

Abstract
Backgrounds:
Hand fractures are the second most common upper-extremity fractures. The standard X-ray has shortcomings, such as exposure to radiation. Ultrasound has been reported as an alternative method of detecting hand fractures. In this study, we used meta-analysis to assess the diagnostic value of ultrasound for hand fractures.
Methods:
Web of Science, PubMed, Embase, and Cochrane Library databases were searched for relative citations up to June 2019. The pooled sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), diagnostic odds ratio (DOR), area under the summary receiver operating characteristic curve (AUC), and summary receiver operating characteristic (SROC) curve were estimated.
Results:
Seven studies including 842 participants (845 examined hands) met our inclusion criteria. The pooled sensitivity, specificity, PLR, and NLR of ultrasound for detecting hand fractures were 91%, 96%, 20.66, and 0.09, respectively. The pooled DOR was 231.17, indicating a very powerful diagnostic ability of ultrasound. Meta-regression showed that there was no heterogeneity with respect to age, cut-off, the performer of the ultrasound, and the types of hand fractures.
Conclusions:
Our results showed that ultrasound had an excellent diagnostic value for hand fractures. In clinic, we proposed using ultrasound as a first-line and radiation-free modality in detecting hand fractures, including phalanx and metacarpal fractures.
Keywords: hand fractures, meta-analysis, metacarpal, phalanx, ultrasound
1. Introduction
Hand fractures, consisting of phalangeal and metacarpal fractures, are the second most common upper-extremity fractures.[1] Approximately 2 per 1000 individuals annually experience hand fractures,[2] and they account for nearly 1.5% of the visits to hospital emergency departments (ED).[3] Anteroposterior and lateral X-rays are traditionally utilized for detecting hand fractures[4]; however, there are some drawbacks to the standard X-ray, including exposure to ionizing radiation and hospital dependency.[5,6]
Several studies have reported that ultrasound might be an alternative method of X-ray in detecting hand fractures.[7–13] Ultrasound could help to diagnose the soft tissue defects around fractures, which is difficult by X-ray.[4] Additionally, ultrasound can be rapidly performed, easily portable, and does not have the risk of radiation.[14–16]
To date, no studies have comprehensively evaluated the literature on hand fractures using ultrasound. Furthermore, data concerning the diagnostic value of ultrasound are variable. Hence, we did a meta-analysis to synthesize the diagnostic performance of ultrasound for phalanx and/or metacarpal fractures.
2. Materials and methods
2.1. Data sources and searches
We followed the preferred reporting items for systematic reviews and meta-analyses criteria.[17] Four English databases (Web of Science, PubMed, Embase, and Cochrane Library) were searched for relative citations up to June 2019. The language was restricted to English. The search terms included were “ultrasound,” “ultrasonography,” “sonography,” “hand fractures,” “finger fractures,” “metacarpal fractures,” and “phalanx fractures.” A comprehensive literature search strategy was applied in PubMed (MeSH terms in combination with title/abstracts): ((((((((thumb fractures [Title/Abstract]) OR metacarpal fractures [Title/Abstract]) OR metacarpal fractures [Title/Abstract]) OR phalanx fractures [Title/Abstract]) OR phalanges fractures [Title/Abstract]) OR figure fractures [Title/Abstract]) OR hand fractures [Title/Abstract])) AND ((“Ultrasonography” [Mesh]) OR (((((((((ultrasound[Title/Abstract]) OR ultrasonography [Title/Abstract]) OR ultrasonic [Title/Abstract]) OR sonogram [Title/Abstract]) OR sonography [Title/Abstract]) OR echotomography [Title/Abstract]) OR echography [Title/Abstract]) OR ultrasonographic [Title/Abstract]) OR sonographic [Title/Abstract])). We screened the references of the identified articles to find additionally eligible studies.
2.2. Study selection
Studies reporting ultrasound for detection of hand fractures were included according to the following criteria:
-
1.
reported on participants with hand (phalanx and/or metacarpal) fractures,
-
2.
used ultrasound as an index test,
-
3.
reported X-ray as the gold standard,
-
4.
the primary outcomes consisted of sensitivity and specificity of ultrasound, and
-
5.
the study design included randomized controlled trials and prospective studies.
The most comprehensive research was selected even though it was published more than twice. Additionally, a study was included twice when it reported phalanx and metacarpal fractures, respectively. Studies not published in English, retrospective case-control studies, guidelines, conference abstracts, veterinary experiments, and case reports were excluded. Two investigators independently determined the literature eligibility.
2.3. Data extraction and quality assessment
The data extracted included the first author, year, country, study setting, number of participants (including number of examined hands), number with fractures, fracture prevalence (%), mean age (years), reference standard, index test, probe frequency of index test (MHz), examiner training of index test, performer of index test, types of hand fractures (metacarpals and/or phalanges), true positive (TP), false positive (FP), false negative (FN), and true negative (TN), sensitivity (%), and specificity (%). Two investigators independently extracted data from the selected articles, and disagreements were settled through discussion and consensus. No ethical reviews were required based on previous published studies.
The Quality Assessment of Diagnostic Accuracy Studies tool-2 (QUADAS-2) evaluated the risk of bias and applicability of eligible studies across four domains: patient selection, index test, reference standard, and flow and timing.[18] According to the QUADAS-2, the same investigators independently reviewed the methodological quality of eligible articles. Disagreements were resolved by consensus. Revman 5.3 software was used to perform the quality assessment.
2.4. Primary data analysis
We used Stata 14.0 software to manage the primary data. Spearman correlation analysis was used to measure whether the threshold effect existed (P < .05) or not (P > .05). I2 and Cochrane Q test, which were utilized to distinguish heterogeneity, could be calculated by the formula “I2 = 100% × (Q – df) / Q.”[19] A bivariate random effects model should be established whenever I2 > 50%/P < .1 and I2 < 50%/P > .1.
We evaluated the primary outcomes to distinguish the diagnostic ability of ultrasound for hand fractures. The pooled sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), and diagnostic odds ratio (DOR) were calculated.[20,21] We constructed the summary receiver operating characteristic (SROC) curve, which was a measure of the diagnostic accuracy of the index test.[22,23] We also calculated the area under the curve (AUC); generally, an AUC more than 0.9 meant that the ultrasound had excellent diagnostic accuracy.
Additionally, we conducted the Galbraith plot analysis to identify the outlier studies. Meta-regression analysis was used to find possible sources of heterogeneity. Furthermore, we did the subgroup analysis including age (only children or not), cut-off (probe frequency range or not), performer of ultrasound (ED physician or expert radiologist), and the types of hand fractures (metacarpals and phalanges vs metacarpals or phalanges). Deeks’ funnel plot was used to assess publication bias.[24]
3. Results
3.1. Research findings
In total, 903 literature records were identified (Fig. 1). Eighty-four duplicates were removed automatically. We screened 819 titles and abstracts and excluded 794 records: 588 were non-eligible for hand fractures; 10 were non-eligible for ultrasound; 4 were non-eligible for primary outcomes; 38 were case reports; 47 focused on animal experiments; 43 were reviews, abstracts or letters; 56 were irrelevant topics; and 8 were repeated. Twenty-five full articles were assessed for inclusion. Ultimately, 7 of those articles were included in this meta-analysis.[7–13]
Figure 1.
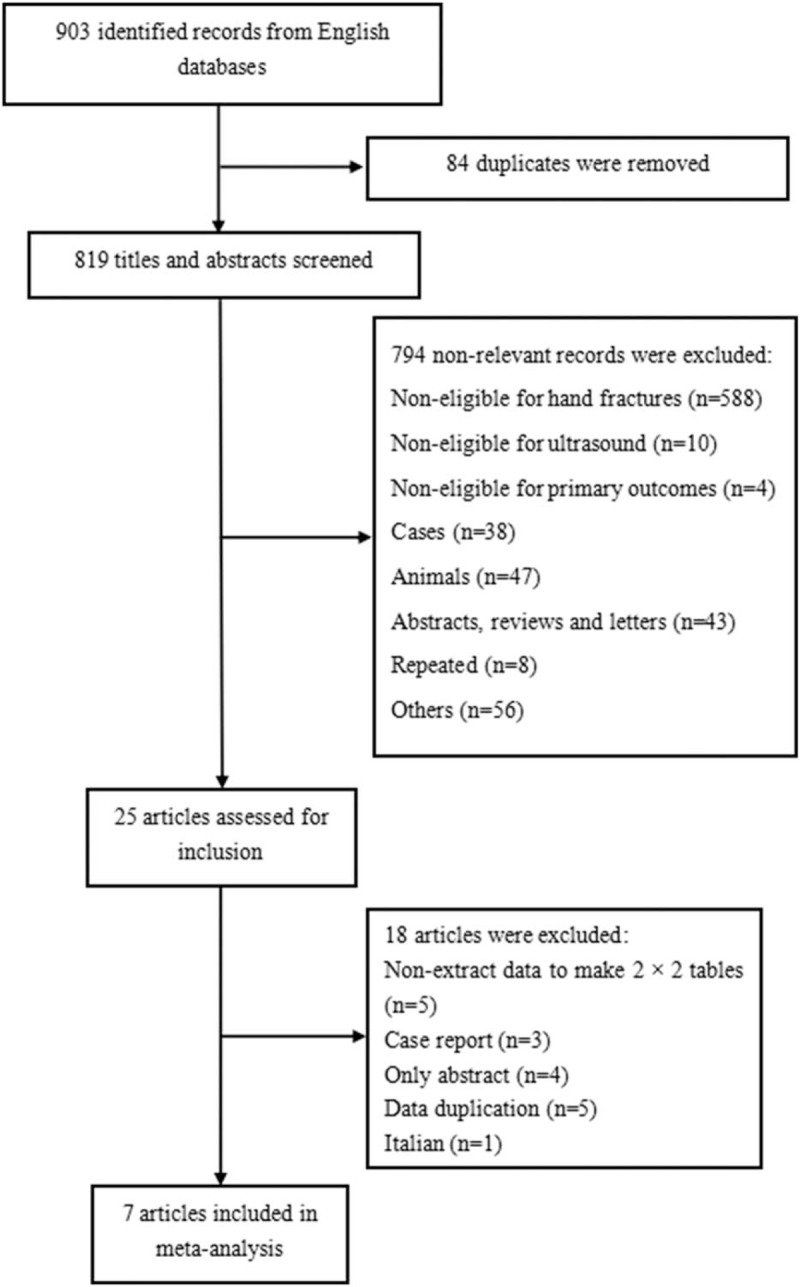
Flow chart of the process of included articles.
3.2. Characteristics and quality of study subjects
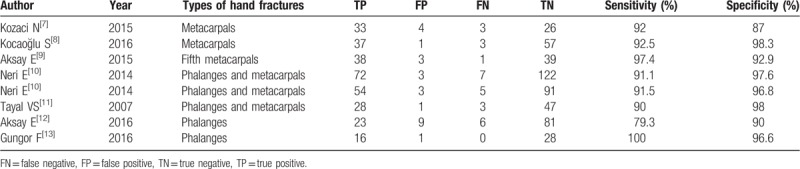
The characteristics of the 7 articles (8 trials) are listed in Table 1. There were 842 participants (845 examined hands) involved. All were prospective observational studies. The prevalence of hand fractures was 39% (329/845). All studies used X-ray as the reference standard, except one patient, who was diagnosed by computed tomography in combination with X-ray.[9] The index test was ultrasound. The probe frequency of the ultrasound ranged from 7.5 to 18 MHz. The ultrasound performers were ED physicians; one study also included an expert radiologist.[10] Three trials only included metacarpal fractures,[7–9] 3 included phalanx and metacarpal fractures[10,11] and 2 only included phalanx fractures.[12,13] The sensitivity, specificity, TP, FP, FN, and TN of ultrasound are shown in Table 2.
Table 1.
Characteristics of eligible studies.
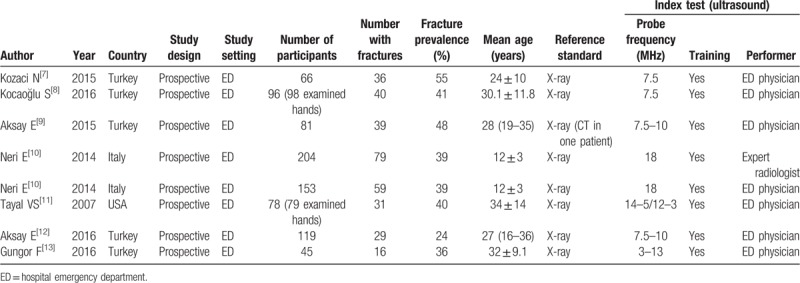
Table 2.
Baseline data of included studies.
As shown in Figure 2, the quality of all the studies was relatively high. Patient selection bias was unclear for one study because it did not report the time and consecutiveness of patient enrolment[11]; four studies had unclear bias in index tests because the ultrasound had a range of probe frequency.[9,11–13] All studies had low risk of bias in reference standard and flow and timing. The applicability concerns were generally low.
Figure 2.
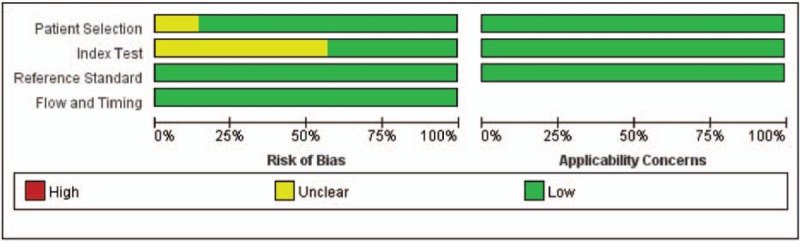
Risk of bias and applicability concerns of included studies.
3.3. Pooled analysis
No threshold effect was found in this meta-analysis (P-value = 1.00). The heterogeneity was relatively small (I2 = 0%, P = .402). A total of 845 hands (842 participants) were detected. The sensitivity for ultrasound was 0.91 (95% CI: 0.88–0.94) and the specificity was 0.96 (95% CI: 0.92–0.97) (Fig. 3). The pooled PLR and NLR of ultrasound were 20.66 (95% CI: 11.89–35.90) and 0.09 (95% CI: 0.06–0.13), respectively. DOR was 231.17 (95% CI: 105.74–505.40), indicating that the ability of ultrasound to detect hand fractures was relatively good. In addition, the AUC was 0.97 (95% CI: 0.95–0.98) and the SROC curves for ultrasound are shown in Figure 4.
Figure 3.
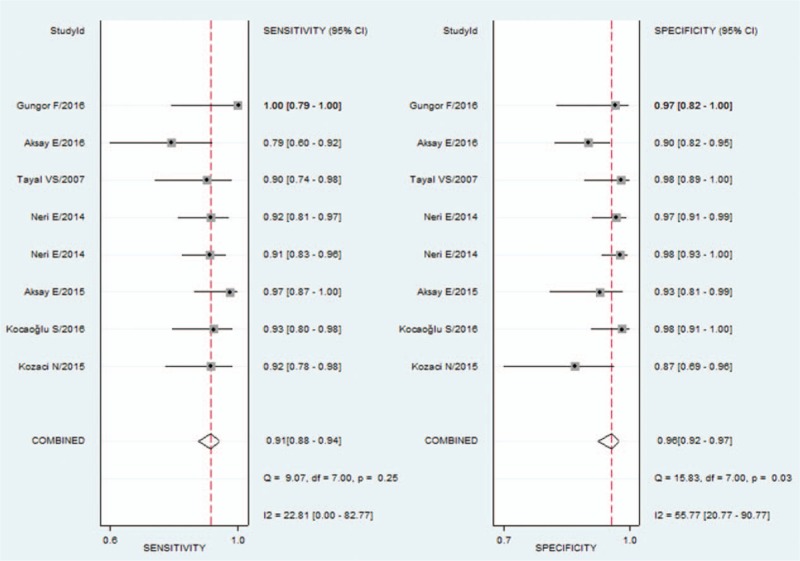
The forest plots of the pooled sensitivity and specificity of ultrasound to detect hand fractures. CI = confidence interval.
Figure 4.
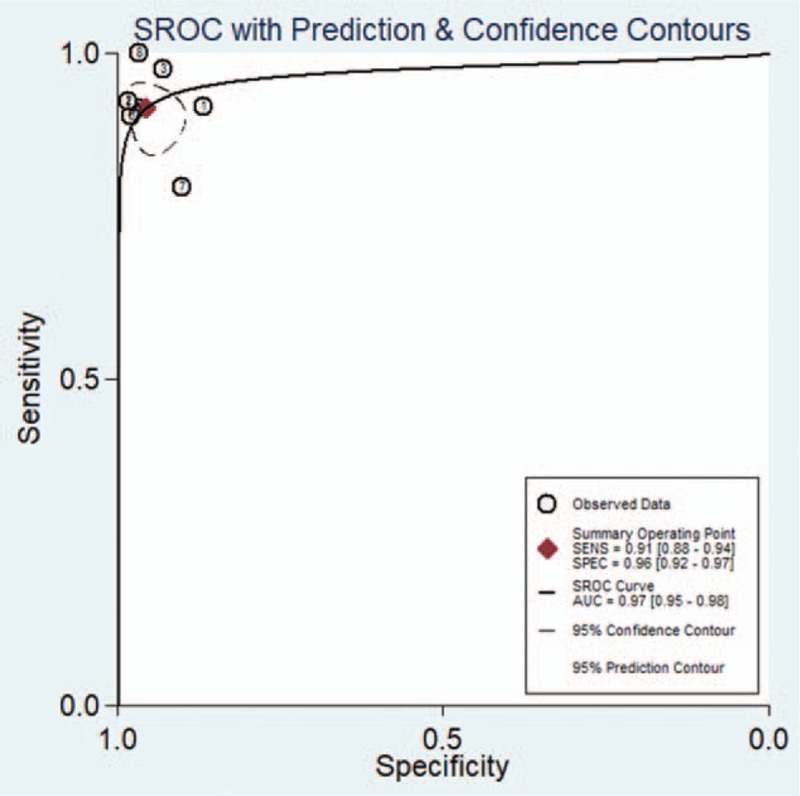
The SROC curve for assessment of ultrasound to detect hand fractures. AUC = area under curve, SE = standard error, SROC = summary receiver operating characteristic.
3.4. Galbraith plot, meta-analysis, and subgroup analysis
The Galbraith plot identified no outlier studies in this meta-analysis (Fig. 5). Age, cut-off, performer of ultrasound, and the types of hand fractures included in the meta-regression analysis were not potential sources of inconsistency (P = .33, .67, .50, and .13, respectively).
Figure 5.
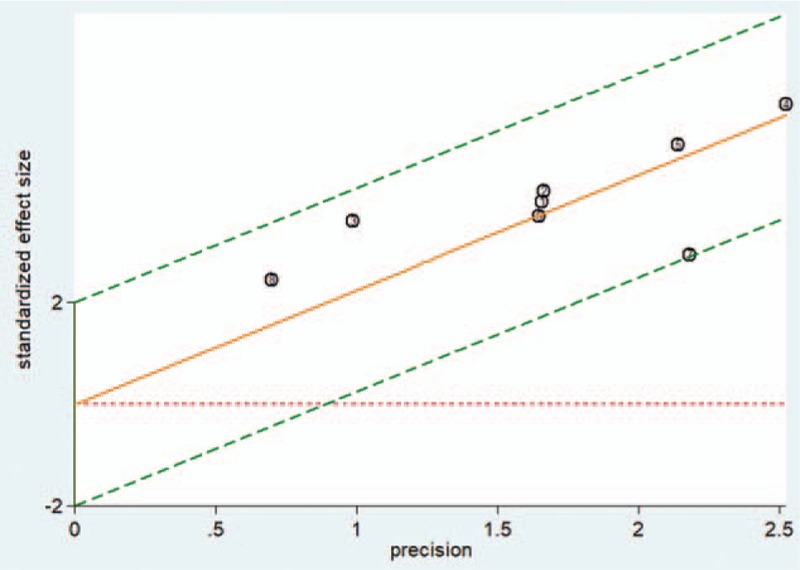
The Galbraith plot of ultrasound to detect hand fractures.
The sensitivity and specificity of children and adults with/without children were similar (91% vs 92% and 97% vs 94%, respectively). With respect to the cut-off of ultrasound, ranged probe frequencies had a comparable diagnostic performance to fixed probe frequencies (sensitivity: 0.91 and 0.92; specificity: 0.94 and 0.96). The sensitivity and specificity between the ED physicians and the expert radiologist were similar (91% and 92%, 98%, and 95%). Finally, a similar overall performance was detected when comparing metacarpals and phalanges with metacarpals or phalanges (sensitivity: 0.91 and 0.92; specificity: 0.97 and 0.93).
3.5. Publication bias
The P-value obtained from the Deek's funnel plot was .68, which indicated no striking publication bias (Fig. 6).
Figure 6.
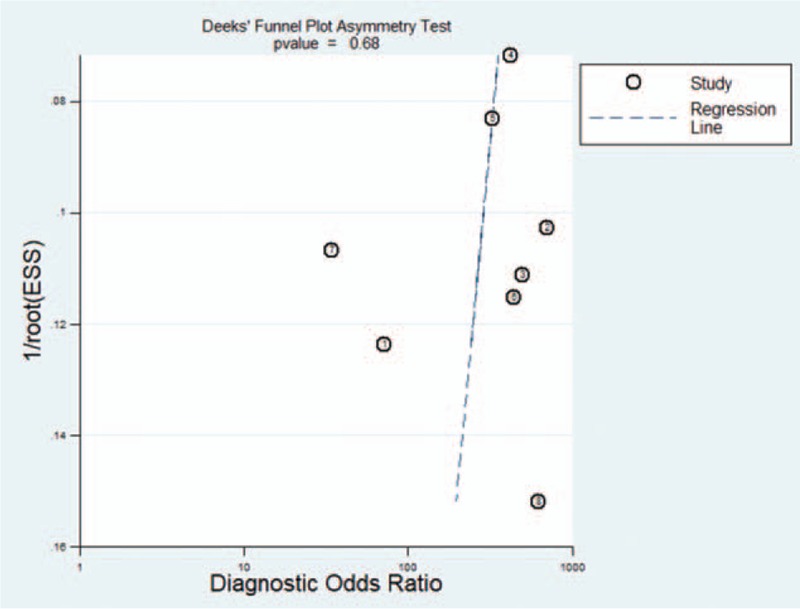
The Deek's funnel plot of ultrasound to detect hand fractures.
4. Discussion
In recent years, many researchers have focused on the value of ultrasound in detecting upper-extremity fractures. Joshi et al reported that ultrasound sensitivity varied from 85% to 100% and specificity varied from 73% to 100% in upper-extremity fractures.[25] Chartier et al found that point-of-care ultrasound showed relatively high sensitivity (93.1%) and specificity (92.9%) for diagnosis in pediatric forearm fractures.[26] Douma-den Hamer et al showed that ultrasound had a perfect value in detecting distal forearm fractures (sensitivity: 97%, specificity: 95%), especially in children.[27] Lee et al suggested that ultrasound should be a first-line tool in detecting pediatric elbow fractures by trained physicians.[14] To fill the gap in knowledge concerning ultrasound for upper-extremity fractures, we investigated its diagnostic value in detecting hand fractures. We suggested that an ultrasound should be a first-line, non-invasive, and radiation-free modality in detecting hand fractures and the upper-extremity fractures.
In this study, we first conducted a meta-analysis to evaluate the overall performance of ultrasound in detecting phalanx and metacarpal fractures. Ultrasound has an excellent diagnostic value (sensitivity: 91%, specificity: 96%, AUC = 0.97) in detecting hand fractures. Additionally, the PLR of 20.66 and NLR of 0.09 suggested that ultrasound had a good value in diagnosing hand fractures.
The results were made more reliable in three important ways. First, we excluded the case-control studies that might overestimate the real results. Second, the overall study quality was high; the ultrasounds and X-rays were performed and analyzed under blind conditions. Third, the inconsistency in this study was relatively small (I2 = 0%, P = .402) and the Galbraith plot identified no outlier studies, increasing the stability of the overall performance of the ultrasound. Furthermore, the absence of a striking publication bias strengthened the correctness of the results (P = .68).
The different types of hand fractures showed similar overall performance in phalanx and/or metacarpal fractures; it did not lead to heterogeneity (P = .4922). In the next step, we need more studies about these different three types of hand fractures to explain these results.
The real value of ultrasound for detecting hand fractures might lower than we reported due to several limitations. First, most of the eligible studies were from Turkey. Also, the same author (Aksay E) reported two studies in the same hospital, one focused on metacarpal fractures and another concentrated with phalanx fractures. The selection bias did exist. Second, the heterogeneity is still a concern. Even though the age, cut-off, performer of ultrasound and the types of hand fractures were not significant sources of inconsistency (P > .05), they could increase it, thereby reducing the stability of the whole outcome. Third, although publication bias was not significant it should not be ignored; because of limited linguistic abilities, we included only English studies.
5. Conclusion
This meta-analysis showed that ultrasound had an excellent diagnostic value for hand fractures. In clinic, we propose the utilization of ultrasound as a first-line and radiation-free modality in detecting hand fractures, including phalanx and metacarpal fractures. Furthermore, multi-center, large, and prospective studies are requested to support this finding.
Acknowledgments
This work was supported by the Natural Science Grants from Science and Technology Bureau of Gansu Provincial (2018–0405-JCC-0506).
Author contributions
Conceptualization: Wenjun Zhao.
Data curation: Wenjun Zhao, Gang Wang, Binjuan Chen.
Formal analysis: Wenjun Zhao, Gang Wang, Binjuan Chen, Jihong Xiao, Xingjie Li.
Funding acquisition: Xingjie Li.
Investigation: Wenjun Zhao, Gang Wang, Binjuan Chen, Jihong Xiao, Xiaoping Sun, Tingting Wu, Haijun Ren.
Methodology: Wenjun Zhao, Gang Wang.
Project administration: Wenjun Zhao.
Resources: Wenjun Zhao.
Software: Wenjun Zhao, Gang Wang, Binjuan Chen, Jihong Xiao, Xiaoping Sun.
Supervision: Wenjun Zhao.
Validation: Wenjun Zhao, Gang Wang, Xingjie Li.
Visualization: Wenjun Zhao.
Writing – original draft: Wenjun Zhao.
Writing – review & editing: Wenjun Zhao, Jihong Xiao, Xiaoping Sun, Tingting Wu, Haijun Ren, Xingjie Li.
Footnotes
Abbreviations: 95% CI = 95% confidence interval, AUC = area under the summary receiver operating characteristic curve, DOR = diagnostic odds ratio, NLR = negative likelihood ratio, PLR = positive likelihood ratio, QUADAS-2 = Quality Assessment of Diagnostic Accuracy Studies tool-2, SROC = summary receiver operating characteristic.
How to cite this article: Zhao W, Wang G, Chen B, Xiao J, Sun X, Wu T, Ren H, Li X. The value of ultrasound for detecting hand fractures. Medicine. 2019;98:44(e17823).
The authors have no conflicts of interest to disclose.
References
- [1].Cheah AE, Yao J. Hand fractures: indications, the tried and true and new innovations. J Hand Surg Am 2016;41:712–22. [DOI] [PubMed] [Google Scholar]
- [2].Karl JW, Olson PR, Rosenwasser MP. The epidemiology of upper extremity fractures in the United States, 2009. J Orthop Trauma 2015;29:e242–4. [DOI] [PubMed] [Google Scholar]
- [3].Torabi M, Lenchik L, Beaman FD, et al. ACR Appropriateness Criteria® acute hand and wrist trauma. J Am Coll Radiol 2019;16(5S):S7–17. [DOI] [PubMed] [Google Scholar]
- [4].Pourmand A, Shokoohi H, Maracheril R. Diagnostic accuracy of point-of-care ultrasound in detecting upper and lower extremity fractures: an evidence-based approach. Am J Emerg Med 2018;36:134–6. [DOI] [PubMed] [Google Scholar]
- [5].Linet MS, Slovis TL, Miller DL, et al. Cancer risks associated with external radiation from diagnostic imaging procedures. CA Cancer J Clin 2012;62:75–100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Schneppendahl J, Windolf J, Kaufmann RA. Distal radius fractures: current concepts. J Hand Surg 2012;37:1718–25. [DOI] [PubMed] [Google Scholar]
- [7].Kozaci N, Ay MO, Akcimen M, et al. The effectiveness of bedside point-of-care ultrasonography in the diagnosis and management of metacarpal fractures. Am J Emerg Med 2015;33:1468–72. [DOI] [PubMed] [Google Scholar]
- [8].Kocaoğlu S, Özhasenekler A, İçme F, et al. The role of ultrasonography in the diagnosis of metacarpal fractures. Am J Emerg Med 2016;34:1868–71. [DOI] [PubMed] [Google Scholar]
- [9].Aksay E, Yesilaras M, Kilic TY, et al. Sensitivity and specificity of bedside ultrasonography in the diagnosis of fractures of the fifth metacarpal. Emerg Med J 2015;32:221–5. [DOI] [PubMed] [Google Scholar]
- [10].Neri E, Barbi E, Rabach I, et al. Diagnostic accuracy of ultrasonography for hand bony fractures in paediatric patients. Arch Dis Child 2014;99:1087–90. [DOI] [PubMed] [Google Scholar]
- [11].Tayal VS, Antoniazzi J, Pariyadath M, et al. Prospective use of ultrasound imaging to detect bony hand injuries in adults. J Ultrasound Med 2007;26:1143–8. [DOI] [PubMed] [Google Scholar]
- [12].Aksay E, Kilic TY, Yesilaras M, et al. Accuracy of bedside ultrasonography for the diagnosis of finger fractures. Am J Emerg Med 2016;34:809–12. [DOI] [PubMed] [Google Scholar]
- [13].Gungor F, Akyol KC, Eken C, et al. The value of point-of-care ultrasound for detecting nail bed injury in ED. Am J Emerg Med 2016;34:1850–4. [DOI] [PubMed] [Google Scholar]
- [14].Lee SH, Yun SJ. Diagnostic performance of ultrasonography for detection of pediatric elbow fracture: a meta-analysis. Ann Emerg Med 2019;pii: S0196-0644(19)30228-8. [DOI] [PubMed] [Google Scholar]
- [15].Pourmand A, Lee D, Davis S, et al. Point-of-care ultrasound utilizations in the emergency airway management: an evidence-based review. Am J Emerg Med 2017;35:1202–6. [DOI] [PubMed] [Google Scholar]
- [16].Avci M, Kozaci N, Beydilli I, et al. The comparison of bedside point-of-care ultrasound and computed tomography in elbow injuries. Am J Emerg Med 2016;34:2186–90. [DOI] [PubMed] [Google Scholar]
- [17].McInnes MDF, Moher D, Thombs BD, et al. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: the PRISMA-DTA statement. JAMA 2018;319:388–96. [DOI] [PubMed] [Google Scholar]
- [18].Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 2011;155:529–36. [DOI] [PubMed] [Google Scholar]
- [19].Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Vamvakas EC. Meta-analyses of studies of the diagnostic accuracy of laboratory tests: a review of the concepts and methods. Arch Pathol Lab Med 1998;122:675–86. [PubMed] [Google Scholar]
- [21].Devillé WL, Buntinx F, Bouter LM, et al. Conducting systematic reviews of diagnostic studies: didactic guidelines. BMC Med Res Methodol 2002;2:9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Chappell FM, Raab GM, Wardlaw JM. When are summary ROC curves appropriate for diagnostic meta-analyses? Stat Med 2009;28:2653–68. [DOI] [PubMed] [Google Scholar]
- [23].Arends LR, Hamza TH, van Houwelingen JC, et al. Bivariate random effects meta-analysis of ROC curves. Med Decis Making 2008;28:621–38. [DOI] [PubMed] [Google Scholar]
- [24].Deeks JJ, Macaskill P, Irwig L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J Clin Epidemiol 2005;58:882–93. [DOI] [PubMed] [Google Scholar]
- [25].Joshi N, Lira A, Mehta N, et al. Diagnostic accuracy of history, physical examination, and bedside ultrasound for diagnosis of extremity fractures in the emergency department: a systematic review. Acad Emerg Med 2013;20:1–5. [DOI] [PubMed] [Google Scholar]
- [26].Chartier LB, Bosco L, Lapointe-Shaw L, et al. Use of point-of-care ultrasound in long bone fractures: a systematic review and meta-analysis. CJEM 2017;19:131–42. [DOI] [PubMed] [Google Scholar]
- [27].Douma-den Hamer D, Blanker MH, Edens MA, et al. Ultrasound for distal forearm fracture: a systematic review and diagnostic meta-analysis. PLoS One 2016;11:e0155659. [DOI] [PMC free article] [PubMed] [Google Scholar]