

Abstract
EBV-associated myoid tumor (EBVMT) comprises a specific group of soft tissue tumors with divergent histologic appearances, which typically occur in immunocompromised patients. To the best of our knowledge, there have been no previous reported of EBVMT in patients with normal immunity. EBVMT with lipoblast-like cells (EBVMT-LIC) is an extremely rare variant of EBVMT. Here, a male patient with normal immunity and EBVMT-LIC is presented. Comprehensive EBV latency expression pattern and tumorigenesis molecular analyses are performed to detail the pathologic features of this disease. Our patient was a 14-year-old who suffered from Burkitt’s lymphoma 6 years ago and got complete remission for 5 years. At his last visit, he presented with pain and weakness in arms and legs. Subsequent MRI revealed an extramedullary mass at the cervical areas. CT-guided resection was then performed and comprehensive histopathologic examination was conducted. We found a haemangiopericytoma-like pattern with EBER-positive lipoblasts exist in this neoplasm and these features were in accordance with the diagnosis of EBVMT-LIC. Also, the EBV type I latency pattern was observed and the activation of Akt/mTOR pathway and Bcl-2 overexpression were found to be involved in the tumorigenesis of EBVMT-LIC. In conclusion, the results of this study suggest that EBVMT can occur in patients with normal immunity. EBV could achieve a latency type I pattern and may promote the development of EBVMT by activation of Akt/mTOR pathway and Bcl-2 overexpression. The role of chronic latent EBV infection in the development of EBVMT may be more important than previously thought.
Keywords: EBV-associated myoid tumor, lipoblast-like cells, EBV latency expression pattern, Akt/mTOR signaling pathway, Bcl-2 oncogene
Background
Epstein-Barr virus (EBV), a double-stranded DNA virus, is thought to serve as a causative agent in a variety of human cancers, including nasopharyngeal carcinoma, Burkitt’s lymphoma (BL) and Hodgkin’s lymphoma. Since the 1990s, EBV has been implicated in the development of a range of myoid tumors, mainly including smooth muscle tumor (EBVSMT) [1-5] and myopericytoma [6-9]. EBV-associated myoid tumor (EBVMT) was previously reported as a specific subcategory, with a divergent histologic appearance, that occurs exclusively in patients with acquired immunodeficiency syndrome (AIDS), clinical immunosuppression and primary immunodeficiency disorder (PID) [10,29].
In 2017, Cheng et al [11] identified a new type of EBVMT named EBVMT with lipoblast-like cells (EBVMT-LIC). They reported that the pathologic features of this tumor were unique compared with other EBVMTs, with the presence of haemangiopericytoma (HPC)-like pattern and Epstein-Barr virus-encoded small RNA (EBER)-positive lipoblast-like cells (LIC). They also demonstrated that, as with other types of EBVMT, immunosuppression was essential for the development of EBVMT-LIC.
At present, there are three well-established patterns of EBV latent gene expression that have been reported in a number of EBV-associated malignancies, including BL, nasopharyngeal carcinoma, post-transplantation lymphoproliferative disorders (PTLD) and EBVSMT. All EBV latency profiles (type I, type II and type III) have been reported in EBVSMT [12-16], as well as an atypical profile i.e., EBER and EBV related nuclear antigen 2 (EBNA 2) expression without EBV-related latency membrane protein 1 (LMP 1) [17]. However, compared with EBVSMT, the EBV latency expression pattern in other types of EBVMT is poorly understood. Improving our understanding of EBV latent gene expression patterns may allow for targeted immunotherapy against specific EBV latent antigens as with PTLD.
Due to its relative rarity, the pathogenesis of EBVMT is not well understood. It has previously been reported that activation of the Akt/mTOR pathway and Bcl-2 overexpression induce cell proliferation in EBVSMT [18-20]; however, without an immunocompromised host, such activation and up-regulation does not lead to EBVSMT. It was therefore posited that immunodeficiency was a key driver for EBVSMT oncogenesis, a theory that was applied to all types of EBVMT. Until now, there have been no cases of EBVMT reported in non-immunocompromised patients.
Here, we present a case of EBVMT-LIC in a patient with normal immunity and persistent latent EBV infection. We investigated whether activation of the Akt/mTOR pathway or Bcl-2 overexpression were involved in the tumorigenesis of this type of EBVMT, and we also assessed the EBV latency expression profile in EBVMT-LIC. A short literature review of the clinicopathologic features of EBVMT-LIC in patients with different immune states was also performed. To date, only two cases of EBVMT-LIC have been reported worldwide, including the present study. Our study is the first to investigate the molecular pathways and EBV latency expression pattern involved in the tumorigenesis of EBVMT-LIC in a host with normal immunity.
Materials and methods
A normal immune patient with EBVMT was identified in the Pediatric Hematology-Oncology Department of Sun Yat-sen Memorial Hospital of Sun Yat-sen University. All clinical records and materials were reviewed and analyzed. Immunostaining was performed using antibodies against Ki-67 (1:200, Abcam), Bcl-2 (1:100, Abcam), caldesmon (1:100, Abcam), smooth muscle actin (SMA) (1:200, Abcam), phosphorylated-mTOR at serine 2448 (1:20, Cell Signaling) and phosphorylated-Akt at serine 473 (1:10, Cell Signaling). All sections were detected by the peroxidase detection system (Dako Cytomation). In-situ hybridization (ISH) for EBV encoded RNAs (EBER) was performed using the Epstein-Barr virus encoded RNAs (EBER) probe kit (Dako Cytomation) on the in-situ hybridization detection system (Dako Cytomation) according to the manufacturer’s instructions. Indirect immunofluorescence analysis was performed using antibody against EBNA 1 (1:100, Santa Cruz). All slices were observed under a fluorescence microscope (Olympus) and digital images were captured using Axio-Cam (Zeiss) and analyzed by Zeiss software (Version 40.4.7). All negative and positive controls were performed with samples in parallel.
Results
Case presentation
An 8-year-old male patient of Chinese Han ethnicity presented with a sigmoid colon mass in his initial visit in 2011. Pathological result of this mass were in accordance with BL. The human immunodeficiency virus (HIV) antibody screening test was negative. Polymerase chain reaction was performed and the results showed that the EBV-DNA loading in his peripheral blood was significantly elevated at 3.17 × 107 copies/ml; however, no EBV-DNA was detected in plasma samples. After diagnosis, the patient received systemic chemotherapy and regular anti-EBV therapy (ganciclovir combined with high-dose immunoglobulin) from 2011 to 2012 and entered complete remission (CR) in December 2012. Despite CR, EBV-DNA loading in his peripheral blood remained high at 1.26 × 107 copies/ml. During the follow-up period from December 2012 to May 2017, the patient continued to receive regular anti-EBV therapy; however, EBV-DNA load in the peripheral blood remained high. No recurrence of BL was observed during the follow-up period. Immunoglobulin and lymphocyte subset measures revealed normal plasma concentrations of IgG, IgA and IgM and normal CD4+ T cell, CD8+ T cell, and NK cell counts in the peripheral blood. A relatively high peripheral blood CD19+/CD20+ B cell count was recorded. These results were indicative of normal immunity in our patient. In June 2017, the patient presented with pain and weakness in the arms and legs with no obvious inducement. Subsequent brain and whole-spine magnetic resonance imaging revealed an extramedullary mass measuring 4 cm at the level of C3-C4 (Figure 1A and 1B). Computed tomography-guided resection of this soft tissue mass was then performed and the mass was successfully removed (Figure 1C). Histopathology results were in accordance with a diagnosis of EBVMT-LIC. After diagnosis, the patient’s immune status was re-examined, tests for EBV-DNA loading and human immunodeficiency virus (HIV) antibody were performed. The results revealed that the patient was negative for the HIV antibody and had normal immunity (IgG, 11.2 g/L, IgA, 1.4 g/L, IgM, 2.3 g/L, CD4+ T cell count 312 × 103/ml, CD8+ T cell count 132 × 103/ml, NK cell count 188 × 103/ml, CD19+ B cell count 512 × 103/ml and CD20+ B cell count 497 × 103/ml) with persistent latent EBV infection (EBV-DNA loading in peripheral blood: 1.86 × 106 copies/ml; in plasma: < 1.0 × 103 copies/ml). We also performed Whole-Exome sequencing analysis to identify whether our patient was a PID patient. The genetic results showed no PID-related mutations in our patient, including ATM, ADA, IL2RG, ZAP70, GATA2 and CARMIL2 gene, which are considered to be linked to the tumorigenesis of EBVMT patients with PID [29]. Those results suggested that our patient had neither secondary immunodeficiency disorder nor PID. After the diagnosis of EBVMT-LIC was made, he received postoperative chemotherapy combined with radiotherapy. At the time of writing, no recurrence of symptoms has been reported.
Figure 1.
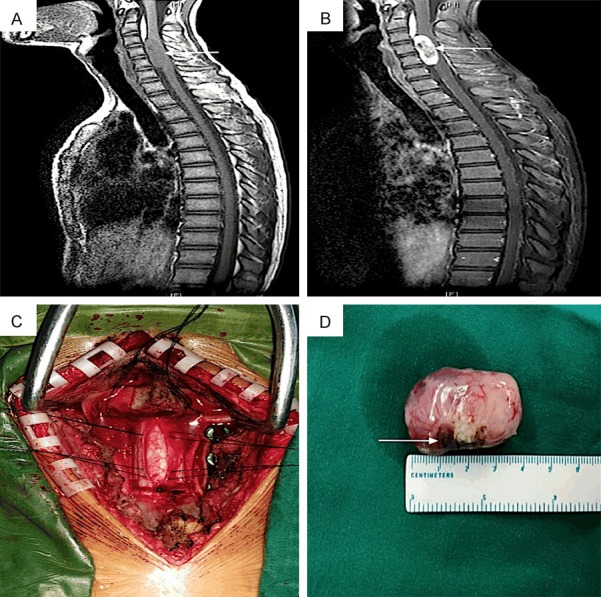
A. Sagittal T1-weighted image of the cervical spine showing an elliptical heterogeneous extramedullary mass (white arrow heads) at C3-C4 with no Dural tails; B. Sagittal post contrast T1-weighted image showing low density unenhanced areas with peripheral enhancement in the mass (white arrowheads); C. Intraoperative view of tumor resection; D. After resection, the extramedullary tumor appeared to be encapsulated with a clear border, ashen elliptical tubercle (size: 4 × 2.5 × 1.5 cm), and focal necrosis in the tumor border area (white arrowheads).
Pathologic findings
Grossly, the extradural soft tissue mass appeared as an encapsulated, ashen elliptical tubercle measuring 4 × 2.5 × 1.5 cm. The tumor surface had a soft, lobulated, white to tan appearance with focal necrosis in the border area (Figure 1D). Light microscopy showed a HPC-like pattern of vessels with spindle tumor cells in association with alternating cellularity (Figure 2A). Most spindle cells formed tightly packed whorls around the blood vessels (Figure 2B). A large number of vacuolated cells were also observed throughout the tumor (Figure 2C), and high-power observation revealed that these were LICs. The majority of LICs had multivacuolated cytoplasm with scalloped nuclear edges resembling signet ring cells (Figure 2D). The mitotic index was ~6/10 high power fields. The light microscopy results were used to corroborate a diagnosis of second primary malignancy instead of BL recurrence, but the diagnosis of this second primary neoplasm was still uncertain.
Figure 2.

A. HPC-like pattern vessels with spindle tumor cells associated with alternating cellularity (H&E staining, magnified × 100); B. Concentric spindle tumor cells around blood vessels resembled myopericytoma (white arrowheads, H&E staining, magnified × 40); C. A large number of vacuolated cells plus spindle tumor cells (H&E staining, magnified × 100); D. High power view revealed that the vacuolated cells were lipoblast-like cells, most of which had multivacuolated cytoplasm (white arrowheads, H&E staining, magnified × 200).
Immunohistochemistry revealed that both the spindle cells and LICs were diffusely positive for vimentin and CD99, whereas they were negative for S-100, cytokeratin and desmin. These results were indicative of solitary fibrous tumor (SFT). However, the neoplasm was negative for CD34 and STAT-6 antibodies, which are specific biomarkers of SFT. Tumor cells, including LICs, were strongly positive for smooth muscle actin (SMA) (Figure 3A) and some LICs and spindle cells were positive for caldesmon (Figure 3B), suggesting that the neoplasm was of myoid origin. Furthermore, < 30% of cells were positive for the proliferation marker Ki-67 (Figure 3C).
Figure 3.

A. Lipoblast-like cells and spindle cells are highlighted by antibodies against smooth muscle actin (IHC, magnified × 40); B. Some lipoblast-like cells and spindle cells stained with antibodies against caldesmon (IHC, magnified × 40); C. The proliferation marker Ki-67 highlighted a few lipoblast-like cells and spindle cells (IHC, magnified × 40); D. Lipoblast-like cells and spindle cells showed diffuse signals after EBER-ISH (ISH, magnified × 40).
EBER-ISH revealed that both spindle cells and LICs were strongly positive for EBER (Figure 3D), which is a specific marker for EBV infection. These results indicated that the neoplasm was related latent EBV infection and a diagnosis of EBVMT-LIC with uncertain malignant potential was made.
Tumorigenesis molecules and EBV latency expression pattern analysis
EBER-ISH was performed and the results revealed that the positive signals for EBER were mainly focused on cell nuclei (Figure 4A), indicating that there was a latent EBV infection in those tumor cells. CD21, the EBV receptor presenting on B cells, cannot be detected by immunostaining, which meant that other routes may exist for EBV to enter the myocytes. Bcl-2 overexpression was detected by immunohistochemistry (Figure 4B), suggesting that Bcl-2 served a role in tumorigenesis. Immunohistochemistry revealed that p-AKT (serine 473) and p-mTOR (serine 2448) were primarily localized in the nuclei of tumor cells. Strong to moderate p-AKT (Figure 4C) and p-mTOR (Figure 4D) staining was observed in >90% of cells, indicating constitutive activation of the AKT/mTOR signaling pathway. Tumor cells were negative for EBV-LMP 1 and EBV-LMP 2A, while indirect immunofluorescence revealed strong nuclear and cytoplasm expression of EBNA 1 (Figure 5) with no detectable EBNA 2 expression in the neoplasm. Together, these results indicated the presence of an EBV type I latency profile in our EBVMT-LIC case.
Figure 4.

A. EBER-ISH produced strong distinct nuclear staining in tumor cells (ISH, magnified × 100); B. High Bcl-2 expression was observed in spindle cells and lipoblast-like cells (IHC, magnified × 100); C. p-AKT staining was mainly localized in tumor cell nuclei (IHC, magnified × 100); D. Strong p-mTOR staining was observed in the nuclei of tumor cells (IHC, magnified × 100).
Figure 5.

Indirect immunofluorescence revealed strong nuclear and cytoplasm expression of EBNA 1 in EBVMT-LIC cells (Red: EBNA 1, Blue: DABI, IF, magnified × 200).
Discussion and conclusion
EBV is associated with a number of malignant neoplasms and has a critical role in their pathogenesis. The association between myoid neoplasms and EBV is uncommon; unlike in EBV-associated lymphoid malignancies or nasopharyngeal carcinoma, it was previously believed that EBVMT only occurs in immunocompromised or immunodeficient patients. Some researchers [10] even coined the term AIDS-associated myoid tumors as an alternative to EBVMT with an expanding spectrum of histopathologic appearance.
EBVMT-LIC, a novel manifestation of EBVMT, was first reported in 2017 in a patient with AIDS [11]. The patient presented in this study showed the same histologic and immunohistochemical features, with an HPC-like pattern, a large number of EBER-positive LICs and immunoreactivity for SMA and caldesmon without desmin (Table 1). A large number of LICs, which were positive for EBER-ISH, were observed throughout the tumor. This is a distinctive pathologic feature of EBVMT-LIC and does not occur in other types of EBVMT. Based on these results, we proposed that, when faced with an unusual myoid tumor with a large amount of LICs and concentric spindle cells around HPC-like pattern vessels, it may be prudent to perform EBER-ISH to exclude the possibility of EBVMT-LIC.
Table 1.
Summary of clinicopathologic features of EBVMT-LIC in patients with different immune status
| Feature | Our Case | Cheng et al [11] |
|---|---|---|
| Host | BL patient who got CR for 5 yrs | AIDS patient |
| Sex | Male | Male |
| Ethnicity | Chinese | Malay |
| Age at tumor presentation (y) | 14 | 43 |
| Tumor site (size, cm) | Spinal dura (C3-C4 level, 4 × 2.5 × 1.5) | Cerebellar (4 × 3 × 1), Spine dura (L1-L3 level, 3.5 × 3.5 × 3) |
| Tumor features | ① presence of haemangiopericytoma pattern; ② existence of lipoblast-like cells; ③ presence of spindle cells as well as lipoblast-like cells in association with EBV infection (EBER-ISH positivity) | |
| Immunohistochemistry | Vimentin+, CD99+, SMA+, Caldesmon+, S100-, CD21-, CD34-, Cytokeratin-, Desmin- | SMA+, Caldesmon+, S100-, CD34-, Cytokeratin-, Desmin-, EMA-, CD163- |
| Immune status at tumor presentation | Normal | Immunodeficiency (HIV infection) |
| EBV-DNA after diagnosis (copies/ml) | Peripheral blood: 1.86 × 106 Plasma: < 1.0 × 103 | Not reported |
| Treatment | Complete excision, Postoperative chemotherapy combined with radiotherapy | Complete excision |
| Follow-up | No recurrence until now | Not reported |
Cheng et al [11] demonstrated that EBVMT-LIC arose in the setting of immunodeficiency due to AIDS, as evidenced by episodes of persistent HIV infection with irregular anti-HIV therapy for 6 years and this result implied that the cause of EBVMT-LIC was related to the setting of an immunocompromised host, but not persistent latent EBV infection. However, the EBVMT-LIC patient presented herein was a BL patient with 5 years of CR, normal immunity and persistent latent EBV infection (Table 1). This discrepancy may indicate that persistent latent EBV infection without the setting of immunocompromised host can also cause EBVMT. The role of persistent latent EBV infection in the pathogenesis of EBVMT may be underestimated.
The pattern of latent EBV genes in different types of EBVMT remains an active area of interest [21-25], as improving our understanding of gene expression may aid in the development of novel treatment approaches. To date, no studies have been performed that show the pattern of EBV latency expression in EBVMT-LIC. In the present study, the EBV latency expression pattern was most consistent with the type I latency pattern, ie., EBNA 1 was positive while EBNA 2 and LMP 1 were undetectable. This latency pattern can occur during the chronic phase of primary infection and in patients with normal immunity, as was the case here. This finding may improve our understanding of EBV latent gene expression patterns in EBVMT, which may help develop targeted immunotherapy against EBVMT.
At present, the pathogenesis of EBVMT and the role of EBV are poorly understood. CD21, the EBV receptor for B cells and epithelial cell entry, was previously considered as an important tumorigenesis receptor for EBV [26]. However, most post-transplant EBVMT patients with mild immunospression were negative for CD21 [17]. However, some EBVMT tumor tissues from immunocompetent children with AIDS were positive for CD21, but to a lesser degree [27]. Tissues from immunodeficient children with AIDS and EBVMT were strongly positive for CD21 [28]. In our patient, tumor cells were negative for CD21. These discrepancies suggest that the route of EBV integration in EBVMT may depend on the immune status of the host. EBV may enter myocytes by CD21 in patients with severe immunodefiency, while in patients with mild to moderate immunosuppression it may enter by other unidentified routes, such as fusion with EBV-infected B cells. This may explain why cells were negative for CD21 in the present study.
The mechanism of cell proliferation in EBVMT is largely unknown, with most research mainly focused on the better-known EBVSMT [29-31]. mTOR plays a significant role in regulating cell growth, and many growth factors are able to activate mTOR to stimulate protein synthesis. High levels of dysregulated mTOR activity are associated with the pathogenesis of many tumor diseases, including EBVSMT. Overactivation of the Akt/mTOR signaling pathway was reported in EBVSMT and considered to serve an essential role in the cell proliferation of this neoplasm [26]. Ong et al [12] reported on eight solid organ transplant patients with EBVSMT, and found that all tumors were positive for phosphorylated Akt and mTOR. Shen et al [26] reported that the Akt/mTOR signaling pathway was also activated in an EBVSMT patient with AIDS. In the present study, the Akt/mTOR signaling pathway was consistently activated, suggesting that this pathway may play a role in the tumorigenesis of EBVMT-LIC. Furthermore, p-Akt/p-mTOR were localized in the nucleus, which indicates formation of the activated mTOR complex 2. This complex is less responsive to inhibition by rapamycin, suggesting that the antitumorigenic effect of rapamycin may be poor in EBVMT-LIC. Bcl-2 expression was also considered to serve a significant role in cell proliferation in EBVMT [17], which was confirmed by the results of the present study. Our findings indicate that the constitutive activation of Akt/mTOR pathway and Bcl-2 overexpression are responsible for cell proliferation in EBVMT-LIC; however, the molecular mechanisms responsible for activating the Akt/mTOR pathway and Bcl-2 overexpression remain unknown. A number of studies have suggested that a variety of EBV-related latency proteins are able to trigger overactivation of the mTOR pathway and Bcl-2 overexpression. It had been reported that mTOR activation can be induced by EBV-LMP 2A [32]. To et al [33] reported that EBV-LMP 1 triggers Bcl-2 overexpression, while another study suggested that Bcl-2 might be induced by EBERs [34]. In the present study, strong Akt/mTOR expression was not correlated with EBV-LMP 2A detection, while Bcl-2 overexpression was not associated with EBV-LMP 1. These results suggest that other EBV genes, such as EBERs and EBNA 1, are involved during latency in EBVMT-LIC, but further research is required to confirm this.
In conclusion, this study is the first to present a case of EBVMT in a patient with normal immunity. Our results suggest that EBVMT-LIC presents with an EBV type I latency pattern and the tumorigenesis of EBVMT-LIC occurs at least in part by constitutive activation of the Akt/mTOR pathway and Bcl-2 overexpression. We propose that the role of persistent latent EBV infection in the development of EBVMT is underestimated. Immunocompromise or immunodeficiency may not be essential for the pathogenesis of EBVMT. Immunocompetent patients with persistent latent EBV infection are also at risk of developing EBVMT.
Acknowledgements
This study was jointly supported by grants from the Technological Science Foundation of Guangdong Province, China (No. 4250011020). We thank the patient and his parents who allow their son to participate in this study and supplied the samples and the medical histories.
Written consent for publication was obtained from the patient’s parents. A copy of the written consent is available for review by the editors or reviews of this journal.
Disclosure of conflict of interest
None.
References
- 1.Sprangers B, Smets S, Sagaert X, Wozniak A, Wollants E, Van Ranst M, Debiec-Rychter M, Sciot R, Vanrenterghem Y, Kuypers DR. Posttransplant Epstein-Barr virus-associated myogenic tumors: case report and review of the literature. Am J Transplant. 2008;8:253–258. doi: 10.1111/j.1600-6143.2007.02054.x. [DOI] [PubMed] [Google Scholar]
- 2.Tan CS, Loh HL, Foo MW, Choong LH, Wong KS, Kee TY. Epstein-Barr virus-associated smooth muscle tumors after kidney transplantation: treatment and outcomes in a single center. Clin Transplant. 2013;27:E462–468. doi: 10.1111/ctr.12139. [DOI] [PubMed] [Google Scholar]
- 3.El Hennawy HM, Habhab W, Almutawa A, Shinawi S, Al Ayad A, Fahmy A. Long-term follow-up of post renal transplantation Epstein-Barr virus-associated smooth muscle tumors: Report of two cases and review of the literature. Transpl Infect Dis. 2018;20:e12841. doi: 10.1111/tid.12841. [DOI] [PubMed] [Google Scholar]
- 4.Yooprasert S, Thanapirom K, Treeprasertsuk S, Kullavanijaya P, Komolmit P. Hepatobiliary and pancreatic: Epstein-Barr virus-associated smooth muscle tumors: unusual cause of hepatic mass in AIDS patient. J Gastroenterol Hepatol. 2017;32:293. doi: 10.1111/jgh.13539. [DOI] [PubMed] [Google Scholar]
- 5.Issarachaikul R, Shuangshoti S, Suankratay C. Epstein-Barr virus-associated smooth muscle tumors in AIDS patients: a largest case (series) Intern Med. 2014;53:2391–2396. doi: 10.2169/internalmedicine.53.2674. [DOI] [PubMed] [Google Scholar]
- 6.Lau PP, Wong OK, Lui PC, Cheung OY, Ho LC, Wong WC, To KF, Chan JK. Myopericytoma in patients with AIDS: a new class of Epstein-Barr virus-associated tumor. Am J Surg Pathol. 2009;33:1666–1672. doi: 10.1097/PAS.0b013e3181aec307. [DOI] [PubMed] [Google Scholar]
- 7.Ramdial PK, Sing Y, Deonarain J, Singh B, Allopi L, Moodley P. Periampullary Epstein-Barr virus-associated myopericytoma. Hum Pathol. 2011;42:1348–1354. doi: 10.1016/j.humpath.2010.12.001. [DOI] [PubMed] [Google Scholar]
- 8.Calderaro J, Polivka M, Gallien S, Bertheau P, Thiebault JB, Molina JM, Gray F. Multifocal Epstein Barr virus (EBV)-associated myopericytoma in a patient with AIDS. Neuropathol Appl Neurobiol. 2008;34:115–117. doi: 10.1111/j.1365-2990.2006.00865.x. [DOI] [PubMed] [Google Scholar]
- 9.Zevgaridis D, Tsonidis C, Kapranos N, Venizelos I, Tsitsopoulos P, Tsitsopoulos P. Epstein-Barr virus associated primary intracranial leiomyoma in organ transplant recipient: case report and review of the literature. Acta Neurochir (Wien) 2009;151:1705–1709. doi: 10.1007/s00701-009-0307-4. [DOI] [PubMed] [Google Scholar]
- 10.Ramdial PK, Sing Y, Deonarain J, Vaubell JI, Naicker S, Sydney C, Hadley LG, Singh B, Kiratu E, Gundry B, Sewram V. Extra-uterine myoid tumours in patients with acquired immunodeficiency syndrome: a clinicopathological reappraisal. Histopathology. 2011;59:1122–1134. doi: 10.1111/j.1365-2559.2011.04049.x. [DOI] [PubMed] [Google Scholar]
- 11.Cheng SKH, Yap WM, Chuah KL. Myoid neoplasm with lipoblast-like cells and haemangiopericytoma pattern: an unusual manifestation of EBV associated myoid tumour. Pathology. 2017;49:435–438. doi: 10.1016/j.pathol.2016.12.350. [DOI] [PubMed] [Google Scholar]
- 12.Ong KW, Teo M, Lee V, Ong D, Lee A, Tan CS, Vathsala A, Toh HC. Expression of EBV latent antigens, mammalian target of rapamycin, and tumor suppression genes in EBV-positive smooth muscle tumors: clinical and therapeutic implications. Clin Cancer Res. 2009;15:5350–5358. doi: 10.1158/1078-0432.CCR-08-2979. [DOI] [PubMed] [Google Scholar]
- 13.Suwansirikul S, Sukpan K, Sittitrai P, Suwiwat S, Khunamornpong S. Epstein-Barr virus-associated smooth muscle tumor of the tonsil. Auris Nasus Larynx. 2012;39:329–332. doi: 10.1016/j.anl.2011.07.013. [DOI] [PubMed] [Google Scholar]
- 14.Rogatsch H, Bonatti H, Menet A, Larcher C, Feichtinger H, Dirnhofer S. Epstein-Barr virus-associated multicentric leiomyosarcoma in an adult patient after heart transplantation: case report and review of the literature. Am J Surg Pathol. 2000;24:614–621. doi: 10.1097/00000478-200004000-00018. [DOI] [PubMed] [Google Scholar]
- 15.Conrad A, Brunet AS, Hervieu V, Chauvet C, Buron F, Collardeau-Frachon S, Rivet C, Cassier P, Testelin S, Lachaux A, Morelon E, Thaunat O. Epstein-Barr virus-associated smooth muscle tumors in a composite tissue allograft and a pediatric liver transplant recipient. Transpl Infect Dis. 2013;15:E182–186. doi: 10.1111/tid.12126. [DOI] [PubMed] [Google Scholar]
- 16.Deyrup AT, Lee VK, Hill CE, Cheuk W, Toh HC, Kesavan S, Chan EW, Weiss SW. Epstein-Barr virus-associated smooth muscle tumors are distinctive mesenchymal tumors reflecting multiple infection events: a clinicopathologic and molecular analysis of 29 tumors from 19 patients. Am J Surg Pathol. 2006;30:75–82. doi: 10.1097/01.pas.0000178088.69394.7b. [DOI] [PubMed] [Google Scholar]
- 17.Rougemont AL, Alfieri C, Fabre M, Gorska-Flipot I, Papp E, Champagne J, Phan V, Fournet JC, Sartelet H. Atypical Epstein-Barr virus (EBV) latent protein expression in EBV-associated smooth muscle tumours occurring in paediatric transplant recipients. Histopathology. 2008;53:363–367. doi: 10.1111/j.1365-2559.2008.03086.x. [DOI] [PubMed] [Google Scholar]
- 18.Jossen J, Chu J, Hotchkiss H, Wistinghausen B, Iyer K, Magid M, Kamath A, Roayaie S, Arnon R. Epstein-Barr virus-associated smooth muscle tumors in children following solid organ transplantation: a review. Pediatr Transplant. 2015;19:235–243. doi: 10.1111/petr.12426. [DOI] [PubMed] [Google Scholar]
- 19.Hayase E, Fujimoto K, Mitsuhashi T, Hatanaka Y, Yoshida M, Takemura R, Iwasaki J, Shiratori S, Sugita J, Kondo T, Tanaka J, Imamura M, Matsuno Y, Teshima T. Epstein-barr virus-associated smooth muscle tumors after bone marrow transplantation. Transplantation. 2014;97:e1–3. doi: 10.1097/01.TP.0000437912.60638.23. [DOI] [PubMed] [Google Scholar]
- 20.Boudjemaa S, Boman F, Guigonis V, Boccon-Gibod L. Brain involvement in multicentric Epstein-Barr virus-associated smooth muscle tumours in a child after kidney transplantation. Virchows Arch. 2004;444:387–391. doi: 10.1007/s00428-004-0975-7. [DOI] [PubMed] [Google Scholar]
- 21.Fitzsimmons L, Kelly GL. EBV and apoptosis: the viral master regulator of cell fate? Viruses. 2017;9 doi: 10.3390/v9110339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lara J, Cohen M, De Matteo E, Aversa L, Preciado MV, Chabay P. Epstein-Barr virus (EBV) association and latency profile in pediatric Burkitt’s lymphoma: experience of a single institution in Argentina. J Med Virol. 2014;86:845–850. doi: 10.1002/jmv.23737. [DOI] [PubMed] [Google Scholar]
- 23.Renouf B, Hollville E, Pujals A, Tetaud C, Garibal J, Wiels J. Activation of p53 by MDM2 antagonists has differential apoptotic effects on Epstein-Barr virus (EBV)-positive and EBV-negative Burkitt’s lymphoma cells. Leukemia. 2009;23:1557–1563. doi: 10.1038/leu.2009.92. [DOI] [PubMed] [Google Scholar]
- 24.Kim D, Ko Y, Suh Y, Koo H, Huh J, Lee W. Characteristics of Epstein-Barr virus associated childhood non-Hodgkin’s lymphoma in the Republic of Korea. Virchows Arch. 2005;447:593–596. doi: 10.1007/s00428-005-1277-4. [DOI] [PubMed] [Google Scholar]
- 25.Hamilton-Dutoit SJ, Rea D, Raphael M, Sandvej K, Delecluse HJ, Gisselbrecht C, Marelle L, van Krieken HJ, Pallesen G. Epstein-Barr virus-latent gene expression and tumor cell phenotype in acquired immunodeficiency syndrome-related non-Hodgkin’s lymphoma. Correlation of lymphoma phenotype with three distinct patterns of viral latency. Am J Pathol. 1993;143:1072–1085. [PMC free article] [PubMed] [Google Scholar]
- 26.Shen Q, Feng W, Long MS, Duan X, Jaijakul S, Arias CA, Brown RE, Zhao B. Multicentric hepatic EBV-associated smooth muscle tumors in an AIDS patient: a case report, investigation of mTOR activation and review of the literature. Int J Clin Exp Pathol. 2011;4:421–429. [PMC free article] [PubMed] [Google Scholar]
- 27.Purgina B, Rao UN, Miettinen M, Pantanowitz L. AIDS-related EBV-associated smooth muscle tumors: a review of 64 published cases. Patholog Res Int. 2011;2011:561548. doi: 10.4061/2011/561548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Deyrup AT. Epstein-Barr virus-associated epithelial and mesenchymal neoplasms. Hum Pathol. 2008;39:473–483. doi: 10.1016/j.humpath.2007.10.030. [DOI] [PubMed] [Google Scholar]
- 29.Magg T, Schober T, Walz C, Ley-Zaporozhan J, Facchetti F, Klein C, Hauck F. Epstein-barr virus(+) smooth muscle tumors as manifestation of primary immunodeficiency disorders. Front Immunol. 2018;9:368. doi: 10.3389/fimmu.2018.00368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Teiken K, Kuehnel M, Rehkaemper J, Kreipe H, Laenger F, Hussein K, Jonigk D. Non-canonical WNT6/WNT10A signal factor expression in EBV+ post-transplant smooth muscle tumors. Clin Sarcoma Res. 2018;8:10. doi: 10.1186/s13569-018-0096-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Petersson F. Epstein-Barr virus-associated smooth muscle tumor-report of 3 tumors including 1 intracerebral case with a prominent intratumoral B-lymphocytic component and plasma cells. Ann Diagn Pathol. 2013;17:91–98. doi: 10.1016/j.anndiagpath.2012.07.007. [DOI] [PubMed] [Google Scholar]
- 32.Moody CA, Scott RS, Amirghahari N, Nathan CO, Young LS, Dawson CW, Sixbey JW. Modulation of the cell growth regulator mTOR by Epstein-Barr virus-encoded LMP2A. J Virol. 2005;79:5499–5506. doi: 10.1128/JVI.79.9.5499-5506.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.To KF, Lai FM, Wang AY, Leung CB, Choi PC, Szeto CC, Lui SF, Yu AW, Li PK. Posttransplant Epstein-Barr virus-associated myogenic tumors involving bone. Cancer. 2000;89:467–472. [PubMed] [Google Scholar]
- 34.Komano J, Maruo S, Kurozumi K, Oda T, Takada K. Oncogenic role of Epstein-Barr virus-encoded RNAs in Burkitt’s lymphoma cell line Akata. J Virol. 1999;73:9827–9831. doi: 10.1128/jvi.73.12.9827-9831.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]