

Abstract
Background
This is one of a series of reviews of methods of cervical ripening and labour induction. The use of complementary therapies is increasing. Women may look to complementary therapies during pregnancy and childbirth to be used alongside conventional medical practice. Acupuncture involves the insertion of very fine needles into specific points of the body. Acupressure is using the thumbs or fingers to apply pressure to specific points. The limited observational studies to date suggest acupuncture for induction of labour has no known adverse effects to the fetus, and may be effective. However, the evidence regarding the clinical effectiveness of this technique is limited.
Objectives
To determine, from the best available evidence, the effectiveness and safety of acupuncture and acupressure for third trimester cervical ripening or induction of labour.
Search methods
We searched the Cochrane Pregnancy and Childbirth Group's Trials Register (30 November 2016), PubMed (1966 to 25 November 2016), ProQuest Dissertations & Theses (25 November 2016), CINAHL (25 November 2016), Embase (25 November 2016), the WHO International Clinical Trials Registry Portal (ICTRP) (3 October 2016), and bibliographies of relevant papers.
Selection criteria
Randomised controlled trials comparing acupuncture or acupressure, used for third trimester cervical ripening or labour induction, with placebo/no treatment or other methods on a predefined list of labour induction methods.
Data collection and analysis
Two review authors independently assessed trials for inclusion and risk of bias, extracted data, and checked them for accuracy. The quality of the evidence was assessed using GRADE.
Main results
This updated review includes 22 trials, reporting on 3456 women. The trials using manual or electro‐acupuncture were compared with usual care (eight trials, 760 women), sweeping of membranes (one trial, 207 women), or sham controls (seven trials, 729 women). Trials using acupressure were compared with usual care (two trials, 151 women) or sham controls (two trials, 239 women). Many studies had a moderate risk of bias.
Overall, few trials reported on primary outcomes. No trial reported vaginal delivery not achieved within 24 hours and uterine hyperstimulation with fetal heart rate (FHR) changes. Serious maternal and neonatal death or morbidity were only reported under acupuncture versus sham control.
Acupuncture versus sham control
There was no clear difference in caesarean sections between groups (average risk ratio (RR) 0.80, 95% confidence interval (CI) 0.56 to 1.15, eight trials, 789 women; high‐quality evidence). There were no reports of maternal death or perinatal death in the one trial that reported this outcome. There was evidence of a benefit from acupuncture in improving cervical readiness for labour (mean difference (MD) 0.40, 95% CI 0.11 to 0.69, one trial, 125 women), as measured by cervical maturity within 24 hours using Bishop's score. There was no evidence of a difference between groups for oxytocin augmentation, epidural analgesia, instrumental vaginal birth, meconium‐stained liquor, Apgar score < 7 at five minutes, neonatal intensive care admission, maternal infection, postpartum bleeding greater than 500 mL, time from the trial to time of birth, use of induction methods, length of labour, and spontaneous vaginal birth.
Acupuncture versus usual care
There was no clear difference in caesarean sections between groups (average RR 0.77, 95% CI 0.51 to 1.17, eight trials, 760 women; low‐quality evidence). There was an increase in cervical maturation for the acupuncture (electro) group compared with control (MD 1.30, 95% CI 0.11 to 2.49, one trial, 67 women) and a shorter length of labour (minutes) in the usual care group compared to electro‐acupuncture (MD 124.00, 95% CI 37.39 to 210.61, one trial, 67 women).
There appeared be a differential effect according to type of acupuncture based on subgroup analysis. Electro‐acupuncture appeared to have more of an effect than manual acupuncture for the outcomes caesarean section (CS), and instrumental vaginal and spontaneous vaginal birth. It decreased the rate of CS (average RR 0.54, 95% CI 0.37 to 0.80, 3 trials, 327 women), increased the rate of instrumental vaginal birth (average RR 2.30, 95%CI 1.15 to 4.60, two trials, 271 women), and increased the rate of spontaneous vaginal birth (average RR 2.06, 95% CI 1.20 to 3.56, one trial, 72 women). However, subgroup analyses are observational in nature and so results should be interpreted with caution.
There were no clear differences between groups for other outcomes: oxytocin augmentation, use of epidural analgesia, Apgar score < 7 at 5 minutes, neonatal intensive care admission, maternal infection, perineal tear, fetal infection, maternal satisfaction, use of other induction methods, and postpartum bleeding greater than 500 mL.
Acupuncture versus sweeping if fetal membranes
One trial of acupuncture versus sweeping of fetal membranes showed no clear differences between groups in caesarean sections (RR 0.64, 95% CI 0.34 to 1.22, one trial, 207 women, moderate‐quality evidence), need for augmentation, epidural analgesia, instrumental vaginal birth, Apgar score < 7 at 5 minutes, neonatal intensive care admission, and postpartum bleeding greater than 500 mL.
Acupressure versus sham control
There was no evidence of benefit from acupressure in reducing caesarean sections compared to control (RR, 0.94, 95% CI 0.68 to 1.30, two trials, 239 women, moderate‐quality evidence). There was no evidence of a clear benefit in reduced oxytocin augmentation, instrumental vaginal birth, meconium‐stained liquor, time from trial intervention to birth of the baby, and spontaneous vaginal birth.
Acupressure versus usual care
There was no evidence of benefit from acupressure in reducing caesarean sections compared to usual care (RR 1.02, 95% CI 0.68 to 1.53, two trials, 151 women, moderate‐quality evidence). There was no evidence of a clear benefit in reduced epidural analgesia, Apgar score < 7 at 5 minutes, admission to neonatal intensive care, time from trial intervention to birth of the baby, use of other induction methods, and spontaneous vaginal birth.
Authors' conclusions
Overall, there was no clear benefit from acupuncture or acupressure in reducing caesarean section rate. The quality of the evidence varied between low to high. Few trials reported on neonatal morbidity or maternal mortality outcomes. Acupuncture showed some benefit in improving cervical maturity, however, more well‐designed trials are needed. Future trials could include clinically relevant safety outcomes.
Plain language summary
Acupuncture or acupressure for induction of labour
What is the issue?
Induction of labour is offered to pregnant women when it is thought the outcome will be better for the mother or her baby if the pregnancy does not continue and the baby is born. Common reasons for induction include the pregnancy going beyond the due date, pre‐term or pre‐labour rupture of the membranes, and concerns about the health of the mother or baby such as pre‐eclampsia or poor growth of the baby. Some women look to using complementary therapies alongside conventional medical practice for induction. Acupuncture involves the insertion of fine needles into specific points of the body while acupressure involves using the thumbs or fingers to apply pressure to specific points. Both have been used to help soften and dilate the cervix with onset of labour contractions. They may provide a way of reducing labour pain and avoiding a medical induction with other methods such as prostaglandins.
Why is this important?
Medical inductions can have significant side effects. Many women therefore choose complementary and alternative methods to bring on labour. Acupuncture is practiced by many midwives together with usual care, and early studies have suggested a benefit from acupuncture.
What evidence did we find?
In October 2016, we searched for evidence from randomised controlled trials on the effectiveness and safety of acupuncture. We identified eight additional trials that were eligible for the review since the last version of the review in 2013. In total, we found 22 trials which reported on 3456 pregnant women. The authors rated most of the trials as having moderate risk of bias.
Moderate to high‐quality evidence found that acupuncture and acupressure did not reduce caesarean sections.
Acupuncture may promote a more favourable state of the cervix within 24 hours in the two trials (192 women) that looked at this. Only one trial reported on serious outcomes for the mother or her baby, finding no serious incidents in either the acupuncture or the control group (low‐quality evidence).
What does this mean?
Acupuncture and acupressure do not appear to reduce the need for caesarean section but may increase the readiness of the cervix for labour. Acupressure did not help in any of the outcomes we examined in this review. The trials varied in the delivery of acupuncture and acupressure, the comparison groups, and the outcomes looked at. These variations mean that we have to be careful in how we interpret the findings. More studies are needed to determine if acupuncture or acupressure increases the number of women who experience vaginal deliveries within 24 hours and to examine the safety of acupuncture and acupressure.
Summary of findings
Background
Description of the condition
Sometimes it is necessary to bring on labour artificially because of safety concerns for the mother or baby. This review is one of a series of reviews of methods of labour induction using a standardised protocol. For more detailed information on the rationale for this methodological approach, please refer to the currently published 'generic' protocol (Hofmeyr 2009). The generic protocol describes how a number of standardised reviews will be combined to compare various methods of preparing the cervix of the uterus and inducing labour.
Description of the intervention
The use of complementary and alternative medicine (CM) has become popular with consumers worldwide. A recent review of 14 studies with large sample sizes (n > 200) on the use of CM in pregnancy identified a prevalence rate ranging from 1% to 87% (with nine falling between 20% and 60%) (Adams 2009). The review identified use of various complementary therapies including acupuncture and acupressure, aromatherapy, massage, yoga, homeopathy, and chiropractic care. The review also showed that many pregnant women had used more than one complementary product or service (Adams 2009). Some women look to alternative therapies during pregnancy and childbirth to be used alongside conventional medical practice. There is evidence of midwives having positive views towards CM, and seeing a role of CM for supporting women in labour and birth as positive (Levett 2016a). In the United Kingdom, a recent survey found a wide variety of CM therapies are recommended to pregnant women by approximately a third of healthcare professionals (Stewart 2014). For some women with a prolonged pregnancy, an induction of labour may be perceived to intervene in the natural process of pregnancy, and may drastically change their expected plan of care during pregnancy. The reasons why pregnant women are interested in using complementary therapies to ripen the cervix and/or induce labour is an important question and needs to be answered when evaluating new options of care.
Acupuncture has been used for more than two thousand years in China and Japan. The diagnosis and treatment prescribed by traditional Chinese medicine (TCM) is influenced by the systems of medicine and philosophy of ancient China. Acupuncture involves the insertion of fine needles into the skin and underlying tissues at precise points on the body. The needle can be left alone, stimulated by turning in various ways, or stimulated by electricity. Electro‐acupuncture involves the use of electricity to stimulate the acupuncture point. To do this, a needle is inserted and a terminal is attached to the handle, while the other terminal is connected to a second needle or neutral electrode. Acupressure uses the same points as acupuncture but applies manual pressure, usually with the finger or thumb, on these points rather than the insertion of a needle. Laser acupuncture is a non‐penetrative form of acupuncture, which uses low power laser light to stimulate acupuncture points. Over time, different styles of acupuncture have been practiced by acupuncturists. Acupuncture treatment is composed of needling aspects (choice of points and needling techniques), specific components relating to the style of diagnosis and treatment used, and generic needling components not specific to acupuncture such as belief, time, and attention given to the patient.
In parts of Europe and Asia, acupuncture and acupressure have been described as methods to alleviate labour pains, and ripen the cervix. More recently, they have been used to stimulate the onset of labour.
Three case series have documented the role of acupuncture for the induction of labour (Tsuei 1974; Tsuei 1977; Yip 1976). Induction of labour using electro‐acupuncture has been reported by Yip 1976. Labour was successfully induced in 21 of the 31 women, with pregnancy duration ranging from 38 to 42 weeks. The pattern of uterine activity was similar to that of normal labour. In a second study, acupuncture with and without electrical stimulation was used to induce labour in 12 pregnant women with a gestational age from 19 to 43 weeks (Tsuei 1974). The success rate was 83% and average induction to delivery time was 13.1 hours. In the third study, 34 term and post‐term women and seven women with intrauterine fetal deaths were induced using electro‐acupuncture. Labour was successfully induced in 32 (78%) women (Tsuei 1977). The limited observational studies to date have suggested that acupuncture for induction of labour appears safe, has no known adverse effects to the fetus, and may be effective.
Two nonrandomised trials have examined whether acupuncture could initiate contractions in women at term (Kubista 1975: Theobald 1973). In the trial by Theobald (Theobald 1973), four electrodes were applied to the skin of the abdomen to induce labour in the treatment group. Treatment was given to 27 women and compared with 102 women who were controls. In the treatment group, 20 (77%) women gave birth on or up to four days before the estimated date of confinement, compared with 47 (46%) in the control group. In the second trial, electro‐acupuncture was administered to 35 women, and 35 women received no electro‐acupuncture. An increase in the intensity of labour contraction frequency was observed in 31 women in the treatment group. In the control group, no increase in labour activity was observed (Kubista 1975).
How the intervention might work
The mechanism underlying acupuncture and acupressure to induce labour is speculative at this stage but may involve stimulation of the uterus by hormonal changes or by the nervous system. In animal studies, low frequency electrical stimulation of the neuro‐hypophyseal system (the posterior lobe of the pituitary gland) induces the secretion of oxytocin. Parasympathetic (the system in the body that is responsible for bodily functions at rest) stimulation close to term has been shown to have an influence on the uterus (Bell 1972). Stimulation of acupuncture points is known to increase the discharge of thalamic nuclei (an increase in firing of the neurons in the thalamus) and the hypothalamic anterior pituitary system (the area of the brain that links both the nervous and endocrine system) (Liao 1979). It is hypothesised that acupuncture neuronal (related to neurons) stimulation may increase uterine contractility either by central oxytocin release or by parasympathetic stimulation of the uterus (Tempfeer 1998).
Why it is important to do this review
Induction of labour traditionally involves mechanical means (membrane sweeping, intrauterine catheter, artificial rupture of membranes) or pharmacological means (prostaglandin or synthetic oxytocin). Some women may seek to avoid these methods of induction, finding them uncomfortable, unacceptable, or both. There are risks and benefits associated with all these procedures. While membrane sweeping may result in women going into labour, softening the cervix and reducing the need for induction (Boulvain 2005), it may also be painful and/or not successful, and uncomplicated vaginal bleeding may occur following the procedure (De Miranda 2006). While membrane sweeping is not pharmacological, it needs to be undertaken by a registered midwife or doctor. Other mechanical or pharmacological means of induction of labour may lead to increased intervention in birth and morbidity for women (Khireddine 2013).
This review is one of a series of reviews of methods of labour induction using a standardised protocol. For more detailed information on the rationale for this methodological approach, please refer to the currently published protocol (Hofmeyr 2009).
Objectives
To determine, from the best available evidence, the effectiveness and safety of acupuncture and acupressure for third trimester cervical ripening or induction of labour.
Methods
Criteria for considering studies for this review
Types of studies
Randomised or quasi randomised controlled trials comparing manual, laser or electro‐acupuncture or acupressure for cervical ripening or labour induction, with placebo/no treatment, sham acupuncture/acupressure or other methods listed on a predefined list of methods of labour induction; the trials included some form of random allocation to either group. Abstracts and cross‐over trials were not included. Cluster‐randomised trials were included.
The control group in a trial of acupuncture can involve sham (mock) acupuncture where the needles are inserted away from the usual location, with the depth and needle stimulation being the same. Or alternatively, minimal acupuncture which involves needles being inserted away from the usual location, with very shallow needling and very slight stimulation, or the use of the noninvasive placebo needle (Streitberger 1998).
Types of participants
Pregnant women carrying a viable fetus due for third trimester induction of labour. We planned to use subgroup analysis for any possible differences in the effect of interventions in these groups.
Types of interventions
Manual, laser, or electro‐acupuncture or acupressure compared with placebo, no treatment, sham acupuncture/acupressure, or any other method on a predefined list of methods of labour induction, as detailed below.
To avoid duplication of data in a series of reviews on interventions for labour induction, the labour induction methods were listed in a specific order, from one to 27, as outlined below. The methods for these reviews are described in the generic protocol for cervical ripening and labour induction in late pregnancy (Hofmeyr 2009). Each review included comparisons between one of the methods (from two to 26) with only those methods above it on the list.
Thus, this review of acupuncture (number 20 on the list) could include comparisons with any of the following: (1) placebo/no treatment; (2) vaginal prostaglandins; (3) intracervical prostaglandins; (4) intravenous oxytocin; (5) amniotomy; (6) intravenous oxytocin with amniotomy; (7) vaginal misoprostol; (8) oral misoprostol; (9) mechanical methods including extra‐amniotic Foley catheter; (10) membrane sweeping; (11) extra‐amniotic prostaglandins (12) intravenous prostaglandins; (13) oral prostaglandins; (14) mifepristone; (15) oestrogens with or without amniotomy; (16) corticosteroids; (17) relaxin; (18) hyaluronidase; (19) castor oil, bath, and/or enema.
The current list is as follows:
(1) placebo/no treatment; (2) vaginal prostaglandins (Kelly 2009); (3) intracervical prostaglandins (Boulvain 2008); (4) intravenous oxytocin (Alfirevic 2009); (5) amniotomy (Bricker 2000); (6) intravenous oxytocin with amniotomy (Howarth 2001; Bimbashi 2012); (7) vaginal misoprostol (Hofmeyr 2010); (8) oral misoprostol (Alfirevic 2006); (9) mechanical methods including extra‐amniotic Foley catheter (Jozwiak 2012); (10) membrane sweeping (Boulvain 2005); (11) extra‐amniotic prostaglandins (Hutton 2001); (12) intravenous prostaglandins (Luckas 2000); (13) oral prostaglandins (French 2001); (14) mifepristone (Hapangama 2009); (15) oestrogens with or without amniotomy (Thomas 2001); (16) corticosteroids (Kavanagh 2006b); (17) relaxin (Kelly 2001b); (18) hyaluronidase (Kavanagh 2006a); (19) castor oil, bath, and/or enema (Kelly 2013); (20) acupuncture (this review); (21) breast stimulation (Kavanagh 2005); (22) sexual intercourse (Kavanagh 2001); (23) homoeopathic methods (Smith 2003); (24) nitric oxide donors (Ghosh 2016); (25) buccal or sublingual misoprostol (Muzonzini 2004); (26) hypnosis (protocol in progress); (27) other methods for induction of labour.
Types of outcome measures
Primary outcomes
Clinically relevant outcomes for trials of methods of cervical ripening/labour induction were prespecified by two authors of labour induction reviews (Justus Hofmeyr and Zarko Alfirevic) (Hofmeyr 2009). Differences were settled by discussion.
Five primary outcomes were chosen as being most representative of the clinically important measures of effectiveness and complications. It was agreed that subgroup analyses would be limited to the primary outcomes: (1) vaginal delivery not achieved within 24 hours; (2) uterine hyperstimulation with fetal heart rate (FHR) changes; (3) caesarean section; (4) serious neonatal morbidity or perinatal death (e.g. seizures, birth asphyxia defined by trialists, neonatal encephalopathy, disability in childhood); (5) serious maternal morbidity or death (e.g. uterine rupture, admission to intensive care unit, septicaemia).
Perinatal and maternal morbidity and mortality are composite outcomes. This is not an ideal solution because some components are clearly less severe than others. It is possible for one intervention to cause more deaths but less severe morbidity. However, in the context of labour induction at term, this is unlikely. All these events will be rare, and a modest change in their incidence will be easier to detect if composite outcomes are presented. The incidence of individual components were explored as secondary outcomes (see below).
Secondary outcomes
Secondary outcomes related to measures of effectiveness, complications and satisfaction.
Measures of effectiveness: (6) cervix unfavourable/unchanged after 12 to 24 hours; (7) oxytocin augmentation.
Complications: (8) uterine hyperstimulation without FHR changes; (9) uterine rupture; (10) epidural analgesia; (11) instrumental vaginal delivery; (12) meconium‐stained liquor; (13) Apgar score less than seven at five minutes; (14) neonatal intensive care unit admission; (15) neonatal encephalopathy; (16) perinatal death; (17) disability in childhood; (18) maternal side effects (all); defined as infection (maternal and fetal), perineal tear; (19) maternal nausea; (20) maternal vomiting; (21) maternal diarrhoea; (22) other maternal side effects; (23) postpartum haemorrhage (as defined by the trial authors); (24) serious maternal complications (e.g. intensive care unit admission, septicaemia but excluding uterine rupture); (25) maternal death.
Measures of satisfaction: (26) woman not satisfied; (27) caregiver not satisfied.
Acupuncture‐specific outcomes: (28) use of other induction methods; (29) time from trial intervention to the birth of the baby; (30) length of labour; (31) spontaneous vaginal delivery.
While all the above outcomes were sought, only those with data appeared in the analysis tables.
The terminology of uterine hyperstimulation is problematic (Curtis 1987). In the reviews, we used the term 'uterine hyperstimulation without FHR changes' to include uterine tachysystole (more than five contractions per 10 minutes for at least 20 minutes) and uterine hypersystole/hypertonus (a contraction lasting at least two minutes) and 'uterine hyperstimulation with FHR changes' to denote uterine hyperstimulation syndrome (tachysystole or hypersystole with FHR changes such as persistent decelerations, tachycardia, or decreased short‐term variability).
Search methods for identification of studies
The following methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Electronic searches
We searched Cochrane Pregnancy and Childbirth’s Trials Register by contacting their Information Specialist (30 November 2016).
The Register is a database containing over 24,000 reports of controlled trials in the field of pregnancy and childbirth. For full search methods used to populate Pregnancy and Childbirth’s Trials Register including the detailed search strategies for CENTRAL, MEDLINE, Embase and CINAHL, the list of handsearched journals and conference proceedings, and the list of journals reviewed via the current awareness service, please follow this link to the editorial information about the Cochrane Pregnancy and Childbirth in the Cochrane Library and select the ‘Specialised Register’ section from the options on the left side of the screen.
Briefly, Cochrane Pregnancy and Childbirth’s Trials Register is maintained by their Information Specialist and contains trials identified from:
monthly searches of the Cochrane Central Register of Controlled Trials (CENTRAL);
weekly searches of MEDLINE (Ovid);
weekly searches of Embase (Ovid);
monthly searches of CINAHL (EBSCO);
handsearches of 30 journals and the proceedings of major conferences;
weekly current awareness alerts for a further 44 journals plus monthly BioMed Central email alerts.
Search results are screened by two people and the full text of all relevant trial reports identified through the searching activities described above is reviewed. Based on the intervention described, each trial report is assigned a number that corresponds to a specific Pregnancy and Childbirth review topic (or topics), and is then added to the Register. The Information Specialist searches the Register for each review using this topic number rather than keywords. This results in a more specific search set which has been fully accounted for in the relevant review sections (Included studies; Excluded studies; Ongoing studies).
In addition, we searched PubMed (1966 to 25 November 2016), ProQuest Dissertations & Theses (25 November 2016), CINAHL (25 November 2016), Embase (25 November 2016), the WHO International Clinical Trials Registry Portal (ICTRP) (3 October 2016), and bibliographies of relevant papers. See Appendix 1 for search strategies used.
Searching other resources
We searched the reference lists of retrieved studies.
We did not apply any language or date restrictions.
Data collection and analysis
For methods used in the previous version of this review, seeSmith 2013.
For this update, the following methods were used for assessing the reports that were identified as a result of the updated search.
The following methods section of this review is based on a standard template used by Cochrane Pregnancy and Childbirth.
Selection of studies
Two review authors independently assessed for inclusion all the potential studies identified as a result of the search strategy. We resolved any disagreement through discussion or, if required, we consulted the third review author.
Data extraction and management
We designed a form to extract data. For eligible studies, two review authors extracted the data using the agreed form. We resolved discrepancies through discussion or, if required, we consulted the third review author. Data were entered into Review Manager software (RevMan 2014) and checked for accuracy.
When information regarding any of the above was unclear, we planned to contact authors of the original reports to provide further details.
Assessment of risk of bias in included studies
Two review authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Any disagreement was resolved by discussion or by involving a third assessor.
(1) Random sequence generation (checking for possible selection bias)
We described for each included study the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups.
We assessed the method as:
low risk of bias (any truly random process, e.g. random number table; computer random number generator);
high risk of bias (any nonrandom process, e.g. odd or even date of birth; hospital or clinic record number);
unclear risk of bias.
(2) Allocation concealment (checking for possible selection bias)
We described for each included study the method used to conceal allocation to interventions prior to assignment and assessed whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment.
We assessed the methods as:
low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes);
high risk of bias (open random allocation; unsealed or non‐opaque envelopes, alternation; date of birth);
unclear risk of bias.
(3.1) Blinding of participants and personnel (checking for possible performance bias)
We described for each included study the methods used, if any, to blind study participants and personnel from knowledge of which intervention a participant received. We considered that studies were at low risk of bias if they were blinded, or if we judged that the lack of blinding unlikely to affect results. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed the methods as:
low, high, or unclear risk of bias for participants;
low, high, or unclear risk of bias for personnel.
(3.2) Blinding of outcome assessment (checking for possible detection bias)
We described for each included study the methods used, if any, to blind outcome assessors from knowledge of which intervention a participant received. We assessed blinding separately for different outcomes or classes of outcomes.
We assessed methods used to blind outcome assessment as:
low, high or unclear risk of bias.
(4) Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data)
We described for each included study, and for each outcome or class of outcomes, the completeness of data including attrition and exclusions from the analysis. We stated whether attrition and exclusions were reported and the numbers included in the analysis at each stage (compared with the total randomised participants), reasons for attrition or exclusion where reported, and whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported, or could be supplied by the trial authors, we planned to reinclude missing data in the analyses which we undertook.
We assessed methods as:
low risk of bias (e.g. no missing outcome data; missing outcome data balanced across groups);
high risk of bias (e.g. numbers or reasons for missing data imbalanced across groups; ‘as treated’ analysis done with substantial departure of intervention received from that assigned at randomisation);
unclear risk of bias.
(5) Selective reporting (checking for reporting bias)
We described for each included study how we investigated the possibility of selective outcome reporting bias and what we found.
We assessed the methods as:
low risk of bias (where it was clear that all of the study’s prespecified outcomes and all expected outcomes of interest to the review had been reported);
high risk of bias (where not all the study’s prespecified outcomes had been reported; one or more reported primary outcomes were not prespecified; outcomes of interest were reported incompletely and so could not be used; study failed to include results of a key outcome that would have been expected to have been reported);
unclear risk of bias.
(6) Other bias (checking for bias due to problems not covered by (1) to (5) above)
We described for each included study any important concerns we had about other possible sources of bias.
(7) Overall risk of bias
We made explicit judgements about whether studies were at high risk of bias, according to the criteria given in the Handbook (Higgins 2011). With reference to (1) to (6) above, we planned to assess the likely magnitude and direction of the bias and whether we considered it was likely to impact on the findings. In future updates, we will explore the impact of the level of bias through undertaking sensitivity analyses ‐ seeSensitivity analysis.
Assessment of the quality of the evidence using the GRADE approach
For this update, the quality of the evidence was assessed using the GRADE approach as outlined in the GRADE Handbook in order to assess the quality of the body of evidence relating to the following outcomes for the main comparisons: acupuncture compared to sham control; acupuncture compared to usual care; acupuncture compared to sweeping of fetal membranes; acupressure compared to sham control; and acupressure compare to usual care.
Vaginal delivery not achieved within 24 hours;
uterine hyperstimulation with FHR changes;
caesarean section;
serious neonatal morbidity or perinatal death;
serious maternal morbidity or death.
GRADEpro Guideline Development Tool was used to import data from Review Manager 5.3 (RevMan 2014) in order to create ’Summary of findings’ tables. A summary of the intervention effect and a measure of quality for each of the above outcomes was produced using the GRADE approach. The GRADE approach uses five considerations (study limitations, consistency of effect, imprecision, indirectness, and publication bias) to assess the quality of the body of evidence for each outcome. The evidence can be downgraded from 'high quality' by one level for serious (or by two levels for very serious) limitations, depending on assessments for risk of bias, indirectness of evidence, serious inconsistency, imprecision of effect estimates, or potential publication bias.
Measures of treatment effect
Dichotomous data
For dichotomous data, we presented results as summary risk ratios with 95% confidence intervals.
Continuous data
We used the mean difference if outcomes were measured in the same way between trials. We used the standardised mean difference to combine trials that measured the same outcome, but used different methods.
Unit of analysis issues
Cluster‐randomised trials
We planned to include cluster‐randomised trials in the analyses along with individually‐randomised trials. No cluster trials were included in this update. In future updates, if identified and eligible for inclusion, we will adjust either their sample sizes or standard errors, as appropriate, using the methods described in the Cochrane Handbook for Systematic Reviews of Interventions (Section 16.3.4 or 16.3.6), using an estimate of the intracluster correlation coefficient (ICC) derived from the trial (if possible), from a similar trial, or from a study of a similar population. If we use ICCs from other sources, we will report this and conduct sensitivity analyses to investigate the effect of variation in the ICC. If we identify both cluster‐randomised trials and individually‐randomised trials, we plan to synthesise the relevant information. We will consider it reasonable to combine the results from both if there is little heterogeneity between the study designs and the interaction between the effect of intervention and the choice of randomisation unit is considered to be unlikely.
We will also acknowledge heterogeneity in the randomisation unit and perform a subgroup analysis to investigate the effects of the randomisation unit.
Cross‐over trials
This study design was not eligible for inclusion due to the unclear washout period when using acupuncture.
Other unit of analyses issues
Trials with multiple arms were included and are described in the Characteristics of included studies. For example, acupuncture might be compared with sham acupuncture and with another arm where no acupuncture was delivered. If there were two acupuncture groups, data from both treatment arms were combined into one group. For studies with a sham control and no treatment control group, the shared intervention was divided evenly between groups as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Where outcomes were repeated measures, analysis of outcomes was undertaken at the end of the intervention.
Dealing with missing data
For included studies, levels of attrition were noted. In future updates, if more eligible studies are included, the impact of including studies with high levels of missing data in the overall assessment of treatment effect will be explored by using sensitivity analysis.
For all outcomes, analyses were carried out, as far as possible, on an intention‐to‐treat basis, i.e. we attempted to include all participants randomised to each group in the analyses. The denominator for each outcome in each trial was the number randomised minus any participants whose outcomes were known to be missing.
Assessment of heterogeneity
We assessed statistical heterogeneity in each meta‐analysis using the Tau², I² and Chi² statistics. We regarded heterogeneity as substantial if I² was greater than 30% and either Tau² was greater than zero, or there was a low P value (less than 0.10) in the Chi² test for heterogeneity. If we identified substantial heterogeneity (above 30%), we planned to explore it by prespecified subgroup analysis.
Assessment of reporting biases
In future updates, if there are 10 or more studies in the meta‐analysis we will investigate reporting biases (such as publication bias) using funnel plots. We will assess funnel plot asymmetry visually. If asymmetry is suggested by a visual assessment, we will perform exploratory analyses to investigate it.
Data synthesis
We carried out statistical analysis using the Review Manager software (RevMan 2014). We used fixed‐effect meta‐analysis for combining data where it was reasonable to assume that studies were estimating the same underlying treatment effect: i.e. where trials were examining the same intervention, and the trials’ populations and methods were judged sufficiently similar, or if the number of studies was small (less than three).
If there was clinical heterogeneity sufficient to expect that the underlying treatment effects differed between trials, or if substantial statistical heterogeneity was detected, we used random‐effects meta‐analysis to produce an overall summary if an average treatment effect across trials was considered clinically meaningful. The random‐effects summary was treated as the average range of possible treatment effects and we discussed the clinical implications of treatment effects differing between trials. If the average treatment effect was not clinically meaningful, we did not combine trials. If we used random‐effects analyses, the results were presented as the average treatment effect with 95% confidence intervals, and the estimates of Tau² and I².
Subgroup analysis and investigation of heterogeneity
If we identified substantial heterogeneity, we planned to investigate it using subgroup analyses and sensitivity analyses and to consider whether an overall summary was meaningful, and if it was, to undertake a random‐effects analysis. Subgroup analyses were not prespecified in the earlier version of the review (Smith 2004). We planned to carry out the following subgroup analyses:
Nulliparity versus multiparity;
cervix unfavourable, versus favourable versus undefined;
membranes intact or ruptured;
classical/traditional acupuncture versus single point therapy, or auricular acupuncture.
In addition, we planned to carry out the following subgroup analyses:
Trials that recruited and treated women prior to due date (< 40 weeks) versus those that treated women with a combination of pre and post‐date or post‐date alone;
trials that reported provided separate outcome data for primiparous and multiparous women.
We planned to use the following outcome in subgroup analyses: caesarean section.
However, in this update, none of subgroups specified above were analysed due to a lack of data in the prespecified subgroups.
We did carry out comparisons according to subgroups by type of intervention:
1. Manual acupuncture versus electro‐acupuncture, for all outcomes.
We assessed subgroup differences by interaction tests available within RevMan (RevMan 2014). We reported the results of subgroup analyses quoting the Chi² statistic and P value, and the interaction test I² value.
Sensitivity analysis
Where subgroup analysis failed to explain the heterogeneity, we planned to analyse the data using a random‐effects model. A priori, we planned to perform sensitivity analysis on the results to look at the possible contribution of: (1) differences in risk of bias with trials having a low risk of bias across four or more domains compared to all trials; and (2) publication bias by country. If publication bias was present, we planned to undertake a sensitivity analysis excluding trials from countries where there was a greater publication bias.
Results
Description of studies
See: Characteristics of included studies; Characteristics of excluded studies; Characteristics of studies awaiting classification.
Results of the search
Figure 1 outlines the search process.
1.
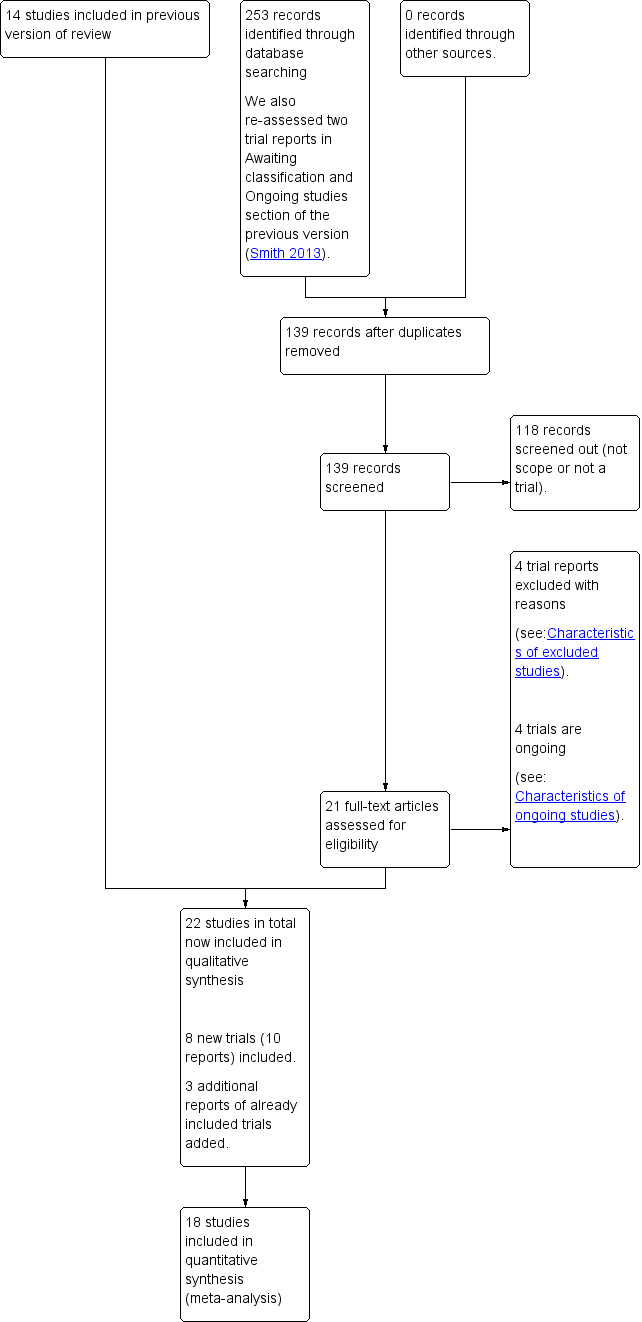
Study flow diagram.
The previous update of this review included 14 trials, and excluded eight trials. This updated review included 22 trials and excluded 12 trials. Eight new trials were included and four new trials were excluded. Four studies are classified as ongoing.
Included studies
Study design
All studies were parallel design. Seventeen trials had two groups (Ajori 2013; Alsharnoubi 2015; Gaudernack 2006; Gaudet 2008; Gregson 2015; Gribel 2011; Harper 2006; Long 1994; Martinez 2004; Modlock 2010; Mollart 2016; Neri 2014; Rabl 2001; Romer 2000; Selmer‐Olsen 2007; Smith 2008; Torkzahrani 2015), four trials had three groups (Andersen 2013; Asher 2009; Torkzahrani 2016; Tremeau 1992) and one trial had five groups (Mackenzie 2011). Eleven studies used sham controls (Ajori 2013; Alsharnoubi 2015; Asher 2009; Gaudet 2008; Gregson 2015; Mackenzie 2011; Modlock 2010; Romer 2000; Smith 2008; Torkzahrani 2016; Tremeau 1992), 15 trials used standard care (Andersen 2013; Asher 2009; Gaudernack 2006; Gribel 2011; Harper 2006; Long 1994; Mackenzie 2011; Martinez 2004; Mollart 2016; Neri 2014; Rabl 2001; Selmer‐Olsen 2007; Torkzahrani 2015; Torkzahrani 2016; Tremeau 1992) and one trial compared acupuncture with sweeping of the fetal membranes (Andersen 2013).
Samples sizes
Sample size of the included studies ranged from 16 (Gaudet 2008) to 553 (Romer 2000).
Study location and sources of women
Three studies were under taken in Iran (Ajori 2013; Torkzahrani 2015; Torkzahrani 2016). Two studies were undertaken in Australia (Mollart 2016; Smith 2008), Denmark (Andersen 2013; Modlock 2010), Norway (Gaudet 2008; Selmer‐Olsen 2007), the United States (Asher 2009; Harper 2006), and in the United Kingdom (Gregson 2015; Mackenzie 2011). One study was undertaken in Austria (Rabl 2001), Brazil (Gribel 2011), Canada (Gaudet 2008), China (Long 1994), Egypt (Alsharnoubi 2015), France (Tremeau 1992), Germany (Romer 2000), Italy (Neri 2014) and the Phillipines (Martinez 2004).
Dates of trials
The majority of the trials took place between the year 2003 to 2015: Ajori 2013 (2010 to 2011); Alsharnoubi 2015 (2013); Andersen 2013 (2007 to 2009); Asher 2009 (2005 to 2007); Gaudernack 2006 (2003 to 2005); Gaudet 2008 (2004 to 2005); Gregson 2015 (2012 to 2014); Gribel 2011 (2007 to 2009); Harper 2006 (2004 to 2005); Martinez 2004 (2003); Modlock 2010 (2005 to 2008); Mollart 2016 (2013); Selmer‐Olsen 2007 (2004 to 2006); Torkzahrani 2015 (2011 to 2012); Torkzahrani 2016 (2015). One study took place in 1990 (Tremeau 1992), and one lasted from 1998 to 2005 (Smith 2008). The duration of the studies ranged from five months (Alsharnoubi 2015) to seven years (Smith 2008). Five trials did not report their study dates (Long 1994; Mackenzie 2011; Neri 2014; Rabl 2001; Romer 2000).
Participants
Ten studies recruited nulliparous women only (Alsharnoubi 2015; Asher 2009; Gaudet 2008; Harper 2006; Mackenzie 2011; Mollart 2016; Romer 2000; Selmer‐Olsen 2007; Torkzahrani 2015; Torkzahrani 2016). Ten trials recruited both nulliparous and primiparous women (Ajori 2013; Andersen 2013; Gaudernack 2006; Gregson 2015; Gribel 2011; Modlock 2010; Neri 2014; Rabl 2001; Smith 2008; Tremeau 1992). Parity was unclear in two trials (Long 1994; Martinez 2004). Six studies included only women who were post‐date (> 40 weeks gestational age) (Andersen 2013; Gregson 2015; Modlock 2010; Mollart 2016; Neri 2014; Smith 2008) and seven studies included women both under and over 40 weeks gestational age (Ajori 2013; Asher 2009; Gaudet 2008; Harper 2006; Selmer‐Olsen 2007; Torkzahrani 2015; Torkzahrani 2016). Three studies (Romer 2000; Torkzahrani 2016; Tremeau 1992) included only women less than 40 weeks gestational age.
Types of interventions
Ten studies used manual acupuncture only (Ajori 2013; Asher 2009; Gaudernack 2006; Modlock 2010; Neri 2014; Rabl 2001; Romer 2000; Selmer‐Olsen 2007; Smith 2008; Tremeau 1992), one trial used laser acupuncture (Alsharnoubi 2015), one trial used electro‐acupuncture only (Gribel 2011), and three trials used manual and electro‐acupuncture (Andersen 2013; Gaudet 2008; Harper 2006). Acupressure was used in four trials (Gregson 2015; Mollart 2016; Torkzahrani 2015; Torkzahrani 2016). Gaudet 2008 used a combination of manual and nonactive electro‐stimulation for the control group.
Fixed points were used in 17 trials (Ajori 2013; Alsharnoubi 2015; Andersen 2013; Asher 2009; Gaudet 2008; Gregson 2015; Gribel 2011; Harper 2006; Mackenzie 2011; Modlock 2010; Mollart 2016; Neri 2014; Rabl 2001; Romer 2000; Torkzahrani 2015; Torkzahrani 2016; Tremeau 1992) and three trials used individualised treatment (Gaudernack 2006; Selmer‐Olsen 2007; Smith 2008). Details were unclear in two trials (Long 1994; Martinez 2004). There was significant variation in the acupuncture points used but frequent acupuncture points included; Stomach 36 (ST36), Liver 3 (LR3), Conception Vessel 4 (CV4), Three Heater 6 (TH6), Large Intestine 4 (LI4), Gall Bladder 41 (GB41), Kidney 6 (KI6), Spleen 6 (SP6), Heart 7 (HT7), and Lung 7 (LU7), Bladder 31 (UB31), Bladder 32 (UB32), Bladder 60 (UB60) Bladder 67 (UB67), Governing Vessel (GV20).
The number of treatments varied from three trials administering one treatment (Gaudernack 2006; Mackenzie 2011; Rabl 2001), six trials administering two treatments (Ajori 2013; Andersen 2013; Gaudet 2008; Modlock 2010; Selmer‐Olsen 2007; Smith 2008) and eight providing three or more (Alsharnoubi 2015; Asher 2009; Gribel 2011; Harper 2006; Mollart 2016; Neri 2014; Romer 2000; Tremeau 1992). The number of treatment sessions was not specified in five trials (Gregson 2015; Long 1994; Martinez 2004; Torkzahrani 2015; Torkzahrani 2016).
Outcome measures
Few trials reported on the primary outcomes relating to this review. Sixteen trials reported on caesarean section (Ajori 2013; Alsharnoubi 2015; Andersen 2013; Asher 2009; Gaudet 2008; Gregson 2015; Gribel 2011; Harper 2006; Mackenzie 2011; Modlock 2010; Mollart 2016; Neri 2014; Selmer‐Olsen 2007; Smith 2008; Torkzahrani 2016; Tremeau 1992), although all trials reported on a selection of the secondary outcomes included in this review.
Funding
Only seven trials provided details for their funding sources. Asher 2009 was funded by American Academy of Family Physicians, UNC Dept of Family Medicine, the NIH National Centre on Complementary and Alternative Medicine, and the UNC School of Medicine; Harper 2006 by the Bowes Cefalo Young Researcher Award and North Carolina Academic Alliance for Integrative medicine Pilot; Mackenzie 2011 by a grant from Oxfordshire Health Services Research Committee and the Uterine Contractility Trust Fund; Modlock 2010 by the Midwifery Union, Denmark, The Skejby Research Fund, Aase and Ejnar Danielsens Funds, Timber Merchant Vilhelm Bangs Fund and the County of Ringkjobing Research Fund; Mollart 2016 by the NSW Ministry of Health Nursing and Midwifery Office, Australian College of Midwives, NSW Branch and Central; Selmer‐Olsen 2007 by Sandvik forlag; and Smith 2008 was funded by the Australian National Health and Medical Research Council, the Women’s and Children’s Hospital Foundation, Adelaide, Australia.
Declarations of interest
Nine trials declared no conflicts of interest (Ajori 2013; Alsharnoubi 2015; Gribel 2011; Mackenzie 2011; Modlock 2010; Mollart 2016; Neri 2014; Rabl 2001; Torkzahrani 2016). The remaining studies did not report whether any conflicts of interest were present.
Excluded studies
Twelve studies were excluded; see Characteristics of excluded studies.
Four trials were excluded because they did not describe any form of randomisation (Dorr 1990; Kubista 1974; Li 1996; SSo 1979) and we were unable to obtain details from authors. One trial was excluded due to an evaluation of acupuncture on pain relief in labour (Bo 2006). Two trials reported on women already in labour (Liu 2012; Lyngso 2010). Three trials used a form of stimulation not relevant to this review (Aghamohammadi 2011; Dunn 1989; Teimoori 2015). One trial was excluded due to examining early mid trimester labour (Li 2007). Levett 2016b used a combination of interventions including yoga, acupressure and visualisation. Separating the effect of acupressure alone was not possible.
Risk of bias in included studies
See Figure 2 and Figure 3 for a graphical summary of the 'Risk of bias' assessment by authors of the included studies based on the six domains of bias. Two studies were at a low risk of bias on all domains (Gregson 2015; Smith 2008).
2.
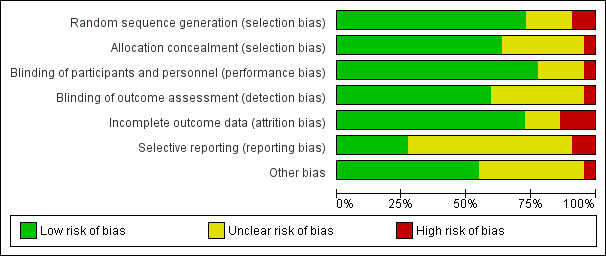
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
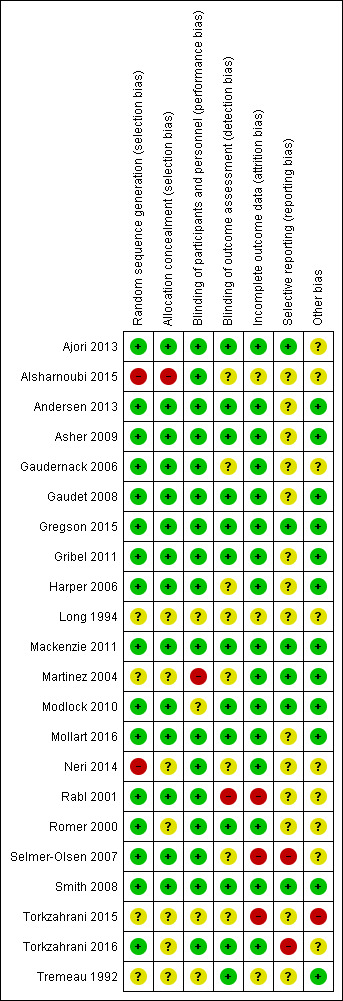
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Sixteen trials were rated at a low risk of bias for adequate generation of the randomisation sequence, generation of the randomisation schedule was unclear in four trials (Long 1994; Martinez 2004; Torkzahrani 2015; Tremeau 1992), and at high risk in two trials (Alsharnoubi 2015; Neri 2014). The method of concealment was high risk in one trial (Alsharnoubi 2015), at low risk in 14 trials, with insufficient reporting in seven trials (Long 1994; Martinez 2004; Neri 2014; Romer 2000; Torkzahrani 2015; Torkzahrani 2016; Tremeau 1992).
Blinding
Seventeen studies were at low risk of performance bias, with one trial having a high risk of bias (Martinez 2004), primarily because participants were not blind to group allocation in the studies using a standard care control. In the other four trials there was not enough information reported to be clear whether or not blinding had taken place (Long 1994; Modlock 2010; Torkzahrani 2015; Tremeau 1992). Detection bias was assessed at a low risk in 13 trials, one trial was assessed at high risk (Rabl 2001), and eight trials were assessed as unclear.
Incomplete outcome data
Sixteen trials were assessed at low risk of bias. Three trials were at high risk (Rabl 2001; Selmer‐Olsen 2007; Torkzahrani 2016). In the Rabl trial (Rabl 2001), there were 11 (20%) post‐randomisation exclusions and losses to follow‐up. There was an imbalance in the post‐randomisation exclusions (five in the treatment group and eight in the control group). The trial author was unable to provide outcome data on the 11 women who had been excluded from analyses. Risk was assessed as unclear in three trials (Alsharnoubi 2015; Long 1994; Tremeau 1992).
Selective reporting
The risk of selective reporting was assessed as low in six trials (Ajori 2013; Gregson 2015; Mackenzie 2011; Martinez 2004; Modlock 2010; Smith 2008), the risk of bias was unclear in 14 trials, and at high risk in two trials (Selmer‐Olsen 2007; Torkzahrani 2016).
Other potential sources of bias
The risk of bias was rated as low in 12 trials, high in one trial (Torkzahrani 2015) and unclear in the other 9 trials.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5
Summary of findings for the main comparison. Acupuncture compared to sham control for induction of labour.
| Acupuncture compared to sham control for induction of labour | ||||||
| Patient or population: women due for third trimester induction of labour Setting: hospital ward/clinic Intervention: acupuncture Comparison: sham control | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with sham control | Risk with Acupuncture | |||||
| Vaginal delivery not achieved within 24 hours ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Uterine hyperstimulation with FHR changes ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Caesarean section | Study population | RR 0.80 (0.56 to 1.15) | 789 (8 RCTs) | ⊕⊕⊕⊕ HIGH | No evidence of benefit for acupuncture | |
| 231 per 1,000 | 184 per 1,000 (129 to 265) | |||||
| Serious neonatal morbidity or death | Study population | not estimable | 364 (1 study) | No events | ||
| 0 per 1,000 | 0 per 1,000 (0 to 0) | |||||
| Serious maternal morbidity or death | Study population | not estimable | 364 (1 study) | No events | ||
| 0 per 1,000 | 0 per 1,000 (0 to 0) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; OR: Odds ratio; | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
Summary of findings 2. Acupuncture compared to usual care for induction of labour.
| Acupuncture compared to usual care for induction of labour | ||||||
| Patient or population: women due for third trimester induction of labour Setting: hospital ward/clinic Intervention: Acupuncture Comparison: usual care | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with usual care | Risk with Acupuncture | |||||
| Vaginal delivery not achieved within 24 hours ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Uterine hyperstimulation with FHR changes ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Caesarean section | Study population | average RR 0.77 (0.51 to 1.17) | 760 (8 RCTs) | ⊕⊕⊝⊝ LOW 1 2 | No evidence of benefit for acupuncture | |
| 211 per 1,000 | 162 per 1,000 (108 to 247) | |||||
| Serious maternal morbidity or death ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Serious neonatal morbidity or death ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
1 Downgraded one level: Three studies with high risk of bias in at least one domain of randomisation or blinding.
2 Downgraded one level: Substantial heterogeneity (I² = 42%).
Summary of findings 3. Acupuncture compared to sweeping of fetal membranes for induction of labour.
| Acupuncture compared to sweeping of fetal membranes for induction of labour | ||||||
| Patient or population: induction of labour Setting: hospital ward/clinic Intervention: Acupuncture Comparison: sweeping of fetal membranes | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with sweeping of fetal membranes | Risk with Acupuncture | |||||
| Vaginal delivery not achieved within 24 hours ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Uterine hyperstimulation with FHR changes ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Caesarean section | Study population | RR 0.64 (0.34 to 1.22) | 207 (1 RCT) | ⊕⊕⊕⊝ MODERATE 1 | No evidence of benefit for acupuncture | |
| 194 per 1,000 | 124 per 1,000 (66 to 237) | |||||
| Serious maternal morbidity or death ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Serious neonatal morbidity or death ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; OR: Odds ratio; | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded one level: Small sample size and wide confidence interval.
Summary of findings 4. Acupressure compared to sham control for induction of labour.
| Acupressure compared to sham control for induction of labour | ||||||
| Patient or population: women due for third trimester induction of labour Setting: hospital ward/clinic Intervention: Acupressure Comparison: sham control | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with sham control | Risk with Acupressure | |||||
| Vaginal delivery not achieved within 24 hours ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Uterine hyperstimulation with FHR changes ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Caesarean section | Study population | RR 0.94 (0.68 to 1.30) | 239 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 1 | No evidence of benefit for acupressure | |
| 391 per 1,000 | 368 per 1,000 (266 to 509) | |||||
| Serious maternal morbidity or death ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Serious neonatal morbidity or death ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; OR: Odds ratio; | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded one level: Small sample size.
Summary of findings 5. Acupressure compared to usual care for induction of labour.
| Acupressure compared to usual care for induction of labour | ||||||
| Patient or population: women due for third trimester induction of labour Setting: hospital ward/clinic Intervention: Acupressure Comparison: usual care | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with usual care | Risk with Acupressure | |||||
| Vaginal delivery not achieved within 24 hours ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Uterine hyperstimulation with FHR changes ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Caesarean section | Study population | RR 1.02 (0.68 to 1.53) | 151 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 1 | No evidence of benefit for acupressure | |
| 373 per 1,000 | 381 per 1,000 (254 to 571) | |||||
| Serious maternal morbidity or death ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Serious neonatal morbidity or death ‐ not reported | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; OR: Odds ratio; | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded one level: Small sample size.
This review included 22 trials of 3456 women, however we were only able to include data from 18 trials (2800 women) in the meta‐analysis.
Because data were not available about the post‐randomisation exclusions for the Rabl 2001 trial and an intention‐to‐treat analysis could not be undertaken, the results of this trial could not be incorporated into the meta‐analysis. Primary data from the Long 1994 trial could not be obtained and no data were included in the analysis. Martinez 2004 reported on no clinically relevant outcomes. Torkzahrani 2015 reported cervical changes at 48 hours onwards and could not be included in the meta‐analysis.
Studies that used a mixture of manual and electro‐acupuncture were classified as electro‐acupuncture in the subgroup analysis.
Comparison 1: Acupuncture versus sham control
Primary outcomes
Eight trials with 789 women reported on caesarean section and one trial with 364 women reported on serious neonatal morbidity. No trial reported on vaginal birth not achieved within 24 hours or uterine hyperstimulation with fetal heart rate (FHR) changes. Only one trial reported on maternal death, and recorded zero deaths in either group (Smith 2008). None of the other trials reported on serious maternal morbidity or death (e.g. uterine rupture, admission to intensive care unit, septicaemia).
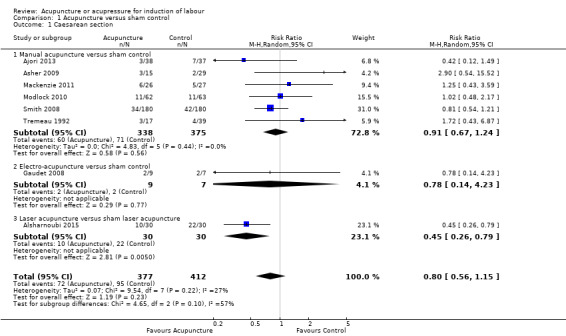
1.1) Outcome: caesarean section
Data on caesarean section were reported from eight trials with 789 women (Analysis 1.1). Overall, there was high‐quality evidence of no clear difference in caesarean deliveries between groups (average risk ratio (RR) 0.80, 95% confidence interval (CI) 0.56 to 1.15, 8 trials, 789 women).
1.1. Analysis.
Comparison 1 Acupuncture versus sham control, Outcome 1 Caesarean section.
1.1.1 Manual acupuncture versus sham control
Six trials (713 women) used manual acupuncture. There was no evidence of a difference in caesarean deliveries between groups (average RR 0.91, 95% CI 0.67 to 1.24, 6 trials, 713 women).
1.1.2 Electro‐acupuncture versus sham control
One small trial (16 women) used electro‐acupuncture. There was no evidence of a difference in caesarean deliveries between groups (RR 0.78, 95% CI 0.14 to 4.23, 1 trial, 16 women).
1.1.3 Laser acupuncture versus sham control
One small trial using laser acupuncture reported on this outcome, with evidence of a benefit for laser acupuncture in caesarean deliveries between groups (RR 0.45, 95% CI 0.26 to 0.79, 1 trial, 60 women).
1.2) Outcome: serious neonatal morbidity
Only one trial using manual acupuncture (Smith 2008) reported on this outcome (Analysis 1.2).
1.2. Analysis.
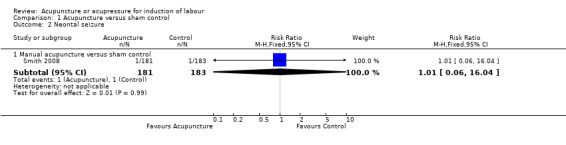
Comparison 1 Acupuncture versus sham control, Outcome 2 Neontal seizure.
1.2.1 Manual acupuncture versus sham control
There was low‐quality evidence of no difference in neonatal seizures between groups (RR 1.01, 95% CI 0.06 to 16.04, one trial, 364 women).
1.3) Outcome: serious maternal morbidity or death
There was low‐quality evidence of no serious outcomes or maternal death reported in one trial (Smith 2008) (Analysis 1.13).
1.13. Analysis.
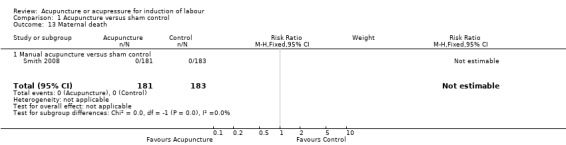
Comparison 1 Acupuncture versus sham control, Outcome 13 Maternal death.
Secondary outcomes
Secondary outcomes related to measures of effectiveness, complications, and satisfaction. Trials reported on cervix unfavourable/unchanged after 12 to 24 hours; oxytocin augmentation; epidural analgesia; instrumental vaginal delivery; meconium‐stained liquor; Apgar score less than seven at five minutes; neonatal intensive care unit admission; perinatal death; postpartum haemorrhage; other maternal side‐effects; and maternal death. The following acupuncture‐specific outcomes were included: use of other induction methods; time from trial intervention to the birth of the baby; and length of labour.
No trial reported on the following outcomes: uterine hyperstimulation without FHR changes; uterine rupture; neonatal encephalopathy; disability in childhood; maternal satisfaction; maternal side effects (all); maternal nausea; maternal vomiting; maternal diarrhoea; serious maternal complications; and caregiver not satisfied.
1.3) Outcome: cervical change within 12 to 24 hours
Data on cervical maturation were available from three trials, with data reported in the meta‐analysis for one trial (Analysis 1.3). Overall, there was evidence of a benefit from acupuncture in increasing cervical maturity within 24 hours (MD 0.40, 95% CI 0.11 to 0.69, 1 trial, 125 women). The Bishop's score was the most common measure of cervical change used in the included trials and provided a single score that encompassed five components including; cervical dilation, cervical effacement, cervical consistency, cervical position, and fetal station. A Bishop's score of nine or greater suggested that labour would most likely commence without any need for induction methods (Tenore 2003).
1.3. Analysis.
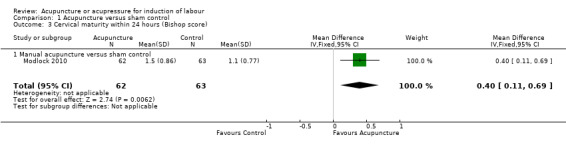
Comparison 1 Acupuncture versus sham control, Outcome 3 Cervical maturity within 24 hours (Bishop score).
Data from the Smith 2008 trial were not included in the meta‐analysis; it reported an increase in the Bishop's score that did not differ between groups (RR 1.08, 95% CI 0.92 to 1.26, 1 trial, 364 women), data not shown.
The Romer 2000 trial did not report on when the cervical change was assessed; however, the authors reported there was a significant change in the Bishop's score (acupuncture 5.9 (1.3) (mean and standard deviation (SD)), nonspecific acupuncture 4.0, (0.9), and no acupuncture 3.6 (1.0)).
1.3.1 Manual acupuncture versus sham control
One trial (125 women) used manual acupuncture. There was greater cervical change in Bishop's score occurring within 24 hours for women receiving acupuncture compared with the sham control, (MD 0.40. 95% CI 0.11 to 0.69, 1 trial, 125 women).
1.4) Outcome: oxytocin augmentation
Data on this outcome were available from four trials and 833 women (Analysis 1.4). Overall, there was no evidence of a difference between groups (RR 0.97 , 95% CI 0.78 to 1.21, 4 trials, 833 women).
1.4. Analysis.
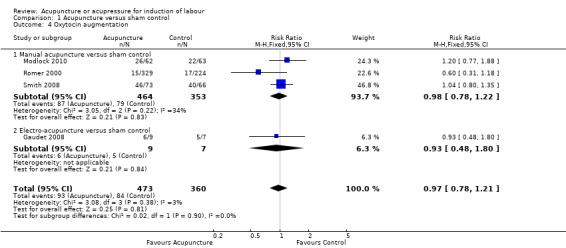
Comparison 1 Acupuncture versus sham control, Outcome 4 Oxytocin augmentation.
1.4.1 Manual acupuncture versus sham control
Three trials (817 women) used manual acupuncture. There was no evidence of a difference in the use of oxytocin augmentation between acupuncture and sham control groups (RR 0.98, 95% CI 0.78 to 1.22, 3 trials, 817 women).
1.4.2 Electro‐acupuncture versus sham control
One trial (16 women) used electro‐acupuncture. There was no evidence of a difference in the use of oxytocin augmentation between electro‐acupuncture and a sham control group (RR 0.93, 95% CI 0.48 to 1.80, 1 trial, 16 women)
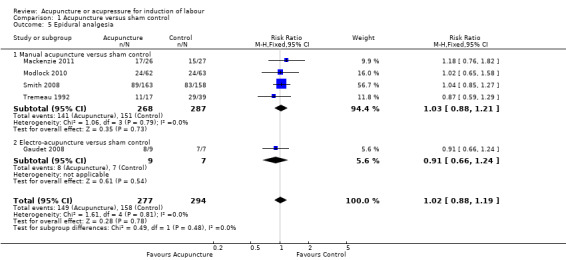
1.5) Outcome: epidural analgesia
This outcome was reported by five trials including 571 women (Analysis 1.5). Overall, there was no evidence of a difference between groups (RR 1.02, 95% CI 0.88 to 1.19, 5 trials, 571 women ).
1.5. Analysis.
Comparison 1 Acupuncture versus sham control, Outcome 5 Epidural analgesia.
1.5.1 Manual acupuncture versus sham control
Four trials (555 women) used manual acupuncture. There was no evidence of a difference in the rate of epidural use between groups (RR 1.03, 95% CI 0.88 to 1.21, 4 trials, 555 women)
1.5.2 Electro‐acupuncture versus sham control
One trial (16 women) used electro‐acupuncture.There was no evidence of a difference in the rate of epidural use between groups (RR 0.91, 95% CI 0.66 to 1.24, 1 trial, 16 women).
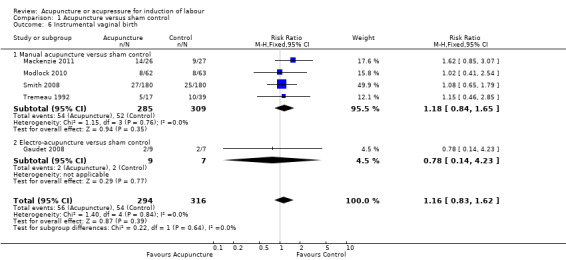
1.6) Outcome: instrumental vaginal birth
Five trials with 610 women reported on this outcome (Analysis 1.6). Overall, there was no evidence for a benefit from acupuncture (RR 1.16, 95% CI 0.83 to 1.62, 5 trials, 610 women).
1.6. Analysis.
Comparison 1 Acupuncture versus sham control, Outcome 6 Instrumental vaginal birth.
1.6.1 Manual acupuncture versus sham control
Four trials (594 women) used manual acupuncture. There was no evidence of a difference in the rate of instrumental delivery between groups (RR 1.18, 95% CI 0.84 to 1.65, 4 trials, 594 women).
1.6.2 Electro‐acupuncture versus sham control
One trial (16 women) used electro‐acupuncture. There was no evidence of a difference in the rate of instrumental delivery between groups (RR 0.78, 95% CI 0.14 to 4.23, 1 trial, 16 women).
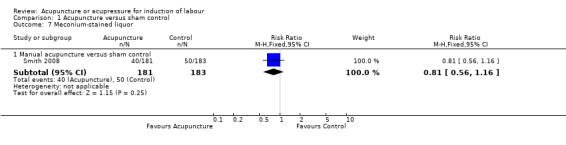
1.7) Outcome: meconium‐stained liquor
One trial using manual acupuncture (364 women) reported on this outcome (Analysis 1.7).
1.7. Analysis.
Comparison 1 Acupuncture versus sham control, Outcome 7 Meconium‐stained liquor.
There was no evidence of a difference in meconium‐stained liquor between groups (RR 0.81, 95% CI 0.56 to 1.16, 1 trial, 364 women).
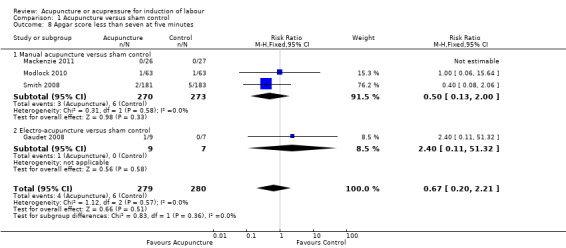
1.8) Outcome: Apgar score less than seven at five minutes
Data on this outcome were reported by four trials (559 women) (Analysis 1.8). Overall, there was no evidence of a benefit for acupuncture (RR 0.67, 95% CI 0.20 to 2.21, 4 trials, 559 women).
1.8. Analysis.
Comparison 1 Acupuncture versus sham control, Outcome 8 Apgar score less than seven at five minutes.
1.8.1 Manual acupuncture versus sham control
Three trials (542 women) used manual acupuncture. There was no evidence of a difference in the Apgar score at five minutes between groups (RR 0.50, 95% CI 0.13 to 2.00, 3 trials, 542 women).
1.8.2 Electro‐acupuncture versus sham control
One trial (16 women) used electro‐acupuncture. There was no evidence of a difference in the Apgar score at five minutes between groups (RR 2.40, 95% CI 0.11 to 51.32, 1 trial, 16 women).
1.9) Outcome: neonatal intensive care unit admission
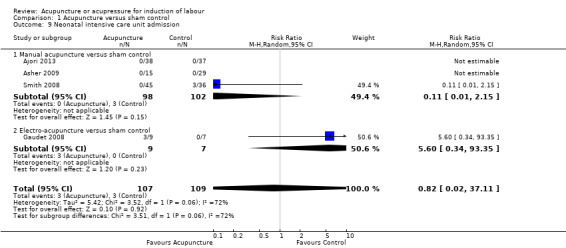
Four trials (216 women) reported on this outcome (Analysis 1.9). Overall, there was no evidence of a benefit for acupuncture (average RR 0.82, 95% CI 0.02 to 37.11, 4 trials, 216 women, I² = 72%, Tau² = 5.42).
1.9. Analysis.
Comparison 1 Acupuncture versus sham control, Outcome 9 Neonatal intensive care unit admission.
1.9.1 Manual acupuncture versus sham control
Three trials (200 women) used manual acupuncture. There was no evidence of a difference between groups (average RR 0.11, 95% CI 0.01 to 2.15, 4 trials, 200 women).
1.9.2 Electro‐acupuncture versus sham control
One trial (16 women) used electro‐acupuncture. There was no evidence of a difference between groups (average RR 5.60, 95% CI 0.34 to 93.35, 1 trial, 16 women).
1.10) Outcome: perinatal death
One trial using manual acupuncture (364 women) reported on this outcome (Analysis 1.10). There were no deaths in either group.
1.10. Analysis.
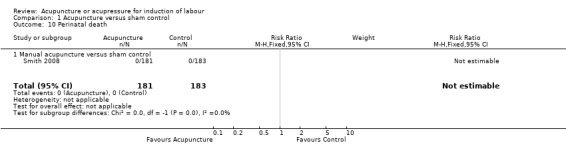
Comparison 1 Acupuncture versus sham control, Outcome 10 Perinatal death.
1.11) Outcome: maternal side effect ‐ maternal infection
One trial using manual acupuncture (44 women) reported on this outcome (Analysis 1.11). There was no evidence of a difference between groups when using manual acupuncture (RR 1.29, 95% CI 0.43 to 3.88, 1 trial, 44 women).
1.11. Analysis.
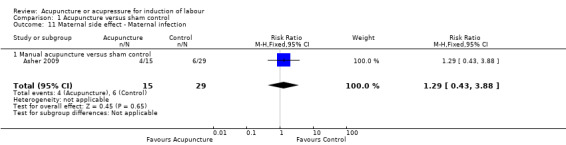
Comparison 1 Acupuncture versus sham control, Outcome 11 Maternal side effect ‐ Maternal infection.
1.12) Outcome: postpartum bleeding greater than 500 mL
Three trials (542 women) reported on this outcome (Analysis 1.12).
1.12. Analysis.
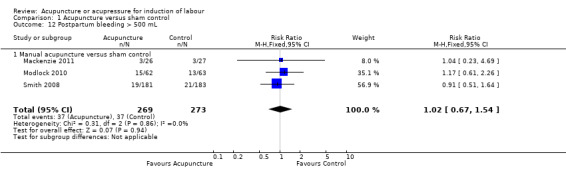
Comparison 1 Acupuncture versus sham control, Outcome 12 Postpartum bleeding > 500 mL.
1.12.1 Manual acupuncture versus sham control
All three trials used manual acupuncture. There was no evidence of a difference between groups (RR 1.02, 95% CI 0.67 to 1.54, 3 trials, 542 women).
1.13) Outcome: maternal death
One trial using manual acupuncture (364 women) reported on this outcome (Analysis 1.13).
There were no maternal deaths in either group.
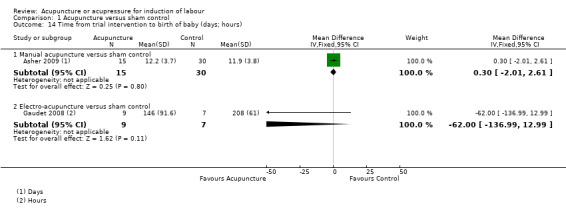
1.14) Outcome: time from trial intervention to the birth of the baby
Two trials (61 women) reported on this outcome (Analysis 1.14).
1.14. Analysis.
Comparison 1 Acupuncture versus sham control, Outcome 14 Time from trial intervention to birth of baby (days; hours).
1.14.1 Manual acupuncture versus sham control
One trial reported on this outcome (Asher 2009) and time was reported in days. There was no evidence of a clear difference in time to delivery between acupuncture and the sham control (MD 0.30, 95% CI ‐2.01 to 2.61, 1 trial, 45 women).
1.14.2 Electro‐acupuncture versus sham control
One trial reported on this outcome (Gaudet 2008) and time was reported in hours. There was no evidence of a clear difference in time to delivery between acupuncture and the sham control (MD ‐62.00, 95% CI ‐136.99 to 12.99, 1 trial,16 women).
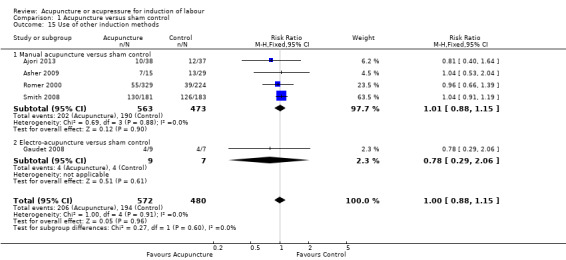
1.15) Outcome: use of other induction methods
Five trials (1052 women) reported on this outcome (Analysis 1.15). Overall, there was no evidence of a difference between groups (RR 1.00, 95% CI 0.88 to 1.15, 5 trials, 1052 women).
1.15. Analysis.
Comparison 1 Acupuncture versus sham control, Outcome 15 Use of other induction methods.
1.15.1 Manual acupuncture versus sham control
Four trials (1036 women) used manual acupuncture. There was no evidence of a difference between groups (RR 1.01, 95% CI 0.88 to 1.15, 4 trials, 1036 women).
1.15.2 Electro‐acupuncture versus sham control
One trial (16 women) used electro‐acupuncture. There was no evidence of a difference between groups (RR 0.78, 95% CI 0.29 to 2.06, 1 trial, 16 women).
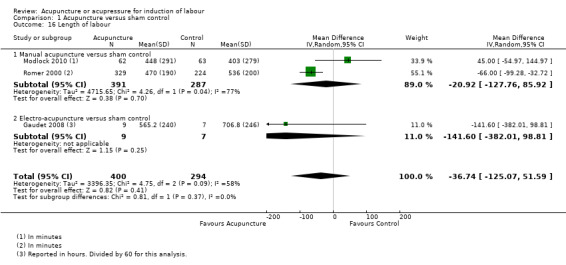
1.16) Outcome: length of labour
Three trials (694 women) reported on this outcome (Analysis 1.16). Overall, there was no evidence of a clear difference between groups (MD ‐36.74 minutes, 95% CI ‐125.07 to 51.59, 3 trials. 694 women, I² = 58%, Tau² = 3396.35).
1.16. Analysis.
Comparison 1 Acupuncture versus sham control, Outcome 16 Length of labour.
1.16.1 Manual acupuncture versus sham control
Two trials (678 women) used manual acupuncture. There was no evidence of a clear difference between groups (MD ‐20.92 minutes, 95% CI ‐127.76 to 85.92, 2 trials, 678 women, I² = 77%, Tau² = 4715.65).
1.16.2 Electro‐acupuncture versus sham control
One trial (16 women) used electro‐acupuncture. There was no evidence of a clear difference between groups (MD ‐141.60 minutes, 95% CI ‐382.01 to 98.81, 1 trial, 16 women).
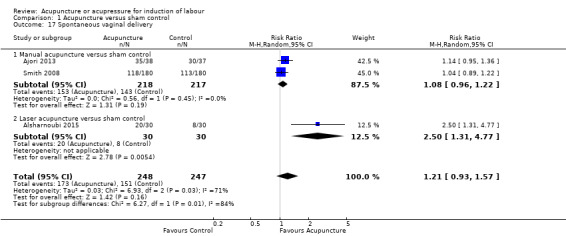
1.17) Outcome: spontaneous vaginal birth
Three trials (495 women) reported on this outcome (Analysis 1.17). A random‐effects model was used due to the high heterogeneity. Overall, there was no evidence of benefit from acupuncture (RR 1.08, 95% CI 0.96 to 1.22, 3 trials, 495 women, I² = 71%, Tau² = 0.043). The test for subgroup interaction was significant (P = 0.01, I² = 84%).
1.17. Analysis.
Comparison 1 Acupuncture versus sham control, Outcome 17 Spontaneous vaginal delivery.
1.17.1 Manual acupuncture versus sham control
Two trials used manual acupuncture. There was no evidence of benefit of acupuncture compared to sham acupuncture (RR 1.08, 95% CI 0.96 to 1.22, 2 trials, 435 women).
1.17.2 Laser acupuncture versus sham control
One trial reported on this outcome. There was evidence of a benefit for laser acupuncture compared to sham laser (RR 2.50, 95% CI 1.31 to 4.77, 1 trial, 60 women).
Comparison 2: Acupuncture versus usual care
Primary outcomes
Eight trials with 760 women reported on caesarean section. No trial reported on serious neonatal morbidity; vaginal birth not achieved within 24 hours; uterine hyperstimulation with fetal heart rate (FHR) changes; and serious maternal morbidity or death (e.g. uterine rupture, admission to intensive care unit, septicaemia).
2.1) Outcome: caesarean section
Data on caesarean section were reported from eight trials with 760 women (Analysis 2.1). Overall, there was low‐quality evidence of no clear difference in caesarean deliveries between groups (average RR 0.77, 95% CI 0.51 to 1.17, 8 trials, 760 women, I² = 42%, Tau² = 0.014). The test for subgroup interaction was significant, suggesting a difference between types of acupuncture (P = 0.04, I² = 75.9%).
2.1. Analysis.
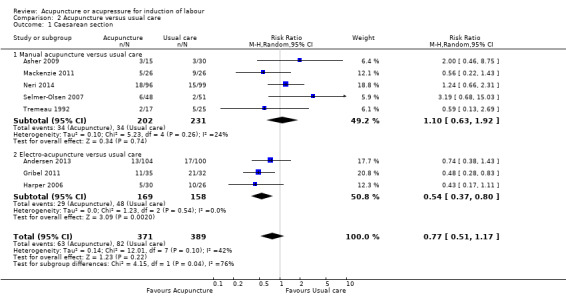
Comparison 2 Acupuncture versus usual care, Outcome 1 Caesarean section.
2.1.1 Manual acupuncture versus usual care
Five trials (433 women) used manual acupuncture. There was no evidence of a difference in caesarean deliveries between groups (average RR 1.10, 95% CI 0.63 to 1.92, 5 trials, 433 women).
2.1.2 Electro‐acupuncture versus usual care
Three trials (327 women) used electro‐acupuncture. There was evidence of a benefit for electro‐acupuncture in reducing caesarean section rate (average RR 0.54, 95% CI 0.37 to 0.80, 3 trials, 327 women).
Secondary outcomes
Secondary outcomes related to measures of effectiveness, complications, and satisfaction. Trials reported on cervix unfavourable/unchanged after 12 to 24 hours; oxytocin augmentation; epidural analgesia; instrumental vaginal delivery; Apgar score less than seven at five minutes; neonatal intensive care unit admission; postpartum haemorrhage; other maternal side effects; maternal death; and woman not satisfied. The following acupuncture‐specific outcomes were included: use of other induction methods; time from trial intervention to the birth of the baby; and length of labour.
No trial reported on the following outcomes: uterine hyperstimulation without FHR changes; uterine rupture; neonatal encephalopathy; meconium‐stained liquor; perinatal death; disability in childhood; maternal side effects (all); maternal nausea; maternal vomiting; maternal diarrhoea; serious maternal complications; and caregiver not satisfied.
2.2) Outcome: cervical change within 12 to 24 hours
Data on cervical maturation were available from two trials (Gribel 2011; Harper 2006) with data reported in the meta‐analysis from one trial (Analysis 2.2). The Bishop's score was the most common measure of cervical change used in the included trials and provided a single score than encompassed five components: cervical dilation, cervical effacement, cervical consistency, cervical position, and fetal station. A Bishop's score of 9 or greater suggested that labour would most likely commence without any need for induction methods (Tenore 2003).
2.2. Analysis.
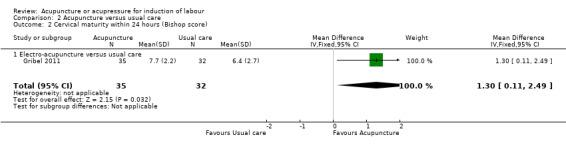
Comparison 2 Acupuncture versus usual care, Outcome 2 Cervical maturity within 24 hours (Bishop score).
2.2.1 Electro‐acupuncture versus usual care
There was an increase in cervical maturation in the acupuncture group compared with the control (MD 1.30, 95% CI 0.11 to 2.49, 1 trial, 67 women).
Data from the Harper 2006 trial were not included in the analysis; there was no difference in cervical dilatation on the day of admission using electro‐acupuncture (3.3.cm versus 2.7 cm, P = 0.28).
2.3) Outcome: oxytocin augmentation
Data on this outcome were available from four trials and 461 women (Analysis 2.3). Overall, there was no evidence of a difference between groups (average RR 1.10, 95% CI 0.90 to 1.34, 4 trials, 461 women).
2.3. Analysis.
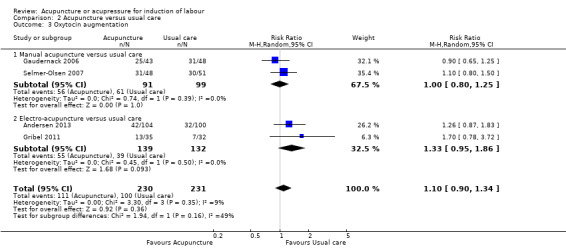
Comparison 2 Acupuncture versus usual care, Outcome 3 Oxytocin augmentation.
2.3.1 Manual acupuncture versus usual care
Two trials (190 women) used manual acupuncture. There was no evidence of a difference in the use of oxytocin augmentation between acupuncture and usual care groups (average RR 1.00, 95% CI 0.80 to 1.25, 2 trials, 190 women).
2.3.2 Electro‐acupuncture versus usual care
Two trials (271 women) used electro‐acupuncture. There was no evidence of a difference in the use of oxytocin augmentation between acupuncture and usual care groups (average RR 1.33, 95% CI 0.95 to 1.86, 2 trials, 271 women).
2.4) Outcome: epidural analgesia
This outcome was reported by six trials and 555 women (Analysis 2.4). Overall, there was no evidence of a difference between groups (average RR 0.92, 95% CI 0.78 to 1.07, 6 trials, 555 women).
2.4. Analysis.
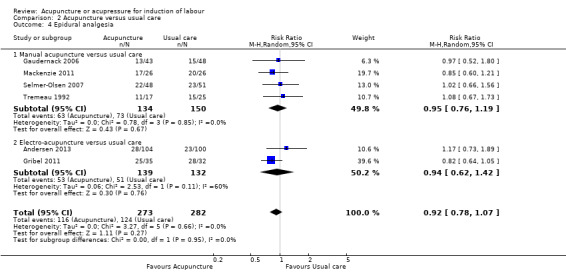
Comparison 2 Acupuncture versus usual care, Outcome 4 Epidural analgesia.
2.4.1 Manual acupuncture versus usual care
Four trials (284 women) used manual acupuncture. There was no evidence of a difference in the rate of epidural use between groups (average RR 0.95, 95% CI 0.76 to 1.19, 4 trials, 284 women).
2.4.2 Electro‐acupuncture versus usual care
Two trials (271 women) used electro‐acupuncture. There was no evidence of a difference in the rate of epidural use between groups (average RR 0.94, 95% CI 0.62 to 1.42, 2 trials, 271 women, I² = 60%, Tau² = 0.06).
2.5) Outcome: instrumental vaginal birth
Six trials with 555 women reported on this outcome (Analysis 2.5). Overall, there was no evidence for a benefit from acupuncture (RR 1.11, 95% CI 0.62 to 1.99, 6 trials, 555 women, I² = 54%, Tau² = 0.27). The test for subgroup interaction was significant, suggesting a difference between different types of acupuncture (P = 0.04, I² = 75.3%).
2.5. Analysis.
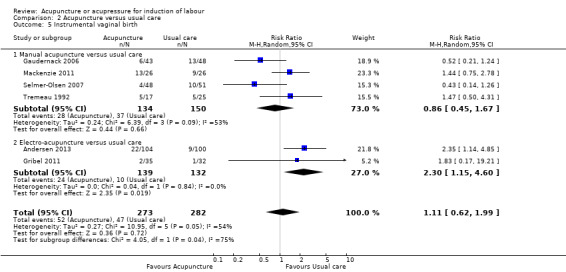
Comparison 2 Acupuncture versus usual care, Outcome 5 Instrumental vaginal birth.
2.5.1 Manual acupuncture versus usual care
Four trials (284 women) used manual acupuncture. There was no evidence of a difference in the rate of instrumental delivery between groups (RR 0.86, 95% CI 0.45 to 1.67, 4 trials, 284 women, I² = 53%, Tau² = 0.24). No one trial appeared to contribute to the significant heterogeneity. A random‐effects model was used due to the significant heterogeneity.
2.5.2 Electro‐acupuncture versus usual care
Two trials (271 women) used electro‐acupuncture. There was evidence of benefit for usual care in the rate of instrumental delivery between groups (RR 2.30, 95% CI 1.15 to 4.60, 2 trials, 271 women).
2.6) Outcome: Apgar score less than seven at five minutes
Data on this outcome were reported by four trials (446 women) (Analysis 2.6). Overall, there was no evidence of a benefit for acupuncture (RR 0.34, 95% CI 0.04 to 3.20, 4 trials, 446 women).
2.6. Analysis.
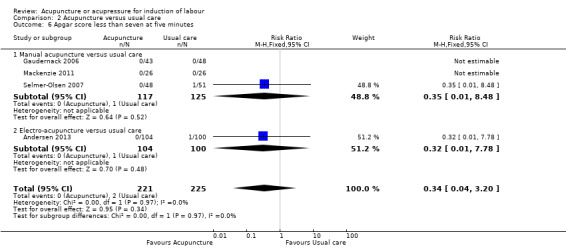
Comparison 2 Acupuncture versus usual care, Outcome 6 Apgar score less than seven at five minutes.
2.6.1 Manual acupuncture versus usual care
Three trials (242 women) used manual acupuncture. There was no evidence of a difference in the Apgar score at five minutes between groups (RR 0.35, 95% CI 0.01 to 8.48, 3 trials, 242 women).
2.6.2 Electro‐acupuncture versus usual care
One trial (204 women) used electro‐acupuncture. There was no evidence of a difference in the Apgar score at five minutes between groups (RR 0.32, 95% CI 0.01 to 7.78, 1 trial, 204 women).
2.7) Outcome: neonatal intensive care unit admission
Two trials (249 women) reported on this outcome (Analysis 2.7). Overall, there was no evidence of a benefit for acupuncture (RR 0.27, 95% CI 0.05 to 1.48, 2 trials, 249 women).
2.7. Analysis.
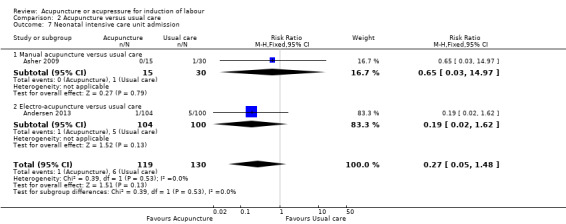
Comparison 2 Acupuncture versus usual care, Outcome 7 Neonatal intensive care unit admission.
2.7.1 Manual acupuncture versus usual care
One trial (45 women) used manual acupuncture. There was no evidence of a difference between groups (RR 0.65, 95% CI 0.03 to 14.97, 1 trial, 45 women).
2.7.2 Electro‐acupuncture versus usual care
One trial (204 women) used electro‐acupuncture. There was no evidence of a difference between groups (RR 0.19, 95% CI 0.02 to 1.62, 1 trial, 204 women).
2.8) Outcome: Maternal side effect ‐ maternal infection
Two trials (136 women) reported on this outcome (Analysis 2.8).
2.8. Analysis.
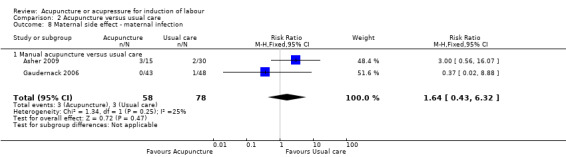
Comparison 2 Acupuncture versus usual care, Outcome 8 Maternal side effect ‐ maternal infection.
2.8.1 Manual acupuncture versus usual care
Two trials (136 women) used manual acupuncture. There was no evidence of a difference between groups (RR 1.64, 95% CI 0.43 to 6.32, 2 trials, 136 women).
2.9) Outcome: Maternal side effect ‐ perineal tear
One trial using manual acupuncture (91 women) reported on this outcome (Analysis 2.9).
2.9. Analysis.
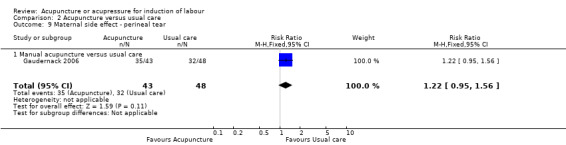
Comparison 2 Acupuncture versus usual care, Outcome 9 Maternal side effect ‐ perineal tear.
2.9.1 Manual acupuncture versus usual care
There was no evidence of a difference in this outcome between groups (RR 1.22, 95% CI 0.95 to 1.56, 1 trial, 91 women).
2.10) Outcome: Maternal side effect ‐ fetal infection
One trial using manual acupuncture (91 women) reported on this outcome (Analysis 2.10).
2.10. Analysis.
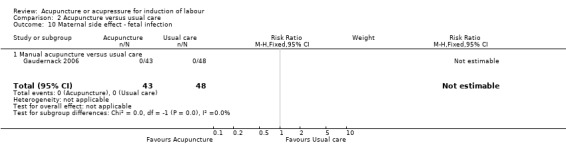
Comparison 2 Acupuncture versus usual care, Outcome 10 Maternal side effect ‐ fetal infection.
2.10.1 Usual care
There were no reports of fetal infection between groups.
2.11) Outcome: postpartum bleeding greater than 500 mL
Two trials (256 women) women reported on this outcome (Analysis 2.11). Overall, there was no evidence of a difference in this outcome between groups (RR 0.81, 95% CI 0.36 to 1.81, 2 trials, 256 women).
2.11. Analysis.
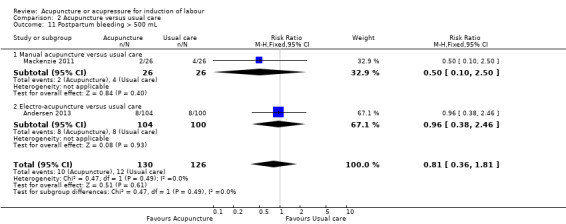
Comparison 2 Acupuncture versus usual care, Outcome 11 Postpartum bleeding > 500 mL.
2.11.1 Manual acupuncture versus usual care
One trial (52 women) used manual acupuncture. There was no evidence of a difference between groups (RR 0.50, 95% CI 0.10 to 2.50, 1 trial, 52 women).
2.11.2 Electro‐acupuncture versus usual care
One trial (204 women) used electro‐acupuncture. There was no evidence of a difference between groups (RR 0.96, 95% CI 0.38 to 2.46, 1 trial, 204 women).
2.12) Outcome: time from trial intervention to the birth of the baby
Two trials (100 women) reported on this outcome (Analysis 2.12).
2.12. Analysis.
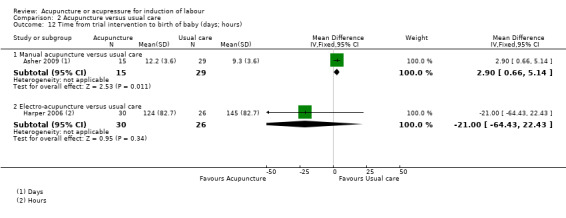
Comparison 2 Acupuncture versus usual care, Outcome 12 Time from trial intervention to birth of baby (days; hours).
2.12.1 Manual acupuncture versus usual care
One trial reported on this outcome (Asher 2009). This outcome was measured in days by Asher 2009. Evidence of a benefit for usual care in reducing time to birth of the baby was found (MD 2.90, 95% CI 0.66 to 5.14; 1 trial, 44 women).
2.12.2 Electro‐acupuncture versus usual care
One trial reported on this outcome (Harper 2006). This outcome was measured in hours by Harper 2006. There was no evidence of a difference between groups (MD ‐21.00, 95% CI ‐64.43 to 22.43, 1 trial, 56 women).
2.13) Outcome: maternal satisfaction
One trial using electro‐acupuncture (67 women) reported on this outcome, (Analysis 2.13).
2.13. Analysis.
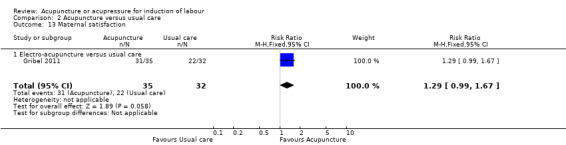
Comparison 2 Acupuncture versus usual care, Outcome 13 Maternal satisfaction.
2.13.1 Electro‐acupuncture versus usual care
There was no evidence of a difference in maternal satisfaction between groups (RR 1.29, 95% CI 0.99 to 1.67, 1 trial, 67 women).
2.14) Outcome: use of other induction methods
Four trials (259 women) reported on this outcome (Analysis 2.14). Overall, there was no evidence of a difference between groups (average RR 1.00, 95% CI 0.69 to 1.45, 4 trials, 259 women, I² = 45%, Tau² = 0.06)
2.14. Analysis.
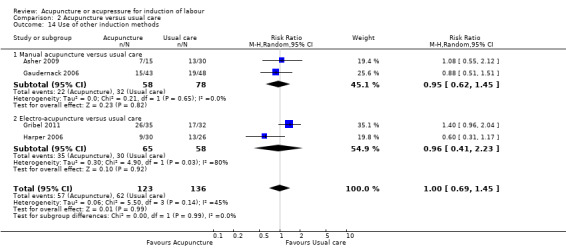
Comparison 2 Acupuncture versus usual care, Outcome 14 Use of other induction methods.
2.14.1 Manual acupuncture versus usual care
Two trials (136 women) used manual acupuncture. There was no evidence of a difference between groups (average RR 0.95, 95% CI 0.62 to 1.45, 2 trials, 136 women)
2.14.2 Electro‐acupuncture versus usual care
Two trials (123 women) used electro‐acupuncture. There was no evidence of a difference between groups (average RR 0.96, 95% CI 0.41 to 2.23, 2 trials, 123 women, I² = 80%,Tau² = 0.30)
2.15) Outcome: length of labour
Two trials (269 women) reported on this outcome; one trial (67 women) were included in the meta‐analysis (Analysis 2.15).
2.15. Analysis.
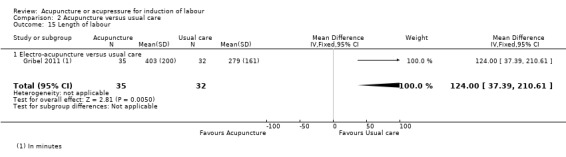
Comparison 2 Acupuncture versus usual care, Outcome 15 Length of labour.
In one trial using electro‐acupuncture (Gribel 2011), there was evidence that the length of labour (in minutes) was shorter in the usual care group compared with acupuncture (MD 124.00 minutes, 95% CI 37.39 to 210.61, 1 trial, 67 women).
One trial using manual acupuncture (Neri 2014) reported data by parity. There was no evidence of a difference in the length of the first stage of labour between groups for both nulliparous women, acupuncture 337 (mean) (99 (SD)) minutes versus usual care 354 (112) minutes and multiparous women, acupuncture 138 (79) minutes versus usual care 179 (93) minutes. There was evidence of a benefit for usual care for nulliparous women in the second stage of labour, acupuncture 58 (30) minutes versus usual care 43.14 (26.3) minutes.
2.16) Outcome: spontaneous vaginal birth
Two trials (117 women) reported on this outcome (Analysis 2.16). A random‐effects model was used due to the high heterogeneity. Overall, there was no evidence of benefit from acupuncture (average RR 1.44, 95% CI 0.70 to 2.98, 2 trials, 117 women, I² = 68.1%, Tau² = 0.23). The test for subgroup interaction was significant, suggesting a difference between different types of acupuncture (P = 0.04, I² = 76.2%).
2.16. Analysis.
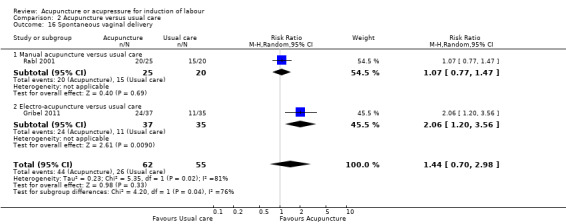
Comparison 2 Acupuncture versus usual care, Outcome 16 Spontaneous vaginal delivery.
2.16.1 Manual acupuncture versus usual care
One trial (45 women) used manual acupuncture. There was no evidence of benefit of acupuncture compared to usual care (RR 1.07, 95% CI 0.77 to 1.47, 1 trial, 45 women).
2.16.2 Electro‐acupuncture versus usual care
One trial (72 women) used electro‐acupuncture. There was evidence of a benefit of electro‐acupuncture compared to usual care (RR 2.06, 95% CI 1.20 to 3.56, 1 trial, 72 women).
Comparison 3: Acupuncture versus sweeping of fetal membranes
Primary outcomes
One trial with 207 women reported on caesarean section. No trial reported on serious neonatal morbidity; vaginal delivery not achieved within 24 hours; uterine hyperstimulation with fetal heart rate (FHR) changes; and serious maternal morbidity or death (e.g. uterine rupture, admission to intensive care unit, septicaemia).
3.1) Outcome: caesarean section
Data on caesarean section were reported from one trial with 207 women (Analysis 3.1). One trial using electro‐acupuncture reported on this outcome, with moderate‐quality evidence of no clear difference in caesarean deliveries between groups (RR 0.64, 95% CI 0.34 to 1.22, 1 trial, 207 women).
3.1. Analysis.
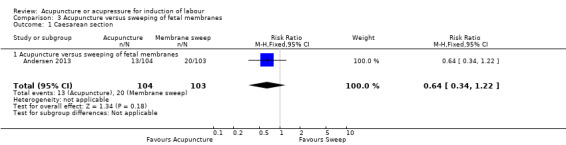
Comparison 3 Acupuncture versus sweeping of fetal membranes, Outcome 1 Caesarean section.
Secondary outcomes
Secondary outcomes related to measures of effectiveness, complications, and satisfaction. Trials reported on oxytocin augmentation; epidural analgesia; instrumental vaginal birth; Apgar score less than seven at five minutes; neonatal intensive care unit admission; and postpartum haemorrhage.
No trial reported on the following outcomes: cervix unfavourable/unchanged after 12 to 24 hours; uterine hyperstimulation without FHR changes; uterine rupture; perinatal death; meconium‐stained liquor; neonatal encephalopathy; disability in childhood; other maternal side effects; maternal death; woman not satisfied; maternal side effects (all); maternal nausea; maternal vomiting; maternal diarrhoea; serious maternal complications; and caregiver not satisfied.The following acupuncture‐specific outcomes were not reported: use of other induction methods; time from trial intervention to the birth of the baby; and length of labour.
3.2) Outcome: oxytocin augmentation
One trial using electro‐acupuncture reported on this outcome (Analysis 3.2). There was no evidence of a difference in the use of oxytocin augmentation between acupuncture and sweeping of the fetal membrane groups (RR 0.90, 95% CI 0.66 to 1.24, 1 trial, 207 women).
3.2. Analysis.
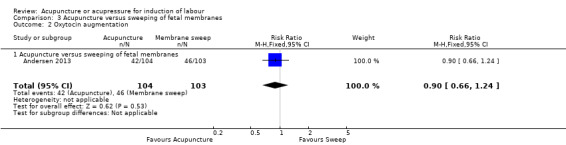
Comparison 3 Acupuncture versus sweeping of fetal membranes, Outcome 2 Oxytocin augmentation.
3.3) Outcome: epidural analgesia
One trial using electro‐acupuncture reported on this outcome (Analysis 3.3). There was no evidence of a difference in the rate of epidural use between groups (RR 0.96, 95% CI 0.61 to 1.49, 1 trial, 207 women).
3.3. Analysis.
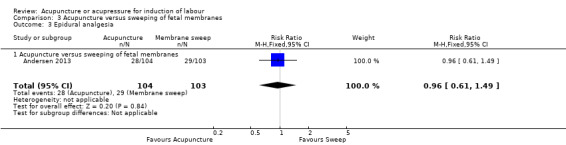
Comparison 3 Acupuncture versus sweeping of fetal membranes, Outcome 3 Epidural analgesia.
3.4) Outcome: instrumental vaginal delivery
One trial using electro‐acupuncture reported this outcome (Analysis 3.4). There was no evidence of a difference in the rate of instrumental delivery between groups (RR 1.68, 95% CI 0.89 to 3.14, 1 trial, 207 women).
3.4. Analysis.
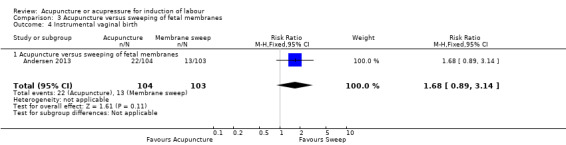
Comparison 3 Acupuncture versus sweeping of fetal membranes, Outcome 4 Instrumental vaginal birth.
3.5) Outcome: Apgar score less than seven at five minutes
One trial using electro‐acupuncture reported on this outcome. There we no Apgar scores less than seven occurring in either group, (Analysis 3.5).
3.5. Analysis.
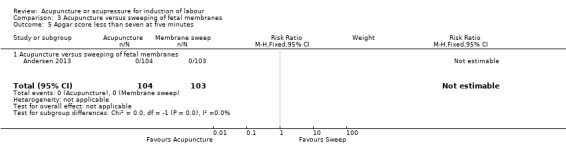
Comparison 3 Acupuncture versus sweeping of fetal membranes, Outcome 5 Apgar score less than seven at five minutes.
3.6) Outcome: neonatal intensive care unit admission
One trial using electro‐acupuncture reported on this outcome (Analysis 3.6). There was no evidence of a difference between groups (RR 0.33, 95% CI 0.03 to 3.12, 1 trial, 207 women).
3.6. Analysis.
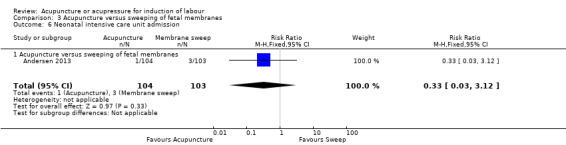
Comparison 3 Acupuncture versus sweeping of fetal membranes, Outcome 6 Neonatal intensive care unit admission.
3.7) Outcome: postpartum bleeding greater than 500 mL
One trial using electro‐acupuncture reported on this outcome (Analysis 3.7). There was no evidence of a difference in the rate of instrumental delivery between groups (RR 1.32, 95% CI 0.47 to 3.67, 1 trial, 207 women).
3.7. Analysis.
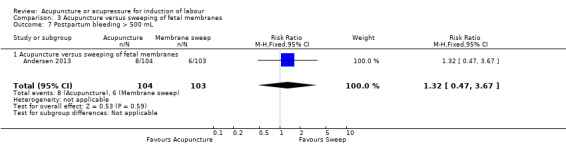
Comparison 3 Acupuncture versus sweeping of fetal membranes, Outcome 7 Postpartum bleeding > 500 mL.
Comparison 4: Acupressure versus sham control
Primary outcomes
Two trials reported on one primary outcome only: caesarean section. No trial reported on serious neonatal morbidity; vaginal delivery not achieved within 24 hours; uterine hyperstimulation with FHR changes; and serious maternal morbidity or death (e.g. uterine rupture, admission to intensive care unit, septicaemia).
4.1) Outcome: caesarean section
Data on caesarean section were reported from two trials with 239 women (Analysis 4.1).
4.1. Analysis.
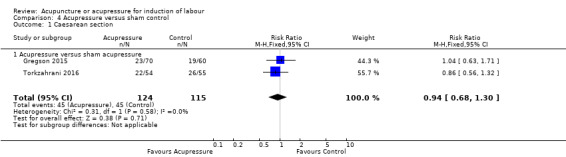
Comparison 4 Acupressure versus sham control, Outcome 1 Caesarean section.
There was moderate‐quality evidence of no clear difference in caesarean deliveries between groups (RR, 0.94, 95% CI 0.68 to 1.30, 2 trials, 239 women).
Secondary outcomes
Secondary outcomes related to measures of effectiveness, complications, and satisfaction. Trials reported on oxytocin augmentation; instrumental vaginal birth; and meconium‐stained liquor. The following acupuncture‐specific outcomes were included: time from trial intervention to the birth of the baby.
No trial reported on the following outcomes: cervix unfavourable/unchanged after 12 to 24 hours; epidural analgesia; perinatal death; postpartum haemorrhage; other maternal side effects; maternal death; woman not satisfied; Apgar score less than seven at five minutes; neonatal intensive care unit admission; uterine hyperstimulation without FHR changes; uterine rupture; neonatal encephalopathy; disability in childhood; maternal side effects (all); maternal nausea; maternal vomiting; maternal diarrhoea; serious maternal complications; caregiver not satisfied; and length of labour. No trial reported on the acupuncture‐specific outcome: use of other induction methods.
4.2) Outcome: oxytocin augmentation
One trial (Gregson 2015) reported on this outcome (Analysis 4.2). There was no evidence of a difference in the use of oxytocin augmentation between acupressure and a sham control group (RR 1.42, 95% CI 0.96 to 2.08, 1 trial, 130 women).
4.2. Analysis.
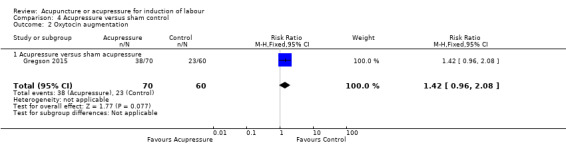
Comparison 4 Acupressure versus sham control, Outcome 2 Oxytocin augmentation.
4.3) Outcome: instrumental vaginal birth
One trial (Gregson 2015) reported on this outcome (Analysis 4.3). There was no evidence of a difference in the rate of instrumental delivery between groups (RR 1.12, 95% CI 0.59 to 2.11, 1 trial, 130 women).
4.3. Analysis.
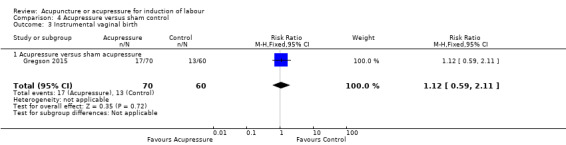
Comparison 4 Acupressure versus sham control, Outcome 3 Instrumental vaginal birth.
4.4) Outcome: meconium‐stained liquor
One trial (Gregson 2015) reported on this outcome (Analysis 4.4). There was no evidence of a difference in meconium‐stained liquor between groups (RR 1.45, 95% CI 0.80 to 2.62, 1 trial, 130 women).
4.4. Analysis.
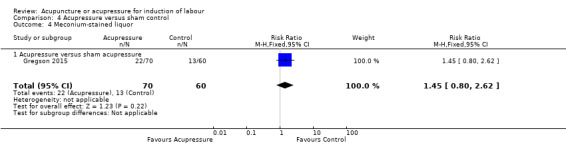
Comparison 4 Acupressure versus sham control, Outcome 4 Meconium‐stained liquor.
4.5) Outcome: time from trial intervention to birth of the baby
One trial (Torkzahrani 2016) reported this outcome in hours (Analysis 4.5).
4.5. Analysis.
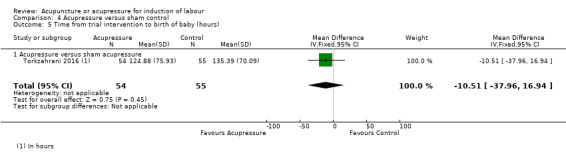
Comparison 4 Acupressure versus sham control, Outcome 5 Time from trial intervention to birth of baby (hours).
There was no evidence of a difference in time to delivery between groups (MD ‐10.51, 95% CI ‐37.96 to 16.94, 1 trial, 109 women).
4.6) Outcome: spontaneous vaginal delivery
Two trials reported on this outcome (Analysis 4.6). There was no evidence of a benefit from acupressure compared to sham (RR 1.04, 95% CI 0.79 to 1.36, 2 trials, 239 women).
4.6. Analysis.
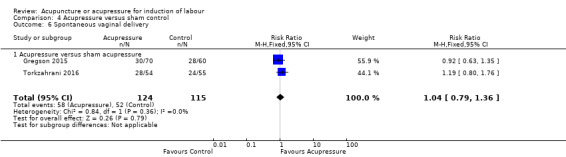
Comparison 4 Acupressure versus sham control, Outcome 6 Spontaneous vaginal delivery.
Comparison 5: Acupressure versus usual care
Primary outcomes
Two trials reported on one primary outcome only: caesarean section. No trial reported on serious neonatal morbidity; vaginal birth not achieved within 24 hours; uterine hyperstimulation with FHR changes; and serious maternal morbidity or death (e.g. uterine rupture, admission to intensive care unit, septicaemia).
5.1) Outcome: caesarean section
Data on caesarean section were reported from two trials with 151 women (Analysis 5.1). Overall. there was moderate‐quality evidence of no clear differences between groups (RR 1.02, 95% CI 0.68 to 1.53, 2 trials, 151 women). A fixed‐effects model was used, due to the small number of studies included in this comparison.
5.1. Analysis.
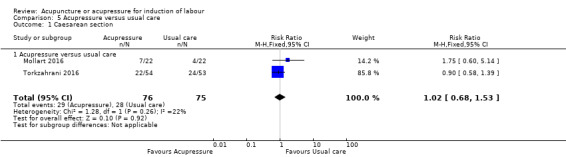
Comparison 5 Acupressure versus usual care, Outcome 1 Caesarean section.
Secondary outcomes
Secondary outcomes related to measures of effectiveness, complications, and satisfaction. Trials reported on epidural analgesia; Apgar score less than seven at five minutes; and neonatal intensive care unit admission. The following acupuncture‐specific outcomes were included: use of other induction methods, and time from trial intervention to the birth of the baby.
No trial reported on the following outcomes: cervix unfavourable/unchanged after 12 to 24 hours; oxytocin augmentation; instrumental vaginal delivery; meconium‐stained liquor; perinatal death; postpartum haemorrhage; other maternal side effects; maternal death; woman not satisfied; uterine hyperstimulation without FHR changes; uterine rupture; neonatal encephalopathy; disability in childhood; maternal side effects (all); maternal nausea; maternal vomiting; maternal diarrhoea; serious maternal complications; caregiver not satisfied; and length of labour.
5.2) Outcome: epidural analgesia
One trial (Mollart 2016) reported on this outcome (Analysis 5.2). There was no evidence of a difference in the rate of epidural use between groups (RR 0.91, 95% CI 0.49 to 1.69, 1 trial, 44 women).
5.2. Analysis.
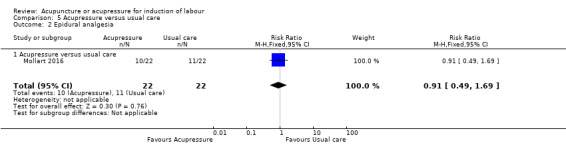
Comparison 5 Acupressure versus usual care, Outcome 2 Epidural analgesia.
5.3) Outcome: Apgar score less than seven at five minutes
One trial (Mollart 2016) reported on this outcome (Analysis 5.3).There was no evidence of a difference in the Apgar score at five minutes between groups (RR 3.00, 95% CI 0.13 to 69.87, 1 trial, 44 women).
5.3. Analysis.
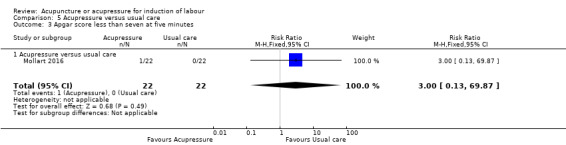
Comparison 5 Acupressure versus usual care, Outcome 3 Apgar score less than seven at five minutes.
5.4) Outcome: neonatal intensive care unit admission
One trial (Mollart 2016) reported on this outcome (Analysis 5.4).
5.4. Analysis.
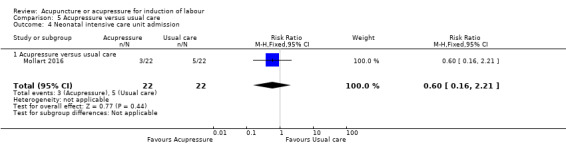
Comparison 5 Acupressure versus usual care, Outcome 4 Neonatal intensive care unit admission.
There was no evidence of a difference between groups (RR 0.60, 95% CI 0.16 to 2.21, 1 trial, 44 women).
5.5) Outcome: time from trial intervention to birth of the baby
One trial (Torkzahrani 2016) reported on this outcome in hours (Analysis 5.5).
5.5. Analysis.
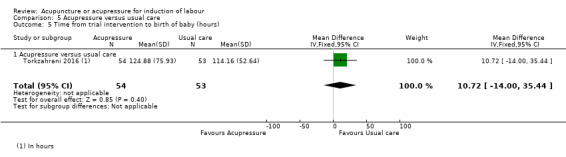
Comparison 5 Acupressure versus usual care, Outcome 5 Time from trial intervention to birth of baby (hours).
There was no evidence of a difference in time to delivery between groups (MD 10.72, 95% CI ‐14.00 to 35.44, 1 trial, 107 women).
5.6) Outcome: use of other induction methods
One trial (Mollart 2016) reported on this outcome (Analysis 5.6).
5.6. Analysis.
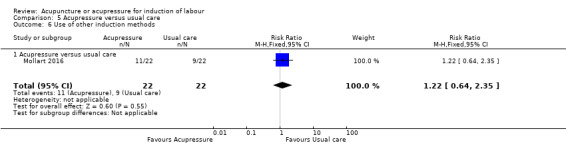
Comparison 5 Acupressure versus usual care, Outcome 6 Use of other induction methods.
There was no evidence of a difference between groups (RR 1.22, 95% CI 0.64 to 2.35, 1 trial, 44 women).
5.7) Outcome: spontaneous vaginal birth
Two trials reported on this outcome (Analysis 5.7). There was no evidence of a benefit from acupressure compared to usual care (RR 0.97, 95% CI 0.69 to 1.34, 2 trials, 151 women, I² = 37%, Tau² = 0.02).
5.7. Analysis.
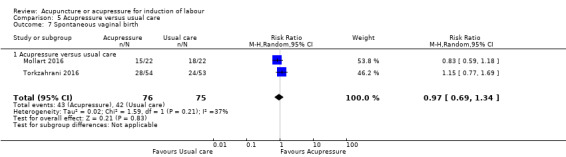
Comparison 5 Acupressure versus usual care, Outcome 7 Spontaneous vaginal birth.
Data from other studies
In the Rabl trial (Rabl 2001), 11 (20%) women were post‐randomisation exclusions and proceeded to have an elective induction of labour. In the acupuncture group, labour was induced for one woman because of fetal heart abnormalities and two inductions were performed due to pre‐labour rupture of membranes. In the control group, two women requested an elective induction of labour, three women received an induction of labour because of pre‐labour rupture of membranes, and in three women, labour was induced due to abnormal FHR patterns. Because data were not available about the post‐randomisation exclusions and an intention‐to‐treat analysis could not be undertaken, no results could be incorporated into this review. In Torkzahrani 2015, changes in the Bishop's score were measured after self‐applied or researcher‐applied acupressure compared to usual care. Changes in Bishop's score were measured at 48 and 96 hours and at presentation to hospital. No data were provided on Bishop's scores at 12 or 24 hours and therefore could not be incorporated into the meta‐analysis. The authors reported that at 48 hours there was a significant difference in Bishop's score (mean and (standard deviation)) between acupressure performed by the researcher 4.88 (1.83), acupressure performed by the mother 5.12 (1.92) and usual care 4.06 (1.59). This difference between groups was also significant at the time of hospital admission, acupressure performed by the researcher 5.95 (2.02), acupressure performed by the mother 6.02 (1.68) and usual care 5.02 (2.03).
Sensitivity analysis
It was proposed to undertake a sensitivity analysis on the results to look at the possible contribution of: (1) differences in risk of bias with trials having a low risk of bias across four or more domains compared to all trials; and (2) publication bias by country. Neither was able to be done due to the small number of trials overall.
Subgroup analysis
We were unable to undertake the planned subgroup analysis due to fewer than five trials reporting on the outcome of interest. We did however carry out comparisons according to subgroups by type of intervention, manual acupuncture versus electro‐acupuncture, for all outcomes where possible.
Discussion
Summary of main results
Findings from this review were based on comparisons between acupuncture and 11 sham‐controlled trials, and comparisons between acupuncture with 15 trials using usual care controls, or usual care plus sham. Evidence from 22 trials with data reporting on 3456 women suggested very limited benefit from acupuncture to induce labour. There was overall no evidence of benefit for acupuncture or acupressure to reduce the need for caesarean section. Subgroup analysis suggested a benefit from electro‐acupuncture for reducing caesarean section rate when compared to usual care. The majority of trials did not report on any other primary outcome.
There was evidence of a benefit from acupuncture with increasing cervical maturity within 24 hours compared to usual care and to sham control. Data on cervical ripening provided conflicting results to those trials that were not included in the meta‐analysis. Four trials used changes in Bishop's scores (Romer 2000; Smith 2008; Torkzahrani 2015; Tremeau 1992) and one used cervical dilatation (Harper 2006). Compared to usual care, acupuncture showed a greater progression in both Bishop's score (Tremeau 1992) and cervical dilatation (Harper 2006). There was no change in Bishop's score when compared to sham control (Smith 2008). One acupressure trial (Torkzahrani 2015) found that cervical ripening (measured via Bishop's score) was increased in both acupressure groups versus usual care.
Overall, trials were characterised by heterogenous acupuncture/acupressure point selection and dosage. There was no evidence of benefit for acupressure for any of the primary or secondary outcomes. Although there have been more trials reported evaluating the role of acupuncture since this review was last updated, there continues to be a relatively small number of trials that have provided relevant health outcomes. This limits the power of the review to detect meaningful differences between groups and analyses, suggesting these limited benefits should be interpreted with caution.
Overall completeness and applicability of evidence
Trials recruited low‐risk nulliparous and primiparous women at term. The majority of trials reported that women who were offered the opportunity to participate in the trial agreed to participate. Smith 2008, however, reported that 18% of women approached declined participation due to a lack of interest in acupuncture.
The systematic review documented wide variation in the delivery of acupuncture and acupressure. This included the mode of stimulation, duration of needling/pressure, number of points used, depth of needling, number of times pressure was applied per day, and duration of the trial. It is unclear how representative the treatment protocols that were used in the research are generalisable to acupuncture, as it is usually practiced. There was insufficient reporting of the rationale of the acupuncture used in the research setting. Some trials used a fixed approach to the selection of points whilst other used a flexible approach, with selection of acupuncture points based on their clinical presentation. The variation in the duration, frequency, and selection of acupuncture points suggests that the acupuncture may not have been therapeutically effective and, in some cases, may not represent best clinical practice. The variation may also reflect the country context in which acupuncture is practiced.
Quality of the evidence
The 'Risk of bias' tables (Figure 2; Figure 3) demonstrated that acupuncture has not been subjected to consistent rigorous study, however, the quality of reporting seems to be improving. Only two trials were assessed at a low risk of bias across all domains. The majority of studies were at a low risk of bias in respect to randomisation. Rates of attrition in the majority of trials were low with only three trials rated at a high risk of bias. The majority of trials were at a low risk of detection bias. Most trials were at a low risk for blinding due to the use of objective outcome measures and/or the use of blinded assessors.
Only one of the sham acupuncture controlled trials used a non‐penetrating needle, however, these were placed at active acupuncture points and, therefore, may be associated with some physiological activity. The methodological quality of studies was also influenced by small sample sizes, with many studies underpowered to detect changes between groups.
We assessed the quality of the evidence for the outcomes presented in five 'Summary of findings' tables using GRADE (see Table 1; Table 2; Table 3; Table 4; Table 5). We were only able to assess the quality of the evidence for one GRADE outcome: caesarean section. Overall, the evidence ranged from low to high quality. Reasons for downgrading included limitations in studies, small sample sizes, and wide confidence intervals.
Potential biases in the review process
We attempted to minimise publication bias. Our search was comprehensive and we included studies identified in languages other than English. However, we cannot rule out the possibility that some studies may have been missed. We acknowledge other foreign language databases have not been searched and there is a potential that some studies have not been identified.
Agreements and disagreements with other studies or reviews
Two recent systematic reviews have examined the role of acupressure on onset and duration of labour (Makvandi 2016; Mollart 2015). Both reviews focused on studies that included women in active labour, once contractions had onset, which are excluded by our review protocol. Makvandi 2016 included 13 studies, while Mollart 2015 included a subset of seven of these trials. Both reviews concluded that acupressure during active labour showed benefits in reducing the duration of labour, while Makvadi also found that it increased the likelihood of vaginal delivery. There were no overlap between studies included in Makvandi 2016 or Mollart 2015 and this review. One systematic review examining the effect of acupuncture on induction of labour and cervical maturation found all studies demonstrated labour induction by acupuncture treatment (Lim 2009). The review included 10 studies consisting of randomised controlled trials, nonrandomised studies with and without controls, and a matched pair study. The review by Lim et al concluded a definitive role for acupuncture was still to be established and further research was needed. A recent systematic review of methods of induction of labour included our earlier Cochrane review (Smith 2004), and three other randomised controlled trials published since the 2004 Cochrane review (Mozurkewich 2011). The authors concluded that acupuncture for induction of labour is investigational, and no advantages have been demonstrated. Overall, all reviews identify there is insufficient evidence of a benefit from acupuncture.
Authors' conclusions
Implications for practice.
Acupuncture does not appear to reduce the need for caesarean section but may improve the cervical readiness for labour. There was no evidence of benefit from acupressure in non‐labouring women. The main limitations were limited reporting of health outcomes. Acupuncture and acupressure appear safe and the review suggests some potential benefit, however the specific timing and how many treatments remain unclear.
Implications for research.
Very few studies reported on the range of primary outcomes included in this review. Further research is required. We suggest future research additionally focuses on gaining a greater understanding of the specific components of acupuncture treatment in relation to working with women during the third trimester, particularly those who are approaching term, and at term. Appropriately powered randomised trials are required to examine the effectiveness of acupuncture on the clinical outcomes described in this review, especially in regards to the timing of measurements of cervical change, such as Bishop's score. Further research could compare acupuncture or acupressure with common conventional methods of induction of labour.
What's new
| Date | Event | Description |
|---|---|---|
| 3 October 2016 | New citation required and conclusions have changed | Eight new trials have been added since the last update (Ajori 2013; Alsharnoubi 2015; Andersen 2013; Gregson 2015; Mollart 2016; Neri 2014; Torkzahrani 2015; Torkzahrani 2016). In this update there is now evidence for the following comparisons: acupuncture versus sweeping of fetal membranes; acupressure versus sham acupressure; and acupressure versus usual care. |
| 3 October 2016 | New search has been performed | Search updated. Change to protocol: addition of outcome vaginal delivery and additional proposed subgroup analyses. Five 'Summary of findings' tables have been incorporated. |
History
Protocol first published: Issue 2, 2000 Review first published: Issue 1, 2001
| Date | Event | Description |
|---|---|---|
| 7 February 2013 | New citation required and conclusions have changed | Eleven trials have been added since the last update. Conclusions have changed for one outcome: need for induction methods. There is now no difference in the use of additional induction methods between acupuncture and standard care groups. |
| 23 November 2012 | New search has been performed | Search updated and 18 trial reports identified. |
| 23 May 2012 | Amended | Search updated. Fifteen reports added to Studies awaiting classification. |
| 10 November 2008 | Amended | Contact details updated. |
| 13 August 2008 | Amended | Corrected typing mistake in the Plain language summary. |
| 8 February 2008 | New search has been performed | Search updated. We identified nine new trial reports for eight trials, two of which have been included (Gaudernack 2006; Harper 2006a), three excluded (Bo 2006; Martinez 2004a; So 1979a), one is awaiting assessment (Coeytaux 2007) and two are ongoing (Lorentzen 2006; Modlock 2006). |
| 8 February 2008 | Amended | Converted to new review format. |
| 31 October 2003 | New search has been performed | Search updated. We identified one new trial that met the inclusion criteria (Rabl 2001) and two new trials which we excluded (Dorr 1990a;Romer 2000a ). |
Acknowledgements
We acknowledge the French to English translation by Peter Smith, the Chinese to English translation by Aidan Tan, and the German to English translation by Richmal Oates‐Whitehead, with additional translation by Gerald Muench, Julie Brown for data extraction of the Smith 2008 trial, and Xun Li for her assistance in attempted contact with Chinese authors and translations.
We acknowledge, with gratitude, the significant contribution that Caroline Crowther made to the original version of this review and each subsequent update. Suzanne Grant contributed to the previous update of this review.
As part of the pre‐publication editorial process, this review has been commented on by two peers (an editor and referee who is external to the editorial team), a member of the Pregnancy and Childbirth Group's international panel of consumers, and the Group's Statistical Adviser.
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to Cochrane Pregnancy and Childbirth. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS, or the Department of Health.
Appendices
Appendix 1. Search Strategies
PubMed
1. exp Acupuncture Therapy (10724)
2. exp Medicine, East Asian Traditional (3238)
3. exp Acupuncture/ (15070)
4. (acupuncture or acupressure or acupoint* or electroacupuncture or electro‐acupuncture or TENS
5. 1 OR 2 OR 3 OR 4 (32010)
6. exp induction of labour (1496)
7. exp labour (21925)
8. labo?r
9. 6 OR 7 OR 8
10. 5 AND 9 (101)
11. randomized controlled trial.pt.
12. controlled clinical trial.pt.
13. randomized.ab.
14. placebo.ab.
15. drug therapy.fs.
16. randomly.ab.
17. trial.ab.
18. groups.ab.
19. 11 or 12 or 13 or14 or 15 or 16 or 17 or 18
20. 10 AND 20 (31)
CINAHL Plus search strategy
1. (MH "Acupuncture+") OR (MH "Acupuncture Points") OR (MH "Acupuncture, Ear") OR (MH "Acupuncturists") OR (MH "Acupuncture Analgesia")
2. electroacupuncture OR electro‐acupuncture
3. acupressure OR acupoint* OR TENS
4. #1 OR #2 OR #3 (10,266)
5. (MH "Labor, Induced+") OR (MH "Labor Stage, First") OR (MH "Labor Stage, Second") OR (MH "Labor Stage, Third") OR (MH "Labor Support")
6. Caesarean OR Pregnancy OR uterine cervix ripening OR Prostaglandin OR intravaginal drug administration OR Oxytocin OR misoprostol OR labo*r induction OR induction of labo*r
7. #5 OR #6 (113,359)
8. (MM "Randomized Controlled Trials") OR (MM "Clinical Trials+")
9. randomized controlled trial.pt. OR controlled clinical trial.pt. OR randomized.ab. OR placebo.ab. OR drug therapy.fs. OR randomly.ab. OR trial.ab. OR groups.ab.
10. #8 OR #9 (146,052)
11. #4 AND #7 AND #10 (118)
Embase search strategy
1. exp acupuncture analgesia/
2. acupuncture.mp.
3. exp acupuncture/
4. exp acupuncture needle/
5. electroacupuncture OR electro‐acupuncture
6. acupressure OR acupoint* OR TENS
7. 1 OR 2 OR 3 OR 4 OR 5 OR 6 (39862)
8. cesarean section/ or pregnancy/ or prostaglandin/ or intravaginal drug administration/ or oxytocin/ or uterine cervix ripening/ or prostaglandin E2/ or misoprostol/ or labor induction/ or induction of labour.mp. or prostaglandin derivative/ (732108)
9. 7 AND 8 (1165)
10. Limited to Human and yr=2012 (59)
11. Randomization.mp/ or controlled clinical trial.pt. / or double blind procedure/ or randomized controlled trials.mp or (topic)/ or random allocation.mp. / or double blind method.sh. / or meta analysis/ or single‐blind method.sh. / or single blind procedure/ or clinical trial.pt.
12. 11 AND 9 (16)
Dissertations and Theses A&I (ProQuest)
Acupuncture AND [labour OR labor] in Title, Subject, Abstract
WHO International Clinical Trials Registry Platform (ICTRP)
Acupuncture OR acupressure AND (labour OR labor)
Data and analyses
Comparison 1. Acupuncture versus sham control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Caesarean section | 8 | 789 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.56, 1.15] |
| 1.1 Manual acupuncture versus sham control | 6 | 713 | Risk Ratio (M‐H, Random, 95% CI) | 0.91 [0.67, 1.24] |
| 1.2 Electro‐acupuncture versus sham control | 1 | 16 | Risk Ratio (M‐H, Random, 95% CI) | 0.78 [0.14, 4.23] |
| 1.3 Laser acupuncture versus sham laser acupuncture | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 0.45 [0.26, 0.79] |
| 2 Neontal seizure | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 Manual acupuncture versus sham control | 1 | 364 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.06, 16.04] |
| 3 Cervical maturity within 24 hours (Bishop score) | 1 | 125 | Mean Difference (IV, Fixed, 95% CI) | 0.40 [0.11, 0.69] |
| 3.1 Manual acupuncture versus sham control | 1 | 125 | Mean Difference (IV, Fixed, 95% CI) | 0.40 [0.11, 0.69] |
| 4 Oxytocin augmentation | 4 | 833 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.78, 1.21] |
| 4.1 Manual acupuncture versus sham control | 3 | 817 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.78, 1.22] |
| 4.2 Electro‐acupuncture versus sham control | 1 | 16 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.48, 1.80] |
| 5 Epidural analgesia | 5 | 571 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.88, 1.19] |
| 5.1 Manual acupuncture versus sham control | 4 | 555 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.88, 1.21] |
| 5.2 Electro‐acupuncture versus sham control | 1 | 16 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.66, 1.24] |
| 6 Instrumental vaginal birth | 5 | 610 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.16 [0.83, 1.62] |
| 6.1 Manual acupuncture versus sham control | 4 | 594 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.18 [0.84, 1.65] |
| 6.2 Electro‐acupuncture versus sham control | 1 | 16 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.78 [0.14, 4.23] |
| 7 Meconium‐stained liquor | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 7.1 Manual acupuncture versus sham control | 1 | 364 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.81 [0.56, 1.16] |
| 8 Apgar score less than seven at five minutes | 4 | 559 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.20, 2.21] |
| 8.1 Manual acupuncture versus sham control | 3 | 543 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.50 [0.13, 2.00] |
| 8.2 Electro‐acupuncture versus sham control | 1 | 16 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.4 [0.11, 51.32] |
| 9 Neonatal intensive care unit admission | 4 | 216 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.02, 37.11] |
| 9.1 Manual acupuncture versus sham control | 3 | 200 | Risk Ratio (M‐H, Random, 95% CI) | 0.11 [0.01, 2.15] |
| 9.2 Electro‐acupuncture versus sham control | 1 | 16 | Risk Ratio (M‐H, Random, 95% CI) | 5.6 [0.34, 93.35] |
| 10 Perinatal death | 1 | 364 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 10.1 Manual acupuncture versus sham control | 1 | 364 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11 Maternal side effect ‐ Maternal infection | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.43, 3.88] |
| 11.1 Manual acupuncture versus sham control | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.43, 3.88] |
| 12 Postpartum bleeding > 500 mL | 3 | 542 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.67, 1.54] |
| 12.1 Manual acupuncture versus sham control | 3 | 542 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.67, 1.54] |
| 13 Maternal death | 1 | 364 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13.1 Manual acupuncture versus sham control | 1 | 364 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14 Time from trial intervention to birth of baby (days; hours) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 14.1 Manual acupuncture versus sham control | 1 | 45 | Mean Difference (IV, Fixed, 95% CI) | 0.30 [‐2.01, 2.61] |
| 14.2 Electro‐acupuncture versus sham control | 1 | 16 | Mean Difference (IV, Fixed, 95% CI) | ‐62.0 [‐136.99, 12.99] |
| 15 Use of other induction methods | 5 | 1052 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.00 [0.88, 1.15] |
| 15.1 Manual acupuncture versus sham control | 4 | 1036 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.88, 1.15] |
| 15.2 Electro‐acupuncture versus sham control | 1 | 16 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.78 [0.29, 2.06] |
| 16 Length of labour | 3 | 694 | Mean Difference (IV, Random, 95% CI) | ‐36.74 [‐125.07, 51.59] |
| 16.1 Manual acupuncture versus sham control | 2 | 678 | Mean Difference (IV, Random, 95% CI) | ‐20.92 [‐127.76, 85.92] |
| 16.2 Electro‐acupuncture versus sham control | 1 | 16 | Mean Difference (IV, Random, 95% CI) | ‐141.60 [‐382.01, 98.81] |
| 17 Spontaneous vaginal delivery | 3 | 495 | Risk Ratio (M‐H, Random, 95% CI) | 1.21 [0.93, 1.57] |
| 17.1 Manual acupuncture versus sham control | 2 | 435 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.96, 1.22] |
| 17.2 Laser acupuncture versus sham control | 1 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 2.50 [1.31, 4.77] |
Comparison 2. Acupuncture versus usual care.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Caesarean section | 8 | 760 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.51, 1.17] |
| 1.1 Manual acupuncture versus usual care | 5 | 433 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.63, 1.92] |
| 1.2 Electro‐acupuncture versus usual care | 3 | 327 | Risk Ratio (M‐H, Random, 95% CI) | 0.54 [0.37, 0.80] |
| 2 Cervical maturity within 24 hours (Bishop score) | 1 | 67 | Mean Difference (IV, Fixed, 95% CI) | 1.30 [0.11, 2.49] |
| 2.1 Electro‐acupuncture versus usual care | 1 | 67 | Mean Difference (IV, Fixed, 95% CI) | 1.30 [0.11, 2.49] |
| 3 Oxytocin augmentation | 4 | 461 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.90, 1.34] |
| 3.1 Manual acupuncture versus usual care | 2 | 190 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.80, 1.25] |
| 3.2 Electro‐acupuncture versus usual care | 2 | 271 | Risk Ratio (M‐H, Random, 95% CI) | 1.33 [0.95, 1.86] |
| 4 Epidural analgesia | 6 | 555 | Risk Ratio (M‐H, Random, 95% CI) | 0.92 [0.78, 1.07] |
| 4.1 Manual acupuncture versus usual care | 4 | 284 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.76, 1.19] |
| 4.2 Electro‐acupuncture versus usual care | 2 | 271 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.62, 1.42] |
| 5 Instrumental vaginal birth | 6 | 555 | Risk Ratio (M‐H, Random, 95% CI) | 1.11 [0.62, 1.99] |
| 5.1 Manual acupuncture versus usual care | 4 | 284 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.45, 1.67] |
| 5.2 Electro‐acupuncture versus usual care | 2 | 271 | Risk Ratio (M‐H, Random, 95% CI) | 2.30 [1.15, 4.60] |
| 6 Apgar score less than seven at five minutes | 4 | 446 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.34 [0.04, 3.20] |
| 6.1 Manual acupuncture versus usual care | 3 | 242 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.35 [0.01, 8.48] |
| 6.2 Electro‐acupuncture versus usual care | 1 | 204 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.32 [0.01, 7.78] |
| 7 Neonatal intensive care unit admission | 2 | 249 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.27 [0.05, 1.48] |
| 7.1 Manual acupuncture versus usual care | 1 | 45 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.65 [0.03, 14.97] |
| 7.2 Electro‐acupuncture versus usual care | 1 | 204 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.19 [0.02, 1.62] |
| 8 Maternal side effect ‐ maternal infection | 2 | 136 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.64 [0.43, 6.32] |
| 8.1 Manual acupuncture versus usual care | 2 | 136 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.64 [0.43, 6.32] |
| 9 Maternal side effect ‐ perineal tear | 1 | 91 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.95, 1.56] |
| 9.1 Manual acupuncture versus usual care | 1 | 91 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.95, 1.56] |
| 10 Maternal side effect ‐ fetal infection | 1 | 91 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 10.1 Manual acupuncture versus usual care | 1 | 91 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11 Postpartum bleeding > 500 mL | 2 | 256 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.81 [0.36, 1.81] |
| 11.1 Manual acupuncture versus usual care | 1 | 52 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.5 [0.10, 2.50] |
| 11.2 Electro‐acupuncture versus usual care | 1 | 204 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.38, 2.46] |
| 12 Time from trial intervention to birth of baby (days; hours) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 12.1 Manual acupuncture versus usual care | 1 | 44 | Mean Difference (IV, Fixed, 95% CI) | 2.90 [0.66, 5.14] |
| 12.2 Electro‐acupuncture versus usual care | 1 | 56 | Mean Difference (IV, Fixed, 95% CI) | ‐21.0 [‐64.43, 22.43] |
| 13 Maternal satisfaction | 1 | 67 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.99, 1.67] |
| 13.1 Electro‐acupuncture versus usual care | 1 | 67 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.29 [0.99, 1.67] |
| 14 Use of other induction methods | 4 | 259 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.69, 1.45] |
| 14.1 Manual acupuncture versus usual care | 2 | 136 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.62, 1.45] |
| 14.2 Electro‐acupuncture versus usual care | 2 | 123 | Risk Ratio (M‐H, Random, 95% CI) | 0.96 [0.41, 2.23] |
| 15 Length of labour | 1 | 67 | Mean Difference (IV, Fixed, 95% CI) | 124.00 [37.39, 210.61] |
| 15.1 Electro‐acupuncture versus usual care | 1 | 67 | Mean Difference (IV, Fixed, 95% CI) | 124.00 [37.39, 210.61] |
| 16 Spontaneous vaginal delivery | 2 | 117 | Risk Ratio (M‐H, Random, 95% CI) | 1.44 [0.70, 2.98] |
| 16.1 Manual acupuncture versus usual care | 1 | 45 | Risk Ratio (M‐H, Random, 95% CI) | 1.07 [0.77, 1.47] |
| 16.2 Electro‐acupuncture versus usual care | 1 | 72 | Risk Ratio (M‐H, Random, 95% CI) | 2.06 [1.20, 3.56] |
Comparison 3. Acupuncture versus sweeping of fetal membranes.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Caesarean section | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.64 [0.34, 1.22] |
| 1.1 Acupuncture versus sweeping of fetal membranes | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.64 [0.34, 1.22] |
| 2 Oxytocin augmentation | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.66, 1.24] |
| 2.1 Acupuncture versus sweeping of fetal membranes | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.66, 1.24] |
| 3 Epidural analgesia | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.61, 1.49] |
| 3.1 Acupuncture versus sweeping of fetal membranes | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.61, 1.49] |
| 4 Instrumental vaginal birth | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.68 [0.89, 3.14] |
| 4.1 Acupuncture versus sweeping of fetal membranes | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.68 [0.89, 3.14] |
| 5 Apgar score less than seven at five minutes | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.1 Acupuncture versus sweeping of fetal membranes | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Neonatal intensive care unit admission | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.03, 3.12] |
| 6.1 Acupuncture versus sweeping of fetal membranes | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.03, 3.12] |
| 7 Postpartum bleeding > 500 mL | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.32 [0.47, 3.67] |
| 7.1 Acupuncture versus sweeping of fetal membranes | 1 | 207 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.32 [0.47, 3.67] |
Comparison 4. Acupressure versus sham control.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Caesarean section | 2 | 239 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.68, 1.30] |
| 1.1 Acupressure versus sham acupressure | 2 | 239 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.68, 1.30] |
| 2 Oxytocin augmentation | 1 | 130 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.42 [0.96, 2.08] |
| 2.1 Acupressure versus sham acupressure | 1 | 130 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.42 [0.96, 2.08] |
| 3 Instrumental vaginal birth | 1 | 130 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.59, 2.11] |
| 3.1 Acupressure versus sham acupressure | 1 | 130 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.59, 2.11] |
| 4 Meconium‐stained liquor | 1 | 130 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.45 [0.80, 2.62] |
| 4.1 Acupressure versus sham acupressure | 1 | 130 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.45 [0.80, 2.62] |
| 5 Time from trial intervention to birth of baby (hours) | 1 | 109 | Mean Difference (IV, Fixed, 95% CI) | ‐10.51 [‐37.96, 16.94] |
| 5.1 Acupressure versus sham acupressure | 1 | 109 | Mean Difference (IV, Fixed, 95% CI) | ‐10.51 [‐37.96, 16.94] |
| 6 Spontaneous vaginal delivery | 2 | 239 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.79, 1.36] |
| 6.1 Acupressure versus sham acupressure | 2 | 239 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.79, 1.36] |
Comparison 5. Acupressure versus usual care.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Caesarean section | 2 | 151 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.68, 1.53] |
| 1.1 Acupressure versus usual care | 2 | 151 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.68, 1.53] |
| 2 Epidural analgesia | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.49, 1.69] |
| 2.1 Acupressure versus usual care | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.91 [0.49, 1.69] |
| 3 Apgar score less than seven at five minutes | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.0 [0.13, 69.87] |
| 3.1 Acupressure versus usual care | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.0 [0.13, 69.87] |
| 4 Neonatal intensive care unit admission | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.6 [0.16, 2.21] |
| 4.1 Acupressure versus usual care | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.6 [0.16, 2.21] |
| 5 Time from trial intervention to birth of baby (hours) | 1 | 107 | Mean Difference (IV, Fixed, 95% CI) | 10.72 [‐12.00, 35.44] |
| 5.1 Acupressure versus usual care | 1 | 107 | Mean Difference (IV, Fixed, 95% CI) | 10.72 [‐12.00, 35.44] |
| 6 Use of other induction methods | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.64, 2.35] |
| 6.1 Acupressure versus usual care | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.64, 2.35] |
| 7 Spontaneous vaginal birth | 2 | 151 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.69, 1.34] |
| 7.1 Acupressure versus usual care | 2 | 151 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.69, 1.34] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ajori 2013.
| Methods | 80 women randomised to either verum (n = 40) or sham (n = 40) acupuncture | |
| Participants | 80 women with gestational age between 38 and 42 weeks presenting to Tajrish Hospital in Tehran, Iran. Women were included if they had cephalic presentation, cervical dilatation less than 3 cm, intact membrane, and no signs of labour. Women were excluded if they had previous caesarean section or incision of the uterus, multiple pregnancy, malformation of pelvis, skin infections, anticoagulant drug use, psychological disorders, previous inability to tolerate acupuncture, intrauterine growth restriction, suspected macrosomia, indications of emergency termination of pregnancy by induction or caesarean section before onset of labour as described by the American College of Obstetricians and Gynecologists (ACOG), and request of elective termination of pregnancy before 42 weeks of gestation. | |
| Interventions | True acupuncture points included which were located on the Spleen 6 (on the inner ankle), Large intestine 4 (in the webbing between thumb and forefinger) and Bladder 67 (on the outer edge of the little toe), and needles were advanced or manipulated until ‘de qi’ was stimulated. Needles were inserted at all points bilaterally and retained for 30 minutes for both groups. Manual stimulation was provided during the time. The procedure was administered up to a maximum of 2 times over a 1‐week period (every 3 days) and routine prenatal care was continued. Sham acupuncture points included non‐acupuncture points in the hands and legs, and insertion was shallow. |
|
| Outcomes | The primary outcome was initiation of labour, defined as active labour (3 contractions in 10‐minute interval with cervical dilatation 4 to 5 cm) or rupture of membranes. The time from entry (first acupuncture treatment) to delivery, mode of delivery, fetal and maternal outcome, and Apgar scores at 1 and 5 minutes were recorded. | |
| Notes | Study duration 2010 to 2011 Funding: not reported Conflicts of Interest: none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random numbers used. |
| Allocation concealment (selection bias) | Low risk | Allocation concealed within sealed envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants blinded. Acupuncturist not blinded however this should not have influenced the outcome measures recorded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Both outcome assessor and statistician were blinded as to randomisation. All the participants were evaluated for outcomes by 1 gynaecologist. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rate low, 2 women discontinued in the verum group, 3 women in the sham group, therefore similar across both groups with no group‐specific differences in the reason for dropout. |
| Selective reporting (reporting bias) | Low risk | No study protocol published but prospective trial registration showed all outcomes were reported. |
| Other bias | Unclear risk | Insufficent reporting to judge. |
Alsharnoubi 2015.
| Methods | 60 participants randomised to either active laser acupuncture (n = 30) or sham laser acupuncture (n = 30). | |
| Participants | 120 post‐term primigravida women requiring induction of labour were recruited in the antenatal clinic of Gynecology and Obstetrics in the National Institute of Laser Enhanced Sciences (NILES), Cairo University and El Galaa obstetric hospital between March and July 2013. Women were included if they were 40 weeks' gestation, singleton and vertex presentation, with normal fetal heart tracing. Women were excluded if they had twin pregnancy, abnormal fetal presentation, previous uterine scar, inadequate pelvis, severe oligohydramnios, placental insufficiency, or reduced fetal movement. | |
| Interventions | Both groups had 1 treatment session per day for 3 consecutive days. The active laser group was treated by infrared low‐level laser acupuncture with 200‐MW power and 830‐nm wave length, laser was applied on large intestine point number 4 (LI4), spleen point number 6 (SP6), bladder point number 31 and 32 (BL31 and 32) (9), with 0.02 Joule per point for 60 s bilaterally. The sham laser group was treated in the same way as the active group, however the laser was inactive. |
|
| Outcomes | Mode of delivery, frequency of spontaneous labour and neonatal complications, and cervical dilation were assessed in both groups. | |
| Notes | Study duration March to July 2013 Funding: not reported Conflicts of Interest: none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Alternating odd and even numbers (author correspondence). |
| Allocation concealment (selection bias) | High risk | Opaque envelopes used, but in set, nonrandom order. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No CONSORT diagram or data on dropouts provided. |
| Selective reporting (reporting bias) | Unclear risk | No trial protocol published or trial registration found. |
| Other bias | Unclear risk | Insufficient reporting. |
Andersen 2013.
| Methods | 407 women were randomly assigned to acupuncture (n = 100), acupuncture + sweeping of fetal membranes (n = 103), sweeping of fetal membranes (n = 100) or usual care (n = 100). | |
| Participants | 407 women at 41 + 2 to 41 + 4 weeks gestational age, presenting at Hvidovre University Hospital, Odense University Hospital, Odense, and Roskilde University Hospital, Roskilde, Denmark, from 1 January 2007 to 31 November 2009. Women were included if they had an uncomplicated spontaneous singleton pregnancy, a cephalic presentation, intact fetal membranes, and with Danish spoken. Women were excluded if they had used any kind of acupuncture or had sweeping of the fetal membranes within the last 2 weeks. | |
| Interventions | All active groups received usual routine care along with CTG monitoring. The women in the active groups were treated twice during 41 + 3 and 41 + 5 weeks of pregnancy or on the nearest working day. Acupuncture group: the acupuncture needles were placed bilaterally at points LI4, ST36, LR3, BL60, BL31 and BL32. 1 needle was placed at GV20 and 2 needles at right SP6. Electrical stimulation was performed at points BL31 and BL32 bilaterally and at right SP6. The needles were left in place for at least 30 min. Stimulation was performed at a frequency of 80 Hz medium. The needles used were Carbo acupuncture needles (Suzhou Sen Sen, SuZhou, Jiangsu, China), 0.30 x 50 mm at BL31 and BL32 and 0.25 × 25 mm at the remaining points. Sweeping of the fetal membranes was performed by circulating the fingers 3 times between the lower membranes and their attachment to the cervix, separating membranes and the cervix as much as possible. If membrane sweeping was not possible because of a closed cervix, cervical massage was performed by moving the cervix in relation to the pregnancy. The women in the usual care group received the usual CTG during week 41 + 3. |
|
| Outcomes | Spontanous labour, type of delivery (NVD, caesarean section), blood loss, oxytocin augmentation, epidural rate, neonatal outcomes: Apgar score < 7 and NICU admission. | |
| Notes | Acupuncture + sweeping of membranes group was not eligible for comparison in this review. Study duration 1 January 2007 to 30 November 2009 Funding: not reported Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Telephone‐based computer‐randomisation system used. |
| Allocation concealment (selection bias) | Low risk | Central randomisation via telephone system. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Not possible for participants to be blinded, however this was unlikely to affect primary or secondary outcome measures. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The midwives, completing the assessment forms for the trial at labour or induction, were blinded to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rates low (< 5%). Dropout rates not defined between groups, however no evidence of a difference between groups for declining to proceed with intervention. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol or prospective trial registration provided. |
| Other bias | Low risk | Sample size calculation provided and groups balanced at baseline. |
Asher 2009.
| Methods | 89 women were randomised to 3 groups: true acupuncture (TCM) (n = 30), sham (n = 29), control (n = 30). Sample size was determined by 30 participants per group to provide 80% power to detect a 3‐day difference between groups. | |
| Participants | The trial took place at a medical centre in North Carolina, USA. Women included were nulliparous, between 38 and 41 weeks of gestation, able to communicate in English, and at least 18 years old. Exclusion criteria included uncertain dating, transportation difficulties, breech presentation, or a previous inability to tolerate acupuncture. | |
| Interventions | The true acupuncture group received needles bilaterally at LI4, SP6, UB32, and UB54 alongside routine prenatal care. Needles were manually stimulated until de qi was attained and retained for 30 minutes. Treatments were administered for up to a maximum of 5 treatments over a 2‐week period. Acupuncture was performed by 2 licensed acupuncturists. Needles were Seirin J‐type (0.16 mm x 30 mm for hand and leg points, 0.24 mm x 40 mm for back points). The sham acupuncture group received invasive shallow needle insertion at non‐acupuncture points on the hands, legs, and lower back, bilaterally, alongside routine prenatal care. Needles were retained for 30 minutes. Participants enrolled in the true acupuncture or sham acupuncture group received treatment within 30 minutes of enrolment. The control group received routine prenatal care only. |
|
| Outcomes | The primary outcome measure was time from enrolment (first acupuncture treatment) to time of delivery. Secondary outcomes were rates of inpatient induction for post‐term pregnancy, spontaneous rupture of membranes, caesarean section, assisted delivery, chorioamnionitis, endometritis, postpartum haemorrhage or uterine atony, maternal length of stay, intrapartum fetal distress, and neonatal outcomes (e.g. Apgar scores, post‐delivery oxygen requirement). |
|
| Notes | Study duration February 2005 to March 2007 Funding: American Academy of Family Physicians, UNC Dept of Family Medicine, and the NIH National Centre on Complementary and Alternative Medicine (grant K23‐AT001194), Verne S Caviness GCRC at UNC School of Medicine (grant RR00046) Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated numbers using Stata (v8, Statacorp, College Station, TX) in equal blocks of 2 and 4. |
| Allocation concealment (selection bias) | Low risk | Consecutively numbered, sealed, manila envelopes containing the study arm assignment were opened by the principal investigator for each participant after all entry criteria were confirmed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Prenatal care providers and participants were masked to the treatment arm assignment if they were receiving acupuncture (TCM or sham acupuncture) but not if they were in the usual care group. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All charts were reviewed by an investigator who was blinded to treatment arm assignment throughout the data abstraction process. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 woman in the sham group refused any treatments, 1 woman in the routine care group received acupuncture outside of the study. All participants were analysed. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol available. |
| Other bias | Low risk | No imbalance at randomisation. |
Gaudernack 2006.
| Methods | Single‐blind, randomised controlled trial of acupuncture versus standard care. | |
| Participants | 100 Norwegian women were randomised, 48 to the acupuncture group and 52 to the control group. The trial was undertaken in Norway, and included women with a singleton pregnancy, with spontaneous rupture of membranes, cephalic presentation, and at term. Women were excluded if contractions were occurring at least every 10 minutes, lasting more than 30 seconds. | |
| Interventions | The acupuncture intervention included stimulation of acupuncture points LR3, ST36, CV4; in addition, acupuncture points were administered according to the TCM diagnosis. A total of 9 points were used. Needles were retained for 20 minutes. Following treatment, women left the hospital to await onset of labour. Women in the control group received conventional medical treatment including prostaglandins and or oxytocin. |
|
| Outcomes | Oxytocin augmentation, use of other induction agents, time from trial intervention to the birth of the baby, epidural analgesia, instrumental vaginal delivery, maternal side effects (infection), bleeding, tears, birthweight, and Apgar score < 7 at 5 minutes. | |
| Notes | There was no power calculation. Study duration 1 April 2003 to 1 February 2005 Funding: not reported Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The trial generated a computer‐generated, randomisation schedule. |
| Allocation concealment (selection bias) | Low risk | Randomisation was concealed in sealed envelopes. Allocation was undertaken by the midwife. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | There was no blinding of participants due to the usual care group, however, this was unlikely to affect the primary outcome. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It was unclear if the outcome assessor and analyst were blind to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 5 women excluded from analysis in the acupuncture group, 1 due to wrong treatment allocation and 4 had caesarean delivery. 4 women were excluded from the control due to caesarean delivery. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol available. |
| Other bias | Unclear risk | Intention‐to‐treat not reported. Baseline characteristics not reported. |
Gaudet 2008.
| Methods | 16 participants were randomised to receive either true acupuncture or sham acupuncture. | |
| Participants | The study took place in an obstetrics clinics in Canada. Women who were 39 + 0 and 40 + 3 weeks' gestation were approached. Inclusion criteria included nulliparity, an uncomplicated singleton gestation, provision of informed consent, a Bishop’s score of < 7 prior to randomisation, and reassuring fetal status. All interested participants underwent a digital cervical examination by the research nurse prior to randomisation in order to determine the Bishop’s score. If the Bishop’s score was < 7, participants underwent an ultrasound to complete a biophysical profile and an amniotic fluid index. Participants were randomised if they had a biophysical profile score of 8/8 and a normal amniotic fluid index. | |
| Interventions | 2 appointments for acupuncture sessions were arranged, the first within 2 to 3 days, and the second within 1 week, with an accredited physiotherapist acupuncturist. The true acupuncture group received electro‐acupuncture at SP6, ST43 and UB60 with manual stimulation of LI4. Participants received electro‐stimulation on 4 points at 1‐2 Hz for 30 to 45 minutes. The sham acupuncture group received acupuncture at sites adjacent to the acupuncture sites. These were not known to have an effect on initiation of labour or to be located on actual acupuncture meridians. The sites used were SP6+, LI4+, ST43+, BL60+ and GB36+. The locations were SP6+: above the anterior ankle joint line slightly lateral to the border of the tibia, LI4+: in the centre of the anatomical snuff box (located between the 1st and 2nd metacarpal bones), ST43+: at the joint line of the ankle superior to the web space of the 3rd and 4th metatarsal bones, BL60+: inferior and posterior to the fibula head, and GB36+: also inferior and posterior to the fibula head. Sham sites were stimulated in the same order as the true acupuncture sites. Electro‐stimulation was applied as in the treatment group. Both groups were instructed in acupressure and encouraged to apply acupressure every few hours for approximately 3 to 5 minutes, at the most important sites (LI4 and SP6, or corresponding sham sites). |
|
| Outcomes | The primary outcome was time from first acupuncture treatment to delivery. Secondary outcomes included the need for standard methods for induction of labour, duration of active labour, the need for standard pain relief, and the incidence of non‐reassuring fetal heart rate in labour. | |
| Notes | Intention‐to‐treat analysis conducted. Study duration February 2004 to October 2005 Funding: not reported Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was performed using a table of random numbers. |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered sealed opaque numbers. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants blinded using sham acupuncture, clinicians administering the treatment not able to be blinded but were blinded to all obstetrical parameters. The obstetric care providers were blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The trial researchers were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No participants lost. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol available. |
| Other bias | Low risk | No difference in baseline characteristics. |
Gregson 2015.
| Methods | 130 women were randomised to either acupressure (n = 70) or sham acupressure (n = 60). | |
| Participants | 131 women of > 41 weeks gestational age presenting at the Maidstone Birth Centre, Maidstone and Tunbridge Wells NHS Trust, UK between July 2012 and September 2014. Women were included if they had a singleton pregnancy at 41 completed weeks or more of pregnancy, cephalic presentation, and no significant maternal, fetal, or medical condition. Women were excluded from the study if they had any previous significant cervical treatment such as cone biopsy, signs that labour had started (including regular, painful contractions, spontaneous rupture of the membranes) or had previously used a complementary therapy or natural remedy to start labour in this pregnancy (e.g. raspberry leaf tea). | |
| Interventions | Both groups received a membrane sweep prior to joining the study. Acupressure group: 20 intermittent presses on SP6 and LI4 initially. Women were then instructed to continue the treatment at home by stimulating these points 4 times per day. Sham acupressure group: 20 intermittent presses on the patella and then the olecranon initially. Women were then instructed to continue the treatment at home by stimulating these points 4 times per day. |
|
| Outcomes | Time from beginning of treatment to commencement of labour, induction of labour, oxytocin augmentation, mode of delivery, analgesia use, duration of labour, caesarean section rate, meconium liquor, NICU admission, Apgar scores, maternal satisfaction. | |
| Notes | Study duration July 2012 to September 2014 Funding: not reported Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random number table used. |
| Allocation concealment (selection bias) | Low risk | Consecutively numbered, opaque, sealed envelopes drawn in consecutive order by the midwife, who was unaware which agent was allocated until the envelope was opened. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants blinded. Midwife demonstrating the intervention was not blinded but unlikely to have influenced the outcome even if group allocation was disclosed. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The investigators were blind to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rate was low and not different between groups. 1 participant went in to labour before treatment was given, and was therefore excluded from the analysis. 2 women required a caesarean section prior to labour (either spontaneous or induced), however these were included in the intention‐to‐treat analysis. |
| Selective reporting (reporting bias) | Low risk | No study protocol published however comprehensive outcome reporting was undertaken. |
| Other bias | Low risk | Sample size calculation provided, small baseline imbalances between groups, but unlikely to have influenced outcomes. |
Gribel 2011.
| Methods | 72 multiparous or nulliparous pregnant women were randomised to receive either acupuncture or misoprostol. | |
| Participants | The study took place in a maternity hospital in Brazil. Women were included if they had a Bishop's score < 7, single cephalic presentation with gestational age confirmed by ultrasound, with normal ranges for reactive cardiotocography, amniotic fluid volume, blood pressure (< 110 and < 160 mmHg), controlled diabetes, and estimated fetal weight. Women with contraindications for vaginal delivery were excluded. | |
| Interventions | The acupuncture group received acupuncture at: LI4, ST36, LR3, SP6, UB23, and UB32. Points were bilaterally electro‐stimulated using 2 distinct frequencies (5 and 50 Hz) that alternated every 7 pulses for 30 minutes. Electro‐acupuncture was performed using a (DIAN series # NS AH1405) pulse generator. The electric current intensity was slowly increased until it could be felt by each participant, although without discomfort (30 min) in the ventral (in lying down position with 30° dorsal elevation) and in the dorsal points (in the sit down position). Stimulation was performed every 7 hours in 1 up to 3 sessions in a 24‐hour period of hospitalisation to all 6 points. Needles were 0.25 x 30. Only 1 physician, with 10 years experience in providing acupuncture to pregnant women, provided the acupuncture. The control group received misoprostol (25 mg intravaginally; every 6 hours; up to 4 tablets) within 24 hours. |
|
| Outcomes | Primary outcome: successful induction of vaginal delivery within 24 hours. Secondary outcomes: labour induction; induction and labour duration; caesarian section rate; and initial and final Bishop's score (defined as the scores at the end of the protocol, or at the beginning of labour). Labour was defined as two to three contractions of 30 to 40 seconds duration every 10 minutes for more than 60 minutes, with a 2 or 3 cm dilation of cervix in multiparous or nulliparous women, patient satisfaction. |
|
| Notes | Study duration January 2007 to February 2009 Funding: not reported Conflicts of Interest: none. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated, Internet‐based block randomisation. |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes were used. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants and clinicians were not blinded, however, this was unlikely to affect the primary outcomes. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessors were blinded (information attained through email correspondence with the author). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3 participants from the misoprostol group were excluded, 2 refused to participate and 1 used a dosage different to the study protocol. 2 participants were excluded from the acupuncture group as they used misoprostol during their hospital stay. These participants that were excluded after randomisation were not included in the final analysis. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol available. |
| Other bias | Low risk | No imbalance at randomisation. |
Harper 2006.
| Methods | Single‐blind, randomised controlled trial of acupuncture versus standard care. Group assignment was made by the principal investigator after entry criteria were confirmed. | |
| Participants | 56 women were randomised to the trial. The trial was undertaken in an outpatient clinic at the University of North Carolina, USA. Women were included if they were primiparous, with a Bishop's score < 7, between 39 and 4 days to 41 weeks, with a cephalic presentation. Women were excluded if they had a contraindication to vaginal delivery, uncertain dating, or an inability to tolerate acupuncture. | |
| Interventions | The intervention group involved acupuncture administered for 3 out of 4 consecutive days from the first day of enrolment. A licensed TCM acupuncturist administered the acupuncture. Acupuncture was administered bilaterally to LI4, SP6, UB31, and 32. Electro‐acupuncture was administered to the sacrum UB31 and 32 points with current at 2 Hz during the 30‐minute treatment. Needles were retained for 30 minutes. The control group received routine care (not specified). |
|
| Outcomes | Caesarean section, cervical change, time from administration of acupuncture to delivery, mode of delivery, spontaneous onset of labour, neonatal complications. | |
| Notes | Pre‐trial power analysis was undertaken. Study duration July 2004 to February 2005 Funding: Bowes Cefalo Young Researcher Award and North Carolina Academic Alliance for Integrative medicine Pilot Funding. Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The trial generated a computer‐generated randomisation schedule. |
| Allocation concealment (selection bias) | Low risk | Randomisation was concealed in sealed envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | It was not feasible for women and therapist to be blind to group allocation, however, this was unlikely to have affected the primary outcome. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It was unclear if the outcome assessor and analyst were blind to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol available. |
| Other bias | Low risk | No imbalance at randomisation. |
Long 1994.
| Methods | This trial compared pregnant women receiving auricular acupressure and rivanol with a control group who received rivanol only. | |
| Participants | 400 women were recruited from China. No other details were provided. | |
| Interventions | Auricular acupuncture was applied to points: Inner genitals, Sympathetic, Shenmen, Liver, Yuanzhong and Adrenal gland, using a white mustard seed or a pill with adhesive plaster. The points were pressed by the woman until the points felt warm, and distention and a numb sensation was generated. The control group received 1% rivanol. | |
| Outcomes | Time to induce labour, amount of bleeding, length of labour, and mental state of the woman. | |
| Notes | Contact was attempted with the author; it was advised the author had retired, and no contact could be established. Study duration not reported Funding: not reported Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Women were equally divided into the 2 groups, no further details provided. |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not stated |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not stated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not stated |
| Selective reporting (reporting bias) | Unclear risk | Not stated |
| Other bias | Unclear risk | Not stated |
Mackenzie 2011.
| Methods | This was a double‐blind manual, electro‐ and sham acupuncture study comparing acupuncture with a control group for analgesia for labour induction. | |
| Participants | Nulliparous women from the United Kingdon with a singleton pregnancy and fetal cephalic presentation with intact membranes undergoing labour induction using vaginal prostaglandins and low amniotomy were eligible for the study. Women with a previous experience of acupuncture were excluded. | |
| Interventions | 105 women were randomised to receive manual acupuncture, electro‐acupuncture, sham acupuncture, sham electro‐acupuncture, or no treatment. In the manual acupuncture and electro‐acupuncture groups, the following points were needled: LI4, SP6, UB60, UB67. Serin needles (0.20 x 30 to 0.30 x 50 mm) were inserted to a depth of 15 to 20 mm with de qi sensation attained. In the manual group, needles were stimulated intermittently and irregularly by hand for 30 minutes. In the electro‐acupuncture group, points were stimulated by an electrical stimulator with 2‐Hz pulses of 0.5 millisecond duration for 30 minutes, sufficient to cause non‐painful muscle contractions. In the sham acupuncture group, needles were inserted at sites adjacent to the specific acupuncture points to a depth of 1 to 1.5 mm only and insufficient to provoke an unusual sensation. The sham electro‐acupuncture group were connected to a electrical stimulator but the current was not activated. Intrapartum care was provided by the routine delivery suite staff. Subsequent pain management including aromatherapy, TENS and parenteral opioids, and regional blockade was provided when requested or recommended by the attending midwife or obstetrician. |
|
| Outcomes | The primary outcome was the rate of intrapartum epidural analgesia requirement. Other outcomes included caesarean section, instrumental delivery, length of labour, Apgar scores. | |
| Notes | A power calculation was done based on the reduction in epidural rates. Study duration not reported Funding: a grant from Oxfordshire Health Services Research Committee and the Uterine Contractility Trust Fund Conflicts of Interest: none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random numbers were generated using a computer program (RALLOC, Stata Corporation, Singleton, TX, USA) and randomisation was stratified by the acupuncturist. |
| Allocation concealment (selection bias) | Low risk | Allocations were concealed in numbered sealed opaque envelopes opened only after consent and immediately before treatment. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Study allocation was concealed from all except the acupuncturist, who was not involved with intrapartum management (double‐blind). Women randomised to the ‘no‐treatment’ control group were aware of their treatment group (single‐blind). Great care was taken to conceal treatment allocation from those providing intrapartum care. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Attempts to ensure outcome assessment was blind to group allocation. The randomisation code was only revealed after completion of the clinical study. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participant data were included in the analysis. 2 protocol violations, 1 woman randomised to control group received acupuncture, and a second woman was randomised to electro‐acupuncture but withdrew from the study before the acupuncture was administered. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported as per outcomes stated on trial registry. |
| Other bias | Low risk | No imbalance at randomisation. |
Martinez 2004.
| Methods | Acupuncture versus no treatment to examine the effect on uterine contractions. | |
| Participants | The Obstetrics Outpatient Department of a university hospital in the Phillipines. 50 pregnant women who were term, singleton, not in labour, and with an uncomplicated course of pregnancy were included in the study. Exclusion criteria: women who were in the active phase of labour, who had previous caesarean section, PROM, concomitant medical illness, or allergy to metals, such as chromium or zinc. |
|
| Interventions | Spleen 6 (point Sanyinjiao), on the lower leg approximately 3 inches proximal to the centre of the medial malleolus, was stimulated bilaterally. SP6 was pierced on both sides of the lower extremities. 2 minutes were allotted for each participant for the insertion of the acupuncture needle. The control group received no intervention. | |
| Outcomes | The frequency, intensity, duration, and interval of uterine contractions were measured for 20 minutes. No outcomes relevant to the review were reported. | |
| Notes | The trial did not report on any outcomes relevant to this review. Study duration January to November 2003 Funding: not reported Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Partcipant and clinician not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Complete data, no losses |
| Selective reporting (reporting bias) | Low risk | Single outcome collected relating to uterine contractions |
| Other bias | Low risk | No imbalance at randomisation |
Modlock 2010.
| Methods | Acupuncture versus sham noninvasive acupuncture. | |
| Participants | The study was undertaken in Aarhus University Hospital, and Herning Hospital, Denmark, 1/2/2007 to 31/5/2008. 125 healthy pregnant women at gestational week 41 + 6 were recruited to the study. Exclusion criteria: woman did not speak or understand the Danish language; multiple pregnancy; PROM or contractions at 4‐ to 5‐minute intervals and increasing in intensity; previous caesarean section; diseases of the mother or unborn child (diabetes, pre‐eclampsia, diseases of the heart, liver or kidneys, HIV/AIDS, malformation of the pelvis, psychological disorders, intrauterine growth restriction, hydrocephalus, suspected macrosomia, fetal malposition, antepartum stillbirth, treatment with anticoagulants, skin infections, allergy to metal, or major complications at previous delivery, such as low Apgar score. |
|
| Interventions | Acupuncture was administered to points BL67, LI4, SP6, GV20. The control used the Park sham needle (noninvasive) at real acupuncture points BL67, LI4, SP6, GV20. The Park supporting device was used to hold the needle in place for both groups. The intervention was delivered by trained midwives. The intervention was administered over 30 minutes, and needles were stimulated every 10 minutes. Treatment commenced at 8.00 am, and if the primary endpoint had not occurred by this time, the treatment was repeated at 2.30 pm. |
|
| Outcomes | The primary outcome was achieved if the participant had undergone delivery or was in active labour, defined as rupture of fetal membranes and/or contractions at 4‐ to 5‐minute (or more frequent) intervals, and increasing in intensity within 24 hours. Secondary outcomes were: the cervical dilatation was sufficient for amniotomy, cervical length and dilatation, length of labour, time from randomisation to start of active labour, postpartum bleeding, use of epidural, augmentation of contractions and instrumental delivery, as well as neonatal outcomes, such as Apgar score and umbilical pH value, when available. |
|
| Notes | Power analysis undertaken. Study duration 1 December 2005 to 31 May 2008 Funding: The Midwifery Union, Denmark, The Skejby Research Fund, Aase and Ejnar Danielsens Funds, Timber Merchant Vilhelm Bangs Fund and the County of Ringkjobing Research Fund. Conflicts of Interest: none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Central computer‐generated. |
| Allocation concealment (selection bias) | Low risk | Phone service. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Acupuncturist not blind. Blinding failed in 6 cases, 2 informed by partners (evenly distributed by group). 4 randomisations and administration of treatment was undertaken by the same midwife. Most women did not know which group they were in. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Principal investigator and nurses gathering data were blind to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1 lost to follow‐up in the acupuncture group, and 2 lost to follow‐up in the control group. 12 protocol violations in the acupuncture group, and 7 in the control group. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported as per entry on trial registry. |
| Other bias | Low risk | No imbalance at randomisation. |
Mollart 2016.
| Methods | 44 women were randomised to either acupressure (n = 22) or standard care (n = 22). | |
| Participants | 44 primigravid women > 40 weeks + 5 days gestational age presenting at 2 outer metropolitan public hospitals in New South Wales, Australia between 13 February to 30 August 2013. Women were included if they had a singleton pregnancy; cephalic fetal presentation; English speaking; ≥ 18 years; and receiving midwifery‐led antenatal care. Women were excluded if they were wanting to use or currently using acupressure (due to concern of cross‐over after randomisation); experiencing regular uterine contractions; any contraindications for vaginal birth; and highly dependent on medical care/requiring specialist medical/obstetric consultation and likely to have medical intervention prior to 41 completed weeks of gestation. | |
| Interventions | In addition to standard care, women randomly allocated to the acupuncture group received verbal and written information on the self‐administration of acupressure to 3 acupoints spleen 6 (SP6 – lower leg), large Intestine 4 (LI4 – hand) and gall bladder 21 (GB21 – shoulder). The participants were asked to apply sustained bilateral pressure using thumb or finger for: 2 minutes on point SP6 (right/left) followed by 2 minutes on LI4 (right/left) every 2 hours during the day; and 2 minutes on point GB21 (right/left) twice a day (morning and evening). Women randomly allocated to the control group received standard clinical antenatal care at either of the 2 study sites. Each woman was advised of her next clinic (Day Assessment Unit (DAU)) appointment at approximately 40 weeks + 10 days (±2 days) for a maternal and fetal assessment that included abdominal palpation, vaginal examination to determine cervical favourability for induction of labour (Bishop's score), and fetal heart pattern (electronic monitoring). This assessment determined the method of medical induction and set an induction date before 40 weeks and 14 days. |
|
| Outcomes | Spontanous onset of labour, mode of birth, use of analgesia, mean birthweight, Apgar score and NICU admission. | |
| Notes | Study duration 13 February to 30th August 2013 Funding: NSW Ministry of Health Nursing and Midwifery Office, Australian College of Midwives, NSW Branch, and Central Coast Local Health District Conflicts of Interest: none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The research assistant provided the woman's hospital medical record number and eligibility criteria, the allocation service randomised the woman based on a block size of 4 and immediately provided the group allocation. |
| Allocation concealment (selection bias) | Low risk | Allocation concealment was assured by using a remote internet‐based allocation service. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participant blinding not possible, however unlikely to have influenced outcomes. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The staff providing clinical care were unaware (blinded) of group allocation unless the participant disclosed study participation. Data were analysed by a statistician blinded to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts in either group. |
| Selective reporting (reporting bias) | Unclear risk | No protocol published; prospective trial registration was undertaken. This was not specific on outcomes but all typical outcomes were reported. |
| Other bias | Low risk | Sample size calculation performed. Baseline imbalance between groups, however, unlikely to have affected outcome. |
Neri 2014.
| Methods | 202 women were randomised to receive either acupuncture (n = 101) or observation (n = 101). | |
| Participants | 202 women with a gestational age ranging between 40 + 2 and 40 + 5 weeks who were referred to the Midwife‐Led Delivery Unit at the Mother‐Infant Department of the University of Modena and Reggio Emilia. Women were included if they had a low‐risk singleton pregnancy, intact membranes, planned delivery at the Unit and gestational age ranging between 40 + 2 and 40 + 5 weeks, as estimated by ultrasound before the 12th week. Women were excluded if they had maternal disorders, previous uterine surgery, contraindications to vaginal delivery, and Bishop's score 6. | |
| Interventions | The acupuncture interventions (performed by a licensed acupuncturist, I.N.) consisted of the insertion of sterile, disposable 0.30 4 mm acupuncture needles (Huanqiu, Qiu Tian, S.Marino) into LI4, SP6, ST36, GB34, LIV3, PC6. After reaching the de qi sensation, needles were left in situ for 30 to 40 minutes. During the session, women were positioned in a right lateral position in a comfortable, quiet room. Sessions of acupuncture were planned every odd day from the randomisation till 41 weeks plus 4 days. The observation group had a serial non‐stress test (40 + 2 and 40 + 4) and an NST and amniotic fluid index evaluations (41 and 41 + 3). These were also carried out in the acupuncture group. |
|
| Outcomes | Length of labour, caesarean section rate. | |
| Notes | Study duration not reported Funding: not reported Conflicts of Interest: none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | A computer‐generated randomisation list, in which odd and even numbers allocated participants to observation or active treatment, was employed. |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | No blinding reported, however unlikely to have affected outcomes. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of assessors not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low dropout rate (< 10%), with small differences between groups which were unlikely to have been related to group allocation. |
| Selective reporting (reporting bias) | Unclear risk | No protocol published. Prospective registration but no specific information on outcomes listed on Clinicaltrials.gov. |
| Other bias | Unclear risk | No sample size calculation reported, insufficient reporting of baseline demographics. |
Rabl 2001.
| Methods | Women were randomised to acupuncture or no acupuncture. | |
| Participants | 56 women were randomised to the trial in Austria. Inclusion criteria were EDC confirmed by ultrasound, uncomplicated pregnancy, and singleton pregnancy with cephalic presentation. Exclusion criteria were cervical dilatation greater than 3 cm, PROM, previous caesarean section, and maternal complications, e.g. pre‐eclampsia, fetal growth retardation. Women were randomised at term. | |
| Interventions | All women were examined at term and at 2‐day intervals thereafter. Fetal heart rate was monitored, the cervical length was measured by ultrasound, cervical mucus was obtained for fetal fibronectin test, and the cervical status was assessed for the Bishop's score. Women received acupuncture at term and at 2‐day intervals thereafter. Acupuncture points ‐ LI4, and SP6 were bilaterally inserted. De qi needling sensation was achieved. Needles were left in for 20 minutes. If the woman was undelivered 10 days after her EDC, labour was induced. The control group received routine care. |
|
| Outcomes | The change in cervical length over time, time from the first fibronectin test to delivery, time period from EDC to time of delivery, number of post‐date indications, length of first and second stage of labour, need for oxytocin augmentation, and mode of delivery. | |
| Notes | No sample size calculation. 11 (20%) women were excluded and follow‐up data were not available on these women. Intention‐to‐treat analysis was reported. Study duration not reported Funding: not reported Conflicts of Interest: none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The trial used a central randomisation service, with computer‐generated sequence of random numbers. |
| Allocation concealment (selection bias) | Low risk | Central randomisation service (central allocation). |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | The study participants were not blind to their group allocation. The care providers were blind to the woman’s study group. This was unlikely to have affected the primary outcomes. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | The outcome assessors and statistician were not blind to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | There were 11 (20%) post‐randomisation exclusions and losses to follow‐up. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol was available. |
| Other bias | Unclear risk | Limited reporting, and unable to assess. |
Romer 2000.
| Methods | Randomised controlled trial of acupuncture, and control using nonspecific acupuncture to examine the effect on cervical maturation and duration of labour. A nonrandomised usual care group was recruited to the study. | |
| Participants | 553 women were randomised to the trial at a Uni‐centre hospital in Mannheim, Germany. Women were primiparous, with exclusion criteria stated as multiple pregnancy, placenta previa, planned caesarean section, any bleeding after 28 weeks, and any coagulation disorder. | |
| Interventions | Acupuncture was administered weekly from 36 weeks until delivery. For the treatment group, fixed acupoints were administered including: ST36, SP6, GB34, BL67. Control acupuncture used nonspecific acupuncture including GC20, PC6, HT7. Points were needled using tonifying techniques, with a treatment duration of 20 minutes. | |
| Outcomes | Bishop's score, length of cervix, duration of labour | |
| Notes | Study duration not reported Funding: not reported Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation using random table numbers. |
| Allocation concealment (selection bias) | Unclear risk | No other details available. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants allocated to acupuncture or the nonspecific acupuncture group were blind to their group allocation. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcome assessor blind to group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There were no dropouts. |
| Selective reporting (reporting bias) | Unclear risk | No details available. |
| Other bias | Unclear risk | No details available. |
Selmer‐Olsen 2007.
| Methods | This was a randomised controlled trial to assess the effect of acupuncture on the onset of labour and the need for induction after pre‐labour rupture of membranes. Women were randomised to receive acupuncture or standard care. | |
| Participants | The study took place in a hospital in Norway between 2004 and 2006. 106 women were included who were nulliparous with an uneventful singleton cephalic pregnancy between 37 and 42 weeks, with confirmed rupture of membranes without contractions of the uterus. | |
| Interventions | All women in the acupuncture group were needled at CV4. Women were then diagnosed into 3 TCM categories based on their constitution. For Spleen qi deficiency, points were UB20, SP6 and ST36. For Liver qi stagnation, points were UB18, LR3, and LI4. For Kidney qi deficiency, points were UB23 and KI3. The following additional points could be used when appropriate: GVl4, GV20, HT7, UB15, LU7, UB32, PC6, TH6. De qi was attained on all points. All Bladder channel points were needled bilaterally, the rest unilaterally. Single use needles (length: 2.5 and 4 cm) were retained for 30 minutes. Women were offered an additional treatment the following day if they were not in labour. The control group received standard care. Standard care for nulliparas was expectant management at home for approximately 48 hours if cardiotocogram, temperature and amniotic fluid were normal, checked on a daily basis. To avoid infection, no digital examination was performed before onset of labour or induction. |
|
| Outcomes | Time from PROM to active phase of labour. The active phase of labour was defined as a cervix dilatation of 3 cm and at least 2 uterine contractions in 10 minutes. The incidence of induction and additional outcomes of birth (Apgar score, epidural, oxytocin, caesarian sections, instrumental delivery) were reported. Self‐reported physical well‐being was registered using a 100‐mm visual analogue scale at randomisation and when they reached the active phase. | |
| Notes | It was unclear who conducted the differential diagnosis to determine treatment and what instrument was used to guide the diagnosis and maximise inter‐rater reliability. Study duration January 2004 to January 2006 Funding: Sandvik forlag Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Internet‐based block randomisation. |
| Allocation concealment (selection bias) | Low risk | Concealed centrally. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | No blinding reported, however unlikely to have affected outcomes. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It was not stated if assessors were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 5 participants were lost to follow‐up, and 1 participant refused further participation. 4 participants were excluded after randomisation, 1 had meconium‐stained waters, 1 did not return the questionnaire, 2 had intact membranes. These participants were not included in the analysis. |
| Selective reporting (reporting bias) | High risk | The outcomes of Apgar score, epidural, instrumental delivery, caesarean sections, inductions, dilatation, and oxytocin were reported but no between‐group analysis was conducted. |
| Other bias | Unclear risk | Baseline characteristics were not reported. |
Smith 2008.
| Methods | Randomised controlled trial of acupuncture versus sham acupuncture sessions to estimate the effectiveness of acupuncture to induce labour. | |
| Participants | The study took place in a Women's and Children's Hospital in Australia between 1998 and 2005. 364 women aged greater than 16 years with a singleton pregnancy and cephalic presentation scheduled for a post‐term induction were recruited to the study. Women were excluded if they were in active labour with regular uterine contractions, if there were contraindications to labour or vaginal birth, or if they presented with spontaneous pre‐labour rupture of membranes. | |
| Interventions | The acupuncture group received acupuncture at LI4, SP6, UB31, UB32, ST36, and LR3. Any underlying pathology from a TCM framework was examined and treated with additional points, e.g. KI7, UB20, UB21, LR3. Needles were retained for 30 to 40 minutes with strong stimulation and de qi. Seirin 1‐2 inch needles were used with a 32 gauge (0.25 mm) diameter. The sham group received the same treatment in terms of timing and duration, but with minimal insertion and stimulation. Sham points were selected on the sacral area, hand, foot, a point below the knee, and lower leg, at points that were not acupuncture points. Treatments were administered over a 2‐day period before the planned induction. |
|
| Outcomes | The primary outcome was the need for induction, a reduction in the need for prostaglandins, oxytocin, and artificial rupture of membranes, change in Bishop's score, time of intervention to time of delivery, and length of active labour. Secondary: methods of pain relief, mode of birth, Apgar scores less than 7 at 5 minutes, admission of the mother and neonate from the labour ward to the postnatal ward together, meconium, nonreassuring fetal heart rate tracing, neonatal jaundice requiring phototherapy, neonatal seizures, acceptability of treatment by the mother, Bishop's score, labour agentry scale of control in childbirth, likes and dislikes regarding participation in the trial. |
|
| Notes | Intention‐to‐treat analysis was conducted. Sample size calculation reported. Study duration May 1998 to February 2005 Funding: Australian National Health and Medical Research Council, the Women’s and Children’s Hospital Foundation, Adelaide, Australia. Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | A computer‐generated randomisation schedule created by an independent statistician in variable block size and stratified by parity (nulliparous and multiparous) and incorporated into a telephone randomisation service. |
| Allocation concealment (selection bias) | Low risk | A central telephone randomisation service was available 7 days a week at the recruiting hospital. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants were blinded to allocation by use of sham control. Caregivers were blind to the women's study group. The treatment allocation was known only to the acupuncturist administering the intervention. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Data collection was done by someone not involved in the administration of the intervention and the analyst was blind until the end of data analysis. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants received at least 1 session in both groups, 11 participants in the acupuncture group received only 1 treatment and 15 women in the sham acupuncture group. Reasons given were problems with childcare, feeling too tired, and lack of transportation to the trial centre. All participants were included in the analysis. |
| Selective reporting (reporting bias) | Low risk | All outcomes reported as per trial registration. |
| Other bias | Low risk | Women in the sham group were older and there were also differences in the categorisation of the Bishop's score. The authors adjusted the primary outcomes for maternal age and the raw Bishop's score. |
Torkzahrani 2015.
| Methods | 150 women were randomised to acupressure performed by the researcher (n = 50), acupressure performed by the mother (n = 50), or a usual care control group (n = 50). | |
| Participants | 150 women with a gestational age of 39 to 41 weeks who were referred to Deziani hospital, Iran between June 2011 to December 2012. Women were included if they were 39 to 41 weeks of gestational age confirmed by first‐trimester ultrasound or normal last menstrual period, normal non‐stress test, age of 18 to 35 years old, low‐risk pregnancy, Bishop's score of ≤ 4, single cephalic presentation, not taking herbal or chemical drugs 36 hours before and up to the end of the study, and not having sexual intercourse 24 hours before and up to the end of study. Women were excluded if they were taking chemical or herbal drugs, having sexual intercourse within 24 hours, or having a high‐risk pregnancy. | |
| Interventions | Both acupressure groups applied pressure to SP6 on the right leg for between 10 seconds to 2 minutes (until half the fingernails turned white). There was a break of the same amount of time as the pressure was applied and this was repeated for 20 minutes in total, once per day. The control group received routine healthcare, however no further details were given. |
|
| Outcomes | Bishop's score | |
| Notes | Study duration June 2011 to December 2012 Funding: not reported Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random number list used but it was unclear from the text how this was generated. |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Acupressure groups had higher dropout rate (10 were reluctant to pursue study) versus no dropouts in the control group. |
| Selective reporting (reporting bias) | Unclear risk | No trial protocol published. |
| Other bias | High risk | Sample size calculation performed but unclear how this was done. Significant demographic imbalances at baseline. |
Torkzahrani 2016.
| Methods | 162 women were randomised to acupressure (n = 54), sham acupressure (n = 55) or usual care control (n = 53). | |
| Participants | 162 women with a gestational age between 39 to 40 weeks who were presented to Shahid Akbar Abadi hospital in Tehran at the Iran University of Medical Sciences, between April 2015 and November 2015. Women were included if they were aged between 18 and 35 years, nulliparous, low‐risk pregnancy, gestational age 39 to 40 weeks as estimated by ultrasound before the 12th week, singleton cephalic presentation, normal BMI, Bishop's score 4, biophysical profile score of 8/8 and a normal amniotic fluid index, not taking herbal or chemical drugs 36 hours before and up to the end of the study, and not having sexual intercourse 24 hours before and up to the end of study. Women were excluded if they were taking chemical or herbal drugs, having sexual intercourse, and not doing acupressure on schedule. | |
| Interventions | In acupressure and sham acupressure groups, pressure was applied on the points for 1 minute and it was interrupted for 1 minute as rest time, so that each point should be pressed 5 times. Acupressure and sham acupressure points were subjected to pressure respectively, and after the completion of acupressure and sham acupressure at each point, the next point was pressed. The total intervention time was 30 min. The bilateral method of pressure was applied on the points with appropriate force (half of the fingernails turned white) and this method was continued to create stimulation reactions such as hotness, drowsiness, soreness, numbness, pinching, and pressing. In the acupressure group, pressure was applied to SP6, BL32 and BL60. In the sham acupressure group, 3 ineffective acupuncture and acupressure points on the hands and legs were pressed. In the control group, women received routine healthcare services. |
|
| Outcomes | Spontanous initiation of labour, caesarean birth, Apgar score, time from initiation of intervention to birth | |
| Notes | Study duration April to November 2015 Funding: not reported Conflicts of Interest: none |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer randomisation system used. |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Blinding not possible with usual care group, however unlikely to have affected any of the outcome measures. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Routine care and data collection was performed by the 2 research assistants (with 10 years of work experience) who were unaware of the research groups. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low loss to follow‐up across all 3 groups. No significant group‐specific reasons for dropouts. |
| Selective reporting (reporting bias) | High risk | Trial registration showed Bishop's score as primary outcome measure, however this was not reported as an outcome in the final paper. Authors contacted to clarify. |
| Other bias | Unclear risk | Sample size calculation provided but in insufficient detail. No baseline imbalances between groups. |
Tremeau 1992.
| Methods | Randomised controlled trial examining the effect of acupuncture on cervical maturation. Parallel design of acupuncture versus usual care and sham acupuncture. | |
| Participants | 128 women met the entry criteria and were randomised. Participants were recruited from a maternity hospital in France. Women were 37 to 38 weeks pregnant with a Bishop's score of less than 4. Exclusion criteria included: at risk of premature delivery, planned caesarean section, placenta previa, and receiving concurrent treatments such as yoga, homeopathy, acupuncture. | |
| Interventions | Acupuncture points were selected based on those used to increase cervical maturation including: CV2, CV3, CV4, Liv3, BL60, GB34, ST36, LI4, SP6, BL67. The acupuncture control was pricked with needles at sites 1 cm from the bilateral acupoint, and 1 cm from the mid‐line points, and a third group received usual care. 3 treatment sessions were administered, with electro‐stimulation for 20 minutes. |
|
| Outcomes | The Bishop's score was assessed 48 hours after the last acupuncture session, duration of labour, and time to 2 cm cervical dilatation. | |
| Notes | Study duration 1st February to 30th October 1990 Funding: not reported Conflicts of Interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No details were reported on whether the integrity of blinding between acupuncture and the sham group was maintained. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The outcome assessment was undertaken by a clinician blind to group. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 16% of women did not complete the protocol due to spontaneous labour before the second examination, 2 women declined the second examination, and 1 woman did not return for acupuncture. |
| Selective reporting (reporting bias) | Unclear risk | Limited reporting and unable to assess. |
| Other bias | Low risk | No imbalance in baseline characteristics. |
ACOG:American College of Obstetricians and Gynecologists AIDS: Acquired Immune Deficiency Syndrome CTG: Cardiotocography DAU: Day Assessment Unit EDC: estimated date of confinement HIV: Human Immunodeficiency min: Minute NICU: Neonatal Intensive Care NST: Non Stress Test NVD: Normal Vaginal Delivery pH: potentia hydrogenii PROM: premature rupture of membranes TCM: traditional Chinese medicine TENS: transcutaneous nerve stimulation
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Aghamohammadi 2011 | This was a randomised double‐blind study comparing TENS versus sham TENS on LI4 and SP6 in 64 nulliparous women who were in the first stage of active labour. Labour time was found to be significantly shorter in the TENS group as was the need for oxytocin to augment labour. The trial was excluded as it did not meet the inclusion criteria of an acupuncture intervention ‐ no needles were used and it did not have a primary outcome that met our inclusion criteria. |
| Bo 2006 | This study evaluated the role of acupuncture primarily during labour on pain relief. No data on induction outcomes were reported. |
| Dorr 1990 | No mention of randomisation and unable to contact authors for clarification. |
| Dunn 1989 | This comparison between electrical acupuncture stimulation or placebo acupuncture assessed the onset of uterine contractions in 20 post‐date pregnant women. There was evidence of strong contractions in the treatment group. TENS did not meet the eligibility criteria for the review. |
| Kubista 1974 | The study was not a randomised controlled trial. This study reported on 60 pregnant women who received acupuncture (ST36, KI8, GB34 and UB 62) compared to a control of 60 pregnant women from the same clinic with a primary outcome of length of labour. |
| Levett 2016b | This study used a combination of interventions including yoga, acupressure, and visualisation. Separating the effect of acupressure alone was not possible. |
| Li 1996 | This study was not a randomised trial and was excluded. |
| Li 2007 | This study examined the effect of acupuncture on mid‐trimester early labour. |
| Liu 2012 | This trial included women who were already in labour and was therefore excluded. |
| Lyngso 2010 | This trial included women who were already in labour and was therefore excluded. |
| So 1979 | No mention of randomisation and unable to contact authors for clarification. |
| Teimoori 2015 | This study examined the effect of Shiatsu, which did not meet the eligibility criteria of this review. |
TENS: transcutaneous nerve stimulation
Characteristics of ongoing studies [ordered by study ID]
NCT00379327.
| Trial name or title | Acupuncture for promotion of timely delivery |
| Methods | Randomised controlled trial |
| Participants | Women at 37 + 3 gestational age |
| Interventions | Acupuncure versus placebo (non‐penetrating) acupuncture. Acupuncture (verum or placebo) administered twice weekly for 30 minutes until onset of labour. |
| Outcomes | 'Timely delivery' ‐ delivery on or before the estimated date of confinement. Secondary outcomes related to cervical ripening, and anxiety around labour and birth. |
| Starting date | January 2006. Terminated 2010. |
| Contact information | John T Farrar (jfarrar@mail.med.upenn.edu) |
| Notes | Study was not completed. PI left institution prior to completing trial and original data were lost in a home disaster. |
NCT01052857.
| Trial name or title | Efficacy of acupuncture on induction of labour |
| Methods | Randomised controlled trial |
| Participants | Women at 40 + 2 to 40 + 4 gestational age |
| Interventions | Acupuncture versus placebo. Acupuncture administered daily from 40 + 4 for 7 days. |
| Outcomes | To evaluate the efficacy of acupuncture administered daily from 40 weeks + 4 days of gestation for induction of labour with respect to placebo, to evaluate safety of acupuncture. |
| Starting date | November 2007. Completed January 2009. |
| Contact information | Facchinetti Fabio, University of Modena and Reggio Emilia, Italy. |
| Notes | The purpose of this study was to evaluate the efficacy and safety of acupuncture for the induction of labour in pregnant women at the 40 weeks + 4 days of gestation. |
NCT02392988.
| Trial name or title | Does acupuncture therapy reduce the need for labor induction after postdate (week 41). |
| Methods | Randomised controlled trial |
| Participants | Women with post‐term pregnancy (> 40 weeks gestational age) |
| Interventions | Verum acupuncture versus sham acupuncture versus no treatment control. Verum and sham acupuncture treatment was to be delivered every 48 to 72 hours, for a maximum of 3 treatments. Sham treatment was to be given on points on the back, on non‐acupuncture points. |
| Outcomes | Number of women receiving induction. Secondary outcomes included number of women who had SROM or AROM, duration of labour, time from treatment till labour, epidural rate, and Apgar score. |
| Starting date | May 2015 |
| Contact information | Liat Edry, PhD (liatedry@gmail.com) |
| Notes | Not currently showing as recruiting. |
NCT02394041.
| Trial name or title | A randomised controlled multicentre trial evaluating the efficacy of acupuncture versus placebo on the caesarean section rate in case of cervical dystocia in full‐term pregnancy |
| Methods | Randomised controlled trial |
| Participants | Women at 37 weeks (+/‐ 2 days) |
| Interventions | Acupuncture versus sham acupuncture versus standard care. 3 acupuncture sessions, 1 per week with 1 or more sessions being performed during delivery. Type of sham needle not described. |
| Outcomes | Caesarean section rate |
| Starting date | November 2012 |
| Contact information | Denis Colin MD, Department of Obstetrics, Hôpital Saint‐Cloud |
| Notes | Study terminated due to insufficient recruitment: 142 participants instead of 2220 planned. |
AROM: artificial rupture of membranes PI: principal investigator SROM: spontaneous rupture of membranes
Differences between protocol and review
Methods were updated to current Cochrane Pregnancy and Childbirth Group standard text. Normal vaginal delivery was added as a secondary outcome measure in this update.
In this update, we added the following planned subgroup analyses to the methods.
Trials that recruited and treated women prior to due date (< 40 weeks) versus those that treated women with a combination of pre and post‐date or post‐date alone.
Trials that provided separate outcome data for primiparous and multiparous women.
Manual acupuncture versus electro‐acupuncture.
In this 2017 update, the control comparisons of sham acupuncture and usual care appeared as separate comparisons, rather than subgroups of the same comparison.
Contributions of authors
Caroline Smith conceptualised and took the lead in writing the protocol, the original review, and subsequent updates. She performed initial searches of databases for trials, was involved in selecting trials for inclusion, performed data extraction and quality assessment of the included trials, was responsible for statistical analysis and interpretation of the data, and wrote the first draft of this update.
Mike Armour was involved in searching databases for trials, selection and screening of trials, data extraction and quality assessment of trials. He performed the statistical analysis on this update and provided editing and contribution to both the draft and final version of this updated manuscript.
Hannah Dahlen was involved in editing both the draft and final version of this manuscript.
Sources of support
Internal sources
University of Western Sydney, Australia.
University of Adelaide, Australia.
External sources
No sources of support supplied
Declarations of interest
Caroline Smith: is an author of one of the included trials (Smith 2008), and so a third independent person assessed and extracted data for this trial.
Mike Armour: is an acupuncturist recently involved in clinical practice and the director of an acupuncture clinic.
Hannah Dahlen: none known.
New search for studies and content updated (conclusions changed)
References
References to studies included in this review
Ajori 2013 {published data only}
- Ajori L, Nazari L, Eliaspour D. Effects of acupuncture for initiation of labor: a double‐blind randomized sham‐controlled trial. Archives of Gynecology and Obstetrics 2013;287(5):887‐91. [DOI] [PubMed] [Google Scholar]
Alsharnoubi 2015 {published data only}
- Alsharnoubi J, Khattab A, Elnoury A. Laser acupuncture effect on fetal well‐being during induction of labor. Lasers in Medical Science 2015;30(1):403‐6. [DOI] [PubMed] [Google Scholar]
Andersen 2013 {published data only}
- Andersen BB, Knudsen B, Lyndrup J, Faelling AE, Illum D, Johansen M, et al. Acupuncture and/or sweeping of the fetal membranes before induction of labor: a prospective, randomized, controlled trial. Journal of Perinatal Medicine 2013;41(5):555‐60. [DOI] [PubMed] [Google Scholar]
Asher 2009 {published data only}
- Asher GN, Coeytaux RR, Chen W, Reilly AC, Loh YL, Harper TC. Acupuncture to initiate labor (Acumoms 2): a randomized, sham‐controlled clinical trial. Journal of Maternal‐Fetal & Neonatal Medicine 2009;22(10):843‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coeytaux RR, Harper T, Chen W, Reilly A, Loh YL. Acupuncture to initiate labor (ACUMOMS 2): a randomized, sham‐controlled clinical trial. Journal of Alternative and Complementary Medicine 2007;13(8):886. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gaudernack 2006 {published data only}
- Gaudernack LC, Forbord S, Hole E. Acupuncture administered after spontaneous rupture of membranes at term significantly reduces the length of birth and use of oxytocin. A randomized controlled trial. Acta Obstetricia et Gynecologica Scandinavica 2006;85(11):1348‐53. [DOI] [PubMed] [Google Scholar]
Gaudet 2008 {published data only}
- Gaudet LM, Dyzak R, Aung SK, Smith GN. Effectiveness of acupuncture for the initiation of labour at term: a pilot randomized controlled trial. Journal of Obstetrics and Gynaecology Canada 2008;30(12):1118‐23. [DOI] [PubMed] [Google Scholar]
Gregson 2015 {published data only}
- Gregson S, Tiran D, Absalom J, Older L, Bassett P. Acupressure for inducing labour for nulliparous women with post‐dates pregnancy. Complementary Therapies in Clinical Practice 2015;21(4):257‐61. [DOI] [PubMed] [Google Scholar]
Gribel 2011 {published data only}
- Gribel GPC, Coca‐Velarde LG, Moreira RAS. Electroacupuncture for cervical ripening prior to labor induction: a randomized clinical trial. Archives of Gynecology and Obstetrics 2011;283(6):1233‐8. [DOI] [PubMed] [Google Scholar]
Harper 2006 {published data only}
- Harper TC, Coeytaux RR, Chen W, Campbell K, Kaufman JS, Moise KJ, et al. A randomized controlled trial of acupuncture for initiation of labor in nulliparous women. Journal of Maternal‐Fetal and Neonatal Medicine 2006;19(8):465‐70. [DOI] [PubMed] [Google Scholar]
- Harper TC, Coeytaux RR, Chen W, Campbell K, Kaufman JS, Thorp J, et al. A randomized controlled trial of acupuncture for initiation of labor in nulliparous women [abstract]. American Journal of Obstetrics and Gynecology 2005;193(6 Suppl):S43. [DOI] [PubMed] [Google Scholar]
Long 1994 {published data only}
- Long Z. Auricular point‐pressing therapy for induced labor in mid‐ and late pregnancy. Acupuncture Research 1994;19(1):181. [Google Scholar]
- Long ZG. 200 cases of ear acupoint press therapy for induced labor by rivanol at middle and late stage. Chinese Acupuncture and Moxibustion 1994;14(5):26. [Google Scholar]
Mackenzie 2011 {published data only}
- Mackenzie I, Xu J, Cusick C, Midwinter‐Morten H, Meacher H, Mollison J, et al. Acupuncture for pain relief during induced labour in nulliparae: a randomised controlled study. British Journal of Obstetrics and Gynaecology 2011;118(4):440‐7. [DOI] [PubMed] [Google Scholar]
- NCT01165099. Acupuncture for pain relief during induced labour for nulliparae. clinicaltrials.gov/ct2/show/record/NCT01165099 (first received 15 July 2010).
Martinez 2004 {published data only}
- Martinez AC, Rivera LN, Arangel CR. Acupuncture as an alternative technique for uterine contraction in term pregnant patients. 5th World Congress on Controversies in Obstetrics and Gynecology; 2004 June 3‐6; Las Vegas, USA. 2004.
Modlock 2010 {published data only}
- Modlock J, Nielsen BB, Uldbjerg N. Acupuncture for the induction of labour: a double‐blind randomised controlled study. British Journal of Obstetrics & Gynaecology 2010;117(10):1255‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT00245752. Can acupuncture be used as preparation for induction of labour?. clinicaltrials.gov/show/NCT00245752 (first received 26 October 2005).
Mollart 2016 {published data only}
- Mollart L, Foureur M, Skinner V. Pregnant women and health professionals views on CAM in pregnancy specifically acupressure and being involved in a randomised controlled trial. Women and Birth 2015;28 Suppl:S50. [Google Scholar]
- Mollart L, Skinner V, Foureur M. A feasibility randomised controlled trial of acupressure to assist spontaneous labour for primigravid women experiencing a post‐date pregnancy. Midwifery 2016;36:21‐7. [DOI] [PubMed] [Google Scholar]
Neri 2014 {published data only}
- Neri I, Chiesa V, Facchinetti F. Acupuncture in post‐date pregnancy: a pilot study. European Journal of Integrative Medicine 2012;4(Suppl 1):53. [DOI] [PubMed] [Google Scholar]
- Neri I, Monari F, Salvioli C, Facchinetti F. Acupuncture in post‐date pregnancy: a pilot study. Journal of Maternal‐Fetal & Neonatal Medicine 2014;27(9):874‐8. [DOI] [PubMed] [Google Scholar]
Rabl 2001 {published data only}
- Rabl M, Ahner R, Bitschnau M, Zeisler H, Husslein P. Acupuncture for cervical ripening and induction of labour at term: a randomised controlled trial. Wiener Klinische Wochenschrift 2001;113(23‐24):942‐6. [PubMed] [Google Scholar]
Romer 2000 {published data only}
- Romer A, Weigel M, Zieger W, Melchart F. Prenatal acupuncture: effects on cervical maturation and duration of labour. Geburtshilfe und Frauenheilkunde 2000;60(10):513‐8. [Google Scholar]
- Romer A, Weigel M, Zieger W, Melchert F. Changes in cervix maturity and length of birth after birth‐preparation accupuncture therapy ‐ Mannheim Rome Scheme [Veranderungen von Cervixreife und Geburtsdauer nach geburtsvorbereitender Akupunkturtherapie ‐ Mannheimer Romer‐Schema.]. Deutsche Zeitschrift fur Akupunktur 1998;41:93‐100. [Google Scholar]
Selmer‐Olsen 2007 {published data only}
- Selmer‐Olsen T, Lydersen S, Morkved S. Does acupuncture used in nulliparous women reduce time from prelabour rupture of membranes at term to active phase of labour? A randomised controlled trial. Acta Obstetricia et Gynecologica Scandinavica 2007;86(12):1447‐52. [DOI] [PubMed] [Google Scholar]
Smith 2008 {published data only}
- Smith CA, Crowther CA, Collins CT, Coyle ME. Acupuncture to induce labor: a randomized controlled trial. Obstetrics & Gynecology 2008;112(5):1067‐74. [DOI] [PubMed] [Google Scholar]
Torkzahrani 2015 {published data only}
- Torkzahrani S, Ghobadi K, Heshmat R, Shakeri N, Jalali Aria K. Effect of acupressure on cervical ripening. Iranian Red Crescent Medical Journal 2015;17(8):e28691. [DOI] [PMC free article] [PubMed] [Google Scholar]
Torkzahrani 2016 {published data only}
- Torkzahrani S, Mahmoudikohani F, Saatchi K, Sefidkar R, Banaei M. The effect of acupressure on the initiation of labor: a randomized controlled trial. Women and Birth 2016;26(139):1‐9. [DOI] [PubMed] [Google Scholar]
Tremeau 1992 {published data only}
- Tremeau ML, Fontanie‐Ravier P, Teurnier F, Demouzon J. Protocol for cervical maturation by acupuncture [Protocole de maturation cervicale par acupuncture]. Journal de Gynecologie, Obstetrique et Biologie de la Reproduction (Paris) 1992;21:375‐80. [PubMed] [Google Scholar]
References to studies excluded from this review
Aghamohammadi 2011 {published data only}
- Aghamohammadi A, Behmanesh F, Zafari M, Tofighi M. Effect of using Transcutaneous Electrical Nerve Stimulation (TENS) in acupuncture points [Hegu (Li4) and Sanyinjiao (Sp6)] on duration of the first stage of labor. Journal of Babol University of Medical Sciences 2011;13(2):19‐24. [Google Scholar]
Bo 2006 {published data only}
- Bo QX, Zhang JX. Observation on therapeutic effect of scalp acupuncture analgesic on labor. Zhongguo Zhen Jiu 2006;26(9):659‐61. [PubMed] [Google Scholar]
Dorr 1990 {published data only}
- Dorr A. The possibility of inducing labour using acupuncture. American Journal of Acupuncture 1990;18(3):286‐90. [Google Scholar]
Dunn 1989 {published data only}
- Dunn PA, Rogers D, Halford K. Transcutaneous electrical nerve stimulation at acupuncture points in the induction of uterine contractions. Obstetrics & Gynecology 1989;73(2):286‐90. [PubMed] [Google Scholar]
Kubista 1974 {published data only}
- Kubista E, Kucera H. Acupuncture as a method of preparation in obstetrics. American Journal of Chinese Medicine 1974;2(3):283‐7. [DOI] [PubMed] [Google Scholar]
Levett 2016b {published data only}
- Levett KM, Smith CA, Bensoussan A, Dahlen HG. Complementary therapies for labour and birth study: a randomised controlled trial of antenatal integrative medicine for pain management in labour. BMJ Open 2016;6(7):e010691. [DOI] [PMC free article] [PubMed] [Google Scholar]
Li 1996 {published data only}
- Li GQ. Treatment effect of electro‐magnetic stimulation on acupuncture points for expediting child delivery. Shanghai Journal of Acupuncture and Moxibustion 1996;15(4):16. [Google Scholar]
- Li XH, Ma WZ, Xu SY. The clinical observation on the effect of electroacupuncture to Sanyinjiao (SP6) and Hegu (LI4) in influencing parturients uterine contraction in the first stage. Journal of Beijing University of Traditional Chinese Medicine 1996;19(6):38. [Google Scholar]
Li 2007 {published data only}
- Li JX. Application of hydro‐acupuncture combined with Valium in middle stage labor induction. Guangxi Medical Journal 2007;29(6):927‐8. [Google Scholar]
Liu 2012 {published data only}
- Liu YL, Jin ZG. Clinical observation of the impacts and safety of electroacupuncture at Sanyinjiao (SP6) on labor. Chinese Acupuncture and Moxibustion 2012;32(5):409‐12. [PubMed] [Google Scholar]
Lyngso 2010 {published data only}
- Lyngso CE, Lorentzen IP, Lauszus F. Use of acupuncture for labour augmentation. Ugeskrift for Laeger 2010;172(4):289‐93. [PubMed] [Google Scholar]
So 1979 {published data only}
- So LK, Sung ML, Yeung KK. Induction of labour by acupuncture [abstract]. 9th World Congress of Gynecology and Obstetrics; 1979 October 26‐31; Tokyo, Japan. 1979:281.
Teimoori 2015 {published data only}
- Teimoori B, Rajabi S, Navvabi‐Rigi SD, Arbabisarjou A. Evaluation effect of shiatsu technique on labor induction in post‐term pregnancy. Global Journal of Health Science 2015;7(3):177‐83. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to ongoing studies
NCT00379327 {published data only}
- NCT00379327. Acupuncture for promotion of timely delivery. clinicaltrials.gov/show/NCT00379327 (first received 19 September 2006).
NCT01052857 {published data only}
- NCT01052857. Efficacy of acupuncture on induction of labour. clinicaltrials.gov/show/NCT01052857 (first received 11 December 2007).
NCT02392988 {published data only}
- NCT02392988. Does acupuncture therapy reduce the need for labor induction after postdate (week 41). clinicaltrials.gov/show/NCT02392988 (first received 2 March 2015).
NCT02394041 {published data only}
- NCT02394041. Randomised controlled trial of the efficacy of acupuncture versus placebo on the caesarean section rate in case of cervical dystocia in full‐term pregnancy (ACUCESAR). clinicaltrials.gov/show/NCT02394041 (first received 16 March 2015).
Additional references
Adams 2009
- Adams J, Lui C‐W, Sibbritt D, Broom A, Wardle J, Homer C, et al. Women’s use of complementary and alternative medicine during pregnancy: a critical review of the literature. Birth 2009;36(3):237‐45. [DOI] [PubMed] [Google Scholar]
Alfirevic 2006
- Alfirevic Z, Weeks A. Oral misoprostol for induction of labour. Cochrane Database of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD001338.pub2] [DOI] [PubMed] [Google Scholar]
Alfirevic 2009
- Alfirevic Z, Kelly AJ, Dowswell T. Intravenous oxytocin alone for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews 2009, Issue 4. [DOI: 10.1002/14651858.CD003246.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bell 1972
- Bell C. Autonomic nervous control of reproduction: circulatory and other factors. Pharmacological Reviews 1972;24:657‐763. [PubMed] [Google Scholar]
Bimbashi 2012
- Bimbashi A, Duley L, Ndoni E, Dokle A. Amniotomy plus intravenous oxytocin for induction of labour. Cochrane Database of Systematic Reviews 2012, Issue 4. [DOI: 10.1002/14651858.CD009821] [DOI] [PMC free article] [PubMed] [Google Scholar]
Boulvain 2005
- Boulvain M, Stan C, Irion O. Membrane sweeping for induction of labour. Cochrane Database of Systematic Reviews 2005, Issue 1. [DOI: 10.1002/14651858.CD000451.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Boulvain 2008
- Boulvain M, Kelly A, Irion O. Intracervical prostaglandins for induction of labour. Cochrane Database of Systematic Reviews 2008, Issue 1. [DOI: 10.1002/14651858.CD006971] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bricker 2000
- Bricker L, Luckas M. Amniotomy alone for induction of labour. Cochrane Database of Systematic Reviews 2000, Issue 4. [DOI: 10.1002/14651858.CD002862] [DOI] [PMC free article] [PubMed] [Google Scholar]
Curtis 1987
- Curtis P, Evans S, Resnick J. Uterine hyperstimulation. The need for standard terminology. Journal of Reproductive Medicine 1987;32:91‐5. [PubMed] [Google Scholar]
De Miranda 2006
- Miranda E, Bom JG, Bonsel GJ, Bleker OP, Rosendaal FR. Membrane sweeping and prevention of post‐term pregnancy in low‐risk pregnancies: a randomised controlled trial. British Journal of Obstetrics and Gynaecology 2006;113(4):402–8. [DOI] [PubMed] [Google Scholar]
French 2001
- French L. Oral prostaglandin E2 for induction of labour. Cochrane Database of Systematic Reviews 2001, Issue 2. [DOI: 10.1002/14651858.CD003098] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ghosh 2016
- Ghosh A, Lattey KR, Kelly AJ. Nitric oxide donors for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews 2016, Issue 12. [DOI: 10.1002/14651858.CD006901.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hapangama 2009
- Hapangama D, Neilson JP. Mifepristone for induction of labour. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD002865.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Hofmeyr 2009
- Hofmeyr GJ, Alfirevic Z, Kelly AJ, Kavanagh J, Thomas J, Neilson JP, et al. Methods for cervical ripening and labour induction in late pregnancy: generic protocol. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD002074.pub2] [DOI] [Google Scholar]
Hofmeyr 2010
- Hofmeyr GJ, Gülmezoglu AM, Pileggi C. Vaginal misoprostol for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews 2010, Issue 10. [DOI: 10.1002/14651858.CD000941.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Howarth 2001
- Howarth GR, Botha DJ. Amniotomy plus intravenous oxytocin for induction of labour. Cochrane Database of Systematic Reviews 2001, Issue 3. [DOI: 10.1002/14651858.CD003250] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hutton 2001
- Hutton E, Mozurkewich E. Extra‐amniotic prostaglandin for induction of labour. Cochrane Database of Systematic Reviews 2001, Issue 2. [DOI: 10.1002/14651858.CD003092] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jozwiak 2012
- Jozwiak M, Bloemenkamp KWM, Kelly AJ, Mol BWJ, Irion O, Boulvain M. Mechanical methods for induction of labour. Cochrane Database of Systematic Reviews 2012, Issue 3. [DOI: 10.1002/14651858.CD001233.pub2] [DOI] [PubMed] [Google Scholar]
Kavanagh 2001
- Kavanagh J, Kelly AJ, Thomas J. Sexual intercourse for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews 2001, Issue 2. [DOI: 10.1002/14651858.CD003093] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kavanagh 2005
- Kavanagh J, Kelly AJ, Thomas J. Breast stimulation for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews 2005, Issue 3. [DOI: 10.1002/14651858.CD003392.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kavanagh 2006a
- Kavanagh J, Kelly AJ, Thomas J. Hyaluronidase for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD003097.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kavanagh 2006b
- Kavanagh J, Kelly AJ, Thomas J. Corticosteroids for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD003100.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kelly 2001b
- Kelly AJ, Kavanagh J, Thomas J. Relaxin for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews 2001, Issue 2. [DOI: 10.1002/14651858.CD003103] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kelly 2009
- Kelly AJ, Malik S, Smith L, Kavanagh J, Thomas J. Vaginal prostaglandin (PGE2 and PGF2a) for induction of labour at term. Cochrane Database of Systematic Reviews 2009, Issue 4. [DOI: 10.1002/14651858.CD003101.pub2] [DOI] [PubMed] [Google Scholar]
Kelly 2013
- Kelly AJ, Kavanagh J, Thomas J. Castor oil, bath and/or enema for cervical priming and induction of labour. Cochrane Database of Systematic Reviews 2013, Issue 7. [DOI: 10.1002/14651858.CD003099.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Khireddine 2013
- Khireddine I, Ray C, Dupont C, Rudigoz RC, Bouvier‐Colle MH, Deneux‐Tharaux C. Induction of labor and risk of postpartum hemorrhage in low risk parturients. PLOS One 2013;8(1):e54858. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kubista 1975
- Kubista E, Kucera H, Muller‐Tyl E. Initiating contractions of the gravid uterus through electro‐acupuncture. American Journal of Chinese Medicine 1975;3(4):343‐6. [DOI] [PubMed] [Google Scholar]
Levett 2016a
- Levett K, Smith CA, Bensoussan A, Dahlen H. The complementary therapies for labour and birth study: making sense of labour and birth ‐ experiences of women, partners and midwives of a complementary medicine antenatal education course. Midwifery 2016;40:124‐31. [DOI] [PubMed] [Google Scholar]
Liao 1979
- Liao Y, Seto K, Saito H, Fujita M, Kawakami M. Effect of acupuncture on adrenocortical hormone production:1. Variation in the ability for adrenocortical hormone production in relation to the duration of acupuncture stimulation. American Journal of Chinese Medicine 1979;7:362‐71. [DOI] [PubMed] [Google Scholar]
Lim 2009
- Lim CE, Wilkinson JM, Wong WS, Cheng NC. Effect of acupuncture on induction of labor. Journal of Alternative and Complementary Medicine 2009;15(11):1209‐14. [DOI] [PubMed] [Google Scholar]
Luckas 2000
- Luckas M, Bricker L. Intravenous prostaglandin for induction of labour. Cochrane Database of Systematic Reviews 2000, Issue 4. [DOI: 10.1002/14651858.CD002864] [DOI] [PMC free article] [PubMed] [Google Scholar]
Makvandi 2016
- Makvandi S, Mirzaiinajmabadi K, Sadeghi R, Mahdavian M, Karimi L. Meta‐analysis of the effect of acupressure on duration of labor and mode of delivery. International Journal of Gynecology & Obstetrics 2016;135(1):5‐10. [DOI] [PubMed] [Google Scholar]
Mollart 2015
- Mollart LJ, Adam J, Foureur M. Impact of acupressure on onset of labour and labour duration: a systematic review. Women and Birth 2015;28(3):199‐206. [DOI] [PubMed] [Google Scholar]
Mozurkewich 2011
- Mozurkewich EL, Chilimigras JL, Berman DR, Perni UC, Romero VC, King VJ, et al. Methods of induction of labour: a systematic review. BMC Pregnancy and Childbirth 2011;11:84. [DOI] [PMC free article] [PubMed] [Google Scholar]
Muzonzini 2004
- Muzonzini G, Hofmeyr GJ. Buccal or sublingual misoprostol for cervical ripening and induction of labour. Cochrane Database of Systematic Reviews 2004, Issue 4. [DOI: 10.1002/14651858.CD004221.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Smith 2003
- Smith CA. Homoeopathy for induction of labour. Cochrane Database of Systematic Reviews 2003, Issue 4. [DOI: 10.1002/14651858.CD003399] [DOI] [PubMed] [Google Scholar]
Smith 2004
- Smith CA, Crowther CA. Acupuncture for induction of labour. Cochrane Database of Systematic Reviews 2004, Issue 1. [DOI: 10.1002/14651858.CD002962.pub2] [DOI] [PubMed] [Google Scholar]
Stewart 2014
- Stewart D, Pallivalappila AR, Shetty A, Pande B, McLay JS. Healthcare professional views and experiences of complementary and alternative therapies in obstetric practice in North East Scotland: a prospective questionnaire survey. British Journal of Obstetrics and Gynaecology 2014;121(8):1015‐9. [DOI] [PubMed] [Google Scholar]
Streitberger 1998
- Streitberger K, Kleinhenz J. Introducing a placebo needle into acupuncture research. Lancet 1998;352:364‐5. [DOI] [PubMed] [Google Scholar]
Tempfeer 1998
- Tempfeer C, Zeisler H, Heinzl H, Hefler L, Husslein P, Kainz CH. Influence of acupuncture on maternal serum levels of interleukin‐8, prostaglandin F2 alpha, and beta‐endorphin: a matched pair study. Obstetrics & Gynecology 1998;92(2):245‐8. [DOI] [PubMed] [Google Scholar]
Tenore 2003
- Tenore JL. Methods for cervical ripening and induction of labor. American Family Physician 2003;67(10):2123‐8. [PubMed] [Google Scholar]
Theobald 1973
- Theobald GW. The Electrical Induction of Labour. New York: Appleton‐Century‐Crofts, 1973. [Google Scholar]
Thomas 2001
- Thomas J, Kelly AJ, Kavanagh J. Oestrogens alone or with amniotomy for cervical ripening or induction of labour. Cochrane Database of Systematic Reviews 2001, Issue 4. [DOI: 10.1002/14651858.CD003393] [DOI] [PMC free article] [PubMed] [Google Scholar]
Tsuei 1974
- Tsuei JT, Lai Y. Induction of labour by acupuncture and electrical stimulation. Obstetrics & Gynecology 1974;43(3):337‐42. [PubMed] [Google Scholar]
Tsuei 1977
- Tsuei JT, Lai Y, Sharma SD. The influence of acupuncture stimulation during pregnancy: the induction and inhibition of labour. Obstetrics & Gynecology 1977;50:479‐88. [PubMed] [Google Scholar]
Yip 1976
- Yip S, Pang J, Sung M. Induction of labour by acupuncture electro stimulation. American Journal of Chinese Medicine 1976;4(3):257‐65. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Smith 2004a
- Smith CA, Crowther. Acupuncture for induction of labour. Cochrane Database of Systematic Reviews 2004, Issue 1. [DOI: 10.1002/14651858.CD002962.pub2] [DOI] [PubMed] [Google Scholar]
Smith 2013
- Smith CA, Crowther CA, Grant SJ. Acupuncture for induction of labour. Cochrane Database of Systematic Reviews 2013, Issue 8. [DOI: 10.1002/14651858.CD002962.pub3] [DOI] [PubMed] [Google Scholar]