

Supplemental Digital Content is available in the text
Keywords: depression status, lifestyle-related disease, mental health and lifestyle survey, polycythemia, traumatic symptoms
Abstract
We have been examining the Comprehensive Health Check of the Fukushima Health Management Survey of residents of 13 municipalities who were forced by the government to evacuate due to the 2011 Great East Japan Earthquake (GEJE). Our findings showed that evacuation is a risk factor for polycythemia and suggested that experiencing an unprecedented disaster and exposure to chronic stress due to evacuation might be a cause of polycythemia.
We analyzed the relationship between the prevalence of polycythemia and the following factors observed in the Mental Health and Lifestyle Survey in an observational study with a cross-sectional design: traumatic symptoms, depression status, socioeconomic factors such as residential environment, and working situation after the GEJE. Target population of the survey included men and women who were at least 15 years of age and who lived in the evacuation zones specified by the government. Participants analyzed consisted of 29,474 persons (12,379 men and 16,888 women) who had participated in both the 2011 Comprehensive Health Check and Mental Health and Lifestyle Survey from June 2011 through March 2012.
The prevalence of polycythemia was not associated with mental states associated with traumatic symptoms (Post-Traumatic Stress Disorder Checklist Scale ≥ 44) and depression status (Kessler 6-item Scale ≥ 13). Furthermore, multivariate analysis showed that there was a tendency for males to develop polycythemia, with characteristics such as being aged 65 years and older, highly educated, obese (body mass index ≥ 25), hypertensive, diabetic, having liver dysfunction, and a smoker being significantly related to the prevalence of polycythemia.
Our findings conclusively demonstrated that polycythemia was not significantly related to psychological factors, but was significantly related to the onset of lifestyle-related disease after the GEJE.
1. Introduction
We previously examined results of the Comprehensive Health Check (CHC) from the Fukushima Health Management Survey (FHMS) of residents of 13 municipalities who were forced by the government to evacuate due to the 2011 Great East Japan Earthquake (GEJE) and the associated accident at the Fukushima Daiichi Nuclear Power Plant.[1,2] Our examinations of the residents demonstrated that evacuation is a risk factor of obesity,[3] hypertension,[4] diabetes mellitus,[5,6] hypo-high-density lipoprotein cholesterolemia,[7] metabolic syndrome,[8] kidney disease,[9] liver dysfunction,[10] and polycythemia.[11] Furthermore, the lifestyle of the evacuees was also shown to be the cause of polycythemia even at 4 years after the GEJE regardless of the presence or absence of being overweight/obesity, smoking, and hypertension.[12]
Therefore, these findings show that experiencing an unprecedented disaster and exposure to chronic stress due to evacuation can be a cause of polycythemia. However, our previous evaluations did not analyze the relationship between the prevalence of polycythemia and traumatic symptoms, depression status, socioeconomic factors such as residential environment, and the working situation after the GEJE. Furthermore, the Mental Health and Lifestyle Survey (MHLS) conducted by the FHMS group showed that psychological distress following the disaster was significantly associated with diet, alcohol intake, sleep satisfaction, and the reduction of physical activity.[13–18]
Subsequently, we then analyzed the relationship between the prevalence of polycythemia and the factors observed during the MHLS.
2. Materials and methods
2.1. Participants
The government designated evacuation zones following the GEJE that occurred on March 11, 2011. Between January and October 2012, the evacuees participated in the FHMS of the Fukushima Daiichi Nuclear Power Plant accident that occurred in 2011. The MHLS, which is part of the previously cited longitudinal study, assesses how the disaster and subsequent lifestyles of the people affected the mental status of the evacuees over a long period of time.
The target population of the survey included men and women who were at least 15 years of age and who lived in the following evacuation zones specified by the government: Hirono, Naraha, Tomioka, Kawauchi, Okuma, Futaba, Namie, Katsurao, Minamisoma, Tamura, Kawamata, Iitate and part of the city of Date. Persons who had a certificate of residence within the evacuation area as of March 11, 2011 were mailed questionnaire on January 18, 2012. Of all the residents living in the area during the disaster, a total of 180,605 were born prior to April 1, 1995 (ie, high-school students or older). Participant response rate was 40.7% (n = 73,569). To guarantee precision when entering the data, data entry experts double-checked all of the entered information. From June 2011 through March 2012, 72,916 persons (32,000 men and 40,916 women) from these communities participated in the MHLS. Participants analyzed consisted of 29,474 persons (12,379 men and 16,888 women) from these groups who had participated in the 2011 CHC.
Participants excluded from the analysis included persons who were aged 91 and older or aged 19 and younger; persons without any peripheral blood: red blood cell count (RBC), hemoglobin (Hb), and hematocrit (Ht) data; persons without any systolic and diastolic blood pressure data (SBP/DBP), body mass index (BMI), and waist circumference data; persons without any information on smoking and drinking history; persons who had not responded to questions on the Kessler 6-item scale (K6) and the Post-Traumatic Stress Disorder Checklist-Scale (PCL-S); to questions on educational background and on evacuation sites; or persons with a history of or current treatment for hematologic disease and those undergoing dialysis due to renal impairment.
2.2. Ethical approval
This study was approved by the Ethics Committee of Fukushima Medical University (# 29064). Informed consent was obtained from community representatives who were conducting an epidemiological study based on the guidelines of the Council for International Organizations of Medical Science. All participants in the FHMS provided written informed consent.
2.3. Definitions and data collection
Height and weight were measured (without shoes and in light clothing), with BMI then calculated as weight (kg)/height2 (m2). Obesity was defined as a BMI ≥ 25 kg/m2. Trained technicians took all of the SBP/DBP measurements. Hypertension was defined as SBP ≥ 140 mm Hg, DBP ≥ 90 mm Hg, or the use of antihypertensive agents.
Laboratory data collected included aspartate aminotransferase (U/L); alanine aminotransferase (U/L); gamma-glutamyltransferase (U/L); high-density lipoprotein cholesterol (mg/dL); low-density lipoprotein cholesterol (mg/dL); triglycerides (mg/dL); fasting plasma glucose (mg/dL); hemoglobin A1c (% of total hemoglobin); and peripheral blood count, which included the RBC, Ht, Hb, platelet count, and white blood cell count with subpopulations of white cells.
We defined hepatobiliary enzyme abnormality based on the definition of the Ministry of Health, Labour, and Welfare for the medical examination judgment value, using the following criteria: aspartate aminotransferase ≥ 31 U/L, alanine aminotransferase ≥ 31 U/L, or gamma-glutamyltransferase ≥51 U/L.[19] Diabetes and dyslipidemia were defined based on a previous report.[10] Participants were divided into 3 groups based on alcohol consumption, based on a previous report.[10]
The quantitative definition of polycythemia is known to differ between research institutes and laboratories. However, the standard values defined for the peripheral blood in the CHC are as follows: RBC, 400 to 579 × 104/μL; Hb, 13.1 to 17.9 g/dL; and Ht, 38.0% to 54.9% in men; RBC, 370 to 549 × 104/μL; Hb, 12.1 to 15.9 g/dL; and Ht, 33.0% to 47.9% in women. Polycythemia was diagnosed if one of these items was greater than the standard value.
Smoking status of the participants was classified as current smokers or current nonsmokers just before the disaster.
In the MHLS, the Japanese versions of the K6[20] and PCL-S[21] were used to assess the participants’ mental health status. The K6 consists of 6 brief questions regarding depression and anxiety symptoms during the past 30 days, with the overall score ranging from 0 to 24. Psychological distress was defined as a K6 score of 13 or higher.[22] The PCL-S is used to evaluate symptoms of post-traumatic stress disorder during the past 30 days. The PCL-S consists of 17 items with the overall score ranging from 17 to 85. Participants were classified as having probable post-traumatic stress disorder if their overall PCL-S score was 44 or higher.[21] In addition to the K6 and PCL-S surveys, the questionnaires also asked about medical history and various lifestyle factors, such as physical activity, living environment, sleeping conditions, cigarette smoking, alcohol intake, living in evacuation area, and job status.
2.4. Statistical analysis
A chi-square test was used to examine disaster-related socioeconomic variables, obesity, hypertension, liver dysfunction, smoking, and heavy drinking between the categories used to determine the prevalence of polycythemia after the disaster.
We also examined the association between the demographic, disaster-related, and psychosocial variables in participants with an onset of polycythemia after the disaster.
Age- and sex-adjusted prevalence ratios and 95% confidence intervals for the changes in the smoking status for demographic, disaster-related and psychosocial variables were calculated using a univariate regression analysis.
In the multivariable-adjusted model, adjustments were made for age (years), sex, and other associated factors that were estimated to be statistically significant by the age- and sex-adjusted model. The factors found to be potentially associated included educational attainment, living arrangement, living in an evacuation area, experiencing a tsunami, experiencing a nuclear power plant accident, bereavement, obesity, hypertension, diabetes, liver dysfunction, smoking, and heavy drinking. The odds ratios between participant characteristics and the prevalence of polycythemia were calculated using logistic regression analysis. All tests were two-tailed, and P < .05 was considered to indicate statistical significance. All statistical analyses were performed in 2018 using the software package SAS version 9.4 (SAS Institute, Inc., Cary, NC).
3. Results
3.1. Relationship between participant characteristics and the prevalence of polycythemia
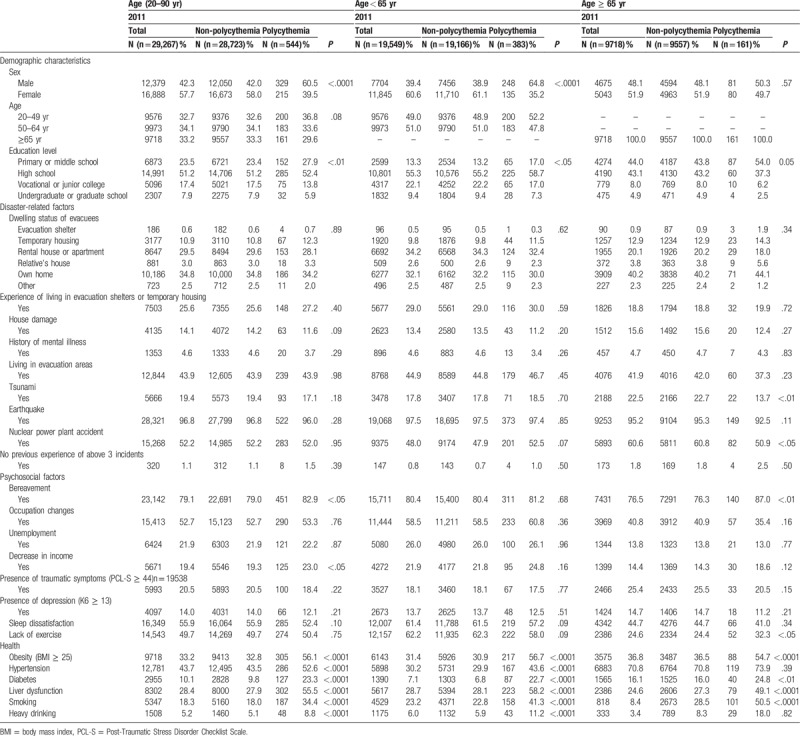
The prevalence of polycythemia was compared with participant characteristics by examining the frequency of polycythemia in individuals under and over the age of 65, since 65 is the general retirement age in Japan and the lifestyle changes greatly at that age. Participant characteristics are shown in Table 1. The demographic characteristics examined included gender, age (20–49, 50–64, 65–90 years), and education level. Disaster-related factors examined included dwelling status of the evacuees; actual experience of living in evacuation shelters or temporary housing; existence of home damage; history of mental illness; experience related to living in evacuation areas, tsunami, earthquake, and of nuclear power plant accident. Psychosocial factors evaluated included bereavement, occupation changes, unemployment, decrease in income, presence of traumatic symptoms (PCL-S ≥ 44), presence of depression (K6 ≥ 13), sleep dissatisfaction, and lack of exercise. The health checkups examined included obesity (BMI ≥ 25), hypertension, diabetes, liver dysfunction, smoking, and heavy drinking. The government evacuated residents from 13 municipalities, with complete evacuations to evacuation shelters or temporary housing occurring in Iitate, Katsurao, Okuma, Tomioka, Futaba, Namie, Hirono, Naraha, and Kawauchi. However, only partial evacuations occurred in Minamisoma, Kawamata, Tamura, and Date. By gender, polycythemia was significantly more common among men, but there was no significant difference at the age of 65 and older. Differences in the prevalence of polycythemia due to educational background were significant under the age of 65, and the incidence was low in individuals with a high education. The relationship between experiencing a tsunami or nuclear power plant accident and the prevalence of polycythemia was not significant at all ages, but was significant at the age of 65 and older. On the other hand, the relationship between bereavement experience and decrease in income was significantly related to the prevalence of polycythemia significantly at all ages, especially the former at the age of 65 and older. The presence of traumatic symptoms (PCL ≥ 44) and the presence of depression (K6 ≥ 13) were not significantly related to the prevalence of polycythemia significantly. In health checkups, all items were significantly related to the prevalence of polycythemia, which were prominent under the age of 65. The lack of exercise was significantly related to the prevalence of polycythemia at the age of 65 and older.
Table 1.
Basic characteristics of participants and prevalence of polycythemia.
The Supplementary Table 1, presents the results of the univariate regression analysis that was conducted on the factors that showed a significant relationship (P < .05) with the prevalence of polycythemia or on the factors that tended to be related with polycythemia after adjusting for age and sex. The age range of 20 to 49 years was the reference for age, and living in one's own home was the reference for the dwelling status of evacuees.
3.2. Multivariate analysis of the relationship between characteristics of the participants and the prevalence of polycythemia
Subsequently, we performed a multivariate analysis on the characteristic factors in the Supplementary Table 1, that exhibited a significant relationship (P < .05) with the prevalence of polycythemia along with the factors that tended to be related with the polycythemia (Table 2). Factors such as the dwelling status of evacuees and the experience of living in an evacuation shelters or temporary housing were excluded because they were not significantly related to the prevalence of polycythemia in the Supplementary Table 1. Interestingly, except for a lack of exercise among psychosocial factors, there was no significant relationship with the prevalence of polycythemia.
Table 2.
Multivariate analysis of relationships between characteristics of participants and the prevalence of polycythemia after the adjustment.
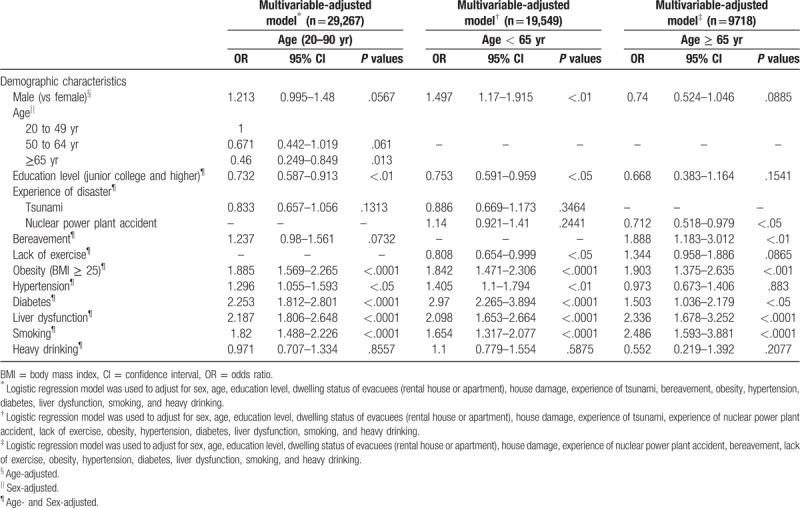
In the participants that ranged in age from 20 to 90 years old, characteristics such as age of 65 years and older, highly educated, obesity (BMI ≥ 25), hypertension, diabetes, liver dysfunction, and smoking were shown to be significantly related to the prevalence of polycythemia, while characteristics such as male, age of 50 years and older (50–64 years old), and in bereavement tended to be related to the polycythemia (P < .1). Because people over 65 years old are considered to experience a large social and economic changes due to retirement in Japan, a separate analysis further examined the participants after categorizing them into groups of under and over the age of 65 years. In the former, characteristics such as male, highly educated, lack of exercise, obesity (BMI ≥ 25), hypertension, diabetes, liver dysfunction, and smoking were all significantly related to the prevalence of polycythemia (P < .05). In the latter group, characteristics such as experiencing a nuclear power plant accident, bereavement, obesity (BMI ≥ 25), diabetes, liver dysfunction, and smoking were significantly related to the prevalence of polycythemia (P < .05), with characteristics such as male and a lack of exercise tending to be related to the polycythemia (P < .1).
Therefore, our results did not indicate a significant relationship between the prevalence of polycythemia and traumatic symptoms (PCL-S), depression status (K6), or socioeconomic factors (such as residential environment and working situation) after the GEJE.
4. Discussion
There are no international diagnostic criteria for polycythemia; therefore, in the present study, we determined that polycythemia was present if one of RBC, Hb, and Ht was greater than the standard value. Furthermore, since polycythemia may be confused with erythrocytosis, we defined polycythemia based on our previous reports.[11,12]
In contrast to our previous reports,[11,12] the participants analyzed in our present study were residents who were evaluated by PCL-S and K6[13] after the initial MHLS of the FHMS. Furthermore, the residents analyzed in the previous 2 reports lived in 13 municipalities that were government-designated evacuation areas. However, this study focused on evacuees who specifically experienced living in an evacuation shelter or temporary housing.
Our findings revealed that the prevalence of polycythemia increased in the residents of these areas after the GEJE, but there were no data on the erythropoietin levels in the sera or on an increase in RBC that was accompanied by an increase in white blood cell count and platelets. Therefore, this polycythemia was presumed to be primarily relative polycythemia. In general, relative polycythemia[23] is treated synonymously with stress polycythemia.[24] However, the mechanism of onset for polycythemia induced by stress is unclear, with a decrease in the circulating plasma volume considered to potentially be the cause.[25] Although previous studies that analyzed the Ht value in the acute phase reported increased Ht level after a speech or calculation test,[26,27] a reliable indicator that can be used to analyze the effects of chronic stress has yet to be established.
We hypothesized that mental stress and life style changes due to evacuation would lead to an increase in the onset of polycythemia because smoking and drinking alcohol,[28–30] hypertension,[31] or lifestyle-related diseases such as obesity, hyperlipidemia, and hyperglycemia[32] have all been reported to be causes of polycythemia. Contrary to our expectations, there was no significant relationship between psychosocial factors and the onset of polycythemia, but there was a significant relationship between obesity, smoking, or hypertension and the onset of polycythemia as reported in the above studies.
In addition, it should be noted that high serum renin levels have been shown to lead to a decrease in the circulating plasma flow and an increase in the Ht level in patients with hypertension, with a decrease in the serum renin level after treatment with antihypertensive agents subsequently leading to an increase in the circulating plasma flow and a decrease in the Ht level.[31] Therefore, Ht is an indicator of the control of hypertension. A further study[32] examined primarily male participants after separating them into 3 Ht groups (I: low, II: intermediate, III: high). Study results showed that the levels of glucose, insulin, TG, and cholesterol in the serum were significantly higher in group III, with the participants in this group consisting of a larger proportion of persons that were overweight. Therefore, polycythemia, especially high Ht, is suggested to be associated with diabetes. In any case, polycythemia is considered to be an index of lifestyle-related disease.
In a large complex disaster such as the GEJE, anxiety about radiation exposure added to the mental health burden of evacuees. Furthermore, it is unclear whether the increase in lifestyle-related diseases would be common throughout the world after such a complex disaster. We suggest that socioeconomic support, including financial compensation, would affect the onset of these diseases.
There are several potential limitations for this study that warrant consideration. First, both the response rate to the MHLS and the examination rate of the CHC were low, with the proportion of residents with data for both surveys even lower. Therefore, those factors might have resulted in an underestimate of the prevalence of polycythemia and have lowered the reliability of the prevalence of polycythemia and the results of PCL-S and K6 in the MHLS. Second, the MHLS and the CHC were not conducted at the same time. Since the former was conducted 10 months after the GEJE, it cannot be used for the analysis of mental state in the acute phase after the GEJE. Therefore, potential recall bias in these surveys cannot be ruled out. Third, the relationship between mental state and the presence or absence of polycythemia was only analyzed in 2011, and furthermore it was not observed consecutively.
5. Conclusion
We found no significant correlation between the prevalence of polycythemia and the results of PCL-S and K6 in the MHLS. However, we did find significant correlations between the factors in the lifestyle survey such as obesity, hypertension, diabetes, liver dysfunction, smoking, excessive alcohol consumption, and the prevalence of polycythemia. These results suggest that lifestyle-related diseases are involved in the onset of polycythemia, similar to findings reported by Smith et al.[32] In fact, other studies have also reported that an increase in the Ht level is a predictor of the onset of acute and long-term cardiovascular disease.[33–36] It has already been 10 years since the GEJE, and residents in the evacuated areas are expected to have experienced an increase in lifestyle-related disease by now. Therefore, it is necessary to make efforts to promote health and health checkups.
Acknowledgments
We thank staff of the FHMS for their cooperation.
Author contributions
AS, HN and TO designed the study and contributed to writing the manuscript. HN, TO, MM and KO collected the data and performed the statistical analysis. AT, YK, HS, AO, MS, JK, SH, MH, and SY contributed to planning the health screening program. HY, HO, and KK contributed to the scientific review. All authors read and approved the final manuscript.
Conceptualization: Akira Sakai, Tetsuya Ohira.
Data curation: Akira Sakai, Hironori Nakano, Tetsuya Ohira, Masaharu Maeda, Hirooki Yabe.
Formal analysis: Akira Sakai, Hironori Nakano, Tetsuya Ohira, Masaharu Maeda, Kanako Okazaki, Hirooki Yabe.
Investigation: Akira Sakai.
Project administration: Akira Sakai, Hironori Nakano, Tetsuya Ohira, Masaharu Maeda, Kanako Okazaki, Atsushi Takahashi, Yukihiko Kawasaki, Hiroaki Satoh, Akira Ohtsuru, Michio Shimabukuro, Junichiro Kazama, Shigeatsu Hashimoto, Mitsuaki Hosoya, Seiji Yasumura, Hitoshi Ohto, Kenji Kamiya.
Supplementary Material
Footnotes
Abbreviations: BMI = body mass index, CHC = comprehensive health check, FHMS = Fukushima Health Management Survey, GEJE = Great East Japan Earthquake, Hb = hemoglobin, Ht = hematocrit, K6 = Kessler 6-item Scale, MHLS = Mental Health and Lifestyle Survey, PCL-S = Post-Traumatic Stress Disorder Checklist Scale, RBC = red blood cell count.
How to cite this article: Sakai A, Nakano H, Ohira T, Maeda M, Okazaki K, Takahashi A, Kawasaki Y, Satoh H, Ohtsuru A, Shimabukuro M, Kazama J, Hashimoto S, Hosoya M, Yasumura S, Yabe H, Ohto H, Kamiya K. Relationship between the prevalence of polycythemia and factors observed in the mental health and lifestyle survey after the Great East Japan Earthquake. Medicine. 2020;99:1(e18486).
Funding: This survey was supported by the National Health Fund for Children and Adults Affected by the Nuclear Incident.
The authors have no financial and conflicts of interest to disclose.
The findings and conclusions of this article are solely the responsibility of the authors and do not represent the official views of the Fukushima Prefecture government.
Supplemental Digital Content is available for this article.
References
- [1].Yasumura S, Hosoya M, Yamashita S, et al. Study protocol for the Fukushima Health Management Survey. J Epidemiol 2012;22:375–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Kawasaki Y, Hosoya M, Yasumura S, et al. The basic data for residents aged 16 years or older who received a comprehensive health check examinations in 2011-2012 as a part of the Fukushima Health Management Survey after the Great East Japan Earthquake. Fukushima J Med Sci 2014;60:159–69. [DOI] [PubMed] [Google Scholar]
- [3].Ohira T, Hosoya M, Yasumura S, et al. Effect of evacuation on body weight after the Great East Japan Earthquake. Am J Prev Med 2016;50:553–60. [DOI] [PubMed] [Google Scholar]
- [4].Ohira T, Hosoya M, Yasumura S, et al. Evacuation and risk of hypertension after the Great East Japan Earthquake: the Fukushima Health Management Survey. Hypertension 2016;68:558–64. [DOI] [PubMed] [Google Scholar]
- [5].Satoh H, Ohira T, Hosoya M, et al. Evacuation after the Fukushima Daiichi Nuclear Power Plant accident is a cause of diabetes: results from the Fukushima Health Management Survey. J Diabetes Res 2015;2015:627390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Satoh H, Ohira T, Nagai M, et al. Evacuation is a risk factor for diabetes development among evacuees of the Great East Japan earthquake: a 4-year follow-up of the Fukushima Health Management Survey. Diabates Metab 2019;45:312–5. [DOI] [PubMed] [Google Scholar]
- [7].Satoh H, Ohira T, Nagai M, et al. Hypo-high-density lipoprotein cholesterolemia is caused by evacuation after the Fukushima Daiichi Nuclear Power Plant accident: results from the Fukushima Health Management Survey. Intern Med 2016;55:1967–76. [DOI] [PubMed] [Google Scholar]
- [8].Hashimoto S, Nagai M, Ohira T, et al. Influence of post-disaster evacuation on incidence of metabolic syndrome: the Fukushima Health Management Survey. J Atheroscler Thromb 2017;24:327–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Hayashi Y, Nagai M, Ohira T, et al. The impact of evacuation on the incidence of chronic kidney disease after the Great East Japan Earthquake: the Fukushima Health Management Survey. Clin Exp Nephrol 2017;21:995–1002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Takahashi A, Ohira T, Yasumura S, et al. Effect of evacuation on liver function after the Fukushima Daiichi Nuclear Power Plant accident. J Epidemiol 2017;27:180–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Sakai A, Ohira T, Hosoya M, et al. Life as an evacuee after the Fukushima Daiichi Nuclear Power Plant accident is a cause of polycythemia: the Fukushima Health Management Survey. BMC Public Health 2014;14:1318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Sakai A, Nakano H, Ohira T, et al. Persistent prevalence of polycythemia among evacuees 4 years after the Great East Japan Earthquake: a follow-up study. Prev Med Rep 2017;5:251–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Yabe H, Suzuki Y, Mashiko H, et al. Psychological distress after the Great East Japan Earthquake and Fukushima Daiichi Nuclear Power Plant accident: results of a mental health and lifestyle survey through the Fukushima Health Management Survey in FY2011 and FY2012. Fukushima J Med Sci 2014;60:57–67. [DOI] [PubMed] [Google Scholar]
- [14].Kunii Y, Suzuki Y, Shiga T, et al. Severe psychological distress of evacuees in evacuation zone caused by the Fukushima Daiichi Nuclear Power Plant accident: the Fukushima Health Management Survey. PLoS One 2016;11:e0158821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Ueda Y, Yabe H, Maeda M, et al. Drinking behavior and mental illness among evacuees in Fukushima following the Great East Japan Earthquake: the Fukushima Health Management Survey. Alcohol Clin Exp Res 2016;40:623–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Uemura M, Ohira T, Yasumura S, et al. Association between psychological distress and dietary intake among evacuees after the Great East Japan Earthquake in a cross-sectional study: the Fukushima Health Management Survey. BMJ Open 2016;6:e011534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Iwasa H, Suzuki Y, Shiga T, et al. Psychometric evaluation of the Japanese version of the posttraumatic stress disorder checklist in community dwellers following the Fukushima Daiichi Nuclear Power Plant incident: the Fukushima Health Management Survey. SAGE Open 2016;6:1–1. [Google Scholar]
- [18].Yabuki S, Ouchi K, Kikuchi S, et al. Pain, quality of life and activity in aged evacuees living in temporary housing after the Great East Japan earthquake of 11 March 2011: a cross-sectional study in Minamisoma City, Fukushima prefecture. BMC Musculoskelet Disord 2015;16:246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Ministry of Health, Labour and Welfare. Medical examination judgment value. Available at: www.mhlw.go.jp/bunya/kenkou/seikatsu/pdf/ikk-a05.pdf [In Japanese]. Accessed May 10, 2017. [Google Scholar]
- [20].Furukawa TA, Kawakami N, Saitoh M, et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int J Methods Psychiatr Res 2008;17:152–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Blanchard EB, Jones-Alexander J, Buckley TC, et al. Psychometric properties of the PTSD Checklist (PCL). Behav Res Ther 1996;34:669–73. [DOI] [PubMed] [Google Scholar]
- [22].Kessler RC, Barker PR, Colpe LJ, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry 2003;60:184–9. [DOI] [PubMed] [Google Scholar]
- [23].Lawrence JH, Berlin NI. Relative polycythemia; the polycythemia of stress. Yale J Biol Med 1952;24:498–505. [PMC free article] [PubMed] [Google Scholar]
- [24].Dameshek W. Stress erythrocytosis. Blood 1953;8:282–4. [PubMed] [Google Scholar]
- [25].Isbister JP. The contracted plasma volume syndromes (relative polycythaemias) and their haemorheological significance. Baillieres Clin Haematol 1987;1:665–93. [DOI] [PubMed] [Google Scholar]
- [26].Patterson SM, Marsland AL, Manuck SB, et al. Acute hemoconcentration during psychological stress: assessment of hemorheologic factors. Int J Behav Med 1998;5:204–12. [DOI] [PubMed] [Google Scholar]
- [27].de Boer D, Ring C, Wood M, et al. Time course and mechanisms of mental stress-induced changes and their recovery: hematocrit, colloid osmotic pressure, whole blood viscosity, coagulation times, and hemodynamic activity. Psychophysiology 2007;44:639–49. [DOI] [PubMed] [Google Scholar]
- [28].Smith JR, Landaw SA. Smokers’ polycythemia. N Engl J Med 1978;298:6–10. [DOI] [PubMed] [Google Scholar]
- [29].Moore-Gillon J, Pearson TC. Smoking, drinking, and polycythaemia. Br Med J (Clin Res Ed) 1986;292:1617–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Moore-Gillon J. Smoking–a major cause of polycythemia. J R Soc Med 1988;81:431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Chrysant SG, Frohlich ED, Adamopoulos PN, et al. Pathophysiologic significance of “stress” or relative polycythemia in essential hypertension. Am J Cardiol 1976;37:1069–72. [DOI] [PubMed] [Google Scholar]
- [32].Smith S, Julius S, Jamerson K, et al. Hematocrit levels and physiologic factors in relationship to cardiovascular risk in Tecumseh, Michigan. J Hypertens 1994;12:455–62. [PubMed] [Google Scholar]
- [33].Kario K, Matsuo T. Increased incidence of cardiovascular attacks in the epicenter just after the Hanshin-Awaji earthquake. Thromb Haemost 1995;74:1207. [PubMed] [Google Scholar]
- [34].Biswas M, Prakash PK, Cossburn M, et al. Life-threatening thrombotic complications of relative polycythaemia. J Intern Med 2003;253:481–3. [DOI] [PubMed] [Google Scholar]
- [35].Allport LE, Parsons MW, Butcher KS, et al. Elevated hematocrit is associated with reduced reperfusion and tissue survival in acute stroke. Neurology 2005;65:1382–7. [DOI] [PubMed] [Google Scholar]
- [36].Pizzi C, De Stavola BL, Meade TW. Long-term association of routine blood count (Coulter) variables on fatal coronary heart disease: 30-year results from the first prospective Northwick Park Heart Study (NPHS-I). Int J Epidemiol 2010;39:256–65. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.