

Abstract
Surgical procedures to treat anterior shoulder instability are basically split into 2 groups: those for patients with important bone loss and those for patients with no bone loss. However, there is a gray zone between these procedures in which a bone graft would not be needed but bone grafting would result in a desirable improvement in stabilizing mechanisms. We describe a technique based on the triple soft-tissue block, Bankart reconstruction, and long head of the biceps tenodesis at the anterior glenoid rim. The long head of the biceps would add an anterior restrictor by itself, as well as by tensioning the inferior part of the subscapularis.
Anterior shoulder instability remains one of the main issues within shoulder surgery. There are several studies showing that arthroscopic Bankart repair is successful in treating traumatic anterior shoulder instability without bone loss.1 On the other hand, glenoid bone loss greater than 21% to 25% and engaging lesions seem to present better results with bony procedures such as the Bristow and Latarjet procedures,2, 3, 4, 5 and both techniques present similar results.6
Some authors have also suggested that other predictive factors, such as age at the first episode, sport, and so on, need to be considered when choosing the surgical procedure, whereas others have suggested that glenoid bone loss can be critical even with 13.5% of bone loss.1, 7 Indeed, there is a gray zone in treating anterior shoulder instability, which can be treated by both the Bankart and Bristow-Latarjet procedures.
Some authors have presented the arthroscopic belt-and-suspenders procedure combining principles of the Bankart and Bristow-Latarjet procedures to improve shoulder stability by using just the soft-tissue stabilizers; however, this procedure is time-consuming, uses a large medial bone tunnel, and presents a recurrence rate of 8%.8 Many authors have reported that the long head of the biceps (LHB) does not have an important function related to shoulder stability. In addition, some studies have suggested that the LHB is just a vestigial structure out of the natural biceps axis.9, 10, 11, 12
On the basis of these fundamentals, it seems more rational to use the LHB to provide both the direct sling effect and tension to the inferior part of the subscapularis.13 These 2 biomechanical stabilizer mechanisms in a lateralized fashion associated with the Bankart procedure can achieve better results for the aforementioned gray zone. We have successfully performed this LHB Bristow-Bankart procedure for 3 years, described as follows.
Surgical Technique
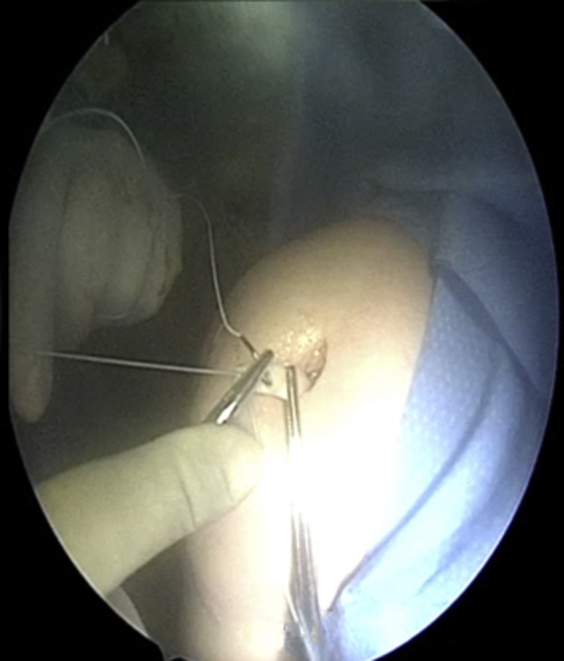
The patient is placed in the beach-chair position under general anesthesia. Through a standard posterior portal, articular inspection is performed, and the lesions are examined under an arthroscopic view. An anteroinferolateral portal is created 1 cm inferior and just lateral to the standard anterior portal. A 16-gauge needle will confirm the best location of this portal. The portal needs to be in line with the humeral head equator. Through this portal, the subscapularis tendon is gently opened in the direction of its fibers using a Kelly device (Fig 1). At this moment, some electrocautery devices and/or a shaver can be useful to widen this subscapularis split.
Fig 1.
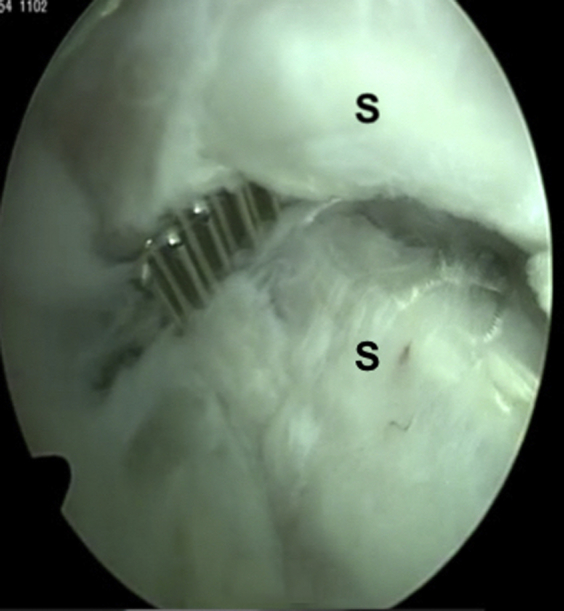
Scope in posterior portal. Split of subscapularis tendon using Kelly hemostatic device. (S, subscapularis and capsule.)
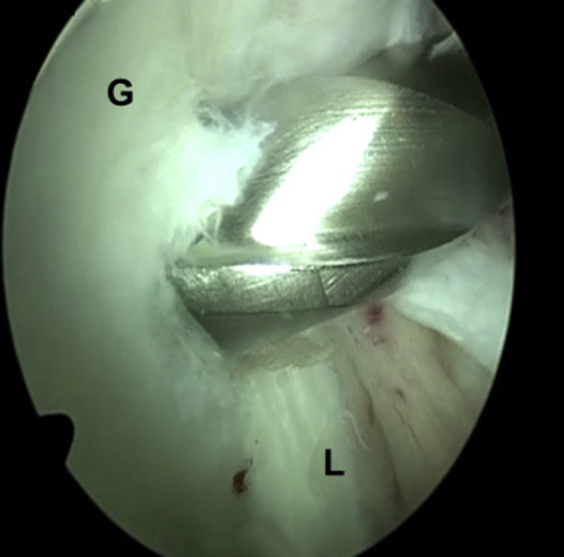
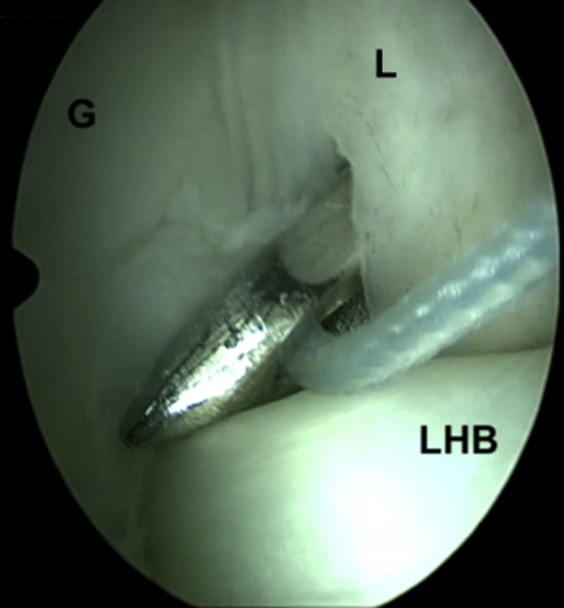
Through the portal, the surgeon also performs the LHB tenotomy (Fig 2). The anterior glenoid rim is exposed, and the bone is shaved to expose a surface to allow it to heal, similarly to the Bankart procedure. Thereafter, the scope is inserted in the anterolateral portal. The scope moves downward in the direction of the pectoralis major insertion, and visualization of the axillary nerve is suggested at this point (Fig 3). Other instruments are inserted through the anteroinferolateral portal. The LHB tendon is then pulled out just over the pectoralis major (Fig 4). Thereafter, it is pulled out of the body through the anteroinferolateral portal using a grasper. If the surgeon does not release the LHB just over the pectoralis major, the LHB cannot present free motion, and the patient can lose movement after surgery.
Fig 2.
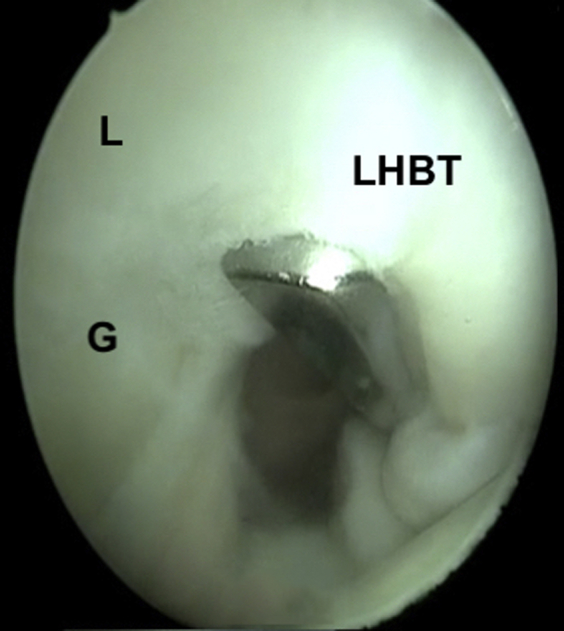
Scope in posterior portal. Cutting of long head of biceps tendon (LHBT) using basket. (G, glenoid; L, labrum.)
Fig 3.
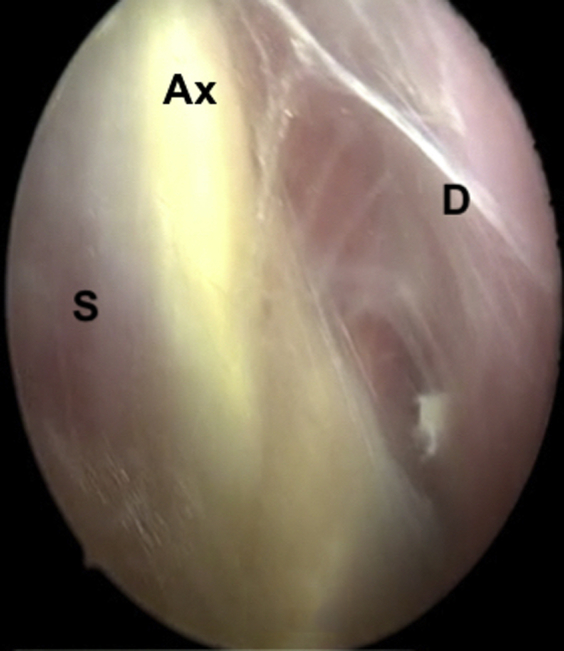
Scope in anterolateral portal. (Ax, axillary nerve; D, deltoid; S, subscapularis.)
Fig 4.
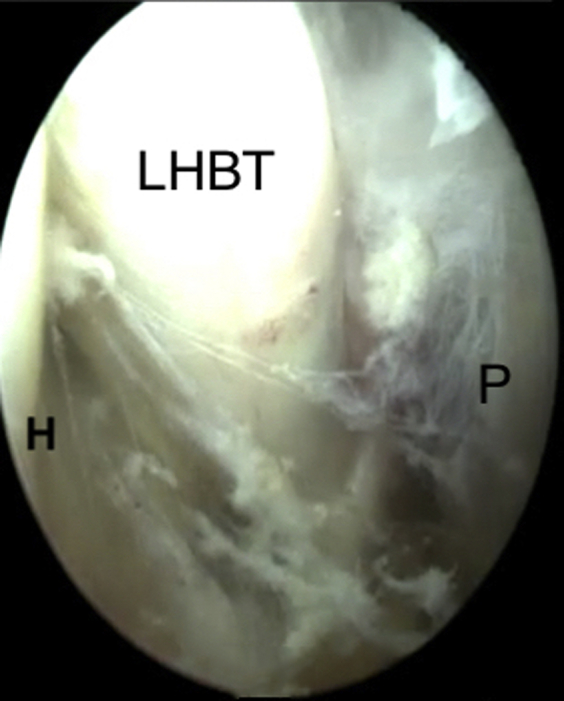
Scope in anterolateral portal downward in direction to pectoralis major tendon (P). (H, humerus; LHBT, long head of biceps tendon).
Out of the body, a Biotenodesis screw (Arthrex, Naples, FL) is attached to the LHB through a Krackow suture using FiberWire (Arthrex) (Fig 5). A Biotenodesis guidewire is inserted in the same portal through which the LHB was pulled out. This wire passes through the subscapularis split and is inserted just medial to the anterior glenoid rim at the 3- to 4-o'clock position. The bone tunnel is made using a 5- to 6-mm-diameter drill, depending on the tendon diameter (Fig 6). We have never used screws of less than 4.75 mm in diameter and have used drills with diameters of at least 0.25 mm greater than the screw diameter. The tendon is inserted through the subscapularis split on the anterior glenoid rim (Figs 7 and 8).
Fig 5.
Krackow suturing of long head of biceps tendon through the anteroinferolateral portal.
Fig 6.
Scope in posterior portal. Drill in anterior glenoid rim. (G, glenoid; L, labrum.)
Fig 7.
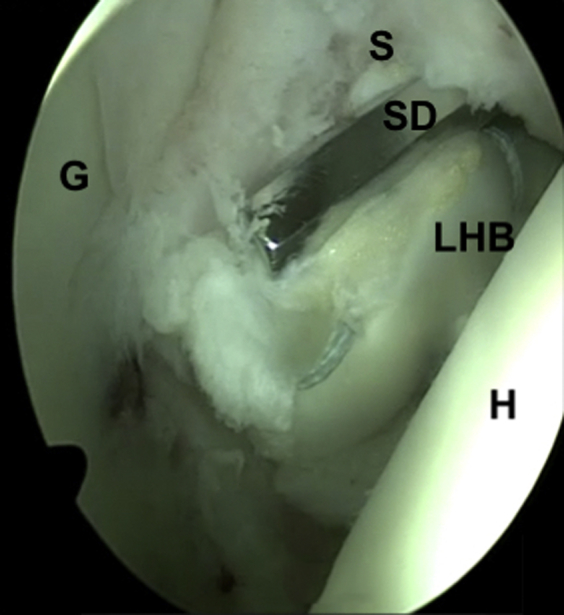
Scope in posterior portal. Insertion of long head of biceps tendon (LHB) in drill hole. (G, glenoid; H, humeral head; S, subscapularis and capsule; SD, Biotenodesis screwdriver.)
Fig 8.
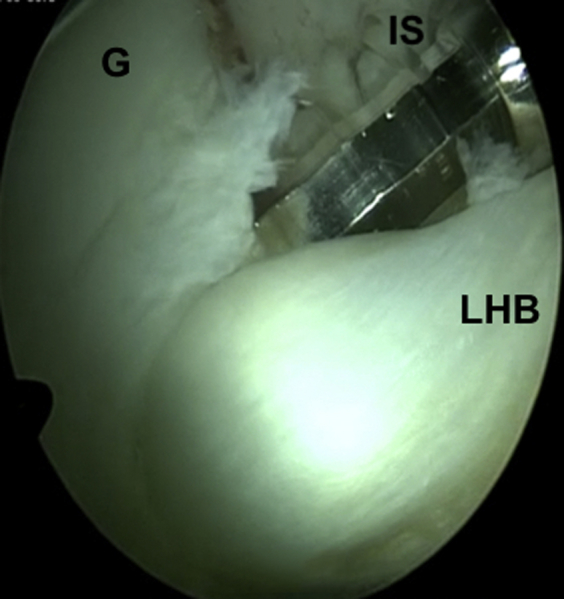
Scope in posterior portal. Insertion of Biotenodesis interference screw (IS). (G, glenoid; LHB, long head of biceps tendon.)
The labrum is sutured just above the inserted tendon using the FiberWire that was inserted with the interference screw (Fig 9). Two 1.5-mm JuggerKnot suture anchors (Zimmer-Biomet, Warsaw, IN) can be inserted above and under the inserted tendon through the subscapularis split using a cannula in the anteroinferolateral portal, allowing labral reconstruction; sometimes, the superior anchor might not be necessary (Fig 10, Video 1). Thus, one could achieve a triple suture for the Bankart repair associated with the sling effect.
Fig 9.
Scope in posterior portal. Superior suture of labrum using interference screw and FiberWire. (G, glenoid; L, labrum; LHB, long head of biceps tendon.)
Fig 10.
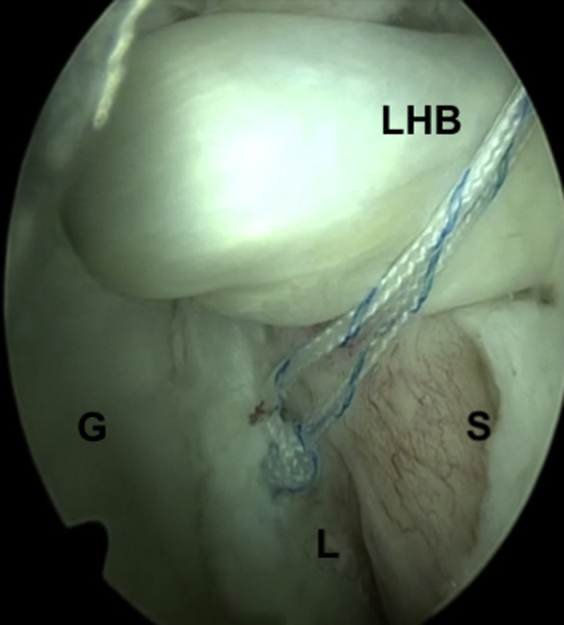
Scope in posterior portal. Inferior suture using JuggerKnot suture anchor. (G, glenoid; L, labrum; LHB, long head of biceps tendon; S, subscapularis and capsule.)
Pearls and pitfalls of the described procedure are stated in Table 1. No recurrence, pain, or LHB lesions have been observed. All patients presenting more than 6 months after surgery returned to their sporting activities with no or minimal range-of-motion loss. For some patients, magnetic resonance imaging examinations were performed after the procedure (Figs 11 and 12).
Table 1.
Pearls and Pitfalls
| Pearls and Pitfalls | |
|---|---|
| Anterolateral portal | The ideal point is 45° anterior to the scapular axis, just over the biceps deflection, guided by an 18-gauge needle via an intra-articular view, with the scope in the posterior portal. |
| Anteroinferolateral portal | The ideal point is through the subscapularis tendon, near its insertion in the humerus, in line with the humeral head equator, guided by an 18-gauge needle via an intra-articular view, with the scope in the posterior portal. |
| Cutting LHB | An anteroinferolateral or anterior standard portal should be used. Cutting should not be performed too proximally and should be performed where the elliptical diameters seem to be more similar to those of the LHB. |
| Accessing superior portion of pectoralis tendon | The scope should be inserted in the anterolateral portal, in the subdeltoid space, in the direction of the pectoralis major insertion. A shaver should be carefully applied to the bursa; the LHB emerges from the bicipital tunnel under the superior portion of the pectoralis major, beneath the short head. Special care is needed for bleeding in this region because vessels can be close. |
| If bicipital tunnel extends distally | The tunnel needs to be opened in this area to pull the biceps tendon in this situation. |
| If biceps does not pass through tunnel | The entire tunnel needs to be opened in this situation. |
| Insertion point | This should be performed just after the LHB tendon is pulled out. The guidewire should be inserted just over the LHB, through the subscapularis split, with no cannula. The guidewire should be inserted just medial to the glenoid rim at the 3-o'clock position, similarly to anchor insertion. The hole should extend to the glenoid. A cannula should not be used. |
| Anchor insertion | Preference should be given to soft-tissue anchors once the space is small. A cannula should be used. If required by the surgeon, an anterior portal can also be made, but in our experience, this is not necessary. |
LHB, long head of biceps.
Fig 11.

Elevation (A) and external rotation (B) 3 months after surgery. (C) Anterolateral portal (1) and anteroinferolateral portal (2).
Fig 12.

Magnetic resonance imaging. (A) Axial T2 image at level of interference screw. (B) Axial T2 image under level of interference screw. (C) Frontal T2 image at level of interference screw. (D) Frontal T2 image anterior to interference screw. (E) Sagittal T2 image at level of lateral part of interference screw plus long head of biceps tendon (LHB). (F) Sagittal T2 image at level of subscapularis split.
Discussion
Dynamic stabilization due to the sling effect can be the main stabilizer of the shoulder even for Bristow and Latarjet procedures, contributing to 51% to 77% of all stabilization, depending on the upper-limb position.13 This procedure presents a triple soft-tissue block in which the key points are the LHB and the tension of the inferior part of the subscapularis during abduction and external rotation, as well as labral reconstruction. It changes the shoulder kinematics similarly to the Latarjet procedure with no bone block.14 In the end-range position, the capsule and ligament plus the sling effect can be responsible for even 100% of the stability of the Latarjet repair.13
A similar triple soft-tissue block was described using the conjoined tendon8 instead of the LHB. However, because of the large transverse area of the conjoined tendon, the interference screw needs to present a larger diameter, as well as its introduction hole. The presented procedure uses smaller interference screws and the LHB as the sling, preserving the bone stock and allowing a more lateral position for inserting this screw. This feature would potentially add stability. Medialization of the graft with the Bristow procedure can increase rates of recurrent instability.15
There is no consensus on the role of the dynamic stabilizers of the shoulder. Thus far, all biomechanical studies using cadavers have rendered ineffective dynamic assessments. Labral proprioception can also play an important and neglected role in shoulder stability.16 We suggest that the described procedure and similar procedures17, 18 will add not only biomechanical stabilization19 but also tendon proprioception of the LHB, and the subscapularis can also play an important role in shoulder stabilization.
A similar technique has been described17; however, the following important differences are highlighted: (1) The position and angle of the interference screw differ. In this procedure, it is inserted more laterally, and it is just medial to the glenoid rim, in the same position at which the surgeon would insert a suture anchor. Thus, this screw will also present more lateral angulation in relation to the glenoid plane. (2) The subscapularis split is more lateral, is smaller, and is opened with a Kelly device in the direction of its fibers, allowing better neurologic and subscapularis preservation. (3) Preparation of the glenoid is ever done posterior to the labrum, and this structure is never pulled through the posterior portal. (4) The bicipital groove is not opened, preserving part of the anterior rotator cable that goes to the lesser tuberosity.20 (5) The tendon is cut where it presents a cylindrical axial aspect, allowing it to move through the bicipital groove and to be pulled out just after the bicipital groove.
Similarly to other authors, we believe that the LHB is a residual structure derived from the ancient coracoid bone of quadrupeds.12, 21 In bipeds, this bone also followed the natural axis of the biceps originating at the coracoid process with a 90° rotation of the original coracoid bone.12, 22 Some primates do not present an LHB similar to that in humans, whereas in some, it can even originate on the pectoralis major insertion or in the humeral head.23
Indeed, the real kinematic importance of the LHB is still controversial. The described procedure would not substitute for bone block procedures with more than 20% to 25% of glenoid bone loss and instead would add stability to the current soft-tissue procedures for smaller amounts of bone loss. It could also be useful for athletes and high-demand patients.1, 4, 7 Advantages and disadvantages of this procedure compared with arthroscopic coracoid and conjoined tendon transfers24, 25, 26 or arthroscopic Bankart repair are suggested in Table 2.
Table 2.
Suggested Differences Between Arthroscopic Bristow-Latarjet, LHB Bristow-Bankart, and Arthroscopic Bankart Procedures
| Arthroscopic Bristow-Latarjet Procedure | LHB Bristow-Bankart Procedure | Bankart Procedure | |
|---|---|---|---|
| Surgical time | High (approximately 1 h 30 min) | Intermediate (approximately 1 h) | Fast (approximately 30 min) |
| Learning curve | Large | Intermediate | Small |
| Intraoperative complications | High | High | Low |
| Postoperative complications | Intermediate | Low | Low |
| Redislocation | Highly improbable | Highly improbable | Improbable |
| Use for contact sports | Strongly recommended | Strongly recommended | Recommended |
| Loss of ER | Moderate | Small | Small |
| Glenoid bone <5% | Not necessary | Not necessary | Strongly recommended |
| Glenoid bone >5% but <21% | Not necessary | Strongly recommended | Recommended |
| Glenoid bone >21% | Strongly recommended | Not recommended | Not recommended |
| Engagement | Strongly recommended | Association with remplissage | Association with remplissage |
ER, external rotation; LHB, long head of biceps.
While performing this procedure, it is possible to incorporate other procedures, such as remplissage. In addition, in case of the failure of this procedure, it is possible to apply the Bristow or Latarjet procedure. There is a possibility of LHB tendon rupture, glenoid fracture, and cyst formation, although we have never observed these.
The surgical time for this procedure to access the superior insertion of the pectoralis major is longer compared with the Bankart procedure, in addition to requiring arthroscopic training. If the LHB is pathologic and presents areas of disruption, it can also be oversized in its intra-articular portion. In this case, opening the intertubercular ligament can be an option. In our opinion, this surgical procedure and similar procedures17 can fit exactly in the gray zone between Bankart and Bristow-Latarjet procedures.19
Footnotes
The authors report the following potential conflicts of interest or sources of funding: J.C.G. is a paid speaker for Latin America Zimmer-Biomet. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
Long head of biceps (LHB) Bristow procedure for anterior shoulder instability. The patient is a 23-year-old skydiver with recurrent anterior shoulder instability. A standard release of the labrum is performed. Debridement using a regular shaver is also performed, followed by marrow bone exposure using a bony shaver. The surgeon then looks upward to the LHB tendon and cuts it using regular arthroscopic scissors. The scope is inserted in the anterolateral portal, and the axillary nerve is found. In addition, the LHB is found behind the pectoralis major, and the tendon is pulled out of the body through the anteroinferolateral portal. A Krackow suture is made in the tendon, and the interference screw is ready to use. The subscapularis is then split in the direction of its fibers using a regular Kelly device. This split can be widened by a shaver or electrocautery device. The guide K-wire is inserted in the anterior glenoid rim. Thereafter, the drill creates the hole into which the biceps and interference screw will be inserted. The LHB is introduced through the subscapularis split to the hole. The interference screw fixes the LHB tendon. The labrum over the biceps can be sutured using the screw wire or a suture anchor. Finally, inferior to the tendon, a suture anchor is inserted to fix the inferior labrum.
References
- 1.DeFroda S., Bokshan S., Stern E., Sullivan K., Owens B.D. Arthroscopic Bankart repair for the management of anterior shoulder instability: Indications and outcomes. Curr Rev Musculoskelet Med. 2017;10:442–451. doi: 10.1007/s12178-017-9435-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Beran M.C., Donaldson C.T., Bishop J.Y. Treatment of chronic glenoid defects in the setting of recurrent anterior shoulder instability: A systematic review. J Shoulder Elbow Surg. 2010;19:769–780. doi: 10.1016/j.jse.2010.01.011. [DOI] [PubMed] [Google Scholar]
- 3.Itoi E., Lee S.B., Berglund L.J., Berge L.L., An K.N. The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: A cadaveric study. J Bone Joint Surg Am. 2000;82:35–46. doi: 10.2106/00004623-200001000-00005. [DOI] [PubMed] [Google Scholar]
- 4.Burkhart S.S., De Beer J.F. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy. 2000;16:677–694. doi: 10.1053/jars.2000.17715. [DOI] [PubMed] [Google Scholar]
- 5.Lo I.K., Parten P.M., Burkhart S.S. The inverted pear glenoid: An indicator of significant glenoid bone loss. Arthroscopy. 2004;20:169–174. doi: 10.1016/j.arthro.2003.11.036. [DOI] [PubMed] [Google Scholar]
- 6.Garcia J.C., Amaral F.M., Belchior R.J., Carvalho L.Q., Markarian G.G., Montero E.F.S. Comparative systematic review of fixation methods of the coracoid and conjoined tendon in the anterior glenoid to treat anterior shoulder instability. Orthop J Sports Med. 2019;7 doi: 10.1177/2325967118820539. 2325967118820539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shaha J.S., Cook J.B., Song D.J. Redefining "critical" bone loss in shoulder instability: Functional outcomes worsen with "subcritical" bone loss. Am J Sports Med. 2015;43:1719–1725. doi: 10.1177/0363546515578250. [DOI] [PubMed] [Google Scholar]
- 8.Boileau P., Bicknell R.T., Fegoun A.B.E., Chuinard C. Arthroscopic Bristow procedure for anterior instability in shoulders with a stretched or deficient capsule: The “belt-and-suspenders” operative technique and preliminary results. Arthroscopy. 2007;23:593–601. doi: 10.1016/j.arthro.2007.03.096. [DOI] [PubMed] [Google Scholar]
- 9.Giphart J.E., Florian E.F., Dewing C.B., Torry M.R., Millett P.J. The long head of the biceps tendon has minimal effect on in vivo glenohumeral kinematics. A biplane fluoroscopy study. Am J Sports Med. 2012;40:202–212. doi: 10.1177/0363546511423629. [DOI] [PubMed] [Google Scholar]
- 10.Kuarm V.P., Satkum K., Balasubramaniam P. The role of the long head of biceps brachii in the stabilization of the head of the humerus. Clin Orthop Relat Res. 1989;244:172–175. [PubMed] [Google Scholar]
- 11.Garcia J.C., Cardoso A.M., Mello M.B.D. Arthroscopic long head biceps tenodesis in coracoid associated with its transfer to the conjoined tendon. Acta Shoulder Elbow Surg. 2017;2:7–10. [Google Scholar]
- 12.Garcia J.C., Nunes C.V., Raffaelli M.D.P. Long head of biceps a vestigial structure? Acta Shoulder Elbow Surg. 2017;2:22–27. [Google Scholar]
- 13.Yamamoto N., Steinmann S.P. The biomechanics of the Latarjet reconstruction: Is it all about the sling? Oper Tech Sports Med. 2019;27:49–54. [Google Scholar]
- 14.Barrett Payne W., Kleiner M.T., McGarry M.H., Tibone J.E., Lee T.Q. Biomechanical comparison of the Latarjet procedure with and without a coracoid bone block. Knee Surg Sports Traumatol Arthrosc. 2016;24:513–520. doi: 10.1007/s00167-015-3885-0. [DOI] [PubMed] [Google Scholar]
- 15.Hovelius L., Korner L., Lundberg B. The coracoid transfer for recurrent dislocation of the shoulder. Technical aspects of the Bristow-Latarjet procedure. J Bone Joint Surg Am. 1983;65:926–934. [PubMed] [Google Scholar]
- 16.Tsuda Y., Amako M., Hirahara Y., Kawaguchi M. Shoulder joint proprioception for patients with traumatic shoulder instability compared to normal subjects. J Shoulder Elbow Surg. 2018;27:1537–1538. [Google Scholar]
- 17.Collin P., Lädermann A. Dynamic anterior stabilization using the long head of the biceps for anteroinferior glenohumeral instability. Arthrosc Tech. 2018;7:e39–e44. doi: 10.1016/j.eats.2017.08.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tang J., Zhao J. Arthroscopic transfer of the long head of the biceps brachii for anterior shoulder instability. Arthrosc Tech. 2017;6:e1911–e1917. doi: 10.1016/j.eats.2017.07.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mehl J., Otto A., Imhoff F.B. Dynamic anterior shoulder stabilization with the long head of the biceps tendon: A biomechanical study. Am J Sports Med. 2019;47:1441–1450. doi: 10.1177/0363546519833990. [DOI] [PubMed] [Google Scholar]
- 20.Rahu M., Kolts I., Põldoja E., Kask K. Rotator cuff tendon connections with the rotator cable. Knee Surg Sports Traumatol Arthrosc. 2017;25:2047–2050. doi: 10.1007/s00167-016-4148-4. [DOI] [PubMed] [Google Scholar]
- 21.Luo Z.X. Origin of the mammalian shoulder. In: Dial K.P., Shubin N.H., Brainerd E.L., editors. Great transformations: Major events in the history of vertebrae life. University of Chicago Press; Chicago: 2015. pp. 167–187. [Google Scholar]
- 22.Kemp T.S. Oxford University Press; Oxford: 2005. The origin and evolution of mammals. [Google Scholar]
- 23.Diogo R., Wood B. CRC Press; Boca Raton: 2012. Comparative anatomy and phylogeny of primate muscles an human evolution. [Google Scholar]
- 24.Garcia J.C., Garcia J.P.M., Mattos C.A., Zabeu J.L.A. Arthroscopic bristow-Latarjet–like procedure: Surgical technique. Tech Shoulder Elbow Surg. 2009;10:94–98. [Google Scholar]
- 25.Garcia J.C., Cordeiro E.F., Mattos C.A. Arthroscopic bristow-Latarjet procedure. Arthroscopy. 2012;28:e3–e4. [Google Scholar]
- 26.Lafosse L., Lejeune E., Bouchard A., Kakuda C., Gobezie R., Kochhar T. The arthroscopic Latarjet procedure for the treatment of anterior shoulder instability. Arthroscopy. 2007;23:1242.e1–1242.e5. doi: 10.1016/j.arthro.2007.06.008. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Long head of biceps (LHB) Bristow procedure for anterior shoulder instability. The patient is a 23-year-old skydiver with recurrent anterior shoulder instability. A standard release of the labrum is performed. Debridement using a regular shaver is also performed, followed by marrow bone exposure using a bony shaver. The surgeon then looks upward to the LHB tendon and cuts it using regular arthroscopic scissors. The scope is inserted in the anterolateral portal, and the axillary nerve is found. In addition, the LHB is found behind the pectoralis major, and the tendon is pulled out of the body through the anteroinferolateral portal. A Krackow suture is made in the tendon, and the interference screw is ready to use. The subscapularis is then split in the direction of its fibers using a regular Kelly device. This split can be widened by a shaver or electrocautery device. The guide K-wire is inserted in the anterior glenoid rim. Thereafter, the drill creates the hole into which the biceps and interference screw will be inserted. The LHB is introduced through the subscapularis split to the hole. The interference screw fixes the LHB tendon. The labrum over the biceps can be sutured using the screw wire or a suture anchor. Finally, inferior to the tendon, a suture anchor is inserted to fix the inferior labrum.