17.Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Nikuei P, Davoodian N, Tahamtan I, Keshtkar AA. Predictive value of miR-210 as a novel biomarker for pre-eclampsia: A systematic review protocol. BMJ Open. 2016;6:e011920. doi: 10.1136/bmjopen-2016-011920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Schulz KF, Altman DG, Moher D, Consort Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials (Chinese version) Zhong Xi Yi Jie He Xue Bao. 2010;8:604–12. doi: 10.3736/jcim20100702. [DOI] [PubMed] [Google Scholar]
- 20.Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:13. doi: 10.1186/1471-2288-5-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- 22.Whitehead A, Whitehead J. A general parametric approach to the meta-analysis of randomized clinical trials. Stat Med. 1991;10:1665–77. doi: 10.1002/sim.4780101105. [DOI] [PubMed] [Google Scholar]
- 23.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.StataCorp L. Stata data analysis and statistical software. Spec Ed Release. 2007;10:733. [Google Scholar]
- 25.Gardiner JC, Luo Z, Roman LA. Fixed effects, random effects and GEE: What are the differences? Stat Med. 2009;28:221–39. doi: 10.1002/sim.3478. [DOI] [PubMed] [Google Scholar]
- 26.Stroup DF, Berlin JA, Morton SC, Olkin I, Williamson GD, Rennie D, et al. Meta-analysis of observational studies in epidemiology: A proposal for reporting.Meta-analysis of observational studies in epidemiology (MOOSE) group. JAMA. 2000;283:2008–12. doi: 10.1001/jama.283.15.2008. [DOI] [PubMed] [Google Scholar]
- 27.Djalalinia S, Kelishadi R, Qorbani M, Peykari N, Kasaeian A, Saeedi Moghaddam S, et al. Suggestions for better data presentation in papers: An experience from a comprehensive study on national and sub-national trends of overweight and obesity. Arch Iran Med. 2014;17:830–6. [PubMed] [Google Scholar]