

Abstract
There is mixed evidence for the relationship between increased levels of the drive for muscularity (DFM) and disordered eating behavior in males, therefore this study analysed the relationship between DFM and disordered eating behavior, giving particular relevance to the patterns of cognitive appraisal. A convenience sample was recruited from fitness centres and sport clubs with 308 participants, all males. Losing muscular mass represented a negative experience for participants, promoting a higher perception of threat appraisal. In addition, losing muscular mass was related to more muscularity-oriented behaviors and disordered eating behavior. Cognitive appraisal mediates the relation between DFM and disordered eating behavior. The results highlight the role of cognitive appraisal in DFM and disordered eating behavior in males in sport contexts.
Key words: mediation, sport, losing muscular mass
Introduction
Body image concerns and disordered eating behaviors are more extensively studied in women compared to men. However, existing evidence suggests that a substantial proportion of males exhibit disordered eating behaviors, which may manifest as muscularity-oriented symptoms driven by the male-specific sociocultural body ideal (Lavender et al., 2017).
In fact, previous studies with male samples have mainly focussed on the dimensions of thinness and obesity and have not focussed on the drive for muscularity (DFM) as an important dimension related to body image and disordered eating behaviors. However, since McCreary and Sasse (2000) identified that males also have body image concerns similar to female concerns, an increasing body of research has emerged on DFM (Edwards et a., 2014). The DFM concept was proposed as a parallel to the established drive for thinness in women, representing the desire of men to increase muscularity and to develop a muscular physique body. DFM implies an aroused state of tension related to the individual’s perceptions that they are not sufficiently muscular, resulting in muscularity-increasing behaviors (Edwards et al., 2014).
Three systematic reviews of the DFM research area have been published (Edwards et al., 2014; McCreary, 2007; Morrison et al., 2006). According to the last review (Edwards et al., 2014), athletes had higher DFM than non-athletes did (Morrison et al., 2003; Zelli et al., 2010). Furthermore, body surveillance (Hallsworth et al., 2005; Martins et al., 2007), depression (Bergeron and Tylka, 2007; Hallsworth et al., 2005), bulimia (Hallsworth et al., 2005), appearance anxiety, social physique anxiety and body shame (Ginis et al., 2005; Martins et al.,2007) were found to be positively related with DFM. There is also a consistent relationship between DFM and selfreported weightlifting, dieting to gain weight/muscularity, and nutritional supplementation (Chittester and Hausenblas, 2009; Litt and Dodge, 2008; McPherson et al., 2010; Morrison et al., 2003). More recently, in an overview regarding traditional and muscularity-oriented disordered eating, Lavender and colleagues (2017) concluded that disordered eating focused on muscularity was more prevalent in males than concerns around thinness, underscoring the centrality of muscularity-oriented manifestations of body dissatisfaction and associations with disordered eating symptoms.
However, the meta-analysis by Tod and Edwards (2015) found small to moderate relationships between DFM and exercise behavior, disordered eating, supplement consumption, and exercise dependence. These modest results indicate the value of adopting theoretical perspectives that allow for the examination of the DFM's role in predicting exercise and dietary behavior. The authors claimed that even if individuals had high drives to be muscular, other factors would influence their decisions to engage in specific physical activity and dietary manipulations. Considering this recommendation, we believe that the Lazarus transactional model (1991) may help improve the prediction of disordered eating behaviors in males.
As far as we know, no previous study has evaluated the relationship between DFM, the experience of muscular mass changing in an undesirable way, and disordered eating behaviors in a sample of exercising males and competitive athletes.
Therefore, regarding the experience of muscular mass changing in an undesirable way, we used the conceptual framework of the Lazarus’s transactional model (1991). In this framework, stress is conceptualized as a complex subjective phenomenon (Lazarus et al., 1985). Given that, we conceptualized the changes of muscular mass (gaining or losing muscular mass) as a source of potential stress for males who exercise on a regular basis. This study analysed the experience of an undesired change in muscular mass in athletes and men exercising on a regular basis by adopting a critical incident methodology (Carver et al., 1989; Folkman and Lazarus, 1988). Specifically, participants were confronted with the possibility of having a significant change in their muscular mass and then we analysed the adaptation process to this stressor according to interactive (Gomes, 2014) and transactional perspectives of stress (Lazarus, 1991). After checking the relevance of exercise/sport activity, we evaluated whether changing muscular mass would be perceived as a more positive (challenging) or negative (threatening) experience. The challenge perception tends to occur if the stressor is perceived as difficult to attain yet offering an anticipated gain; the threat perception tends to occur if the stressor is perceived as difficult to attain and posing anticipated harm or potential loss (Lazarus, 1999). In addition, we tested the possibility of cognitive appraisal of undesirable changes of muscular mass mediating the relation between DFM and disordered eating behavior. To the best of our knowledge, this is the first study that evaluates the specific relations between these variables and tests the possibility of cognitive appraisal mediation between DFM and disordered eating behavior. Three goals were formulated:
Analysing the association between the experience of muscular mass changing, DFM and disordered eating behavior.
Analysing the relation between cognitive appraisal of muscular mass changing, DFM and disordered eating behavior.
Analysing the mediating role of cognitive appraisal of muscular mass changing and disordered eating behavior.
Methods
Participants
A convenience sample was recruited from fitness centres (n = 138; 44.8%) and sport clubs (n = 170; 55.2%), with a total of 308 participants, all males. The majority of participants from fitness centres performed weight training as their main activity (n = 110; 79.7%), and 26 (18.8%) trained CrossFit. Participants from sport clubs had a greater diversity of activities, mostly related to soccer (n = 85; 50%), other team sports (e.g., basketball, handball, soccer, n = 30; 17.6%), and individual sports (e.g., swimming, athletics, n= 55; 32.4%). Participants from fitness centres had a mean age of 25.49 years (SD = 6.28; minimum = 18; maximum = 45) and practised their activity from one to four sessions per week (M = 2.20; SD = 0.91). Participants from sport clubs had a mean age of 26.18 years (SD = 6.61; minimum = 18; maximum = 47) and practised their activity from one to four sessions per week (M = 2.58; SD = 0.89).
Measures
Drive for Muscularity Scale (DMS; McCreary and Sasse, 2000). This instrument evaluates muscularity-oriented attitudes and behaviors, including two dimensions: (a) muscularity-oriented body image (seven items; α = 0.91 for this study), and (b) muscularity-oriented behaviors (seven items; α = 0.85 for this study). Each item is scored on a 6-point scale, ranging from always to never. Confirmatory factor analysis showed an acceptable fit for the two-factor model of drive for muscularity, χ2(73 g.l) = 182,55, p < .001; RMSEA = .070; CFI = .96; TLI = .94.
Primary and Secondary Cognitive Appraisal Scale (PSCAS; Gomes and Teixeira, 2016). For the purpose of this study, dimensions of primary cognitive appraisal were used. More specifically, instructions and items of the PSCAS were adapted for this study in order to evaluate three dimensions: (a) sport importance (three items; α = 0.84 for this study); (b) threat perception (three items; α = 0.90 for this study); and (c) challenge perception (three items; α = 0.84 for this study). According to the interactive and transactional perspectives of stress (Gomes, 2014; Lazarus, 1999) the PSCAS was used to evaluate the personal meaning of exercise and sports. Then, participants were confronted with the possibility of their muscular mass changing significantly without intention. Each item was measured on a 7-point Likert scale (0 = Means nothing to me; 6 = Means a lot to me). High scores on each scale indicate greater importance, threat, and challenge perceptions. We also included a final question for participants, asking to specify whether this event could be one of losing muscular mass, gaining muscular mass, or both. Confirmatory factor analysis (Bentler, 2007) showed an acceptable fit for the three-factor model of primary cognitive, χ2(24 g.l) = 62.151, p < .001; RMSEA = .072; CFI = .97; TLI = .96.
Eating Disorders Cognitions and Behaviors (ED.15; Tatham et al., 2015). This instrument includes two dimensions related to weight and shape concerns (six items; α = .87, for this study) and eating concerns (four items; α = .75, for this study). A global score was also calculated from the average of the two subscales scores (α = .86, for this study). The ED.15 also includes five items assessing specific behaviors related to eating disorders (objective binges, vomiting episodes, laxative use days, restriction days, and exercise days). The confirmatory factor found acceptable fit indices, χ2(32 g.l.) = 79.115, p < .001; RMSEA = .069; CFI = .96; TLI = .95.
Procedures
This study was approved by the Ethics Committee of the University (ref. SECSH 043/2016). Data collection involved: (a) permission from directors of sport clubs and fitness centres; and (b) contact with the participants to explain the goals of the study, the confidentiality, and the voluntary nature of participation.
Statistical Analysis
All analyses were conducted using SPSS and AMOS (v. 24).
First, we tested the relation between changes of muscular mass (independent variable) and cognitive appraisal, DFM and disordered eating behavior (dependent variables). To this end, we defined three groups of participants regarding changes of muscular mass according to how they responded to the PSCAS instrument (i.e., their thinking on the possibility of losing muscular mass, gaining muscular mass, and both possibilities). Then, we carried out multivariate analysis (one-way MANOVA) with Schefée post hoc tests.
Second, we tested the relation between cognitive appraisal (independent variable), DFM and disordered eating behavior (dependent variables). For that, we applied a median to define groups of participants with higher and lower threat and challenge perceptions. Then, we carried out multivariate analysis (two-way MANOVA).
Third, we tested the mediating role of cognitive appraisal in the relation between DFM and disordered eating behavior by using structural equation modelling (SEM).
Finally, all these analyses were conducted by first checking the data for univariate and multivariate outliers (Tabachnic and Fidell, 2013).
Results
Changes of Muscular Mass and Cognitive Appraisal
The interaction between changes of muscular mass (n = 46 losing muscle; n = 144 gaining weight; n = 101 both possibilities) and cognitive appraisal was tested. Multivariate tests revealed significant differences between groups, Wilks’ λ = .84, F(4, 574) = 12.66, p < .001, η2 =.08. Tests of between-subjects effects revealed significant differences between groups in terms of threat, F(2, 288) = 15.84, p < .001, η2 =.10, and challenge perceptions, F(2, 288) = 11.03, p < .001, η2 =.07. Schefée post hoc tests revealed that losing muscular mass was a more threatening experience than gaining muscular mass and that the possibility of gaining and losing muscular mass represented a more threatening experience than only gaining muscular mass. In addition, Schefée post hoc tests revealed that losing muscular mass was a less challenging experience than gaining muscular mass and the possibility of both gaining and losing muscular mass.
Changes of Muscular Mass and the Drive for Muscularity
Although multivariate tests did not reveal significant differences between groups, Wilks’ λ = .97, F(4, 592) = 2.16, p = .07, η2 =.01, tests of between-subjects effects revealed significant differences between groups in terms of muscularity-oriented behaviors, F(2, 297) = 4.02, p = .02, η2 =.03. Schefée post-hoc tests revealed that losing muscular mass was related to more muscularity-oriented behaviors than gaining muscular mass.
Changes of Muscular Mass and Disordered Eating Behavior
Although multivariate tests did not reveal significant differences between groups, Wilks’ λ = .98, F(4, 568) = 1.57, p < .18, η2 =.01, tests of between-subjects effects revealed significant differences between groups in terms of eating concerns, F(2, 285) = 3.08, p = .05, η2 =.02. Schefée post-hoc tests revealed that losing muscular mass was related to a greater tendency for eating concerns than gaining muscular mass (results of post hoc tests were significant, with a p-value of .078) and the possibility of both gaining and losing muscular mass (post hoc test results were significant with a p-value of .064).
Cognitive Appraisal and the Drive for Muscularity
The interaction between groups of threat (n = 132 low threat; n = 176 higher threat) and groups of challenge (n = 166 low threat; n = 142 higher threat) was tested. Multivariate tests revealed significant differences between groups, Wilks’ λ = .97, F(2, 303) = 4.17, p = .02, η2 =.03. Tests of between-subjects effects revealed significant differences between groups in terms of challenge perception. In fact, participants who perceived changes of muscular mass as more challenging reported a higher tendency for muscularity-oriented body image, F(1, 304) = 18.56, p < .001, η2 =.06, and muscularity-oriented behaviors, F(1, 304) = 8.25, p = .004, η2 =.03.
Cognitive Appraisal and Disordered Eating Behavior
Although multivariate tests did not reveal significant differences between groups, Wilks’ λ = .99, F(2, 291) = .83, p < .44, η2 =.01, tests of between-subjects effects revealed significant differences between groups in terms of challenge perception. In fact, participants who perceived changes of muscular mass as more challenging reported a higher tendency for weight and shape concerns, F(1, 292) = 14.37, p < .001, η2 =.05, and eating concerns F(1, 292) = 7.03, p = .01, η2 =.02.
The same relation was tested for the five specific behaviors related to disordered eating behaviors included in the ED.15. The interaction between groups of threat (n = 126 low threat; n = 170 higher threat) and groups of challenge (n = 160 low threat; n = 136 higher threat) was tested. Although multivariate tests did not reveal significant differences between groups, Wilks’ λ = .98, F(3, 290) = 1.81, p < .15, η2 =.02, tests of between-subjects effects revealed significant differences between groups in terms of the number of exercise days. In fact, participants who perceived changes of muscular mass as more challenging and less threatening reported a higher tendency to perform intense exercise than participants who perceived changes of muscular mass as less challenging and more threatening F(1, 292) = 5.13, p = .02, η2 =.02.
Mediating Role of Cognitive Appraisal
The partial mediation model, which included all direct and indirect effects, presented the best overall fit (χ2(387 g.l.) = 780.76, p < 0.001; RMSEA = 0.61; CFI = 0.92; TLI = 0.91) when compared with the direct effects model (χ2(241 g.l.) = 544.82, p < 0.001; RMSEA = 0.069; CFI = 0.91, TLI = 0.90) and the full mediation model (χ2(389 g.l.) = 582.99, p < 0.001; RMSEA = 0.066; CFI = 0.90; TLI = 0.89). Moreover, we found that the direct effects of muscularity-oriented body image (X1) and muscularity-oriented behaviors (X2) on disordered eating behavior (Y) were statistically significant (Effect X1-Y = 0.278, p = .007; Effect X2-Y = 0.295, p = .009). However, when we introduced cognitive appraisal variables, the indirect effects of muscularity-oriented body image and muscularity-oriented behaviors on disordered eating behavior did not appear to be significant (Effect X1-Y = 0.052, p = .074; Effect X2-Y = 0.002, p = .913), although the total effect of muscularity-oriented body image and muscularity-oriented behaviors on disordered eating behavior, which consists of both the direct and indirect effects, was statistically significant (Effect X1-Y = 0.33, p = .003; Effect X2-Y = 0.298, p = .006). In addition, the partial mediation model contributed with more explained variance to disordered eating behavior (39%) when compared to the direct model (33%) and the full mediation model (15%). Higher muscularity-oriented body image and higher muscularity-oriented behaviors were related to disordered eating behavior. Perception of a possible situation of change in muscular mass, either as a threat or a challenge, was related to disordered eating behavior.
Figure 1.
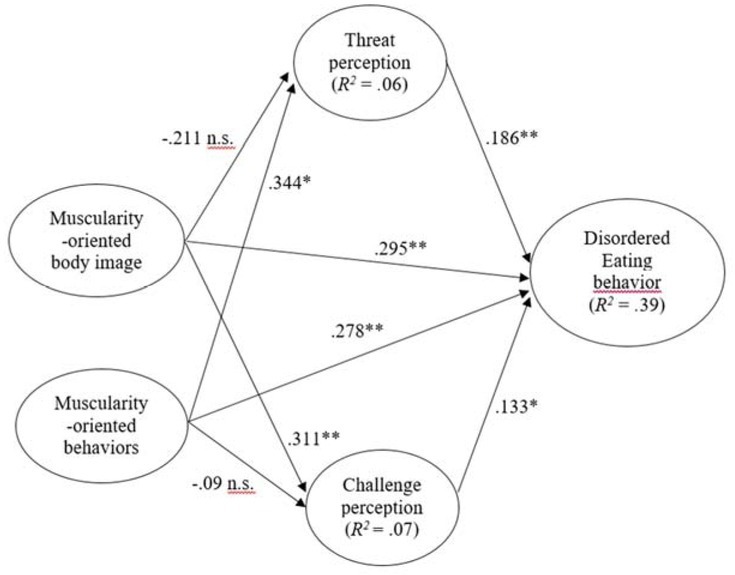
The partial mediation model: Adjusted model with standardized regression coefficients. *p < .05; ** p < .01; *** p < .001 Note: confidence intervals of parameter estimates of the structural paths’ coefficients were as follows: - Muscularity-oriented body image to threat perception [-0.437; 0.028]; - Muscularity-oriented behaviours to challenge perception [-0.337; 0.146]; - Muscularity-oriented body image to eating disordered behavior – indirect effect [0.073; 0.479]; - Muscularity-oriented behaviors to eating disordered behavior – indirect effect [0.066; 0.513]; - Threat perception to disordered eating behavior [0.043; 0.306]; - Challenge perception to disordered eating behavior [0; 0.265]. Confidence intervals of squared multiple correlation coefficients were as follows: - Threat perception [0.059; 0.284];
Analysis of Multigroup Invariance
Finally, we tested the invariance of cognitive appraisal as a mediating variable between muscularity-oriented body image and higher muscularity-oriented behaviors, as well as disordered eating behavior, according to the type of physical activity undertaken by participants (fitness centres vs. sport clubs). An analysis of multigroup invariance was conducted to examine whether the partial mediation model showed equivalence for these variables (Byrne, 2006).
Considering the unconstrained model to be correct, the measurement model presented a significantly worse adjustment to groups (χ2 (131) = 1333.899, p ≤ .001) compared to the unconstrained model (χ2 (156) = 1284.466, p ≤ .001), since p Δχ2 < .05 (Δχ2 (25) = 49.433, p = .003). These results demonstrate the variance of the measurement model across the two groups of variables, so the invariance of the structural model (Δχ2 (8) = 6.176, p = .062) cannot be imputed to the specificity of the variable in comparison.
Additionally, we tested for the moderator effect of the type of physical activity, using PROCESS 3.0 (Hayes, 2018). Considering the mediation effect of cognitive appraisal variables, the type of physical activity did not present a significant interaction effect in the relationship between muscularity-oriented body image and disordered eating behavior (F = 2.064, p = .152), and in the relationship between muscularity-oriented behaviors and disordered eating behavior (F = 0.1934, p = .660).
Discussion
There is mixed evidence for the relationship between increased levels of DFM and disordered eating behaviour (Edwards et al., 2014). A recent meta-analysis (Tod and Edwards, 2015) has shown that a small to moderate relationship exists between DFM and disordered eating behaviour, suggesting that the relationship between these variables may not be simple or straightforward. The same meta-analysis argued for the evaluation of this relationship within a broader theoretical perspective that acknowledges other variables. Therefore, this study analysed the relation between DFM and disordered eating behavior, giving particular relevance to the role of patterns of cognitive appraisal.
This analysis was conducted by making participants face the possibility of experiencing an undesirable change of muscular mass. The results of our study indicate that losing muscular mass represented the more negative experience for participants, promoting a higher perception of threat appraisal and a lower perception of challenge appraisal. In addition, losing muscular mass was related to more muscularity-oriented behaviors and eating concerns. For health professionals, this finding can provide useful insights about which situation can put individuals at more risk of negative appraisal of changes of muscular mass, making them more prone to disordered eating. This result may be related to the internalization of a muscular physique as a standard for men’s beauty and health (Leit et al., 2002; Morrison et al., 2003). On the other hand, loss of muscular mass may be perceived as a risk for sport and exercise performance in males who practice regular exercise. In fact, in 66% of studies, athletes had higher DFM than non-athletes (Morrison et al., 2004; Zelli et al., 2010).
Additionally, this study indicates that cognitive appraisal can represent a pivotal dimension when explaining disordered eating behavior and DFM. The set of analyses conducted in this study confirmed this idea, as did analysing the results of multivariate analysis and structural equation models.
Multivariate analysis indicated that cognitive appraisal, and, more specifically, perceiving changes of muscular mass as more challenging was related to a higher tendency for muscularity-oriented body image, muscularity-oriented behaviors, weight and shape concerns, and eating concerns. Besides, the combination between perceiving changes of muscular mass as more challenging and less threatening was related to a higher tendency for performing intense exercise in order to control weight. These results noted that cognitive appraisal can be related to DFM and disordered eating behavior. However, the uniqueness of these results is the possibility that perceiving undesirable changes of muscular mass as challenging can also put participants at higher risk of eating disorders. In general, this is not in accordance with the general literature, showing that perceiving sources of stress as more challenging relates to a higher tendency to adapt positively to these demands (Gomes et al., 2017; Jones et al., 2009; Moore et al., 2013). One possible explanation for our results may be related to the possibility of participants evaluating the change of muscular mass as something that they can manage and control, and the tendency to change habits of eating and exercise likely represents some of the strategies used to deal with the undesirable change of muscular mass. Nevertheless, this result notes that, under some circumstances, a challenge perception can expose individuals to unhealthy behaviors, which is not strictly in accordance with previous research that demonstrated the benefits of challenge appraisal in distinct contexts and populations (Gomes et al., 2017).
Structural equation models indicated that cognitive appraisal mediated the relation between DFM and disordered eating behavior, providing a better understanding of eating problems than considering only the direct (and mostly tested) relation between a specific dimension (such as DFM) and disordered eating behavior. In fact, the mediation improved the explained variance of disordered eating behavior, from 34% in the direct model and 15% in the full mediation model to 39% in the partial model. This result reinforces the need of considering the role of cognitive appraisal in the comprehension of disordered eating behaviors in males in sport contexts, something that has been recognized in other health problems (Ahmad, 2005, 2010). However, our data provide additional insights into the role of cognitive appraisal. When comparing the full and partial mediations, the results indicate that partial mediation occurred for the three possibilities of mediation (muscularity-oriented body image – threat – disordered eating behavior; muscularity-oriented body image – challenge – disordered eating behavior; and muscularity-oriented body behaviors – threat –disordered eating behavior). The only exception was the mediation between muscularity-oriented body behaviors – challenge – disordered eating behavior. This finding means that although cognitive appraisal represents an important variable explaining disordered eating behavior, we cannot ignore the direct relation between higher DFM and disordered eating behavior. The mediation was invariant according to the type of physical activity assumed by the participants, meaning that all previous conclusions sustain despite the specific physical activity considered in our study.
The present study has some limitations, including the cross-sectional design; as such, causality cannot be inferred from the current results and the use of self-report measures. Further limitations are related to the use of self-reporting measures to evaluate complex constructs like, for instance, cognitive appraisal and disordered eating, the use of a convenience sample that may not be representative for the male population who practice sports regularly, and finally the combination of fitness center athletes and competitive athletes that may have different body perceptions, motives and values related to the sport’s practice. Future research should, therefore, evaluate differences between these specific samples regarding the role of cognitive appraisal in the association between drive for muscularity and disordered eating behaviour. On the positive side, this study included a conceptual framework to understand the relation between DFM and disordered eating behavior. On the other hand, the majority of DFM research sampled undergraduate students, and our study evaluates males who exercised on a regular basis, a group that we believe may be a high-risk group for DFM and disordered eating.
In summary, our results highlight the role of cognitive appraisal in DFM and disordered eating behavior in sport contexts. However, the results require replication throughout the inclusion of other important theoretical elements proposed by transactional perspectives (e.g., secondary cognitive appraisal) and the inclusion of sport activities even more prone to DFM (e.g., bodybuilding).
Acknowledgements
This study was conducted at Psychology Research Centre (UID/PSI/01662/2013), University of Minho, and supported by the Portuguese Foundation for Science and Technology, the Portuguese Ministry of Science, Technology and Higher Education through national funds and co-financed by FEDER through COMPETE2020 under the PT2020 Partnership Agreement (POCI-01-0145-FEDER-007653).
References
- Ahmad MM. Psychometric evaluation of the Cognitive Appraisal of Health Scale with patients with prostate cancer. J Adv Nurs. 2005;49(1):78–86. doi: 10.1111/j.1365-2648.2004.03266.x. [DOI] [PubMed] [Google Scholar]
- Ahmad MM. Validation of the cognitive appraisal health scale with Jordanian patients. Nurs Health Sci. 2010;12(1):74–79. doi: 10.1111/j.1442-2018.2009.00492.x. [DOI] [PubMed] [Google Scholar]
- Bentler PM. On tests and indices for evaluating structural models. Pers Indiv Differ. 2007;42(5):825–829. [Google Scholar]
- Bergeron D, Tylka TL. Support for the uniqueness of body dissatisfaction from drive for muscularity among men. Body Image. 2007;4(3):288–295. doi: 10.1016/j.bodyim.2007.05.002. [DOI] [PubMed] [Google Scholar]
- Byrne BM. Structural equation modeling with AMOS. New York: Routledge; 2010. (2nd ed.) [Google Scholar]
- Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: A theoretically based approach. J Pers Soc Psychol. 1989;56(2):267–283. doi: 10.1037/0022-3514.56.2.267. doi. [DOI] [PubMed] [Google Scholar]
- Chittester NI, Hausenblas HA. Correlates of drive for muscularity: The role of anthropometric measures and psychological factors. J Health Psychol. 2009;14(7):872–877. doi: 10.1177/1359105309340986. [DOI] [PubMed] [Google Scholar]
- Edwards C, Tod D, Molnar GA. Systematic review of the drive for muscularity research area. Int Rev Sport Exerc Psychol. 2014;7(1):18–41. [Google Scholar]
- Folkman S, Lazarus RS. Coping as a mediator of emotion. J Pers Soc Psychol. 1988;54:466–475. doi: 10.1037/0022-3514.54.3.466. doi. [DOI] [PubMed] [Google Scholar]
- Ginis KAM, Eng JJ, Arbour KP, Hartman JW, Phillips SM. Mind over muscle? Sex differences in the relationship between body image change and subjective and objective physical changes following a 12-week strength-training program. Body Image. 2005;2(4):363–372. doi: 10.1016/j.bodyim.2005.08.003. [DOI] [PubMed] [Google Scholar]
- Gomes AR. Gomes AR, Resende R, Albuquerque A. Positive human functioning from a multidimensional perspective: Promoting stress adaptation. New York: Nova Science; 2014. Positive human functioning in stress situations: An interactive proposal. [Google Scholar]
- Gomes AR, Faria S, Vilela C. Anxiety and burnout in young athletes: The mediating role of cognitive appraisal. Scand J Med Sci Spor. 2017;27(12):2116–2126. doi: 10.1111/sms.12841. doi. [DOI] [PubMed] [Google Scholar]
- Gomes AR, Simães C, Dias D. Occupational health. Hyderabad, India: Avid Science; 2017. A theoretical approach of adaptation to stress and implications for evaluation and research. [Google Scholar]
- Gomes AR, Teixeira P. Stress, cognitive appraisal, and psychological health: Testing instruments for health professionals. Stress and Health. 2016;32(2):167–172. doi: 10.1002/smi.2583. doi. [DOI] [PubMed] [Google Scholar]
- Hallsworth L, Wade T, Tiggemann M. Individual differences in male body-image: An examination of self-objectification in recreational body builders. Br J Health Psychol. 2005;10(3):453–465. doi: 10.1348/135910705X26966. [DOI] [PubMed] [Google Scholar]
- Hayes AF. Introduction to mediation, moderation, and conditional process analysis: A Regression-based approach. New York, NY: The Guilford Press; 2018. 2nd ed. 2018. [Google Scholar]
- Jones MV, Meijen C, McCarthy PJ, Sheffield D. A theory of challenge and threat states in athletes. Int Rev Sport Exerc Psychol. 2009;2(2):161–180. doi: 10.1080/17509840902829331. doi. [DOI] [Google Scholar]
- Lazarus RS. Emotion and adaptation. New York: Oxford University Press; 1991. [Google Scholar]
- Lazarus RS. Stress and emotion: A new synthesis. New York: Springer; 1999. [Google Scholar]
- Lazarus RS, DeLongis A, Folkman S, Gruen R. Stress and adaptational outcomes: The problem of confounded measures. Am Psychol. 1985;40(7):770–779. [PubMed] [Google Scholar]
- Lavender JM, Brown TA, Murray SB. Men, muscles, and eating disorders: an overview of traditional and muscularity-oriented disordered eating. Curr Psychiatry Rep. 2017;19(6):32. doi: 10.1007/s11920-017-0787-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leit RA, Gray JJ, Pope HG. The media's representation of the ideal male body: A cause for muscle dysmorphia? Int J Eat Disord. 2012;31(3):334–338. doi: 10.1002/eat.10019. [DOI] [PubMed] [Google Scholar]
- Litt D, Dodge TA. longitudinal investigation of the Drive for Muscularity Scale: Predicting use of performance enhancing substances and weightlifting among males. Body Image. 2008;5(4):346–351. doi: 10.1016/j.bodyim.2008.04.002. [DOI] [PubMed] [Google Scholar]
- Martins Y, Tiggemann M, Kirkbride A. Those speedos become them: The role of self-objectification in gay and heterosexual men's body image. Pers Soc Psychol Bull. 2007;33(5):634–647. doi: 10.1177/0146167206297403. [DOI] [PubMed] [Google Scholar]
- McCreary DR, Sasse DK. An exploration of the drive for muscularity in adolescent boys and girls. J Am Coll Health. 2000;48(6):297–304. doi: 10.1080/07448480009596271. [DOI] [PubMed] [Google Scholar]
- McCreary DR. Thompson JK, Cafri G. The muscular ideal: Psychological, social, and medical perspectives. Washington, DC: American Psychological Association; 2007. The Drive for Muscularity Scale: Description, psychometrics, and research findings. [Google Scholar]
- McPherson KE, McCarthy P, McCreary DR, McMillan S. Psychometric evaluation of the Drive for Muscularity Scale in a community-based sample of Scottish men participating in an organized sporting event. Body Image. 2010;7(4):368–371. doi: 10.1016/j.bodyim.2010.06.001. [DOI] [PubMed] [Google Scholar]
- Moore LJ, Wilson MR, Vine SJ, Coussens AH, Freeman P. Champ or chump? Challenge and threat states during pressurized competition. J Sport Exerc Psychol. 2013;3:551–562. doi: 10.1123/jsep.35.6.551. [DOI] [PubMed] [Google Scholar]
- Morrison TG, Morrison MA, Hopkins C. Striving for bodily perfection? An exploration of the drive for muscularity in Canadian men. Psychol Men Masculinity. 2003;4(2):111. [Google Scholar]
- Morrison TG, Morrison MA, Hopkins C, Rowan ET. Muscle mania: Development of a new scale examining the drive for muscularity in Canadian males. Psychol Men Masculinity. 2004;5(1):30. [Google Scholar]
- Morrison TG, Morrison MA, McCann L. Striving for bodily perfection? An overview of the drive for muscularity. Body image: New research. 2006:1–34. [Google Scholar]
- Zelli A, Lucidi F, Mallia L. The relationships among adolescents’ drive for muscularity, drive for thinness, doping attitudes, and doping intentions. J Clinic Sport Psychol. 2010;4(1):39–52. [Google Scholar]
- Tatham M, Turner H, Mountford VA, Tritt A, Dyas T, Waller G. Development, psychometric properties and preliminary clinical validation of a brief, session-by-session measure of eating disorder cognitions and behaviors: The ED-15. Int J Eat Disord. 2015;48:1005–1015. doi: 10.1002/eat.22430. doi. [DOI] [PubMed] [Google Scholar]
- Tabachnic BG, Fidell LS. Using multivariate statistics. Boston: Pearson; 2013. (6th ed.) [Google Scholar]
- Tod D, Edwards C. A meta-analysis of the drive for muscularity's relationships with exercise behaviour, disordered eating, supplement consumption, and exercise dependence. Int Rev Sport Exerc Psychol. 2015;8(1):185–203. [Google Scholar]