

Abstract
Background and Objectives:
Pleomorphic adenoma, being the most common benign tumors of salivary gland, is morphologically characterized by a biphasic pattern containing the epithelial and mesenchymal components. The modified myoepithelial cells present are thought to play an important role in its histologic diversity by the formation of extracellular matrix. The aim of the present study was to observe, compare and correlate the histomorphological diversity of epithelial and stromal components along with different morphological cell types of modified myoepithelial cells.
Materials and Method:
Histomorphological features were compared in twenty cases of pleomorphic adenoma of major salivary glands and twenty cases of minor salivary glands using hematoxylin and eosin stains. The features were analyzed by observing under the light microscope.
Results:
Statistical analysis showed significance of plasmacytoid cells, and squamous metaplasia was extensive with formation of keratin cyst-like structure resembling cystic pleomorphic adenoma, in minor salivary gland tumors.
Conclusion:
Plasmacytoid cells, squamous cells and areas of hyalinization were observed predominantly in major salivary gland tumors compared to minor salivary glands. Keratin pearls were predominant in minor salivary gland tumors.
Keywords: Histopathology, keratin pearls, major salivary glands, minor salivary glands, pleomorphic adenoma
INTRODUCTION
Among human neoplasias, salivary gland tumors are probably the most complex due to their broad histological spectrum resulting from a multiple tumor cell differentiation, cellular arrangements and extracellular matrix synthesis produced by certain tumor cells. Concerning head-and-neck regions, the tumors of the salivary glands correspond to 3%, the majority of which are epithelial origin presenting varied etiology and several risk factors that have been identified so far. Pleomorphic adenoma is the most common salivary gland tumor, accounting nearly 50% of all neoplasms occurring at the head-and-neck region.[1,2] The term pleomorphic adenoma suggested by “WILLIS” characterizes closely the unusual histologic pattern of the lesion.[3] It derives its name from the architectural pleomorphism seen by light microscopy.[4] Very few studies have been done on histomorphological findings of pleomorphic adenoma of salivary glands. Hence, the present study is planned to find the comparative study of histomorphological findings in the major and minor salivary glands to know the occurrence, diagnosis and treatment plan of the condition.
MATERIALS AND METHOD
The materials for the study comprised a total of forty biopsy specimens from the Department of Oral Pathology and Microbiology, Sri Rajiv Gandhi College of Dental Sciences and Hospital, Bengaluru. The material retrieved was comprised twenty cases each of pleomorphic adenoma of major and minor salivary glands that include both parotid and submandibular glands which were obtained by surgical excision biopsy of tumor. The obtained biopsy specimens were fixed in 10% formalin, and routine tissue processing was done. The tissues were sectioned of 5-μ thickness from the tissue blocks obtained by paraffin-embedded technique. The tissue sections were stained with hematoxylin and eosin stain and then observed under light microscope of power: ×4, ×10 and ×40 each. 3–5 sections were studied from different areas according to the size of the lesion.
RESULTS
The study included a total of forty cases which were divided into pleomorphic adenoma of major and minor salivary glands. The hematoxylin and eosin-stained sections were observed for epithelial and stromal components to compare and evaluate the histopathologic variations/differences. The statistical analysis was considered under which the results were averaged (mean ± standard deviation) for continuous data and are presented in tables. One-way analysis of variance was used to test the difference between groups. Data analysis was carried out using the Statistical Package for the Social Sciences (SPSS) version 10.5. IBM Chicago, Illinois state, USA.
The morphological patterns, cellular components, stromal components and capsular alterations were considered. Morphological patterns are of trabecular, ductal, cystic and solid patterns. Among morphological patterns, ductal and solid patterns were observed 100% in both major and minor salivary glands pleomorphic adenoma and among cellular components; the percentage of plasmacytoid cells and squamous cells was more in major salivary gland in comparison to minor salivary gland pleomorphic adenoma. The areas of hyalinization were predominantly noted in major salivary gland, whereas keratin pearls were more in minor salivary glands pleomorphic adenoma. Osteoid areas were absent in both major and minor salivary glands pleomorphic adenoma, with myxoid and chondroid areas seen equally in both major and minor salivary glands pleomorphic adenoma. Few areas of hyalinization and keratin pearls were also observed in both the types. Major salivary gland pleomorphic adenoma was encapsulated, with the absence of satellite nodules. Minor salivary glands were partially encapsulated [Table 1].
Table 1.
Representing morphological patterns, cellular components, stromal components and capsular alterations, presented in forty cases of pleomorphic adenoma between major and minor salivary glands
| Site | Pattern | Cellular components observed | Stromal components | Capsular alterations | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Trabecular | Ductal | Cystic | Solid | Plasmacytoid cells | Spindle cells | Squamous cells | Basaloid cells | Cuboidal cells | Myxoid | Areas of hyalinization | Chondroid | Osteoid areas | Keratin pearls | Capsule present | Partial encapsulation | Satellite nodules | |
| Major salivary glands (n=20) | 0 | 20 (100) | 0 | 20 (100) | 15 (75) | 19 (95) | 9 (45) | 18 (90) | 20 (100) | 20 (100) | 15 (75) | 19 (95) | 0 | 4 (20) | 20 (100) | 0 | 0 |
| Minor salivary glands (n=20) | 1 (5) | 20 (100) | 0 | 20 (100) | 6 (30) | 20 (100) | 7 (35) | 20 (100) | 20 (100) | 20 (100) | 6 (30) | 19 (95) | 0 | 7 (35) | 0 | 20 (100) | 0 |
Using one-way ANOVA test, there is no difference in the trabecular pattern between pleomorphic adenoma of major and minor salivary glands, and that there was statistical difference (P < 0.004) in mean number of plasmacytoid cells, thus showing the significance [Table 2].
Table 2.
Comparison between trabecular pattern and cells of epithelial component present in pleomorphic adenoma of major and minor salivary glands
| Cellular components | Sites | n | Mean | SD | SE | F | Significance (P) |
|---|---|---|---|---|---|---|---|
| Plasmacytoid cells | Major salivary glands | 20 | 0.75 | 0.444 | 0.099 | 9.679 | 0.004* |
| Minor salivary glands | 20 | 0.30 | 0.470 | 0.105 | |||
| Total | 40 | 0.53 | 0.506 | 0.080 | |||
| Spindle cells | Major salivary glands | 20 | 0.95 | 0.224 | 0.050 | 1.000 | 0.324 |
| Minor salivary glands | 20 | 1.00 | 0.000 | 0.000 | |||
| Total | 40 | 0.98 | 0.158 | 0.025 | |||
| Squamous cells | Major salivary glands | 20 | 0.45 | 0.510 | 0.114 | 0.400 | 0.531 |
| Minor salivary glands | 20 | 0.35 | 0.489 | 0.109 | |||
| Total | 40 | 0.40 | 0.496 | 0.078 | |||
| Basaloid cells | Major salivary glands | 20 | 0.90 | 0.308 | 0.069 | 2.111 | 0.154 |
| Minor salivary glands | 20 | 1.00 | 0.000 | 0.000 | |||
| Total | 40 | 0.95 | 0.221 | 0.035 | |||
| Cuboidal cells, clear cells, oncocytoid cells, mucous cells, serous cells, sebaceous cells | Major salivary glands | 20 | 1.00 | 0.000 | 0.000 | - | - |
| Minor salivary glands | 20 | 1.00 | 0.000 | 0.000 | |||
| Total | 40 | 1.00 | 0.000 | 0.000 | |||
| Trabecular pattern | Major salivary glands | 20 | 0.00 | 0.000 | 0.000 | 1.000 | 0.324 |
| Minor salivary glands | 20 | 0.05 | 0.224 | 0.050 | |||
| Total | 40 | 0.03 | 0.158 | 0.025 |
ANOVA test *P<0.05=Significance. SD: Standard deviation, SE: Standard error
When the morphological patterns, cells of epithelial component, stromal components and capsular alterations of pleomorphic adenoma were compared between parotid, submandibular and minor salivary glands, ductal and solid patterns are seen in the parotid, submandibular and minor salivary glands pleomorphic adenoma with an exception of trabecular pattern that is seen in minor salivary gland pleomorphic adenoma. Pleomorphic adenoma of parotid gland showed 100% of cuboidal cells; submandibular gland showed 100% of plasmacytoid cells, spindle cells, basaloid cells and cuboidal cells, respectively. Minor salivary gland pleomorphic adenoma showed 100% of spindle cells, basaloid cells and cuboidal cells. Parotid gland and minor salivary glands pleomorphic adenoma showed 100% of myxoid areas, whereas submandibular gland showed 100% of myxoid, chondroid and hyalinized areas.
All the glands showed the presence of capsule and absence of satellite nodules. Major salivary glands pleomorphic adenoma is encapsulated, and minor salivary glands pleomorphic adenoma is partially encapsulated [Table 3].
Table 3.
Morphological patterns, cells of epithelial component, stromal components and capsular alterations of pleomorphic adenoma present in parotid, submandibular and minor salivary glands
| Site | Present, n (%) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pattern | Cellular components observed | Stromal components | Capsular alterations | ||||||||||||||
| Trabecular | Ductal | Cystic | Solid | Plasmacytoid cells | Spindle cells | Squamous cells | Basaloid cells | Cuboidal cells | Myxoid | Areas of hyalinization | Chondroid | Osteoid areas | Keratin pearls | Capsule present | Partial encapsulation | Satellite nodules | |
| Parotid (n=17) | 0 | 17 (100) | 0 | 17 (100) | 12 (70) | 16 (94.1) | 8 (47) | 15 (88.2) | 17 (100) | 17 (10 | 12 (70.5) | 16 (94.1) | 0 | 4 (20) | 17 (100) | 0 | 0 |
| Sub mandibular (n=3) | 0 | 3 (100) | 0 | 3 (100) | 3 (100) | 3 (100) | 1 (33.3) | 3 (100) | 3 (100) | 3 (100) | 3 (100) | 3 (100) | 0 | 0 | 3 (100) | 0 | 0 |
| Minor salivary glands (n=20) | 1 (5) | 20 (100) | 0 | 20 (100) | 6 (30) | 20 (100) | 7 (35) | 20 (100) | 20 (100) | 20 (100) | 6 (30) | 19 (95) | 0 | 7 (35) | 0 | 20 (100) | 0 |
DISCUSSION
Several attempts were made to know the clinical and histomorphological changes in pleomorphic adenoma of major and minor salivary glands. The present study was focused on the comparison of histomorphological features between major and minor salivary glands.[5] Broadly, salivary gland is categorized into major and minor which are distributed over the upper aerodigestive tract, of which the salivary gland tumor arises in the parotid gland is 80%–91%, 5%–22% in minor salivary glands and only 4%–8% is in the submandibular gland[6] which is consistent with the study.
Pleomorphic adenoma occurs at all ages, even occasionally in the newborn. Frazell et al. in 1954 reported instances in a young age of 7-year-old patient and an 82-year-old patient. However, the commonly affected age groups are the fifth and sixth decades; 60% of them are women.[7] It is relatively rare in children and the majority of cases occur in major salivary gland, especially parotid; it is rare in minor salivary glands and if it occurs, involves palatal gland.[8] In this study, the patients aged between 41 and 50 years are affected more comprising around 40% of cases, followed by 31–40 years (35%), 21–30 years (15%), 51–60 years (7.5%) and 61–70 years (2.5%), respectively. No cases involving the children were reported in this study [Table 4].
Table 4.
Gender- and age-wise distribution of forty pleomorphic adenoma cases between major and minor salivary glands
| Site | Gender | Age (years) | Total | |||||
|---|---|---|---|---|---|---|---|---|
| Male, (%) | Female, (%) | 21-30 | 31-40 | 41-50 | 51-60 | 61-70 | ||
| Major salivary glands | 11 (55) | 09 (45) | 3 | 5 | 9 | 1 | 0 | 20 |
| Minor salivary glands | 13 (65) | 07 (35) | 3 | 7 | 7 | 2 | 1 | 20 |
Pleomorphic adenoma has a female predilection with female:male ratio of 4.4:1,[9] and recent literature shows around 2:1 ratio.[10] In a recent study among Jordian patients, of the 62 cases, 32 (51.6%) occurred in men, with a male-to-female ratio of 1.06:1.[11] In the present study, it shows male predilection in both major and minor salivary glands of 40 cases in total, with 55% of cases occurring in males and 45% of cases in females in major salivary glands. In minor salivary glands, it is 65% of cases males and 35% females, respectively [Table 4].
Clinical presentation
In the present study, the tumor clinical presentations were consistent with the literature.[12] The major salivary glands and minor salivary glands were small in size and gradually increased in size at the time of reporting. The major salivary gland tumor mass was mobile, asymptomatic, firm and was not attached to the overlying mucosa, but minor salivary gland tumor was seen present in the palate with firmly attached to the underlying mucosa with no surface ulceration, as there was no history of trauma in all the cases. The growth size of all minor salivary glands was not >3 cm in size; except with one case, around 5 cm in size.[4,12]
Gross pathology
On gross examination, the present study revealed both minor and major salivary glands round to ovoid, well-circumscribed masses with soft to firm in consistency and grayish-white to tan in color.[13] Majority of major salivary glands showed bosselated surfaces with multiple surface nodules in one case of the submandibular gland. Few cases of minor salivary glands showed bosselated surface and predominantly showed smooth surfaces. Most of the masses were encapsulated and few were partially encapsulated.[14,15,16] One case involving submandibular gland showed multiple nodules, but the recurrence rate was not noted, as follow-up of the case was not done. Recurrent pleomorphic adenoma has the tendency for multiple recurrences, when the tumor is predominantly multinodular; however, according to few studies, its biological behavior and histomorphological features contribute to the recurrence nature.[16,17]
Histomorphological features
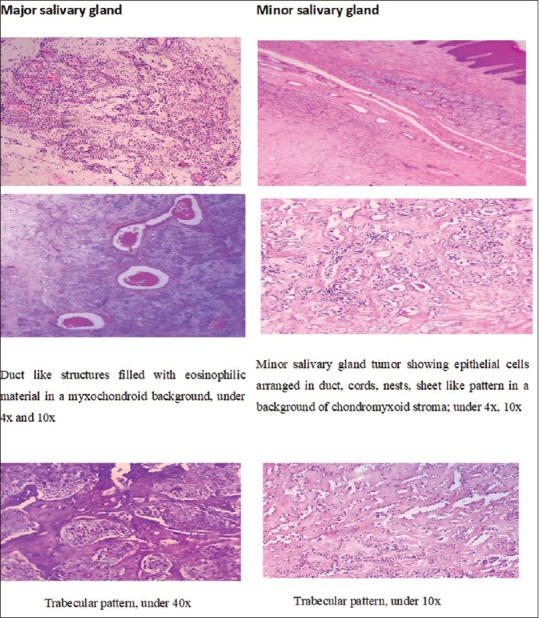
The study shows predominant ductal and solid structures. Trabecular patterns were seen in one case of minor salivary gland tumor [Table 2 and Figure 1]. The cellular component, when compared between the tumors of major and minor salivary glands, showed predominantly cuboidal cells constituting majority of the tumoral mass followed by spindle cells, basaloid cells, plasmacytoid cells and squamous cells, respectively [Tables 1 and 2]. The plasmacytoid cells showed significance and were predominantly observed in submandibular (100%), parotid (70%) and minor salivary glands (30%), whereas spindle cells, basaloid cells and squamous cells were predominantly seen in submandibular and minor salivary glands than parotid [Table 3].
Figure 1.

Photomicrographs of the hematoxylin and eosin-stained tissue sections showing trabecular and ductal pattern of pleomorphic adenoma of major and minor salivary glands
The stromal components were constituting predominantly of myxoid and chondroid stromas representing around 50% of the tumoral mass, with limited areas of hyalinization [Figure 2]. In the myxoid stroma, the modified myoepithelial cells designated as myxoid cells were seen with stellate morphology which was morphofunctionally modified for the synthesis of mucopolysaccharides. The chondroid zones showed areas abundant with extracellular matrix rich in mucopolysaccharides with chondroid lacunae. The chondrocytes were seen round to columnar when isolated or in group as two cells accordingly with round-to-oval nucleus that is placed central or little eccentric with clear or weak acidophilic cytoplasm. The stromal zones with osteoid areas were absent [Table 1].
Figure 2.
Photomicrographs of the hematoxylin and eosin-stained tissue sections showing cellular components, stromal components, capsular alterations and inflammatory changes of pleomorphic adenoma of major and minor salivary glands
Keratin pearls were observed in the tumors of both major and minor salivary glands but were predominant in tumors of minor salivary glands [Table 1]. In few cases of minor salivary gland tumor, extensive squamous metaplasia is observed forming cyst-like structures of variable size and shape lined by the epithelial cells resembling cystic pleomorphic adenoma [Figure 2]. Few cyst-like structures showed keratin degeneration also. The extensive squamous metaplasia does not signify malignant transformation until unless it is associated with the capsular invasion, hemorrhage, necrosis alternating with areas presenting classical features of pleomorphic adenoma;[5] rather it signifies only diagnostic pitfall[12,17] [Figure 2]. Hence, cases mimicking malignant tumors that may mislead to diagnosis of squamous cell carcinoma or mucoepidermoid carcinoma in preexisting pleomorphic adenoma must be ruled out.[18]
All the cases of major salivary gland tumors were encapsulated with partial encapsulation seen in minor salivary gland tumors; the tumor tissue merging with fat or salivary gland tissue [Table 1]. Other capsular characteristics such as capsular penetration, satellite nodules and pseudopodia were not appreciated. Chronic inflammatory cells were seen moderate to dense in the peritumoral area as well as in stroma in almost all the cases of major and minor salivary glands of the connective tissue capsule as well as in the connective tissue stroma [Tables 5 and 6].
Table 5.
Areas of inflammation present both in major and minor salivary glands pleomorphic adenoma
| Site | Areas of inflammation present (%) |
|---|---|
| Major salivary glands | 19 (95) |
| Minor salivary glands | 19 (95) |
Table 6.
Areas of inflammation in pleomorphic adenoma of parotid, submandibular and minor salivary glands
| Site | Areas of inflammation present (%) |
|---|---|
| Parotid gland | 16 (80) |
| Submandibular gland | 3 (100) |
| Minor salivary gland | 19 (95) |
CONCLUSION
Our study demonstrated the diversity of histomorphological aspects of cells in these tumors; the most frequent is being the plasmacytoid cells that were seen predominantly in major salivary gland tumors. Increased density of blood vessels was seen in major salivary gland tumors indicating its role in angiogenesis. Areas of hyalinization were predominantly present in major salivary gland tumors. Squamous metaplasia with formation of cyst-like structures and trabecular pattern was evident in minor salivary gland tumors, which may pose significant diagnostic challenge. Hence, careful evaluation of such cases is mandatory not to mislead the diagnosis, which may mimic malignant lesion leading to aggressive therapy. Pleomorphic adenoma can mimic other salivary gland tumors, so the knowledge of diversity of cells, architecture and morphologic characteristics present in the tumor is very essential for the correct diagnosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Lima SS, Soares AF, de Amorim RF, Freitas Rde A. Epidemiologic profile of salivary gland neoplasms: Analysis of 245 cases. Braz J Otorhinolaryngol. 2005;71:335–40. doi: 10.1016/S1808-8694(15)31332-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ito FA, Jorge J, Vargas PA, Lopes MA. Histopathological findings of pleomorphic adenomas of the salivary glands. Med Oral Patol Oral Cir Bucal. 2009;14:E57–61. [PubMed] [Google Scholar]
- 3.Rajendran R, Sivapathasundharam B. 5th ed. New Delhi (India): Elseiver; 2007. Shafer's Text of Oral Pathology; p. 311. [Google Scholar]
- 4.Rahnama M, Orzędała-Koszel U, Czupkałło L, Lobacz M. Pleomorphic adenoma of the palate: A case report and review of the literature. Contemp Oncol (Pozn) 2013;17:103–6. doi: 10.5114/wo.2013.33438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Melkundi M, Babaji P, Saikhedkar R, Chaluvaiah MB. Pleomorphic adenoma of parotid gland: A case report. OMPJ. 2012;3:228–31. [Google Scholar]
- 6.Rao SA, More MP, Chinde VV. Pleomorphic adenoma of submandibular salivary gland in a young female of 27 years. Bombay Hosp J. 2008;50:534–5. [Google Scholar]
- 7.Mubeen K, Vijayalakshmi KR, Abhishek RP, Giraddi GB, Singh C. Benign pleomorphic adenoma of minor salivary gland of palate. J Dent Oral Hyg. 2011;3:82–8. [Google Scholar]
- 8.Yamamoto H, Fukumoto M, Yamaguchi F, Sakata K, Oikawa T. Pleomorphic Adenoma of the buccal gland in a child. Int J Oral Maxillofac Surg. 1986;15:474–7. doi: 10.1016/s0300-9785(86)80041-2. [DOI] [PubMed] [Google Scholar]
- 9.Gani AN, Megat Shiraz MA, Siti Aishah MA, Norazizah M, Mazita A, Sharifah NA. Pleomorphic adenoma originating from submandibular salivary gland in an 8-year-old girl: A case report. Med Health. 2007;2:164–8. [Google Scholar]
- 10.Rawat DS, Sonkhya D, Sonkhya N, Gupta S. Myoepithelial cell-rich pleormorphic adenoma of minor salivary gland of parapharyngeal space. Case Rep Otolaryngol. 2012;2012:537381. doi: 10.1155/2012/537381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Al-Khtoum N, Qubilat AR, Al-Zaidaneen S, Al Mefleh S, Al-Qudah A. Clinical characteristics of pleomorphic adenoma of salivary glands among Jordanian patients. J Pak Med Assoc. 2013;63:358–60. [PubMed] [Google Scholar]
- 12.Chidzonga MM, Lopez Perez VM, Portilla Alvarez AL. Pleomorphic adenoma of the salivary glands. Clinicopathologic study of 206 cases in Zimbabwe. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79:747–9. doi: 10.1016/s1079-2104(05)80310-5. [DOI] [PubMed] [Google Scholar]
- 13.Ellis GL, Auclair PL, Gnepp DR. Philadelphia: WB Saunders; 1991. Mixed tumor (pleomorphic adenoma) and myoepithelioma. Surgical Pathology of Salivary Glands; pp. 167–82. [Google Scholar]
- 14.Soares AB, Altemani A, de Araújo VC. Study of histopathological, morphological and immunohistochemical features of recurrent pleomorphic adenoma: An attempt to predict recurrence of pleomorphic adenoma. J Oral Pathol Med. 2011;40:352–8. doi: 10.1111/j.1600-0714.2010.00956.x. [DOI] [PubMed] [Google Scholar]
- 15.Goulart MC, Freitas-Faria P, Goulart GR, Oliveira AM, Carlos-Bregni R, Soares CT, et al. Pleomorphic adenoma with extensive squamous metaplasia and keratin cyst formations in minor salivary gland: A case report. J Appl Oral Sci. 2011;19:182–8. doi: 10.1590/S1678-77572011000200016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Nezhad MJ, Moghadam SA, Mokhtari S, Taravati S. Different histopathologic features of pleomorphic adenoma of salivary glands. Int J Oral Maxillofac Pathol. 2013;4:7–11. [Google Scholar]
- 17.Kara MI, Göze F, Ezirganli S, Polat S, Muderris S, Elagoz S. Neoplasms of the salivary glands in a Turkish adult population. Med Oral Patol Oral Cir Bucal. 2010;15:e880–5. doi: 10.4317/medoral.15.e880. [DOI] [PubMed] [Google Scholar]
- 18.Mag SA, Cotulbea AH, Marin C, Doros D, Neamtu N, Balica A, et al. Carcinoma ex pleomorphic adenoma in parotid gland - case report. J Exp Med Surg Res. 2010;27:205–9. [Google Scholar]