

Abstract
Background:
The aim of this study was to compare three intubation methods during cardiopulmonary resuscitation using an adult-manikin.
Methods:
Thirty-nine paramedics were included in this study. Each participant performed endotracheal intubation during continuous chest compressions using 3 different methods: conventional Macintosh laryngoscope without additional intubation aids (MAC), conventional Macintosh laryngoscope with gum-elastic bougie (GEB), or flexible tip bougie (FTB). First attempt intubation success rate and intubation time was measured.
Results:
Intubation success rate was 39% with the use of MAC, 92% with GEB and 95% with FTB. It was statistically lower with MAC than with GEB (P < .001) and FTB (P < .001). There was no difference between GEB and FTB in intubation success rate (P = .644). The mean(SD) intubation time was 28.43 (13.81)s with MAC, 25.69 (5.35)s with GEB and 21.41 (2.88)s with FTB. Intubation time was significantly longer with GEB than with FTB (P < .001).
Conclusions:
Within limitations, results of our study suggest that intubation aids facilitate tracheal intubation during continuous chest compressions. Using flexible tip bougie shortens the duration of the procedure compared to gum elastic bougie.
Keywords: cardiopulmonary resuscitation, flexible tip bougie, gum elastic bougie, intubation, macintosh laryngoscope
1. Introduction
In the US, out-of-hospital cardiac arrest (OHCA) occurs more than 350,000 times each year, with fewer than 10% of patients in 2016 surviving to discharge.[1] Endotracheal intubation is considered the method of choice in effective airway management during cardiopulmonary resuscitation (CPR). It allows delivery of a high concentration of oxygen, enables ventilation without interrupting chest compressions, avoids gastric insufflation and protects the airway from gastric contents.[2] Unfortunately, endotracheal intubation has a high failure rate and often requires multiple attempts, especially when performed by inexperienced personnel.[3,4] Almost a fourth of all CPR interruptions are caused by tracheal intubation attempts.[5] According to European Resuscitation Council guidelines endotracheal intubation should be performed without stopping chest compressions, or any pause should be shorter than five seconds.[6] A gum-elastic bougie (GEB) can be used to facilitate placement of the endotracheal tube (ET tube). The diameter of this device is smaller than the ET tube and increases the intubation success rate, especially in difficult airway scenarios.[7–9] The flexible tip bougie (FTB) is a new device that can be used during direct and video laryngoscopy procedures. It has a slider tabs, which allow the operator to move the tip anteriorly and posteriorly. The tip of this device has a bright phosphorous coating to increase its visibility (Fig. 1). The operator can use anterior flexion when introducing the bougie into the airway and straighten the tip to advance the tube.
Figure 1.

Flexible tip bougie (A). Posterior (B) and anterior (C) flexion of the tip.
The aim of this study was to compare intubation success rates and times using three different intubation methods during continuous chest compressions.
2. Methods
This is a prospective, randomized crossover manikin study. The ethics committee of the Department of Medicine and Health Science at Jan Kochanowski University approved the study protocol. Written informed consent was obtained from all participants.
An ALS manikin (MegaCode Kelly, Laerdal Medical, Norway) was used to simulate the patient for this study, in which 39 paramedics participated. A LUCAS 2 System device (Physio-Control, Lund, Sweden) was used to achieve continuous chest compression. All participants attended a workshop prior to data collection to learn how to use the intubation aids. Each participant was able to practice endotracheal intubation on a different manikin for 5 minutes.
In this study each participant performed endotracheal intubation during continuous chest compressions at a rate of 100 min−1 (achieved with the LUCAS 2 System), using three different methods: conventional Macintosh laryngoscope without additional intubation aids (MAC), conventional Macintosh laryngoscope with gum-elastic bougie (GEB), conventional Macintosh laryngoscope with flexible tip bougie (FTB). The order in which subjects used these methods was randomized using www.researchrandomizer.org (Fig. 2). A cuffed ET tube with an internal diameter of 8.0 was used in each scenario. In cases of the use of intubation aids an assistant was available to “railroad” the ET tube onto the introducer. After each intubation all participants were asked to describe glottis views based on the Cormack-Lehane system.[10]
Figure 2.
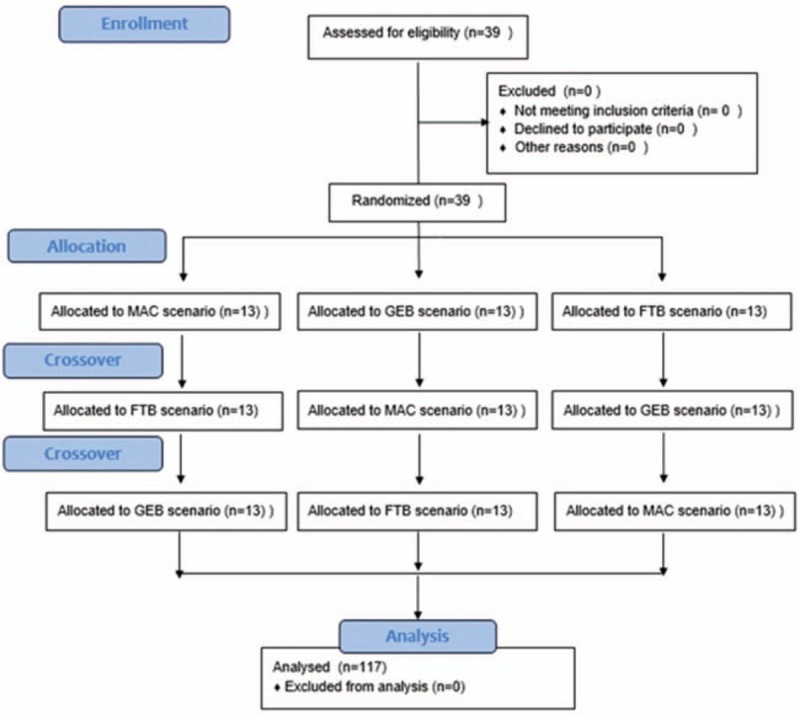
Randomization flow chart. FTB = flexible tip bougie, GEB = gum elastic bougie, MAC = conventional Macintosh laryngoscope.
The primary outcome of this study was the success rate of the first intubation attempt, and the secondary outcome was intubation time. Failed intubation was defined as the inability to intubate, by insertion of the endotracheal tube into the esophagus of the manikin, within 60 seconds. Intubation time was defined as the time between the participant picking up the laryngoscope and the first chest inflation using a ventilation bag.
Statistical analysis was performed using the Statistica 13.1 software (StatSoft, Tulsa, OK). Data for intubation times had normal distribution in all groups and a parametric t test was used for statistical analysis. To compare intubation success rates a Pearson's chi-square test was used. A result of P < .05 was considered statistically significant.
3. Results
In total, 39 paramedics were screened for eligibility; all met eligibility criteria and were randomized between July and September 2019.
3.1. Glottis view
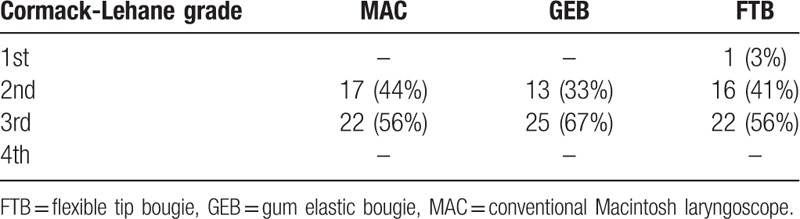
During all scenarios the median glottis view was described as the 3rd degree based on the Cormack–Lehane scale. The 2nd degree glottis view was obtained in 44% of cases in the MAC group, 33% in GEB and 41% in FTB. There was one case of 1st degree glottis view in an FTB scenario and there were no cases of 4th degree (Table 1). There was no statistically significant difference in glottis view between all groups (P > .05).
Table 1.
Glottis view based on Cormack–Lehane scale.
3.2. Intubation success rate
The success rate of the first intubation attempt was 39% using MAC, 92% with GEB and 95% with FTB (Fig. 3). It was statistically lower in the MAC, than in the GEB (P < .001) and FTB (P < .001) scenarios. There was no statistically significant difference between GEB and FTB in intubation success rates (P = .644).
Figure 3.
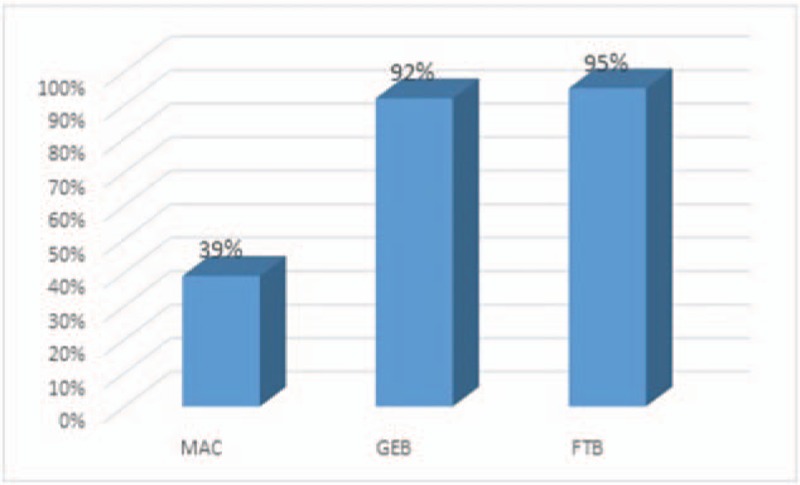
Intubation success rate chart.
3.3. Intubation time
The mean (SD) intubation time was 28.43 (13.81)s in MAC, 25.69 (5.35)s in GEB and 21.41 (2.88)s in FTB. The difference between MAC and GEB or FTB showed no statistical significance (P > .05). Intubation time was statistically shorter in the FTB scenario than for GEB (P < .001) (Fig. 4).
Figure 4.
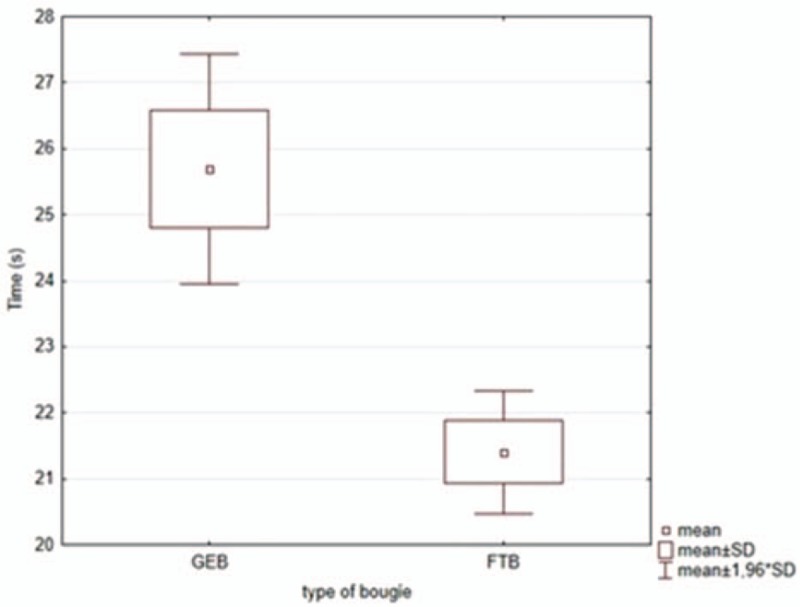
Mean intubation time using gum elastic bougie and flexible tip bougie.
4. Discussion
In this manikin study, the effectiveness and time needed to intubate a patient during cardiopulmonary resuscitation was compared, with and without the use of intubation introducers. All procedures were performed by paramedics working in the Polish Emergency Medical Services.
Participants were able to effectively intubate the manikin in only 39% of cases using a conventional Macintosh laryngoscope alone. During continuous chest compressions, oscillatory head movements may increase the difficulty of visualizing entrance to the trachea and impede achieving a stable sniffing position. In a randomized clinical trial conducted by Wang et al the rate of initial airway success was 51.6% (760/1499) in cases of OHCA.[11]
The results of the study indicate that the use of a gum-elastic bougie or flexible tip bougie improves first attempt intubation success rates during CPR. The smaller diameter and flexible structure of those devices made it easier to place them in the trachea. Results of the randomized clinical study performed on 757 patients, indicate that in patients undergoing emergency endotracheal intubation, first-attempt intubation success was higher when there was use of a bougie compared with use of a tracheal tube with stylet (98% vs 87%). In the same study among patients with at least 1 difficult airway characteristic, first-attempt intubation success was also significantly higher in the bougie group (96% vs 82%).[12] In another study, intubation performed by novice physicians during chest compressions was successful only in 10 out of 17 participants without the use of GEB, compared with 16 out of 17 with use of GEB.[13]
Another finding was that even though the difference between intubation success rates in the GEB and FTB group was not statistically significant, participants needed less time to intubate the manikin using a flexible tip bougie. Participants reported that the phosphorous coating of the tip and the ability to bend the tip anteriorly were the reasons why it was easier to place in the trachea than the gum-elastic bougie. In the study by Frass et al higher efficacy and a shorter intubation time were associated with the use of the flexible tip bougie than with the gum-elastic bougie in a difficult airway scenario.[14] Human trials are necessary to determine if this difference has an impact on a patient's outcome.
This study has several limitations worth noting. The use of a manikin may not fully imitate the real condition of the patient. In the GEB and FTB group an assistant, who may not be available in cases of OHCA, was needed to “railroad” the ET tube onto introducers. It is understood that this is the first study comparing flexible tip bougie to other devices during CPR. Future studies should investigate the use of flexible tip bougie on actual patients during cardiopulmonary resuscitation.
5. Conclusions
Within limitations, the findings suggest that intubation introducers facilitate tracheal intubation during continuous chest compressions. Flexible tip bougie decrease the time needed to intubate the patient compared with use of gum-elastic bougie.
Author contributions
Conceptualisation: Michał Bączek.
Formal analysis: Michał Bączek, Michalina Zagańczyk-Bączek.
Investigation: Michał Bączek.
Methodology: Michał Bączek, Michalina Zagańczyk-Bączek.
Project administration: Michał Bączek, Michalina Zagańczyk-Bączek.
Writing – original draft: Michalina Zagańczyk-Bączek.
Writing – review & editing: Michał Bączek.
Michał Marian Bączek orcid: 0000-0002-7652-2759.
Footnotes
Abbreviations: FTB = flexible tip bougie, GEB = gum-elastic bougie, MAC = conventional Macintosh laryngoscope, SD = standard deviation.
How to cite this article: Bączek M, Zagańczyk-Bączek M. Flexible tip bougie - the new introducer for intubation during cardiopulmonary resuscitation: A randomized crossover manikin study. Medicine. 2020;99:1(e18452).
The authors have no conflicts of interest to disclose.
The project is supported under the program of the Minister of Science and Higher Education under the name “Regional Initiative of Excellence” in 2019–2022 project number: 024/RID/2018/19, financing amount: 11.999.000,00 PLN.
References
- [1].Benjamin EJ, Muntner P, Alonso A, et al. Heart disease and stroke statistics—2019 update: a report from the American Heart Association. Circulation 2019;139:e56–28. [DOI] [PubMed] [Google Scholar]
- [2].Ruben H, Johansen S. Gastric inflation due to artificial respiration. Acta Anaesthesiol Scand 1970;14:281–5. [DOI] [PubMed] [Google Scholar]
- [3].Katz SH, Falk JL. Misplaced endotracheal tubes by paramedics in an urban emergency medical services system. Ann Emerg Med 2001;37:32–7. [DOI] [PubMed] [Google Scholar]
- [4].Sayre M, Sakles J, Mistler A, et al. Field trial of endotracheal intubation by basic EMTs. Ann Emerg Med 1998;31:228–33. [PubMed] [Google Scholar]
- [5].Wang HE, Yealy DM. How many attempts are required to accomplish out-of-hospital endotracheal intubation? Acad Emerg Med 2006;13:372–7. [DOI] [PubMed] [Google Scholar]
- [6].Soar J, Nolan J, Böttiger B, et al. European Resuscitation Council guidelines for resuscitation 2015 section 3. adult advanced life support. Resuscitation 2015;95:100–47. [DOI] [PubMed] [Google Scholar]
- [7].Viswanathan S, Campbell C, Wood D. The Eschmann tracheal tube introducer (gum elastic bougie). Anesthesiol Rev 1992;19:29–34. [PubMed] [Google Scholar]
- [8].Kidd J, Dyson A, Latto I. Successful difficult intubation use of the gum elastic bougie. Anaesthesia 1988;43:437–8. [DOI] [PubMed] [Google Scholar]
- [9].Dogra S, Flaconer R, Latto I. Successful difficult intubation: tracheal tube placement over a gum elastic bougie. Anaesthesia 1990;45:774–6. [DOI] [PubMed] [Google Scholar]
- [10].Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia 1984;39:1105–11. [PubMed] [Google Scholar]
- [11].Wang HE, Schmicker RH, Daya MR, et al. Effect of a strategy of initial laryngeal tube insertion vs endotracheal intubation on 72-hour survival in adults with out-of-hospital cardiac arrest: a randomized clinical trial. JAMA 2018;320:769–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Driver B, Prekker M, Klein L, et al. Effect of use of a bougie vs endotracheal tube and stylet on first-attempt intubation success among patients with difficult airways undergoing emergency intubation: a randomized clinical trial. JAMA 2018;319:2179–89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Komasawa N, Cho T, Mihara R, et al. Utility of gum-elastic bougie for tracheal intubation during chest compressions in a manikin: a randomized crossover trial. Am J Emerg Med 2016;34:54–6. [DOI] [PubMed] [Google Scholar]
- [14].Frass M, Smereka J, Ruetzer K, et al. New flexible tip bougie catheter for difficult airway intubation: a randomized, crossover pilot study. Disaster Emerg Med J 2019;4:50–4. [Google Scholar]