

Abstract
Recent data suggest that subclinical atherosclerosis is more related to visceral adipose tissue distribution than to overall fat mass. Both perirenal fat and epicardial fat are visceral fat depots surrounding the kidneys and the myocardium, respectively, which can be easily assessed by ultrasound. Their clinical relevance in children is largely unknown. This review describes studies relating perirenal and epicardial fat to cardiovascular disease or carotid intima-media thickness (cIMT), a well-established surrogate for subclinical atherosclerosis, and discusses this in context with our own data from children. In adults, both perirenal and epicardial fat are useful biological markers of visceral obesity. The former has been related to hypertension in overweight subjects and with atherosclerosis in patients with human immunodeficiency virus. The latter was associated with several metabolic syndrome components and with calcification of the carotid artery. In healthy prepubertal children, both epicardial and perirenal fat thickness, rather than total body fat mass, were related to cIMT. Ultrasonography measures of perirenal and epicardial fat are related to atherosclerosis in adults and may be convenient tools for the assessment of cardiometabolic risk in children.
Keywords: Body fat distribution, Intra-abdominal fat, Cardiovascular diseases, Carotid intima-media thickness, Child
Introduction
Atherosclerosis is the most common cause of morbidity and mortality worldwide and can remain silent for a long period of time before clinical manifestations of cardiovascular disease (CVD) are evident [1]. Carotid intima-media thickness (cIMT) is a well-established surrogate of subclinical atherosclerosis [2]. cIMT has been shown to be higher in children with traditional CVD risk factors, such as obesity, hypertension, diabetes, and chronic kidney disease, in comparison with healthy children [3]. Effective prevention and treatment of CVD in adulthood requires the improved identification of cardiovascular risk factors from childhood [4].
An excess of adipose tissue as seen in obesity, and especially its abnormal distribution among visceral fat depots, to a large extent, is related to the development of metabolic disorders and CVD [5]. Visceral adipose tissue is considered to be a type of "ectopic fat" because this type of fat depot, as opposed to subcutaneous adipose tissue, is not the usual location for lipid storage [6]. Some visceral fat reservoirs are more associated with increased risk for CVD than others. This may be especially true for abdominal visceral fat and liver fat [6].
Among visceral adipose tissue deposits, those located around the kidneys are regarded as metabolically active tissue that secretes pro-inflammatory cytokines, which in turn exert both local and systemic effects on the vasculature [7,8]. The association of perirenal fat thickness with hypertension [9] and atherosclerosis [10] has been described in adult patients.
Epicardial fat is enclosed between the pericardium and the myocardium layers and is also regarded as a metabolically active fat depot, secreting hormones, inflammatory cytokines, and chemokines [11]. Increased epicardial fat thickness has been described as a new risk factor for cardiometabolic diseases [12] as it plays a plausible role in the progression of atherosclerosis [13,14]. Thus, the extent and severity of CVD have been recently related to epicardial fat thickness [15].
Despite these observations and the fact that perirenal and epicardial fat depots can be easily assessed by ultrasound effortlessly, their clinical relevance in children is largely unknown. The objective of this review is to describe published studies in adults and adolescents and discuss them in the context of our own data with children.
Ectopic fat and CVD
According to the adipose tissue expandability hypothesis, the cause of metabolic health complications does not lie in total body fat excess. Instead, excess ectopic fat (within viscera or surrounding viscera), together with relatively less subcutaneous adipose tissue to buffer a surplus of exogenous lipids, may cause a state of lipotoxicity or chronic low-grade inflammation that increases the risk for CVD [16].
Following the development of techniques for measuring the different components of abdominal fat [17], studies have focused on the accumulation of fat in the abdominal region and its relationship to cardiovascular risk [18]. These studies have shown that abdominal visceral fat but not abdominal subcutaneous fat was associated with an unfavorable metabolic and cardiovascular profile, which includes all components of the metabolic syndrome [19].
1. Abdominal fat and CVD
The relationship between various adiposity measurements (body mass index [BMI], waist, and fat mass) and cIMT has been reported in adults and adolescents [20,21]. In adults from the Framingham Heart Study, more specific measurements of fat accumulation in the abdominal region were associated with metabolic syndrome and inflammatory markers [19,22]. A pediatric study that assessed subcutaneous and intra-abdominal fat thickness in children aged 5 years old found a significant association between body fat mass (especially intra-abdominal fat) and artery wall thickness and stiffness [23]. In another study in children and adolescents that assessed subcutaneous, intra-abdominal, and preperitoneal fat, both homeostasis model assessment for insulin resistance (HOMA-IR) and preperitoneal fat were predictors of cIMT [24].
2. Perirenal fat and risk factors for CVD
Fewer studies have related perirenal fat to CVD. In adults, higher perirenal fat was related to multiple risk factors for metabolic disease [25], including high blood pressure in overweight subjects [9] and atherosclerosis in patients with human immunodeficiency virus (HIV) [10]. Perirenal fat was also considered to be a proxy for visceral obesity in adult subjects [26].
Perirenal fat is located between the kidney capsule and the renal fascia. Both, perirenal adipose tissue and kidney cortex receive blood from the abdominal aorta. Perirenal fat is mainly composed of white adipose tissue that exerts several important physiologic functions including lipid storage and the synthesis of pro-inflammatory adipokines [8]. Perirenal fat of diet-induced obese mice showed an increased number of proinflammatory macrophages that participated in the synthesis of adipokines [27]. Thus, this fat deposition can exert direct effects on the kidney due to the local synthesis of adipokines [8]. The fact that perirenal fat and the kidney cortex are located nearby and receive blood from the same blood vessels reinforces the idea that the adipokines derived from the perirenal adipose tissue can directly impair renal function. In addition, a negative association between perirenal fat and kidney function has been described in patients with diabetes [28] and hypertension [29]. A recent study of obesity-related metabolic derangement in pigs showed that perirenal adipose tissue exerts a harmful effect on the endothelial function of the renal artery, which is mediated by pro-inflammatory cytokines derived from such adipose tissue to a certain extent [7].
Perirenal adipose tissue might also have a systemic effect through the production of adipokines that can exert metabolic and cardiovascular effects. In this regard, it should be noted that in our cohort of apparently healthy children, perirenal fat was the only fat deposition independently associated with serum high-molecular-weight adiponectin in obese children [30].
3. Epicardial fat and risk factors for CVD
A number of studies relate epicardial fat and risk for CVD in adult subjects [31-33] (reviewed in [15] and [34]). The International Atherosclerosis Society and the International Chair on Cardiometabolic Risk Working Group on Visceral Obesity have recently reported a joint position statement that summarizes the current evidence regarding ectopic adipose tissue deposition, including epicardial adipose tissue, as a relevant emerging cardiometabolic risk factor [35].
Epicardial adipose tissue is located below the visceral pericardium layer adjacent to the heart surface and encloses the epicardial coronary arteries. Epicardial fat is the genuine visceral fat reservoir of the heart, receives blood from the branches of the coronary arteries, and together with mesenteric and omental fat are derived from the splanchnopleuric mesoderm [15].
The role of epicardial adipose tissue in CVDs has been previously explained by its capacity to accumulate excess lipids and to produce pro-inflammatory molecules and other vasoactive substances that locally or systemically can impair vascular endothelial function and promote the development of atherosclerosis [11,36]. Epicardial fat also secretes adiponectin that can offer protection from vascular damage by any of the following mechanisms: stimulation of endothelium vasodilation, inhibition of inflammation, and blockage of growth factor-stimulated vascular smooth muscle cell growth. In obese subjects, epicardial fat is known to secrete less adiponectin and more tumor necrosis factor-alpha. As a consequence, epicardial fat has an impaired anticontractile function in obesity [36]. In summary, in hypertrophy of epicardial fat, such as that seen in obese subjects, an inability to store lipids, increased lipolysis, and inflammation arise to contribute to its deleterious effects on the vasculature [36].
Another aspect of epicardial fat is the higher mRNA expression of uncoupling protein-1 in this tissue in comparison to other adipose tissue reservoirs, leading some to speculate that it may function as brown adipose tissue (BAT) [36]. BAT, unlike white adipose tissue, is more resistant to a high-fat diet-induced inflammation. However, epicardial fat is not a bona fide BAT, as it does not contain characteristic multilocular cells. Although it cannot be excluded, because these BAT-like characteristics of epicardial fat are lost during hypertrophy of the fat depot.
In clinical studies, the thickness of epicardial adipose tissue has been suggested to be a novel cardiometabolic risk factor, as it shows a good correlation with visceral abdominal fat (measured by magnetic resonance imaging) and is related to the components of the metabolic syndrome [12,34]. Furthermore, it is associated with carotid calcification even after an adjustment for visceral abdominal fat [31-33].
Studies in adolescents
1. Perirenal fat and risk factors for CVD
To our knowledge, no studies have been published in adolescents.
2. Epicardial fat and risk factors for CVD
Few studies have examined the associations of epicardial fat with cardiometabolic risk factors in adolescents, and most have sought associations in obese adolescents.
Kim et al. [37] reported independent associations between epicardial fat and pulse wave velocity in 65 obese Korean adolescents (15–17 years of age). Elshorbagy et al. [38] reported that epicardial fat was independently associated with cIMT in subjects with obesity and metabolic syndrome in 60 obese children and adolescents (8–16 years of age) from Saudi Arabia. Similarly, Cabrera-Rego et al. [39] and Akyol et al. [40] described that epicardial fat was independently associated with cIMT in 66 obese children (9–16 years of age) from Cuba and 138 obese children (9–18 years of age) from Turkey, respectively.
Studies in children
To our knowledge, except for our own study reporting that perirenal adipose tissue was the main abdominal adipose tissue reservoir related to cIMT in apparently healthy prepubertal children, no other studies have been published [30]. Our results are summarized herein and data regarding epicardial fat are also presented.
We assessed a cohort of 702 Caucasian apparently healthy prepubertal children (47% girls; mean age, 8 years) from Northeastern Spain [30]. The study subjects were grouped according to their obesity status into lean (BMI-standard deviation score [SDS]<1, n=418), overweight (≤1 BMI-SDS<2, n=142), and obese (BMI-SDS ≥2, n=142). The methods for this study have already been reported [30]. In brief, cIMT was measured 1 cm away from the bifurcation of the right distal common carotid artery by ultrasonography (Fig. 1A). For perirenal fat, the ultrasound probe searched the point where the kidney surface was parallel to the skin. The thickness from the inner side of the abdominal musculature to the surface of the kidney was measured (Fig. 1B). Favre et al. [8] showed that the thickness of perirenal fat measured on the computed tomography scan was highly correlated with total perirenal fat volume. Therefore, perirenal fat thickness, rather than total perirenal adipose tissue volume, was chosen in our study because it was simple to measure using ultrasound.
Fig. 1.
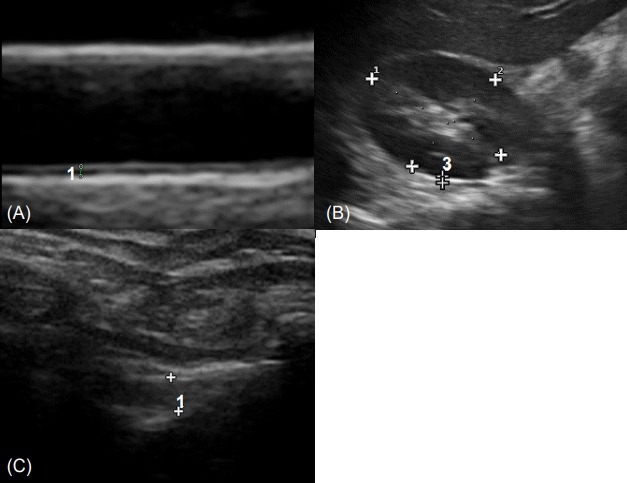
(A) Echocardiographic carotid intima-media thickness. Diastolic images were obtained using a linear 12-MHz transducer at the level of the distal common carotid artery, 1 cm away from its bifurcation. The intima-media thickness in the image is indicated between the 2 cursors and marked using the number 1. (B) Echocardiographic perirenal fat thickness. Children were placed in the supine position and the probe was moved to find the position at which the surface of the kidney was almost parallel to the skin. Longitudinal scans were then performed using a linear 12-MHz transducer. The thickness from the inner side of the abdominal musculature to the surface of the kidney was measured. The perirenal fat thickness in the image is indicated between the 2 cursors and marked using the number 3. (C) Echocardiographic epicardial fat thickness. Children were placed in the left lateral decubitus position. Measurements of the fat thickness adjacent to the free wall of the right ventricle were taken from the parasternal long-axis views using a linear 12-MHz transducer. Epicardial adipose tissue appears as an echo-free space between the pericardium and myocardium indicated by the 2 cursors and marked using the number 1.
Epicardial fat was measured in a sample of 239 children (42% girls; mean age, 8 years). This sample was to some extent enriched with obese subjects to increase the range of epicardial fat values. Because of the smaller sample size, subjects were categorized into 2 groups for further analyses, rather than 3 groups, based on BMI: lean (BMI-SDS<2, n=150) and obese (BMI-SDS≥2, n=89). Epicardial fat was measured by ultrasonography using a transthoracic linear 12-MHz transducer (Esaote MyLabTM25, Firenze, Italy) [41]. Children were placed in the left lateral decubitus position. Measurements of the fat thickness adjacent to the free wall of the right ventricle were taken from the parasternal long-axis views. Epicardial adipose tissue is assessed as an echo-free space between the pericardium and myocardium (Fig. 1C) [41].
1. Perirenal fat and risk factors for CVD
In all the studied subjects (n=702), perirenal fat was related to various metabolic and cardiovascular risk factors (higher height, weight, BMI, waist, fat mass, systolic blood pressure [SBP], triacylglycerol, intra-abdominal preperitoneal, subcutaneous, and cIMT, and lower high-density lipoprotein cholesterol) [30]. Associations with cIMT were similar in lean, overweight, and obese children (Fig. 2).
Fig. 2.
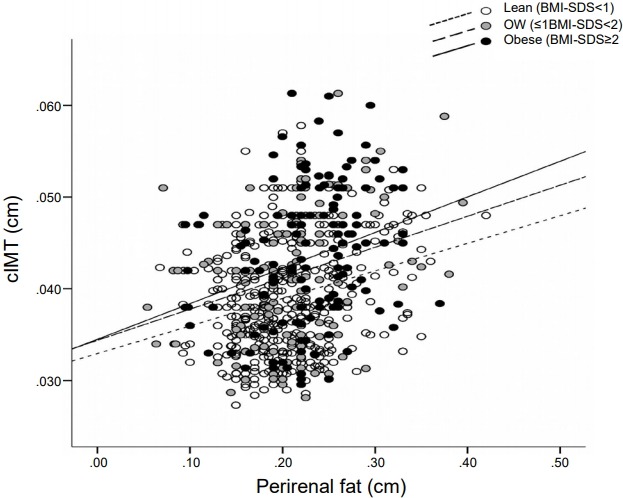
Scatter plot of perirenal fat and the cIMT of children according to BMI categories. White dots and a dotted line depict lean children (BMI-SDS<1), gray dots and a dashed line depict overweight (OW) children (≤1 BMI-SDS <2), and black dots and a solid line depict obese children (BMI-SDS ≥2). cIMT, carotid intima-media thickness; BMI, body mass index; SDS, standard deviation score.
In linear regression analyses adjusted for potential confounding, perirenal fat was an independent predictor of cIMT in all children. In overweight and obese children, perirenal fat was the only abdominal fat depot related to cIMT [30].
2. Epicardial fat and risk factors for CVD
In the subjects selected for epicardial fat measurement (n=239), higher values of epicardial fat were related to a poorer metabolic profile, displaying positive associations with anthropometric and cardiovascular parameters (weight, BMI, fat mass, waist, SBP, HOMA-IR, triacylglycerol; not shown) and with ultrasonographic assessments of perirenal fat and cIMT. Results were similar in lean and obese children.
In linear regression analyses, both epicardial fat and perirenal fat, but not fat mass or waist, were independent predictors of cIMT in all the studied subjects, as well as in lean and obese children (Table 1).
Table 1.
Multivariate linear models of carotid IMT as a dependent variable in apparently healthy prepubertal children from Northeastern Spain in whom epicardial fat was measured (n=239) and subgroups in relation to BMI (lean and obese)
| Variable | All children (n=239) |
Lean (BMI-SDS <2) (n=150) |
Obese (BMI-SDS ≥2) (n=89) |
|||
|---|---|---|---|---|---|---|
| Beta | Sig. | Beta | Sig. | Beta | Sig. | |
| Epicardial fat (cm) | 0.223 | 0.001 | 0.187 | 0.029 | 0.279 | 0.009 |
| Perirenal fat (cm) | 0.290 | <0.0001 | 0.347 | <0.0001 | 0.240 | 0.023 |
| Total R2 | 19.1 | 20.6 | 16.2 | |||
Nonpredictive variables: age, sex, fat mass, waist, homeostasis model assessment insulin resistance, and serum lipids.
IMT, intima-media thickness; BMI, body mass index; SDS, standard deviation score.
Conclusion
In adults, both perirenal and epicardial fat have been validated as surrogate markers of visceral obesity. The former has been related to hypertension in overweight subjects and with atherosclerosis in patients with HIV. The latter was related to several components of the metabolic syndrome and with carotid calcification.
In apparently healthy prepubertal children, cIMT was related to epicardial and perirenal fat thickness, rather than to body adiposity. These observations were found in both lean and obese children, which give further support for the independence of cIMT from general measurements of body adiposity.
Measurements of perirenal and epicardial fat by ultrasonography, rather than general measurements of body adiposity, may be convenient tools for the assessment of cardiometabolic risk in children.
Acknowledgments
We are grateful to all the families that participated in this study. JB is an investigator of the Miguel Servet Fund from Carlos III National Institute of Health, Spain (MS12/03239). ALB is an investigator of the I3 Fund for Scientific Research (Ministry of Economy and Competitiveness, Spain).
Footnotes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.
References
- 1.Must A, Jacques PF, Dallal GE, Bajema CJ, Dietz WH. Longterm morbidity and mortality of overweight adolescents. A follow-up of the Harvard Growth Study of 1922 to 1935. N Engl J Med. 1992;327:1350–5. doi: 10.1056/NEJM199211053271904. [DOI] [PubMed] [Google Scholar]
- 2.Lorenz MW, Markus HS, Bots ML, Rosvall M, Sitzer M. Prediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and metaanalysis. Circulation. 2007;115:459–67. doi: 10.1161/CIRCULATIONAHA.106.628875. [DOI] [PubMed] [Google Scholar]
- 3.Brady TM, Schneider MF, Flynn JT, Cox C, Samuels J, Saland J, et al. Carotid intima-media thickness in children with CKD: results from the CKiD study. Clin J Am Soc Nephrol. 2012;7:1930–7. doi: 10.2215/CJN.03130312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Celermajer DS, Ayer JG. Childhood risk factors for adult cardiovascular disease and primary prevention in childhood. Heart. 2006;92:1701–6. doi: 10.1136/hrt.2005.081760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Després JP. Body fat distribution and risk of cardiovascular disease: an update. Circulation. 2012;126:1301–13. doi: 10.1161/CIRCULATIONAHA.111.067264. [DOI] [PubMed] [Google Scholar]
- 6.Britton KA, Fox CS. Ectopic fat depots and cardiovascular disease. Circulation. 2011;124:e837. doi: 10.1161/CIRCULATIONAHA.111.077602. [DOI] [PubMed] [Google Scholar]
- 7.Ma S, Zhu XY, Eirin A, Woollard JR, Jordan KL, Tang H, et al. Perirenal fat promotes renal arterial endothelial dysfunction in obese swine through tumor necrosis factor-α. J Urol. 2016;195(4 Pt 1):1152–9. doi: 10.1016/j.juro.2015.08.105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Favre G, Grangeon-Chapon C, Raffaelli C, François-Chalmin F, Iannelli A, Esnault V. Perirenal fat thickness measured with computed tomography is a reliable estimate of perirenal fat mass. PLoS One. 2017;12:e0175561. doi: 10.1371/journal.pone.0175561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.De Pergola G, Campobasso N, Nardecchia A, Triggiani V, Caccavo D, Gesualdo L, et al. Para- and perirenal ultrasonographic fat thickness is associated with 24-hours mean diastolic blood pressure levels in overweight and obese subjects. BMC Cardiovasc Disord. 2015;15:108. doi: 10.1186/s12872-015-0101-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Grima P, Guido M, Zizza A, Chiavaroli R. Sonographically measured perirenal fat thickness: an early predictor of atherosclerosis in HIV-1-infected patients receiving highly active antiretroviral therapy? J Clin Ultrasound. 2010;38:190–5. doi: 10.1002/jcu.20664. [DOI] [PubMed] [Google Scholar]
- 11.Iacobellis G, Bianco AC. Epicardial adipose tissue: emerging physiological, pathophysiological and clinical features. Trends Endocrinol Metab. 2011;22:450–7. doi: 10.1016/j.tem.2011.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Iacobellis G, Ribaudo MC, Assael F, Vecci E, Tiberti C, Zappaterreno A, et al. Echocardiographic epicardial adipose tissue is related to anthropometric and clinical parameters of metabolic syndrome: a new indicator of cardiovascular risk. J Clin Endocrinol Metab. 2003;88:5163–8. doi: 10.1210/jc.2003-030698. [DOI] [PubMed] [Google Scholar]
- 13.Djaberi R, Schuijf JD, van Werkhoven JM, Nucifora G, Jukema JW, Bax JJ. Relation of epicardial adipose tissue to coronary atherosclerosis. Am J Cardiol. 2008;102:1602–7. doi: 10.1016/j.amjcard.2008.08.010. [DOI] [PubMed] [Google Scholar]
- 14.Iacobellis G, Lonn E, Lamy A, Singh N, Sharma AM. Epicardial fat thickness and coronary artery disease correlate independently of obesity. Int J Cardiol. 2011;146:452–4. doi: 10.1016/j.ijcard.2010.10.117. [DOI] [PubMed] [Google Scholar]
- 15.Fitzgibbons TP, Czech MP. Epicardial and perivascular adipose tissues and their influence on cardiovascular disease: basic mechanisms and clinical associations. J Am Heart Assoc. 2014;3:e000582. doi: 10.1161/JAHA.113.000582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gray SL, Vidal-Puig AJ. Adipose tissue expandability in the maintenance of metabolic homeostasis. Nutr Rev. 2007;65(6 Pt 2):S7–12. doi: 10.1111/j.1753-4887.2007.tb00331.x. [DOI] [PubMed] [Google Scholar]
- 17.Tokunaga K, Matsuzawa Y, Ishikawa K, Tarui S. A novel technique for the determination of body fat by computed tomography. Int J Obes. 1983;7:437–45. [PubMed] [Google Scholar]
- 18.Matsuzawa Y. Establishment of a concept of visceral fat syndrome and discovery of adiponectin. Proc Jpn Acad Ser B Phys Biol Sci. 2010;86:131–41. doi: 10.2183/pjab.86.131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Fox CS, Massaro JM, Hoffmann U, Pou KM, Maurovich-Horvat P, Liu CY, et al. Abdominal visceral and subcutaneous adipose tissue compartments: association with metabolic risk factors in the Framingham Heart Study. Circulation. 2007;116:39–48. doi: 10.1161/CIRCULATIONAHA.106.675355. [DOI] [PubMed] [Google Scholar]
- 20.Czernichow S, Bertrais S, Oppert JM, Galan P, Blacher J, Ducimetière P, et al. Body composition and fat repartition in relation to structure and function of large arteries in middle-aged adults (the SU.VI.MAX study) Int J Obes (Lond) 2005;29:826–32. doi: 10.1038/sj.ijo.0802986. [DOI] [PubMed] [Google Scholar]
- 21.Park MH, Skow Á, De Matteis S, Kessel AS, Saxena S, Viner RM, et al. Adiposity and carotid-intima media thickness in children and adolescents: a systematic review. BMC Pediatr. 2015;15:161. doi: 10.1186/s12887-015-0478-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pou KM, Massaro JM, Hoffmann U, Vasan RS, Maurovich-Horvat P, Larson MG, et al. Visceral and subcutaneous adipose tissue volumes are cross-sectionally related to markers of inflammation and oxidative stress: the Framingham Heart Study. Circulation. 2007;116:1234–41. doi: 10.1161/CIRCULATIONAHA.107.710509. [DOI] [PubMed] [Google Scholar]
- 23.Geerts CC, Evelein AM, Bots ML, van der Ent CK, Grobbee DE, Uiterwaal CS. Body fat distribution and early arterial changes in healthy 5-year-old children. Ann Med. 2012;44:350–9. doi: 10.3109/07853890.2011.558520. [DOI] [PubMed] [Google Scholar]
- 24.Epifanio M, Baldisserotto M, Sarria EE, Lazaretti A, Mattiello R. Ultrasound evaluation of carotid intima-media thickness in children. J Atheroscler Thromb. 2015;22:1141–7. doi: 10.5551/jat.29280. [DOI] [PubMed] [Google Scholar]
- 25.Roever L, Resende ES, Veloso FC, Diniz AL, Penha-Silva N, Casella-Filho A, et al. Perirenal fat and association with metabolic risk factors: The Uberlândia Heart Study. Medicine (Baltimore) 2015;94:e1105. doi: 10.1097/MD.0000000000001105. [DOI] [PubMed] [Google Scholar]
- 26.Jung M, Volonté F, Buchs NC, Gayet-Ageron A, Pugin F, Gervaz P, et al. Perirenal fat surface area as a risk factor for morbidity after elective colorectal surgery. Dis Colon Rectum. 2014;57:201–9. doi: 10.1097/DCR.0000000000000029. [DOI] [PubMed] [Google Scholar]
- 27.Weisberg SP, McCann D, Desai M, Rosenbaum M, Leibel RL, Ferrante AW., Jr Obesity is associated with macrophage accumulation in adipose tissue. J Clin Invest. 2003;112:1796–808. doi: 10.1172/JCI19246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Lamacchia O, Nicastro V, Camarchio D, Valente U, Grisorio R, Gesualdo L, et al. Para- and perirenal fat thickness is an independent predictor of chronic kidney disease, increased renal resistance index and hyperuricaemia in type-2 diabetic patients. Nephrol Dial Transplant. 2011;26:892–8. doi: 10.1093/ndt/gfq522. [DOI] [PubMed] [Google Scholar]
- 29.Chughtai HL, Morgan TM, Rocco M, Stacey B, Brinkley TE, Ding J, et al. Renal sinus fat and poor blood pressure control in middle-aged and elderly individuals at risk for cardiovascular events. Hypertension. 2010;56:901–6. doi: 10.1161/HYPERTENSIONAHA.110.157370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bassols J, Martínez-Calcerrada JM, Prats-Puig A, Carreras-Badosa G, Xargay-Torrent S, Lizarraga-Mollinedo E, et al. Perirenal fat is related to carotid intima-media thickness in children. Int J Obes (Lond) 2018;42:641–7. doi: 10.1038/ijo.2017.236. [DOI] [PubMed] [Google Scholar]
- 31.Rosito GA, Massaro JM, Hoffmann U, Ruberg FL, Mahabadi AA, Vasan RS, et al. Pericardial fat, visceral abdominal fat, cardiovascular disease risk factors, and vascular calcification in a community-based sample: the Framingham Heart Study. Circulation. 2008;117:605–13. doi: 10.1161/CIRCULATIONAHA.107.743062. [DOI] [PubMed] [Google Scholar]
- 32.Liu J, Fox CS, Hickson D, Sarpong D, Ekunwe L, May WD, et al. Pericardial adipose tissue, atherosclerosis, and cardiovascular disease risk factors: the Jackson heart study. Diabetes Care. 2010;33:1635–9. doi: 10.2337/dc10-0245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Yun CH, Lin TY, Wu YJ, Liu CC, Kuo JY, Yeh HI, et al. Pericardial and thoracic peri-aortic adipose tissues contribute to systemic inflammation and calcified coronary atherosclerosis independent of body fat composition, anthropometric measures and traditional cardiovascular risks. Eur J Radiol. 2012;81:749–56. doi: 10.1016/j.ejrad.2011.01.035. [DOI] [PubMed] [Google Scholar]
- 34.Iacobellis G, Willens HJ. Echocardiographic epicardial fat: a review of research and clinical applications. J Am Soc Echocardiogr. 2009;22:1311–9. doi: 10.1016/j.echo.2009.10.013. [DOI] [PubMed] [Google Scholar]
- 35.Neeland IJ, Ross R, Després JP, Matsuzawa Y, Yamashita S, Shai I, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. Lancet Diabetes Endocrinol. 2019;7:715–25. doi: 10.1016/S2213-8587(19)30084-1. [DOI] [PubMed] [Google Scholar]
- 36.Okada K, Ohshima S, Isobe S, Harada K, Hirashiki A, Funahashi H, et al. Epicardial fat volume correlates with severity of coronary artery disease in nonobese patients. J Cardiovasc Med (Hagerstown) 2014;15:384–90. doi: 10.2459/JCM.0b013e32836094da. [DOI] [PubMed] [Google Scholar]
- 37.Kim SJ, Kim HS, Jung JW, Kim NS, Noh CI, Hong YM. Correlation between epicardial fat thickness by echocardiography and other parameters in obese adolescents. Korean Circ J. 2012;42:471–8. doi: 10.4070/kcj.2012.42.7.471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Elshorbagy HH, Fouda ER, Kamal NM, Bassiouny MM, Fathi WM. Evaluation of epicardial fat and carotid intima-media thickness in obese children. Iran J Pediatr. 2016;26:e2968. doi: 10.5812/ijp.2968. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Cabrera-Rego JO, Iacobellis G, Castillo-Herrera JA, Valiente-Mustelier J, Gandarilla-Sarmientos JC, Marín-Juliá SM, et al. Epicardial fat thickness correlates with carotid intima-media thickness, arterial stiffness, and cardiac geometry in children and adolescents. Pediatr Cardiol. 2014;35:450–6. doi: 10.1007/s00246-013-0799-9. [DOI] [PubMed] [Google Scholar]
- 40.Akyol B, Boyraz M, Aysoy C. Relationship of epicardial adipose tissue thickness with early indicators of atherosclerosis and cardiac functional changes in obese adolescents with metabolic syndrome. J Clin Res Pediatr Endocrinol. 2013;5:156–63. doi: 10.4274/Jcrpe.1064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Schejbal V. Epicardial fatty tissue of the right ventricle--morphology, morphometry and functional significance. Pneumologie. 1989;43:490–9. [PubMed] [Google Scholar]