

Abstract
Introduction:
Teen dating violence is a serious public health problem with few effective prevention strategies. This study examines whether the Dating Matters comprehensive prevention model, compared with a standard of care intervention, prevented negative relationship behaviors and promoted positive relationship behaviors.
Study design:
This longitudinal, cluster-RCT compared the effectiveness of Dating Matters with standard of care across middle school. Standard of care was an evidence-based teen dating violence prevention curriculum (Safe Dates) implemented in eighth grade.
Setting/participants:
Forty-six middle schools in high-risk urban neighborhoods in four U.S. cities were randomized. Schools lost to follow-up were replaced with new schools, which were independently randomized (71% school retention). Students were surveyed in fall and spring of sixth, seventh, and eighth grades (2012–2016). The analysis sample includes students from schools implementing Dating Matters or standard of care for >2 years who started sixth grade in the fall of 2012 or 2013 and had dated (N=2,349 students, mean age 12 years, 49% female, and 55% black, non-Hispanic, 28% Hispanic, 17% other).
Intervention:
Dating Matters is a comprehensive, multicomponent prevention model including classroom-delivered programs for sixth to eighth graders, training for parents of sixth to eighth graders, educator training, a youth communications program, and local health department activities to assess capacity and track teen dating violence–related policy and data.
Main outcome measures:
Self-reported teen dating violence perpetration and victimization, use of negative conflict resolution strategies, and positive relationship skills were examined as outcomes. Imputation and analyses were conducted in 2017.
Results:
Latent panel models demonstrated significant program effects for three of four outcomes; Dating Matters students reported 8.43% lower teen dating violence perpetration, 9.78% lower teen dating violence victimization, and 5.52% lower use of negative conflict resolution strategies, on average across time points and cohorts, than standard of care students. There were no significant effects on positive relationship behaviors.
Conclusions:
Dating Matters demonstrates comparative effectiveness, through middle school, for reducing unhealthy relationship behaviors, such as teen dating violence and use of negative conflict resolution strategies, relative to the standard of care intervention.
Trial registration:
This study is registered at www.clinicaltrials.gov .
INTRODUCTION
Teen dating violence (TDV) is defined as physical, sexual, or psychological/emotional violence, including stalking, occurring within a teen dating relationship.1 TDV is a significant public health problem with substantial, long-term consequences, including low academic achievement, depression, suicidal ideation, substance use disorders, and adult intimate partner violence victimization.2–5 National estimates indicate that 10% of U.S. high-school students that dated in the last year report physical violence victimization and 10% report sexual violence victimization from a dating partner.6 Attention to the primary prevention of TDV is critical, given the magnitude of the problem and its public health burden.7 However, three notable gaps exist in understanding how to prevent TDV.
First, most evidence-based TDV prevention programs were developed for mid- to late-adolescents8–10, when TDV is most prevalent.6,11 However, intervening earlier in adolescence may prevent initiation of violent behaviors as youth embark on romantic relationships. Second, existing programs tend to have a single component, often targeting youth in school with didactic curricula.12 In the broader field of violence prevention, comprehensive, multicomponent strategies addressing risk and protective factors across the levels of the social ecology (i.e., individual, relationship, community, and society)13 are more effective at preventing violence in the long term than single-component approaches targeting one level of the social ecology.14,15 Third, few TDV prevention programs have been tested in high-crime, high-poverty urban environments where youth often face multiple risks (e.g., violence exposure),16–19 which may increase risk for TDV.20,21
To address these gaps, the Centers for Disease Control and Prevention (CDC) developed Dating Matters: Strategies to Promote Healthy Teen Relationships (DM), a comprehensive TDV prevention model targeting middle school youth in high-risk urban communities with strategies at multiple levels of the social ecology to promote healthy relationships and prevent TDV.22–24 The current study presents results of a comparative effectiveness, cluster-RCT of DM on primary outcomes (TDV and other relationship behaviors) among two cohorts of students that had the opportunity of full exposure to DM during middle school (sixth to eighth grade; Appendix, available online). It is hypothesized that students exposed to DM would report less TDV perpetration and victimization, less use of negative conflict resolution strategies, and more engagement in healthy relationship behaviors over time than students exposed to the standard of care (SC) condition, the Safe Dates evidence-based TDV prevention curriculum (eighth grade). Although outcomes of interest are at the student level, participants were enrolled through a cluster-randomized design, which reflects the comprehensive, schoolwide nature of DM.
METHODS
Study Sample
CDC conducted a multisite, cluster-randomized (school) longitudinal design to evaluate the comparative effectiveness of the DM comprehensive prevention model relative to an evidence-based, SC intervention to prevent TDV. CDC funded local health departments (LHDs) in four urban U.S. cities to implement the two prevention approaches. LHDs in Alameda County, California (Oakland); Baltimore, Maryland; Broward County, Florida (Ft. Lauderdale); and Chicago, Illinois were awarded funding for implementation. The four LHDs selected ten to 12 neighborhood middle schools in high-risk urban communities; neighborhoods were defined as high-risk if they had above average crime and above average economic disadvantage in comparison to the rest of the city or the state. The LHDs identified 46 schools that were randomly assigned within site using a computer-generated random numbers approach (Figure 1, Appendix, available online) to implement DM or SC during the trial (2012–2016). Schools implemented DM or SC for four consecutive school years (the 2012–2013 through the 2015–2016 school year). A power analysis using Optimal Design by Raudenbush et al.25 based on a three-level cluster-randomized trial (the three levels included site [city], schools, and cohorts) indicated that <40 schools would afford 90% power to detect differences as small as 8 percentage points. Because some schools dropped out, replacement schools were recruited and independently randomized to condition during the first 3 years of the study to ensure sufficient power (Appendix Text and Appendix Figure 1, available online).
Figure 1. CONSORT diagram for study enrollment, allocation, and data collection and analysis.
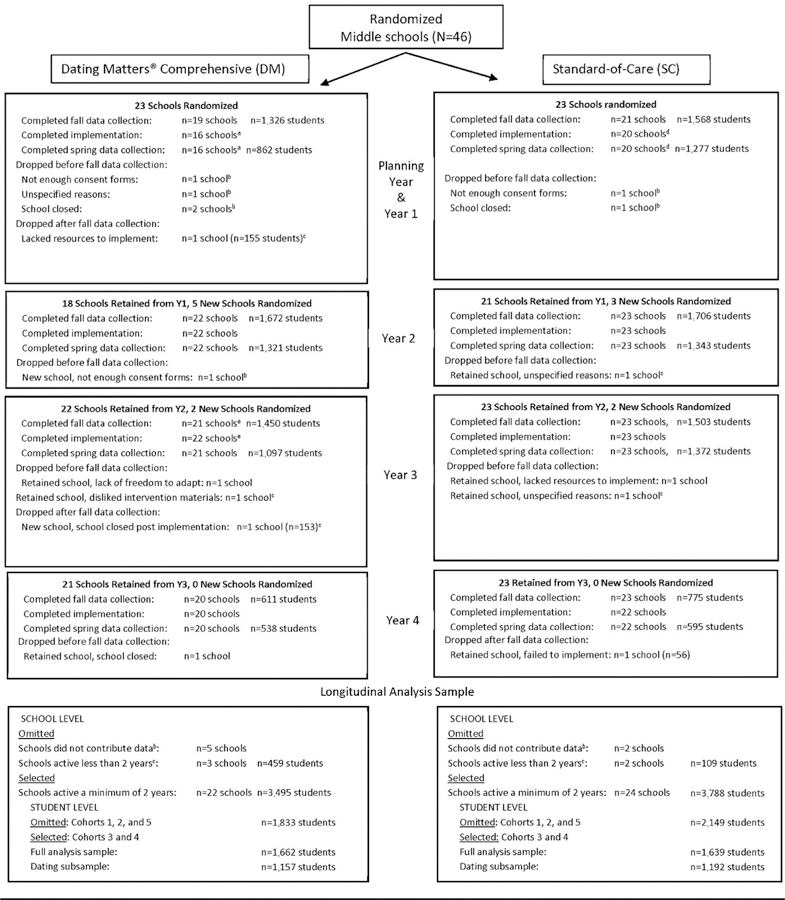
Note: Implementation was whole-school, so more students were exposed to the intervention than were included in the trial. Therefore, only school numbers are included for completing implementation, although student numbers are provided for participation in data collection. aTwo schools lacked resources to implement in Y1 and did not complete spring data collection but stayed in the study and were active Y2 (n=81 and 44). bSchools did not contribute data; these schools dropped before fall data collection and therefore student numbers for participation cannot be estimated. 0Schools contributed some data but were active <2 years and therefore were not included in analyses. dOne school that lacked resources to implement in Y1 and did not complete spring data collection stayed in the study and was active Y2 (n=95). eOne retained school did not participate in fall data collection but implemented and participated in spring data collection.
The study used active parental consent, where guardians returned forms indicating whether they allowed their child to complete surveys. All sites struggled to get consent forms returned, but this was not atypical for the high-risk urban schools in the study. Many schools reported having great difficulty getting any forms back from parents, including ones that directly benefited the student and family, such as forms to qualify for free- or reduced-price lunch. Because of difficulty attaining even the minimum return rate (60%), one site switched from active to passive consenting procedures in the second year.26 Across sites, the consent form return rate was 74%, with 78% of returned forms indicating permission to participate, resulting in an overall positive consent rate of 58%. In schools with four classrooms per grade or less, all students were recruited. In one site with exceptionally large schools, students were recruited from four randomly selected classrooms per grade per school. However, these schools still administered the assigned intervention to all students, even though not all students participated in the surveys.
To be included in analysis, schools had to have implemented either DM (n=22) or SC (n=24) for >2 full academic years (Appendix, available online). The decision to include schools with 2 full years of participation in the trial was based on the fact that schools implementing <2 years would have implemented less than half of the 3-year middle school span covered by the DM components and that students from the schools would have less than half of the survey data collection opportunities across the 3 years of middle school. The analytic sample included students in two cohorts in these schools who started sixth grade in either 2012 or 2013 (students with an opportunity for full exposure to DM in DM schools during the period of implementation; Appendix, available online), reported having dated before or during middle school, and therefore answered questions on the dating outcomes examined in this analysis (N=2,349; n=1,157 for DM; n=1,192 for SC). In this sample, 48% of the participants were female; 55%, black, non-Hispanic; and 28%, Hispanic of any race; full sample demographics and average outcome scores are presented in Appendix Table 1 (available online). Differences by race were seen for some cohorts (Appendix Table 2, available online).
Measures
The DM comprehensive prevention model22,23 (Appendix Text, Appendix Table 3, available online) was developed to create a comprehensive approach to TDV prevention with components at each level of the social ecology.13 In other areas of violence prevention, evidence shows that comprehensive approaches are more effective than single-component approaches; therefore, the intent with this model was to create a “surround sound” effect, promoting healthy relationship behaviors and preventing unhealthy ones at the individual, family, neighborhood, and community levels of the social ecology.14,15 DM was also designed to enhance expectations for and teach skills to have respectful and healthy relationships with others, with the goal of addressing a constellation of risk and protective factors that would prevent not only TDV but a host of other interpersonal and behavioral risk outcomes. The DM comprehensive prevention model includes classroom-delivered programs for sixth to eighth graders, training for parents of sixth to eighth graders, training for teachers/school personnel, a youth communications program, and activities at the LHD to assess and build TDV prevention capacity and track TDV-related policy and data. Students in sixth and seventh grade received CDC-developed DM youth programs. Eighth graders received Safe Dates, an evidence-based TDV prevention program.27 All three student programs teach students about healthy relationships and assist youth in practicing healthy relationship skills. The parent programs included an adapted version of Parents Matter!28 (sixth grade), DM for Parents (seventh grade; CDC-developed), and Families for Safe Dates29 (eighth grade). Each parenting program taught participants skills for positive parenting and communicating effectively with their children about healthy relationships. All teachers/staff in DM schools were asked to complete a CDC-developed online educator training that provided information and resources regarding TDV and motivated participants to implement prevention measures in their schools. The youth communications program (i2i: What R U Looking 4) reinforced messaging about healthy relationships using near-peer brand ambassadors with community activities, printed materials, and digital resources. Finally, LHDs implementing DM were assisted in assessing and building capacity for comprehensive TDV prevention and tracking local policy and indicator data related to TDV prevention; these activities were conducted at the community-level and may have impacted students in both DM and SC schools. Schools were required to do whole-school implementation, so that all students in DM schools were exposed to the grade-appropriate components. SC schools implemented only Safe Dates in eighth grade. All eighth graders in SC schools were to be exposed to the Safe Dates curriculum.
Procedures and materials were approved by multiple IRBs and the Office of Management and Budget (OMB #0920–0941). Before program implementation, students completed a paper and pencil baseline survey in the school setting (e.g., classroom or other designated space). Following program implementation and >4 months after the baseline survey, students completed a follow-up survey in the same manner. Students were surveyed in the fall and spring of middle school during four consecutive years (2012–2016; Appendix Figure 1, available online).
Surveys assessed demographic characteristics (e.g., family composition), historical risk factors (e.g., exposure to family violence), and multiple primary and secondary outcomes (e.g., TDV, negative and positive relationship behaviors, substance use, bullying). Appendix Tables 4–8 (available online) include outcome measures, items, means, and reliability coefficients from the current study at each time point.
Participants were asked if they had ever dated (baseline) or dated in the past 4 months (follow-up). Participants who had dated in that timeframe were asked to respond to 62 questions about TDV (31 each on victimization and perpetration) including 50 items from the Conflict in Adolescent Dating Relationships Inventory (CADRI)30 assessing five TDV types: physical abuse, threatening behaviors, sexual abuse, relational abuse, and emotional/verbal abuse, and 12 items from the Safe Dates scales assessing severe physical abuse and threatening with a weapon.31 The CADRI was chosen as the main measure for TDV because it more robustly captures sexual aggression in adolescent relationships than other measures, and the 12 items from the Safe Dates scales were added to capture more severe physically abusive behaviors than are measured in the CADRI. These items were combined into three indicators, coded separately for victimization and perpetration: (1) verbal/physical/threat of violence, (2) relational/sexual violence, and (3) severe behaviors (e.g., choking, weapon use). These indicators were created using facet-representative parceling, which relies on grouping items into substantive distinct but interrelated subscales of the higher-order victimization (TDV-V) and perpetration (TDV-P) constructs (Appendix, available online). Cronbach’s α coefficients for TDV-P and TDV-V ranged from 0.89 to 0.93 across time.
Use of negative conflict resolution strategies with a dating partner or friend in the prior 4 months was assessed by three subscales (Compliance, Conflict Engagement, Withdrawal) with four items each from the Conflict Resolution Style Inventory.32 Items reference the use of negative behaviors in a conflict situation with a partner in response to the stem: How often do YOU use these styles? (e.g., exploding and getting out of control). Reliability ranged from 0.76 to 0.85.
Four items adapted from the Supporting Healthy Marriage Study33 were used to assess use of positive relationship skills; these items included behaviors such as being honest and working out differences in a dating relationship. Items were selected and adapted to reflect behaviors appropriate to pre-teen and teen dating relationships rather than adult marriages. The baseline version did not specify a recall period even though follow-up referenced the past 4 months. Reliability ranged from 0.81 to 0.88.
Statistical Analysis
Data analysis was conducted in 2017. During data preparation (Appendix, available online), multiple imputation of missing data was employed using PcAux.34 The imputation models drew from all available student responses and school-level information. Before modeling, the indicators were adjusted for covariate effects (residual scoring)35,36 and outliers (donor method; Appendix, available online).37 All outcome indicators reflect percentage of maximum scaling (POMS; Appendix Text, Appendix Table 8, available online), which ranges from 0 (lowest possible score) to 100 (highest possible score).38
Because students were nested within schools (cluster) and schools were nested within the four study sites (strata), indicators of school membership were included as covariates to adjust for design effects. All models also controlled for: timeframe reference for behaviors (lifetime versus 4 months), witnessing violence in the community and home, relative age within grade, race and ethnicity, guardian status, time-varying dating status, lag in assessment timing, and for the use of negative conflict resolution strategies only, the type of relationship partner (friend versus dating partner).
Student-level program effects on each outcome were evaluated separately using multiple group structural equation models on 100 imputed datasets using Mplus, version 7.4.39 Eight groups were represented by the intersections of sex (male and female), cohort (Cohorts 3 and 4), and treatment condition (DM and SC). Each model assessed six time points: fall and spring of sixth, seventh, and eighth grades. Measurement invariance, a modeling restriction underlying the assumption that outcome measures have the same meaning for all groups and time points, was evaluated and then imposed (Appendix Table 9, available online).
Equivalent means were identified by iteratively imposing equality constraints, evaluated using nested chi-squared difference tests.40 To evaluate the choice of constraints, the magnitude of the freely estimated means was assessed to identify characteristic patterns consistent with the hypothesis of protective program effects. Because the equality constraints are placed across the full set of 48 means (six waves by eight groups), these models evaluate the overall preponderance of evidence, rather than each time point for each group independently. The results of these models are presented in Figures 2–4 and Appendix Figure 6 (available online). These models present the constrained POMS means for all eight groups (y-axis) evaluated in each model at the six middle school time points (x-axis). Because non–significantly different means were constrained to be equal, any difference in means depicted in the figures represent statistically significant differences between groups. Comparisons are separated into four graphs to visually distinguish between groups.
Figure 2. Constrained means across time by sex and cohort: teen dating violence perpetration.
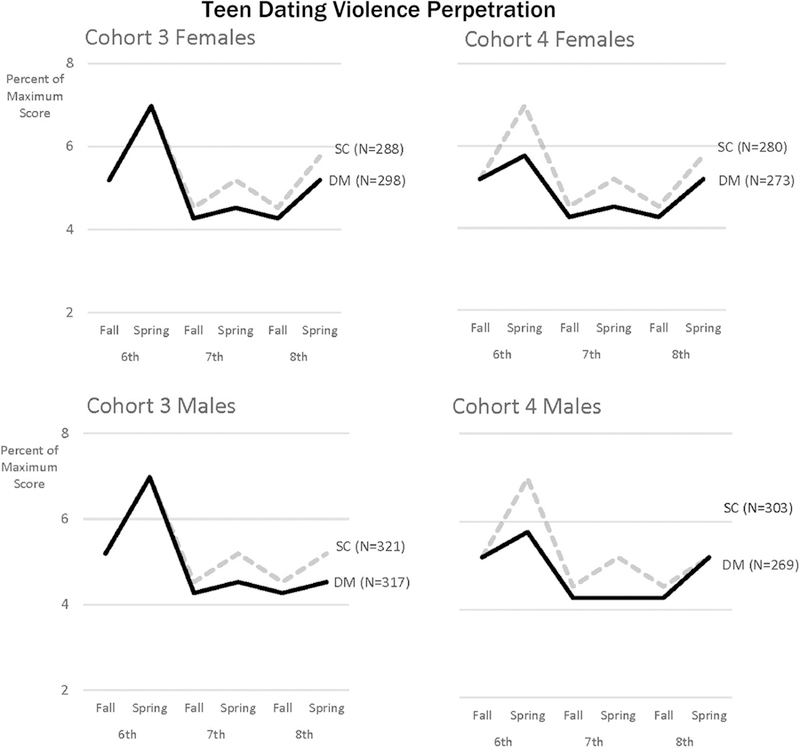
Note: Sample size (n) for each condition within each group are reported next to the condition label of the respective line in each figure. POMS refers to the maximum possible score, given the number of items and response categories in a scale, rather than the maximum observed score. Non-overlapping lines represent significant group differences. SEs, CIs, and statistical significance for each estimated mean value is reported in Appendix Table 11 (available online).
DM, Dating Matters condition; POMS, percent of maximum score; SC, standard of care condition.
Figure 4. Constrained means across time by sex and cohort: negative conflict resolution strategies.
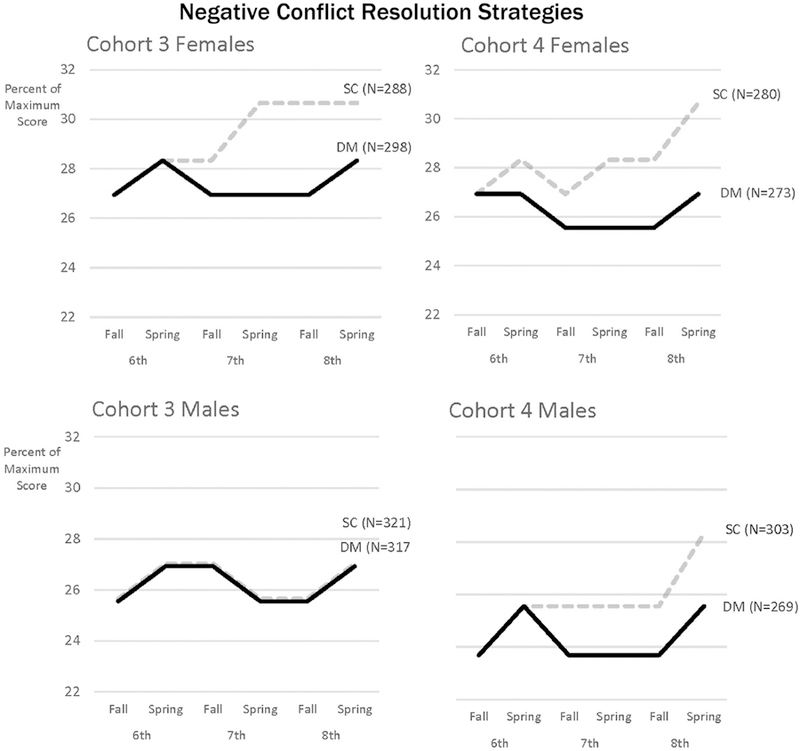
Note: Sample size (n) for each condition within each group are reported next to the condition label of the respective line in each figure. POMS refers to the maximum possible score given the number of items and response categories in a scale, rather than the maximum observed score. Non-overlapping lines represent significant group differences. SEs, CIs, and statistical significance for each estimated mean value is reported in Appendix Table 11 (available online).
DM, Dating Matters condition; POMS, percent of maximum score; SC, standard of care condition.
To capture the magnitude of these effects, post hoc Wald tests were used to evaluate the difference between means estimated for DM and SC, operationalized as RR. The average and range of DM/SC differences are presented in terms of RR. Program effects presented as percentage risk reduction are provided in Appendix Figures 2–5 (available online). Additionally, effect sizes (Cohen’s d) were calculated and are presented in Appendix Table 12 (available online). Because TDV behaviors are generally rare in middle school, even small RR reductions were considered clinically meaningful.
RESULTS
All outcome variables had baseline equivalence within each sex/cohort group (Appendix Table 10, available online). Five distinct mean constraints described all 48 means without significantly degrading the fit of the freely estimated model (Figure 2). Means were low (mean, 4.27–6.98), indicating TDV-P self-reports were relatively infrequent, but not so rare that it lacked sufficient variability to be examined as an outcome. DM students reported lower TDV-P than SC students at most time points and across groups. TDV-P differences between DM and SC students averaged 0.46 POMS (range, 0.00–1.21) and estimates of RR reduction ranged from 5.63% (CI=2.36, 8.90) to 17.68% (CI=12.80, 22.55; Appendix Figure 2, available online), averaging 8.43% (Appendix Figure 5, available online). In all groups, DM students had significantly lower TDV-P scores than SC students by the final time point, except that scores for DM and SC male students in Cohort 4 were not different at spring of eighth grade, although differences at other time points supported protective program effects. Effect sizes (Cohen’s d), which ranged from 0 to –0.03 (mean= −0.01), are presented in Appendix Table 12 (available online).
Five distinct mean constraints captured the 48 mean scores of victimization (mean, 5.02–7.79; Figure 3). Protective program effects emerged at all time points for all groups. TDV-V differences between DM and SC students averaged 0.61 POMS (range, 0.34–0.89) with risk reduction estimates ranging from 6.32% (CI=2.86, 9.77) to 15.08% (CI=11.31, 18.85; Appendix Figure 3, available online) with an average of 9.78% (Appendix Figure 5, available online). In all groups, DM students had significantly lower TDV-V means than SC students by spring of eighth grade. Effect sizes (Cohen’s d), which ranged from −0.01 to −0.02 (mean= −0.01), are presented in Appendix Table 12 (available online).
Figure 3. Constrained means across time by sex and cohort: teen dating violence victimization.
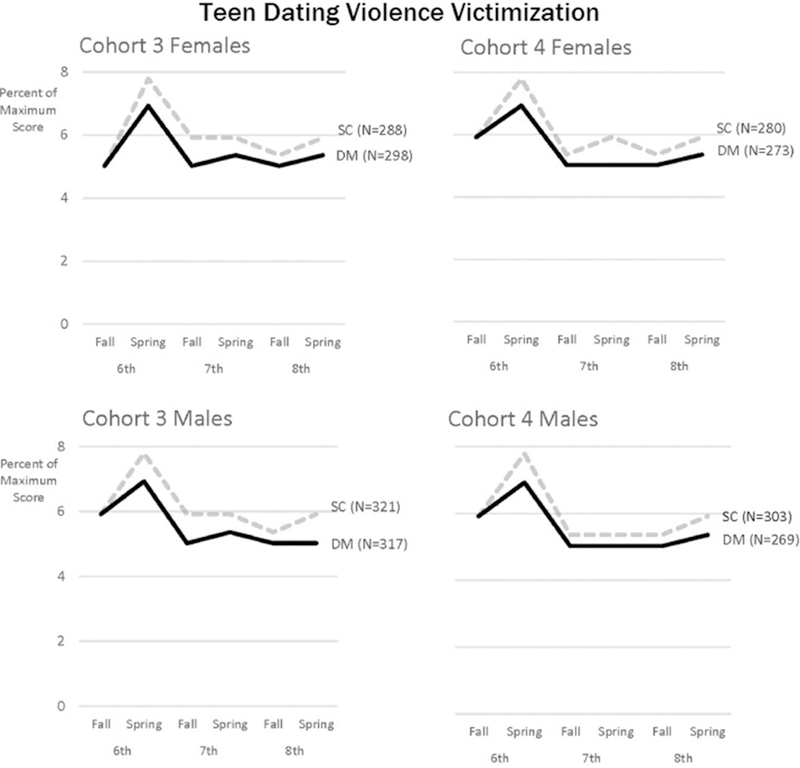
Note: Sample size (n) for each condition within each group are reported next to the condition label of the respective line in each figure. POMS refers to the maximum possible score given the number of items and response categories in a scale, rather than the maximum observed score. Non-overlapping lines represent significant group differences. SEs, CIs, and statistical significance for each estimated mean value is reported in Appendix Table 11 (available online).
DM, Dating Matters condition; POMS, percent of maximum score; SC, standard of care condition.
Five distinct mean constraints well represent the 48 means (mean, 23.68–30.66; Figure 4) for negative conflict resolution strategies. DM students reported lower use of these negative strategies than SC students at most time points and across most groups. Mean differences between DM and SC students on negative conflict resolution strategies ranged from 0.00 to 3.72. The average difference between DM and SC was 1.58 POMS. Estimates of risk reduction ranged from 4.92% (CI=2.08, 7.76) to 12.14% (CI=8.28, 16.00; Appendix Figure 4, available online), with an average of 5.52% (Appendix Figure 5, available online). In all groups except Cohort 3 males, DM students had lower negative conflict resolution strategy scores than SC students by spring of eighth grade. Effect sizes (Cohen’s d), which ranged from 0.00 to −0.01 (mean= −0.01), are presented in Appendix Table 12 (available online).
A single constraint described all 48 means; students’ mean positive relationship skills did not differ by condition or over time for any group (Appendix Figures 5 and 6, available online).
DISCUSSION
Findings from this cluster-RCT suggest that the DM comprehensive prevention model is more effective at reducing TDV and use of negative conflict resolution styles in early adolescence than the SC intervention, the evidence-based Safe Dates program. Results identified statistically significant protective program effects throughout middle school on three of four primary outcomes: TDV-P, TDV-V, and use of negative conflict resolution styles. As hypothesized, findings suggest that a multicomponent, multi-year comprehensive prevention model is more effective for reducing negative dating behaviors than a school-based curriculum implemented in a single year.
All four groups (cohort by sex) demonstrate consistent intervention effects on TDV-V across middle school. The same pattern was true for TDV-P, except that male students in Cohort 4 no longer showed effects on TDV-P by the spring of eighth grade. Both conditions received the same evidence-based curriculum in eighth grade, potentially contributing to reduced group differences at that point; however, this pattern was not seen in other groups. Significant RR reductions in TDV-P and TDV-V for DM students, compared with SC students, ranged from 6% to 18%. These results are particularly notable, given that DM was compared with an evidence-based TDV intervention and in a young sample with low base rates of TDV-P and -V.
Similarly, significant program effects on use of negative conflict resolution strategies were found for both cohorts of female students and one cohort of male students. Scores for DM students remained relatively stable across middle school for most cohorts, whereas scores for SC students generally increased over time. The significant RR reductions in negative conflict resolution for DM students compared with SC students ranged from 5% to 12%. No effects were seen for Cohort 3 males on this outcome. Analysis of additional waves of data may elucidate why this cohort of males did not demonstrate the same program effects found for the other groups. Despite the lack of findings for Cohort 3 males, overall findings suggest a protective effect of DM on the use of these negative relationship behaviors.
No significant effects were found for use of positive relationship skills. Students reported high use of positive relationship skills, and the construct was measured using only four items. Thus, detecting change may have been difficult because of a ceiling effect or a lack of variability. Observational measures of relationship skills require substantial resources but are more sensitive to change and might have provided more of an opportunity to see program effects.41 Lack of an effective self-report measure of positive relationship behaviors remains a research gap42 and hinders researchers’ ability to measure intervention effects in promoting positive, respectful relationship behaviors.
This study has several important strengths. First, the comparative effectiveness design was a practical choice to assess whether DM was more effective than an evidence-based alternative already available to communities. Second, notwithstanding the resources required and multiple challenges of conducting a multisite, cluster-randomized trial, especially in understudied and under-resourced communities, the trial design was rigorous, sufficiently powered, and implemented with integrity. Finally, the intervention was implemented in middle school to try to accomplish the primary prevention of TDV; however, this presents the issue of low base rates of TDV behaviors, making it more challenging to measure change. Despite low base rates for TDV in this early developmental period, analyses were able to detect small but significant positive program effects.
Limitations
Findings should be interpreted in the context of several limitations. First, conducting a cluster-randomized trial in high-risk urban communities posed several challenges including the following: variability in site characteristics, intervention implementation, and evaluation protocols; challenges in consent form return; and school retention.26 Second, these intent-to-treat analyses do not account for variations in fidelity or exposure to the intervention and may obscure larger-magnitude effects when fidelity or exposure was greater. Third, this study relied on self-report of TDV and relationship behaviors and cannot be sure if reported behaviors accurately reflect actual behavior. Fourth, although this sample consisted of primarily black, non-Hispanic, and Hispanic (any race) students, examining race/ethnicity as an additional group variable is beyond the scope of this initial evaluation, but this is a future direction for research. Finally, DM was evaluated in high-risk urban communities to expand the evidence base for these populations. However, given the low positive consent rate (58%), one cannot assume that this sample is generalizable to this population, nor is it yet known whether these findings will generalize to other types of communities.
CONCLUSIONS
Results from this study are exciting, particularly given the use of a comparative effectiveness approach and low base rates of TDV in middle school. A cost analysis of the DM comprehensive approach is underway and will help decision makers weigh the benefits of DM, given its multiple components and resource burden. Studies examining DM intervention effect on secondary outcomes, such as bullying and substance use, are also in progress, and may speak further to the potential benefits of DM. Analyses evaluating the impact of dosage and fidelity on treatment effects among the DM school students are also currently underway and will inform how exposure to and delivery of the student programs affected outcomes. Additionally, further research is needed to examine whether these effects persist over time, perhaps leading to prevention of partner violence in young adulthood. Longitudinal follow-up of this sample into high school is underway and will provide an opportunity to see whether effects are sustained as adolescents mature and engage in more intimate relationships. Additionally, testing DM outside of high-risk urban samples would increase confidence in the model’s generalizability.
When compared with an existing evidence-based intervention, DM demonstrated consistent protective effects on TDV-P, TDV-V, and use of negative conflict resolution strategies. The DM comprehensive prevention model holds promise as an effective strategy for reducing violence and unhealthy relationship behaviors among middle school–aged youth.
Supplementary Material
ACKNOWLEDGMENTS
The authors acknowledge the participation of students and schools in the Dating Matters Initiative. The authors also would like to acknowledge the contribution of each funded public health department and their partners; specifically staff working with or housed at the Alameda County Public Health Department (cooperative agreement number CE002052), including Caroline Miller, Melissa Espinoza, Mauro Sifuentes, Molly Baldridge, and Chen Kong-Wick; the Baltimore City Health Department (cooperative agreement number CE002050), including Byron Pugh, Aisha Burgess, and Katrina Brooks; the Broward County Health Department (cooperative agreement number CE002048), including Lenny Mujica, Aimee Wood, Heidi Vaniman, Stacey Lazos, and Renee Podolsky; and the Chicago Department of Public Health (cooperative agreement number CE002054), including Erica Davis, Marlita White, and Delrice Adams. Lastly, the authors acknowledge the contracting organizations that contributed substantially to program implementation and data collection efforts: NORC at the University of Chicago (contract number 200–2011-40998), Research Triangle Institute (contract number 200–2012-51959), and Ogilvy Public Relations (contract number 200–2007-20014/0015); and those who assisted with data imputation and statistical analysis: 2M Research services (contract number 200–2015-62568) and their subcontractors at Texas Tech University, Institute for Measurement, Methodology, Analysis and Policy.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention (CDC).
None of the authors have conflicts of interest. Funding for the entire initiative was provided by the National Center for Injury Prevention and Control at the CDC. PHN, AMVK, NEL, ATT, SD, LFE, WLKM, HK, TB, BF, and LAV worked for the funding organization during most of their participation on the project. BT, EAM, SN, and HJ were funded by CDC through a contract to assist with research design and collect all data (contract number 200-2011-40998). AJT, TDL, KML, and SRG were funded by 2M Research Services (contract number 200-2015-62568). Karna, LLC, is a contractor employing the data manager, who was an onsite contractor at CDC (Johnson).
Footnotes
No financial disclosures were reported by the authors of this paper.
SUPPLEMENTAL MATERIAL
Supplemental materials associated with this article can be found in the online version at https://doi.org/10.1016/j.amepre.2019. 02.022.
REFERENCES
- 1.CDC. Preventing Teen Dating Violence https://www.cdc.gov/violence-prevention/pdf/tdv-factsheet.pdf. Accessed May 13, 2019.
- 2.Exner-Cortens D, Eckenrode J, Bunge J, Rothman E. Revictimization after adolescent dating violence in a matched, national sample of youth. J Adolesc Health 2017;60(2):176–183. 10.1016/j.jadohealth.2016.09.015. [DOI] [PubMed] [Google Scholar]
- 3.Exner-Cortens D, Eckenrode J, Rothman E. Longitudinal associations between teen dating violence victimization and adverse health outcomes. Pediatrics 2013;131(1):71–78. 10.1542/peds.2012-1029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Offenhauer P, Buchalter A. Teen Dating Violence: A Literature Review and Annotated Bibliography Washington, DC: Library of Congress, 2011. [Google Scholar]
- 5.Foshee VA, Benefield TS, Ennett ST, Bauman KE, Suchindran C. Longitudinal predictors of serious physical and sexual dating violence victimization during adolescence. Prev Med 2004;39(5):1007–1016. 10.1016/j.ypmed.2004.04.014. [DOI] [PubMed] [Google Scholar]
- 6.Kann L, McManus T, Harris WA, et al. Youth risk behavior surveillance - United States, 2015. MMWR Surveill Summ 2016;65(6):1–174. 10.15585/mmwr.ss6506a1. [DOI] [PubMed] [Google Scholar]
- 7.Tharp AT, McNaughton Reyes HL, Foshee V, et al. Examining the prevalence and predictors of injury from adolescent dating violence. J Aggress Maltreat Trauma 2017;26(5):445–461. 10.1080/10926771.2017.1287145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.De La Rue L, Polanin JR, Espelage DL, Pigott TD. A meta-analysis of school-based interventions aimed to prevent or reduce violence in teen dating relationships. Rev Educ Res 2017;87(1):7–34. https://doi. org/10.3102/0034654316632061. [Google Scholar]
- 9.Miller E, Tancredi DJ, McCauley HL, et al. One-year follow-up of a coach-delivered dating violence prevention program: a cluster randomized controlled trial. Am J Prev Med 2013;45(1):108–112. 10.1016/j.amepre.2013.03.007. [DOI] [PubMed] [Google Scholar]
- 10.Wolfe DA, Crooks CV, Jaffe P, et al. A school-based program to prevent adolescent dating violence: a cluster randomized trial. Arch Pediatr Adolesc Med 2009;163(8):692–699. 10.1001/archpediatrics.2009.69. [DOI] [PubMed] [Google Scholar]
- 11.O’Leary KD, Slep AMS. Prevention of partner violence by focusing on behaviors of both young males and females. Prev Sci 2012;13(4):329–339. 10.1007/s11121-011-0237-2. [DOI] [PubMed] [Google Scholar]
- 12.Whitaker DJ, Murphy CM, Eckhardt CI, Hodges AE, Cowart M. Effectiveness of primary prevention efforts for intimate partner violence. Partner Abus 2013;4(2):175–195. 10.1891/1946-6560.4.2.175. [DOI] [Google Scholar]
- 13.Dahlberg LL, Krug EG. Violence-a global public health problem. In: Krug E, Dahlberg LL, Mercy JA, Zwi AB, Lozano R, eds. World Report on Violence and Health Geneva, Switzerland: WHO, 2002:1–56. [Google Scholar]
- 14.David-Ferdon C, Simon TR. Preventing Youth Violence: Opportunities for Action Atlanta, GA: National Center for Injury Prevention and Control, CDC, 2014. [Google Scholar]
- 15.Matjasko JL, Vivolo-Kantor AM, Massetti GM, et al. A systematic meta-review of evaluations of youth violence prevention programs: common and divergent findings from 25 years of meta-analyses and systematic reviews. Aggress Violent Behav 2012;17(6):540–552. 10.1016/j.avb.2012.06.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cunradi CB, Caetano R, Clark C, Schafer J. Neighborhood poverty as a predictor of intimate partner violence among white, black, and Hispanic couples in the United States: a multilevel analysis. Ann Epidemiol 2000;10(5):297–308. 10.1016/S1047-2797(00)00052-1. [DOI] [PubMed] [Google Scholar]
- 17.Gorman-Smith D, Tolan P. The role of exposure to community violence and developmental problems among inner-city youth. Dev Psychopathol 1998;10(1):101–116. 10.1017/S0954579498001539. [DOI] [PubMed] [Google Scholar]
- 18.Halliday-Boykins CA, Graham S. At both ends of the gun: testing the relationship between community violence exposure and youth violent behavior. J Abnorm Child Psychol 2001;29(5):383–402. 10.1023/A:1010443302344. [DOI] [PubMed] [Google Scholar]
- 19.Sampson RJ, Lauritsen JL. Violent victimization and offending: individual-, situational-, and community-level risk factors. In: Reiss AJ, Roth JA, eds. Understanding and Preventing Violence, volume 3, Social Influences Washington, DC: National Academy Press, 1994:1–114. [Google Scholar]
- 20.Black BM, Chido LM, Preble KM, et al. Violence exposure and teen dating violence among African American youth. J Interpers Violence 2015;30(12):2174–2195. 10.1177/0886260514552271. [DOI] [PubMed] [Google Scholar]
- 21.Johnson RM, Parker EM, Rinehart J, Nail J, Rothman EF. Neighborhood factors and dating violence among youth. Am J Prev Med 2015;49(3):458–466. 10.1016/j.amepre.2015.05.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Teten Tharp A Dating Matters: the next generation of teen dating violence prevention. Prev Sci 2012;13(4):398–401. 10.1007/s11121-012-0307-0. [DOI] [PubMed] [Google Scholar]
- 23.Teten Tharp A, Burton T, Freire K, et al. Dating Matters™: strategies to promote healthy teen relationships. J Womens Health 2011;20 (12):1–5. 10.1089/jwh.2011.3177. [DOI] [PubMed] [Google Scholar]
- 24.CDC. Dating Matters website www.cdc.gov/violenceprevention/datingmatters/. Accessed October 10, 2017.
- 25.Raudenbush SW, Spybrook J, Congdon R, et al. Optimal Design Plus Empirical Evidence New York, NY: William T. Grant Foundation, 2011. [Google Scholar]
- 26.Niolon PH, Taylor BG, Latzman NE, et al. Lessons learned in evaluating a multisite, comprehensive teen dating violence prevention strategy: design and challenges of the evaluation of dating matters: strategies to promote healthy teen relationships. Psychol Viol 2016;6 (3):452–458. 10.1037/vio0000043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Foshee VA, Bauman KE, Ennett ST, et al. Assessing the long-term effects of the Safe Dates program and a booster in preventing and reducing adolescent dating violence victimization and perpetration. Am J Public Health 2004;94(4):619–624. 10.2105/AJPH.94.4.619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Forehand R, Armistead L, Long N, et al. Efficacy of a parent-based sexual-risk prevention program for African American preadolescents: a randomized controlled trial. Arch Pediatr Adolesc Med 2007;161(12):1123–1129. 10.1001/archpedi.161.12.1123. [DOI] [PubMed] [Google Scholar]
- 29.Foshee VA, McNaughton Reyes HL, Ennett ST, et al. Assessing the effects of Families for Safe Dates, a family-based teen dating abuse prevention program. J Adolesc Health 2012;51(4):349–356. 10.1016/j.jadohealth.2011.12.029. [DOI] [PubMed] [Google Scholar]
- 30.Wolfe DA, Scott K, Reitzel-Jaffe D, et al. Development and validation of the conflict in adolescent dating relationships inventory. Psychol Assess 2001;13(2):277 10.1037/1040-3590.13.2.277. [DOI] [PubMed] [Google Scholar]
- 31.Foshee VA, Bauman KE, Arriaga XB, et al. An evaluation of Safe Dates, an adolescents dating violence prevention program. Am J Public Health 1998;88(1):45–50. 10.2105/AJPH.88.1.45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kurdek LA. Conflict resolution styles in gay, lesbian, heterosexual nonparent, and heterosexual parent couples. J Marriage Fam 1994;56 (3):705–722. 10.2307/352880. [DOI] [Google Scholar]
- 33.Miller Gaubert J, Gubits D, Principe Alderson D, Knox V. The Supporting Healthy Marriage Evaluation: final implementation findings: OPRE Report 20122–12 Washington, DC: Office of Planning, Research and Evaluation, the Administration for Children and Families, HHS; 2012. [Google Scholar]
- 34.Lang KM, Little TD, PcAux Development Team. PcAux: automatically extract auxiliary features for simple, principled missing data analysis (R package version 0.0.0.9004) http://github.com/PcAux-Package/PcAux/. Published 2017. Accessed February 6, 2019.
- 35.Lance CE. Residual centering, exploratory and confirmatory moderator analysis, and decomposition of effects in path models containing interactions. Appl Psychol Meas 1988;12(2):163–175. 10.1177/014662168801200205. [DOI] [Google Scholar]
- 36.Little TD. Longitudinal Structural Equation Modeling New York: Guilford Press, 2013. [Google Scholar]
- 37.Ghosh-Dastidar B, Schafer JL. Multiple edit/multiple imputation for multivariate continuous data. J Am Stat Assoc 2003;98(464):807–817. 10.1198/016214503000000738. [DOI] [Google Scholar]
- 38.Cohen P, Cohen J, Aiken LS, West SG. The problem of units and the circumstance for POMP. Multivariate Behav Res 1999;34(3):315–346. 10.1207/S15327906MBR3403_2. [DOI] [Google Scholar]
- 39.Muthén LK, Muthén BO. Mplus Users Guide 8th ed. Los Angeles, CA: Muthén & Muthén, 1998–2017. [Google Scholar]
- 40.Little TD, Lopez DF. Regularities in the development of children’s causality beliefs about school performance across six sociocultural contexts. Dev Psychol 1997;33(1):165–175. 10.1037/0012-1649.33.1.165. [DOI] [PubMed] [Google Scholar]
- 41.Wolfe DA, Crooks CV, Chiodo D, Hughes R, Ellis W. Observations of adolescent peer resistance skills following a classroom-based healthy relationship program: a post-intervention comparison. Prev Sci 2012;13(2):196–205. 10.1007/s11121-011-0256-z. [DOI] [PubMed] [Google Scholar]
- 42.Smith J, Mulford C, Latzman NE, et al. Taking stock of behavioral measures of adolescent dating violence. J Aggress Maltreat Trauma 2015;24(6):674–692. 10.1080/10926771.2015.1049767. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.