

Summary
Introduction and purpose
The consumption of alcohol among young people and young adults has undergone, in recent decades, a sharp upsurge with the increasingly frequent intake of large quantities of alcohol. The aim of our study was to investigate socio-demographic, economic and behavioural factors that have a major impact on the voluntary alcohol habit in young people.
Methods
The survey was conducted via administration of an anonymous questionnaire based on “the WHO Alcohol Use Disorders Identification Test”, disseminated on-line, to young people and young adults (aged 18 to 35).
Results
We examined a sample of 365 subjects. Consumption of wine and beer were predominant followed by super-alcohol mixes. We found correlations between alcohol use and the following variables: marital status (p < 0.001), parental education (mother p < 0.05; father p < 0.001), income level (p < 0.05), physical activity (p < 0.05) and voluptuous habits (smoke and coffee: p < 0.001.The 5% of men and 1% of women had car accidents during the previous year due to alcohol use and 15% said they did not remember what happened in an alcoholic evening once or twice a month.
Conclusions
The phenomenon of alcohol consummation is deeply ingrained in our reality, with dangerous episodes of binge drinking in young adults with a higher prevalence in the female sex.
Keywords: Young people, Binge drinking, Alcohol
Introduction
The consumption of alcohol among adolescents has undergone a sharp upsurge in recent decades with behavioral changes and increasingly frequent intake of large quantities of alcohol. In community and adolescent social contexts in particular, this is called “binge drinking” or the so-called alcoholic binge which consists in taking five or six alcoholic beverages outside a meal and concentrated in a short time – two hours or less – for the purpose of getting drunk [1]. It is a recreational consumption away from the family context, but among friends, where drinking is associated with a state of well-being, joy and fun combined with emancipation, and where getting drunk becomes a fashion and a source of pride. There is no safe consumption for health, but if you drink alcohol, you should not drink on an empty stomach and you must not exceed the quantities considered at low risk, i.e. 2 units of alcohol per day for men, 1 unit of alcohol per day for women and for over 65s, zero units of alcohol for those under 18 [2]. The excess limits [3] correspond to the one-time consumption of more than 6 Alcoholic Units (UA = 12 grams of pure alcohol) of any alcoholic beverage. The alcoholic unit corresponds to about 10-12 grams of pure alcohol, corresponding to a standard glass of wine (12°, 125 ml), a can of beer (4.5°, 330 ml), an aperitif (18°, 80 ml), or a small glass of spirits (36°, 40 ml). The survey on the consumption of alcohol in adolescence and post-adolescence has aroused great concern in the scientific community as it is closely linked to social problems arising from it, as well as metabolic and behavioral disorders. The problems arising from alcohol consumption in young people, in fact, are different from those of adults [4]. In young people, the negative effects involve changes in the relationship with family members, classmates, colleagues and teachers, with poor academic performance and progressive lengthening of the time needed to complete primary education, aggression, anti-social behavior, crime, public disorder and other high-risk behaviors, such as driving while intoxicated, unprotected sexual activity involving a greater risk of unwanted pregnancy and transmission of sexual diseases [5]. Young people who consume a large amount of alcohol are on the whole more at risk than young people who do not drink at all [6]. Alcohol abuse therefore contributes directly and indirectly to the development of physical, mental and social harm in the drinker. Not only does all this combine to harm the young person physically, emotionally and socially, it is also a permanent negative modifier in the school and university environment, resulting in delayed training and entry to the world of labor.
The ISTAT data [7] report alcohol consumption in the 18-24 age group, compared to the older adult population, with a more episodic frequency, but with higher overall consumption, including heavy drinking prolonged for entire nights. Some authors report a greater likelihood of using psychoactive substances in adolescence and early adulthood, with a positive association between education level and socio-economic situation and consumption and substance abuse [8].
Given these premises, it is essential to investigate the socio-demographic and economic factors that have an overall impact on the voluntary habit of alcohol consumption, especially since the data confirm that young Italians are in the top rank among drinkers worldwide, despite the measures predisposed to reduce this abuse [9].
The aim of the study was to investigate the consumption of alcoholic substances by young people and young adults resident in southern Italy in relation to the socio-economic and cultural situation.
Methods
An observational study was carried out between January 2018 and June 2018, by administration of an anonymous questionnaire, disseminated online to subjects aged between 18 and 35through social networks and based on multiple-choice questions.
The questionnaire was based on the WHO Alcohol Use Disorders Identification Test. Questions were asked concerning the subject’s socio-economic condition, educational level and family nucleus, with particular attention to income. Habits and lifestyles were investigated regarding, apart from alcohol consumption, cigarette smoking, physical activity and coffee consumption. Also assessed were the frequency of alcohol intake, the amount taken daily, the excess consumption of spirits and the effects of alcohol on daily life, with particular attention to alcohol-induced driving accidents. Lastly, we investigated the type of alcohol consumed most frequently.
The sample was defined considering the prevalence of alcohol consummation of 73.3% for males with a n=75 and 44.7% and so a n=95 for women in Sicily, identifying a 95% Confidence Interval (CI) and an absolute accuracy of 10%.
We stratified the sample in relation to age (18-4 years and 25-35 years) and sex, their education (graduate or undergraduate), parents’ education (under or over eight years of education) and income level (0-10.000, 10.000-30.000, 30.000-50.000, 50.000-80.000, > 80.000 euros).
STATISTICAL ANALYSIS
The mean and standard deviation (SD) were calculated with regard to the quantitative variable (age), while absolute and relative frequencies were obtained for categorical data. The Chi-Square test of independence with Yates correction (only for samples with n between 40 and 200) was used to determine any statistically significant associations between the alcohol consummation and all the categorical variables, adopting a relative partition model where the null hypothesis was rejected. Statistical significance thresh-old was set at p = 0.050; p-values of less than 0.050 on two-tailed tests were considered statistically significant. We chose to perform statistical analyses both on all samples (n = 365) and on samples stratified in two age groups (18-24 years and 25-35 years), to identify associations between young people and young adults. All statistical analyses were performed using R software.
Results
All respondents joined the questionnaire: we examined a sample of 365 subjects aged between 18 and 35 years with a mean of 24.70 years (4.5), of which 140/365 (38.6%) were males and 225/365 (62,4%) were females. Of these, 212/365 (58%) said they had used alcohol in the last year at least occasionally; of these, 40% of drinkers were males and 60% were women, with a mean age of 24.68 years (4.1) (Tab. I).
Tab. I.
Distribution of the sample in “drinkers” and “non-drinkers” by sex, age, education, work (employed or not), type of work, sector of work, parents’ education, income level, voluptuous habits.
| Non-drinkers | ||||||
|---|---|---|---|---|---|---|
| Male | Female | |||||
| 15.34% (56) | 26.58% (97) | |||||
| 18-24 yrs | 25-35 yrs | |||||
| 23.29% (85) | 18.63% (68) | |||||
| Single | Married | |||||
| 36.44%(133) | 5.48% (20) | |||||
| Less than 8 yrs | More than 8 yrs | |||||
| 31.51%(115) | 10.41%(38) | |||||
| Employed | Unemployed | |||||
| 9.04%(33) | 32.88%(120) | |||||
| Public employee | Private employee | Business owner | Self-employed | Housewife | Student | Worker |
| 2.47% | 2.19% | 0.27% | 2.74% | 0.82% | 30.96% | 0.55% |
| Agriculture/fishing | Building | Industry | Trade/turism | Public health | Administration | Other |
| 0.27% | 0.55% | 0.82% | 0.55% | 33.42% | 0.27% | 0.82% |
| Mother’s education | Father’s education | |||||
| Less than 8 yrs | More than 8 yrs | Less than 8 yrs | More than 8 yrs | |||
| 12.05% | 29.86% | 15.34% | 26.57% | |||
| < 10,000 | 10,000-30,000 | 30,000-50,000 | 50,000-80,000 | > 80,000 | ||
| 8.77% | 18.90% | 10.14% | 3.56% | 0.55% | ||
| Physical activity | ||||||
| No | Yes | |||||
| 21.92% (80) | 20% (73) | |||||
| Smoker | ||||||
| No | Yes | |||||
| 16.16% (59) | 25.75%(94) | |||||
| Coffee drinker | ||||||
| No | Yes | |||||
| 28.22% (103) | 13.70%(50) | |||||
| Drinkers | ||||||
| Male | Female | |||||
| 23.01% (84) | 35.07% (128) | |||||
| 18-24 yrs | 25-35 yrs | |||||
| 30.14% (110) | 17.95% (102) | |||||
| Single | Married | |||||
| 55.07% (201) | 3.01% (11) | |||||
| Less than 8 yrs | More than 8 yrs | |||||
| 0.27%(1) | 57.81% (211) | |||||
| Employed | Unemployed | |||||
| 15.89%(58) | 42.19% (154) | |||||
| Public employee | Private employee | Business owner | Self-employed | Housewife | Student | Worker |
| 2.74% | 6.30% | 1.37% | 4.11% | 0.55% | 42.19% | 0.27% |
| Agriculture/fishing | Building | Industry | Trade/turism | Public health | Administration | Other |
| 1.10% | 1.10% | 0.27% | 1.10% | 44.38% | 1.37% | 1.91% |
| Mother’s education | Father’s education | |||||
| Less than 8 yrs | More than 8 yrs | Less than 8 yrs | More than 8 yrs | |||
| 10.96% | 46.85% | 11.23% | 46.85% | |||
| < 10,000 | 10,000-30,000 | 30,000-50,000 | 50,000-80,000 | > 80,000 | ||
| 7.40% | 24.38% | 15.07% | 8.49% | 2.74% | ||
| Physical activity | ||||||
| No | Yes | |||||
| 38.08%(139) | 20%(73) | |||||
| Smoker | ||||||
| No | Yes | |||||
| 38.90%(142) | 19.18%(70) | |||||
| Coffee drinker | ||||||
| No | Yes | |||||
| 50.14%(183) | 7.95%(29) | |||||
*the percentage was calculated on the entire sample (n=365); the percentage does not represent “no answer”.
We stratified the sample in two age groups: 18-24 years and 25-35 years. The former represented 195/365 (53.4%) of the sample. Of these 131/195 (67.2%) were women and 64/195 (32.8%) were men. The age group of25-35 years made up 170/365 (46.6%) of the sample, of which 94/170 (55.3%) were women and 76/170 (44.7%) were men (Tab. II).
Tab. II.
Distribution of the sample in two ranges (18-25 yrs and 25-35 yrs) and in “drinkers” and “non-drinkers”, by sex, education, work (employed or not), type of work, parents’ education, income level and voluptuous habits.
| Young people(18-24 years) n = 195 | |||||||
|---|---|---|---|---|---|---|---|
| Non-drinkers | Drinkers | ||||||
| Male | Female | Male | Female | ||||
| 24 (12.31%) | 61 (31.28%) | 40 (20.51%) | 70 (35.90%) | ||||
| Single | Married | Single | Married | ||||
| 84 (43.08) | 1 (0.51%) | 110 (56.41%) | 0 (0%) | ||||
| Less than 8 yrs | More than 8 yrs | Less than 8 yrs | More than 8 yrs | ||||
| 1 (0.51%) | 84 (43.08%) | 1 (0.51%) | 109 (56.41%) | ||||
| Unemployed | Employed | Unemployed | Employed | ||||
| 83 (42.56%) | 2 (1.03%) | 94 (48.21%) | 16(8.21%) | ||||
| Mother’s education | Father’s education | Mother’s education | Father’s education | ||||
| < 8 yrs | > 8 yrs | < 8 yrs | < 8 yrs | < 8 yrs | > 8 yrs | < 8 yrs | > 8 yrs |
| 21 (10.77%) | 64 (32.82%) | 31 (15.9%) | 54 (27.69%) | 23 (11.79%) | 87 (44.62%) | 25 (27.70%) | 85 (43.59%) |
| < 30,000 | 30,000-50,000 | > 50,000 | < 30,000 | 30,000-50,000 | > 50,000 | ||
| 21 (10.7%) | 57(29.23%) | 7 (3.59%) | 12 (6.15%) | 80 (41%) | 18 (9.23%) | ||
| Physical activity | |||||||
| No | Yes | No | Yes | ||||
| 41 (21.03%) | 44 (22.56%) | 43 (22.05%) | 67 (34.36%) | ||||
| Smoker | |||||||
| No | Yes | No | Yes | ||||
| 55 (28.21%) | 30 (15.38%) | 42 (21.54%) | 68 (34.87%) | ||||
| Coffee drinker | |||||||
| No | Yes | No | Yes | ||||
| 31 (15.9%) | 54 (27.69%) | 15 (7.69%) | 95 (48.72%) | ||||
| Young adults (25-35 years) n = 170 | |||||||
| Non-drinkers | Drinkers | ||||||
| Male | Female | Male | Female | ||||
| 32 (18.82%) | 36 (21.18%) | 44 (25.88%) | 58 (34.12%) | ||||
| Single | Married | Single | Married | ||||
| 49 (28.82%) | 19 (11.18%) | 91 (53.53%) | 11 (6.47%) | ||||
| Less than 8 yrs | More than 8 yrs | Less than 8 yrs | More than 8 yrs | ||||
| 3 (1.76%) | 65 (38.24%) | 0 | 81 (60%) | ||||
| Unemployed | Employed | Unemployed | Employed | ||||
| 37 (21.76%) | 31 (18.24%) | 60 (35.29%) | 42 (24.71%) | ||||
| Mother’s education | Father’s education | Mother’s education | Father’s education | ||||
| < 8 yrs | > 8 yrs | < 8 yrs | > 8 yrs | < 8 yrs | > 8 yrs | < 8 yrs | > 8 yrs |
| 23 (13.53%) | 45 (26.47%) | 25 (14.71%) | 43 (25.29%) | 17 (10%) | 84 (49.42%) | 16 (9.41%) | 86 (50.59%) |
| < 30,000 | 30,000-50,000 | > 50,000 | < 30,000 | 30,000-50,000 | > 50,000 | ||
| 11 (6.47%) | 49 (19.%) | 8 (4.7%) | 15(8.8%) | 64 (37.6%) | 23 (13.5%) | ||
| Physical activity | |||||||
| No | Yes | No | Yes | ||||
| 32 (18.82%) | 36 (21.18%) | 30 (17.65%) | 72 (42.35%) | ||||
| Smoker | |||||||
| No | Yes | No | Yes | ||||
| 39 (22,94%) | 29 (17,06%) | 28 (16,47%) | 74 (43,53%) | ||||
| Coffee drinker | |||||||
| No | Yes | No | Yes | ||||
| 19 (11.18%) | 49 (21.82%) | 14 (8.24%) | 88 (51.76%) | ||||
DEMOGRAPHIC FACTORS AND EDUCATION
We compared the responses of drinkers and non-drinkers, evaluating the presence of associations by gender and age. However, we found no statistical associations by sex (χ2: 0.3431; p = 0.55) or age (χ2: 0.4807; p = 0.49). It is important to underline the high percentage of alcohol use in women (71.15%) above the Sicilian average, while the percentage in males is lower (62.5%).
Other factors investigated were years of education and the presence of a paid job and, for students, which type of degree course they are attending (medical or not).
No associations emerged between the years of education, less than or equal to 8, between drinkers and non-drinkers (χ2 = 1.488; p = 0.22) and the presence of a paid job. However, more than half of those who joined the questionnaire were students. Within the subdivision for degree courses, it emerged that in this age group, 30/39 (77%) of medical students usually consume more alcohol than those who attend other degree programs, but we did not find any statistical difference (χ2=0.5959; p = 0.44).
It also emerged that non-drinkers were both male and female, had a stable relationship or were married in greater numbers (of these 22% were males and 33% were women) than drinkers with high statistical associations (χ2 = 7.1059; p < 0.001).
We also investigated whether there were behavioral associations between young people and young adults, dividing the sample in two age groups, 18-24 yrs and 25-35 yrs.
Among the18-24-year-olds, the male drinkers represented 40/64 (62%) while female drinkers represented 70/131 (53%) of the sample. Among the 25-35-year-olds, males drinkers represented 58/94 (61%) of the sample while female drinkers were 44/76 (58%). We did not find any statistical difference by sex.
We investigated associations in the same age groups by education (graduate and undergraduate) and employment. For the former, we found no statistical difference, while a statistical difference emerged from the latter (χ2 with Yates correction = 8.5072; p < 0.01), with medium statistical significance.
For marital status, we found medium statistical associations in young adults, with 60% of drinkers single and 36.67% married (χ2 with Yates correction = 7.1255; p < 0.01).
SOCIO-ECONOMIC FACTORS
Regarding the parents’ education, we observed that both fathers and mothers of non-drinkers have a lower educational qualification with high statistical associations (for mothers: χ2 = 4.7991; p < 0.05; for fathers: χ2 = 13.0779; p < 0.001).
As regards income level, we found statistical associations between income levels of drinkers and non-drinkers (χ2 = 9.8957; p < 0.05). Only 12.7% of drinkers, in fact, had an income of less than 10,000 euros per year, 42% had an income of between 10,000 and 30,000 euros, 25.9% between 30,000 and 50,000 euros, 19.1% between € 50,000 and € 80,000 and as many as 4.7% exceeding € 80,000 annually. Among non-drinkers, on the other hand, 20.9% had an income of less than 10,000 euros a year and only 9.8% have an income of between 50,000 and 80,000 euros or more.
For these factors, we also evaluated associations between young people and young adults and we found a correlation with income level (lower, medium or higher) only for the first group (χ2 with Yates correction = 8.0836; p < 0.05). For parents’ education we found statistical associations both in young people (for fathers χ2 with Yates correction = 3.7782; p < 0.05, that in young adults (χ2 with Yates correction = 8.7869; p < 0.05 for fathers; χ2 with Yates correction = 5.5881; p < 0.05 for mothers).
PHYSICAL ACTIVITY AND VOLUPTUOUS HABITS
We investigated the presence of associations between drinkers and non-drinkers for voluptuous habits and we found high statistical associations between drinkers and non-drinkers for coffee consumption (χ2 = 18.9172; p < 0.001 ) and cigarettes smoking (χ2 = 29.0068; p < 0.001).Statistical associations were also found for physical activity (χ2 = 6.5286; p < 0.05), 63.8% in the drinkers’ group not performing any compared with 50% that did. In the non-drinkers’ group we found 47.2% that did not perform physical activity compared with 50% that did.
As regards lifestyle, drinkers aged 25-35 perform more physical activity than non-drinkers, with statistical associations (χ2 with Yates correction = 4.7487; p < 0.05). Drinkers take coffee more frequently and in higher quantities non-drinkers (χ2 with Yates correction= 12.6321; p < 0.001 for 18-25 yrs; χ2 with Yates correction = 814.0507; p < 0.001). Lastly, drinkers are also smokers in significantly higher percentages than non-drinkers (χ2 with Yates correction = 12.4535; p < 0.05 for 18-25 yrs; for 25-35 yrs χ2 with Yates correction = 14.0507). It is interesting that among drinkers (but this can also be observed in non-drinkers), more women smoke (67%) than men (53%) (Tab. II).
FREQUENCY AND AMOUNT OF ALCOHOL INTAKE
We stratified the sample by frequency of alcohol intake: never or less than once a month, twice/four times a month, twice/three times a week, four time or more per week. We investigated associations of consumption frequency by sex and age and we found statistical associations only in the first case (χ2=10.2781; p < 0.05).
We evaluate alcohol intake according to each age group and sex (1-2 glasses, 3-4 glasses, over 4 glasses). The data are shown in Figure 1. We analyzed the presence of associations between sex and age group in the amount of alcohol intake, but we did not find any statistical associations, even when stratifying the samples between young people and young adults. Among those who drink from 3 to 4 glasses per night, it is interesting to evaluate the relationship between amount and frequency. There emerged a repetition of such high consumption 2-4 times a month, 2-3 times a week or even over 4 times a week, far exceeding the limits set by the WHO (Fig. 2).
Fig. 1.
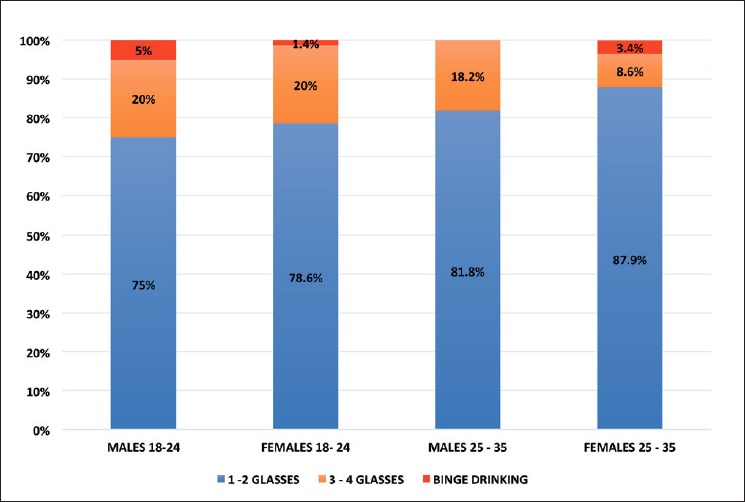
Number of glasses drunk during a single alcoholic evening.
Fig. 2.
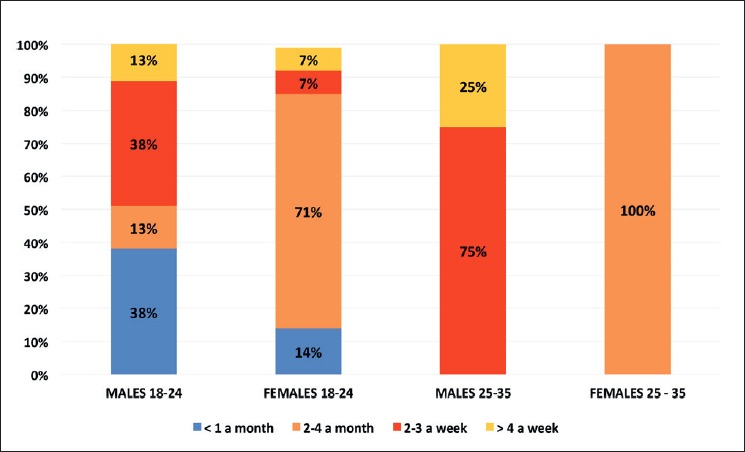
Ratio between frequency and quantity for those who drink 3-4 glasses a night.
In the 18-24 age group, women drank occasionally and monthly, respectively 24.3% and 60% against 20% and 52% for men. Instead, increasing the frequency of drinking, men drank more, respectively 22.5% drink weekly against 12.9% for women, while 5% of men in this age group drank daily against 2.9% for women. In the 25-35 age group, ratios remain similar, with women drinking less frequently than men. 13.8% drank occasionally against 9.1% for men, while 72.4% drank monthly compared with 27.3% for men. As the frequency increases, the results reverse, with 47.7% of men drinking weekly and 15.9% daily compared to 10.3% and 3.4% for women.
TYPE OF ALCOHOL CONSUMED
The most frequently consumed types of alcohol, on the basis of the frequency range of 2-4 times a month, is beer, at 49%, followed by wine 38%, mix of spirits and, lastly, liqueurs and spirits (Fig. 3).
Fig. 3.
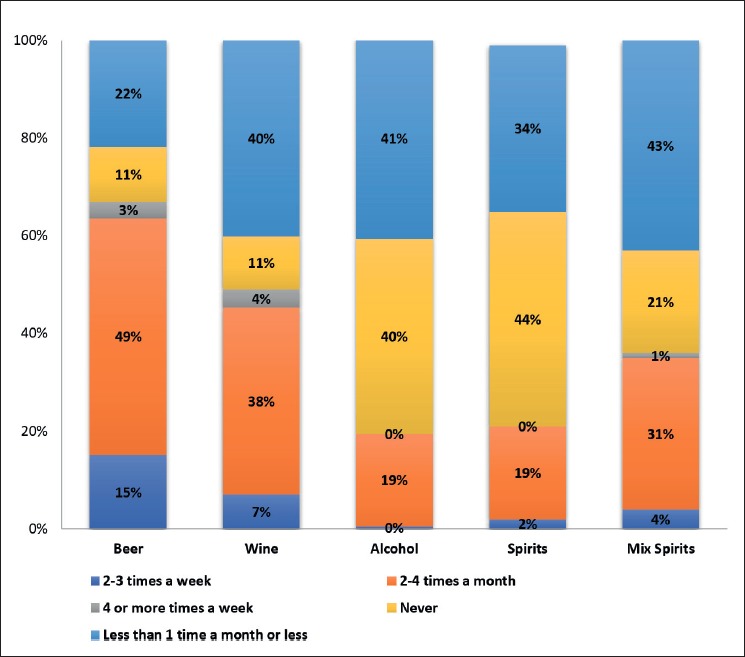
Type of alcoholic beverages most frequently consumed.
THE EFFECT OF ALCOHOL ON EVERYDAY LIFE
6% of men aged 18 to 24 yrs said they could not stop drinking once they started, both several times in the same month and in the same week. 15% felt remorse for the amount of alcohol taken while 3% said that several times a month they had no memory of what happened after an alcoholic evening. Among women between the ages of 18 and 24 years, 4% could not stop drinking once they started, 8% said they could not complete their daily activities due to drinking, 23% had remorse for the alcohol taken and 23% could not remember, several times in the same month, what happened the night before.
In the 25-35 age group, 4% of men failed to complete their daily activities, 7% needed a drink in the morning, 16% felt remorse for the alcohol taken and 12% could not remember what happened the night before. Among women of the same age group, 3% failed to perform normal daily activities, 12% felt guilty about the amount of alcohol taken and 10% had no memory, on several occasions, of what happened the night before.
Among those who responded to the questionnaire, 5% of men and 1% of women aged 18-24 reported having had an alcohol-related accident in the last year, 5% of men and 3% of women in previous years. While in the 25-35 age-band, only 2% of men had accidents in the last year due to drinking and 7% of women in previous years. Lastly, 5% and 3% of men and women aged 18-24, respectively, admitted having a relative concerned about their alcohol consumption and having received advice to stop drinking. In the 25- to 35-year age group, 2% of both men and women had received the same advice.
Discussion and conclusion
Our results are in line with national data and in particular with Sicily, where the percentage of consumers of at least one alcoholic beverage in 2016 was 73.3%among men, 44.7% among women, compared to the national average for both genders [7, 8]. In our sample, women, in all age groups considered, had a higher educational qualification than men. Furthermore, when comparing drinkers and non-drinkers, drinkers showed to have a higher educational qualification and greater availability of financial resources, as they have more often a paid job. As regards socio-economic conditions, younger and older adult drinkers belong to economically more well-off and scholastically higher families, in line with international literature, though some studies reported more drinkers in families with low education [9, 10].
Non-drinkers tend to have stable relationships, but drinkers are predominantly single, according to international literature, with a decrease in drinking accompanying the transition from being single to a first marriage [11, 12].
The people that consume alcoholic beverages are also more often consumers of coffee and cigarettes, but paradoxically they perform more physical activity. Women of both categories smoke and drink more coffee and more often. These data confirm the literature and are worrying due to effects that these three factors can have on health [13].
When alcohol is mixed with caffeine, this can mask its depressant effects, making drinkers feel more alert than they would otherwise. As a result, they may drink more alcohol and become more impaired than they realize, increasing the risk of alcohol-attributable damage [14].
The effects of excessive consumption on respondents have more or less serious repercussions on daily life, influencing them in carrying out normal daily activities, reducing their prudence while driving. About this point, worrying is the fact that 8% of respondents in the last year alone had alcohol-related traffic accidents [15, 16], a figure in line with the national one (ISTAT, 2018) where 7.8% of accidents are caused by drunkenness and the percentage is increasing [17]. The ISTISAN data then showed that among those who had a car accident in the 18-29 age group, the main cause turned out to be driving under the influence of alcohol and drugs (61.6% of cases) [18]. Alarming is the percentage of young people (3.4% compared to 0.7% of those over 30) who, although they know they have to drive, choose not to limit their consumption of alcohol [19]. The results of this study confirm that alcohol abuse is an important risk factor for public health.
It has been shown that reducing or stopping drinking produces health benefits at any age. The elimination of alcohol involves an inversion of the danger for all related chronic diseases, such as cirrhosis of the liver or depression, although there remains a level of risk due to protracted exposure [20]. Reduction or cessation of alcohol consumption is associated with a rapid improvement in physical conditions and a reduction in overall mortality [21]. In particular, young people who drastically decrease their alcohol consumption in the proximity of adulthood significantly reduce the risk of developing alcohol-related damage, particularly to the nervous system [22].
Limiting intake also allows subjects to keep their body weight under control: alcohol provides about 7 kilocalories per gram, requiring a certain activity in order to dispose of it [23-26].
Drinking alcohol, as well as smoking, also involves a considerable expense, not only for drinkers but for all society [27]. According to a recent review, in fact, the economic burden of alcohol on society is substantial, accounting for 0.45% to 5.44% of the Gross Domestic Product [28].
Moreover, we found in our study a statistical association between family income for young people but not for young adults, probably because the latter work more than the former and have a personal salary. Another factor is, as previously reported, that more people in this age group are more married and this could limit alcohol use.
Lastly, a recent study conducted by the University of Washington and published in September 2018 [29] highlighted that the amount of alcohol that should be taken, for safe consumption, is zero. This fact, taken with the due exceptions, highlights even more how policies aimed at reducing alcohol consumption should be an absolute priority. The WHO, too, after a study published recently, has established that there is no safe level to drink alcohol [30].
Obviously, there is low-risk consumption, but the WHO does not set particular limits, because the evidence shows that the ideal situation for health is not drinking at all. Research has shown a lower risk of ischemic events (heart disease, stroke and type 2 diabetes) among middle-aged and older light to moderate drinkers. However, the damaging effects of alcohol far outweigh any potential protective benefit. An older person will get much greater health benefits from being physically active and eating healthy foods that from alcohol [31].
The limit of our study is represented by the fact that self-reported data is often inaccurate, especially for adolescents and furthermore, we used an online survey, and this could have limited the effects of underestimation because the interviewer cannot view the respondents [32].
Diseases resulting from unhealthy behavior, facilitated by an unhealthy environment and solicited by commercial interests, are the dominant health problem of the 21st century. However, there is a clear need to motivate everyone, from young people to adults, so that we can start an important and radical cultural change [33], especially in behaviors adopted at a younger age. The model of drinking we have imported from northern Europe (binge drinking), must therefore be countered by the most effective means and in the shortest time possible.
Prevention remains the key element to combat this phenomenon. Highly necessary is the collaboration between families and the school. Indeed, the first signs of discomfort are among the school desks; it would therefore be very useful to train teachers to intercept this malaise in order to prevent the consequent possible use of tobacco, alcohol and drugs in young adolescents. Although this problem persists enormously on our territory with colossal consequences for the economic, psychic and general lives of the drinkers, prevention measures are lacking.
Promotion programs, such as vaccination, water potabilization, prevention of HAIs remain the most important weapons in the hands of public health: it is, therefore, imperative to establish structured forms of primary and secondary prevention at territorial level in order to prevent this phenomenon [34-43].
Other possible benefits could come from careful control policies and health programs, by increasing the taxation of alcoholic beverages, controlling their sales and sales hours and reducing the exposure of buyers to alcoholic beverage advertisements.
Figures and tables
Acknowledgements
Funding sources: this research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Footnotes
Conflict of interest statement
The authors declare no conflict of interest.
Authors’ contributions
VLF conceived, designed and coordinated the research. VLF, RS, VA, PS, CG and NL contributed to the acquisition, analysis and interpretation of data . VLF, VA and CG evaluated the results. VLF, and VA wrote the manuscript. All Authors revised the manuscript and gave their contribution to improve the paper. All authors read and approved the final manuscript.
References
- [1].Stolle M, Sack PM, Thomasius R. Binge drinking in childhood and adolescence: epidemiology, consequences, and intervention. Dtsch Arztebl Int 2009;106:323-8, https://doi.org/10.3238/arztebl.2009.0323 10.3238/arztebl.2009.0323 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Ministry of Health. Available at: http://www.salute.gov.it/portale/temi/p2_6.jsp?lingua=italiano&id=2346&area=alcol&menu=problema (Last accessed:. 2019, Jan 22).
- [3].Istituto Superiore di Sanità. “L’impatto dei nuovi livelli stabiliti dalle rinnovate linee guide sul consumo alcolico sulla definizione del rischio e il monitoraggio dei consumi a rischio nella popolazione”. Available at: http://www.epicentro.iss.it/alcol/apd2015/nuovo%20indicatore%20rischio(finale).pdf (Last accessed:. 2019, Jan 22).
- [4].Stueve A, O’Donnell LN. Early alcohol initation and subsequent sexual and alcohol risk behaviours among urban youths. Am J Public Health 2005;95:887-93. https://doi.org/10.2105/AJPH.2003.026567 10.2105/AJPH.2003.026567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Townshend JM, Kambouropoulos N, Griffin A, Hunt FJ, Milani RM. Binge drinking, reflection impulsivity, and unplanned sexual behavior: impaired decision-making in young social drinkers. Alcohol Clin Exp Res 2014;381143-50. https://doi.org/10.1111/acer.12333 10.1111/acer.12333 [DOI] [PubMed] [Google Scholar]
- [6].Hingson RW, Heeren T, Winter MR. Age at drinking onset and alcohol dependence: age at onset, duration, and severity. Arch Pediatr Adolesc Med 2006;160:739-46. https://doi.org/10.1001/archpedi.160.7.739 10.1001/archpedi.160.7.739 [DOI] [PubMed] [Google Scholar]
- [7].Dati ISTAT Available at: https://www.istat.it/it/files//2017/04/Consumo_alcol_in_Italia_2016.pdf (Last accessed:. 2019, Jan 22).
- [8].Velásquez J, Scoppetta O. Consumo de sustanciaspsicoactivas en estudiantes de carrerastécnicas y tecnológicas de Santa Fe de Bogotá. Bogotá: 1998, p. 80. [Google Scholar]
- [9].Epidemiologia e monitoraggio alcol-correlato in Italia e nelle Regioni Valutazione dell’Osservatorio Nazionale Alcol sull’impatto del consumo di alcol ai fini dell’implementazione delle attività del Piano Nazionale Alcol e Salute Rapporto 2018 Emanuele Scafato, Silvia Ghirini Claudia Gandin Monica Vichi Riccardo Scipione e il Gruppo di Lavoro CSDA (Centro Servizi Documentazione Alcol). [Google Scholar]
- [10].Keyes KM, Hasin DS. Socio-economic status and problem alcohol use: the positive relationship between income and the DSM-IV alcohol abuse diagnosis. Addiction 2008;103:1120-30. https://doi.org/10.1111/j.1360-0443.2008.02218.x 10.1111/j.1360-0443.2008.02218.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Sargent JD, Wills TA, Stoolmiller M, Gibbons J, Gibbons FX. Alcohol use in motion pictures and its relation with early-onset teen drinking. J Stud Alcohol 2006;67:54-65. https://doi.org/10.15288/jsa.2006.67.54 10.15288/jsa.2006.67.54 [DOI] [PubMed] [Google Scholar]
- [12].Prescott CA, Kendler KS. Associations between marital status and alcohol consumption in a longitudinal study of female twins. J Stud Alcohol 2001;62:589-604. https://doi.org/10.15288/jsa.2001.62.589 10.15288/jsa.2001.62.589 [DOI] [PubMed] [Google Scholar]
- [13].Vinader-Caerols C, Monleón S, Carrasco C, Parra A. Effects of alcohol, coffee, and tobacco, alone or in combination, on phyrsiological parameters and anxiety in a young population, J Caffeine Res 2012;2:70-6. https://doi.org/10.1089/jcr.2012.0018 10.1089/jcr.2012.0018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].McKetin R, Coen A, Kaye S. A comprehensive review of the effects of mixing caffeinated energy drinks with alcohol. Drug Alcohol Depend 2015;151:15-30. https://doi.org/10.1016/j.drugalcdep.2015.01.047 10.1016/j.drugalcdep.2015.01.047 [DOI] [PubMed] [Google Scholar]
- [15].Rehm J, Gmel G, Sempos CT, Trevisan M. Alcohol-related morbidity and mortality. Alcohol Res Health 2003;27:39-51. [PMC free article] [PubMed] [Google Scholar]
- [16].Taylor B, Rehm J. The relationship between alcohol consumption and fatal motor vehicle injury: high risk at low alcohol levels. Alcohol Clin Exp Res 2012;36:1827-34. https://doi.org/10.1111/j.1530-0277.2012.01785.x 10.1111/j.1530-0277.2012.01785.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].ISTAT. Incidenti stradali. Avaible at: https://www.istat.it/it/files/2018/07/Incidenti-stradali_2017.pdf (Last accessed: May 2019).
- [18].Rapporti ISTISAN. Avaible at: http://old.iss.it/binary/publ/cont/11_4_web.pdf (Last accessed: May 2019).
- [19].Istituto Superiore di Sanità: Epidemiologia e monitoraggio alcol-correlato in Italia e nelle Regioni. Avaible at: https://www.epicentro.iss.it/alcol/apd2018/Rapporto%20ISTISAN%20monitoraggio%20alcol%20correlato%20in%20Italia%202018.pdf (Last accessed: May 2019).
- [20]. Global status report on alcohol and health. 2014 Avaible at: http://apps.who.int/iris/bitstream/handle/10665/112736/9789240692763_eng.pdf;jsessionid=EEFA1BEFABB665D290349718E3C76924?sequence=1 (Last accessed: Jan 2019).
- [21].Charakida M, Georgiopoulos G, Dangardt F, Chiesa ST, Hughes AD, Rapala A, Davey Smith G, Lawlor D, Finer N, Deanfield JE. Early vascular damage from smoking and alcohol in teenage years: the ALSPAC study. Eur Heart J 2019;40:345-53. https://doi.org/10.1093/eurheartj/ehy524 10.1093/eurheartj/ehy524 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].López-Caneda E, Cadaveira F, Correas A, Crego A, Maestú F, Rodríguez Holguín S. The brain of binge drinkers at rest: alterations in theta and beta oscillations in first-year college students with a binge drinking pattern. Front Behav Neurosci 2017;11:168 https://doi.org/10.3389/fnbeh.2017.00168 10.3389/fnbeh.2017.00168 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Romano-Spica V, Macini P, Fara GM, Giammanco G, GSMS - Working Group on Movement Sciences for Health Italian Society of Hygiene Preventive Medicine and Public Health Adapted physical activity for the promotion of health and the prevention of multifactorial chronic diseases: the Erice Charter. Ann Ig 2015;27:406-14. https://doi.org/10.7416/ai.2015.2028 10.7416/ai.2015.2028 [DOI] [PubMed] [Google Scholar]
- [24].Squeri R, Genovese C, Palamara MAR, Trimarchi G, Ceccio C, Donia V, Pecoraro M, La Monica G, La Fauci V. Childhood obesity: risk factors involved An observational study on the effects of early and late risk factors on the development of childhood obesity in the South of Italy. EBPH 2018;15(4). [Google Scholar]
- [25].Lazzeri G, Panatto D, Pammolli A, Azzolini E, Simi R, Meoni V, Giacchi MV, Amicizia D, Gasparini R. Trends in overweight and obesity prevalence in Tuscan schoolchildren (2002-2012). Public Health Nutr 2015;18:3078-85. https://doi.org/10.1017/S1368980015001676 10.1017/S1368980015001676 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Lazzeri G, Panatto D, Domnich A, Arata L, Pammolli A, Simi R, Giacchi MV, Amicizia D, Gasparini R. Clustering of health-related behaviors among early and mid-adolescents in Tuscany: results from a representative cross-sectional study. J Public Health (Oxf) 2018;40:e25-e33. https://doi.org/10.1093/pubmed/fdw134 10.1093/pubmed/fdw134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].La Fauci V, Squeri R, Genovese C, Alessi V, Facciolà A. The ‘Dangerous Cocktail’: an epidemiological survey on the attitude of a population of pregnant woman towards some pregnancy risk factors. J Obstet Gynaecol. 2019. August 2:1-6 [Epub ahead of print] https://doi.org/10.1080/0143615.2019.1621818 10.1080/0143615.2019.1621818 [DOI] [PubMed] [Google Scholar]
- [28].Thavorncharoensap M, Teerawattananon Y, Yothasamut J, Lertpitakpong C, Chaikledkaew U. The economic impact of alcohol consumption: a systematic review. Subst Abuse Treat Prev Policy 2009;4:20 https://doi.org/10.1186/1747-597X-4-20 10.1186/1747-597X-4-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].GBD 2016 Alcohol Collaborators. Alcohol use and burden for 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018;392:1015-35. https://doi.org/10.1016/S0140-6736(18)31310-2 10.1016/S0140-6736(18)31310-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Burton R, Sheron N. No level of alcohol consumption improves health. Lancet 2018;392:987-8. https://doi.org/10.1016/S0140-6736(18)31571-X 10.1016/S0140-6736(18)31571-X [DOI] [PubMed] [Google Scholar]
- [31].Avaible on http://www.euro.who.int/en/health-topics/disease-prevention/alcohol-use/data-and-statistics/q-and-a-how-can-i-drink-alcohol-safely (Last accessed: Jan 2019).
- [32].Bertol E, Vaiano F, Boscolo-Berto R, Fioravanti A, Palumbo D, Catalani V, Mari F, Patussi V, Serpelloni G. Alcohol, caffeine, and nicotine consumption in adolescents: hair analyrsis versus self-report. Am J Drug Alcohol Abuse 2017;43:341-9. https://doi.org/10.1080/00952990.2016.1216556 10.1080/00952990.2016.1216556 [DOI] [PubMed] [Google Scholar]
- [33].Cannavò G, Delia S, Grecò MC, Laganà P. Adolescents and alcohol: a survey in the city of Messina (Italy). Igiene e Sanità Pubblica 2009;65:53-8. [PubMed] [Google Scholar]
- [34].Caselli E, Brusaferro S, Coccagna M, Arnoldo L, Berloco F, Antonioli P, Tarricone R, Pelissero G, Nola S, La Fauci V, Conte A, Tognon L, Villone G, Trua N, Mazzacane S, SAN-ICA Study Group Reducing healthcare-associated infections incidence by a probiotic-based sanitation system: a multicentre, prospective, intervention study. PLoS One 2018;1:e0199616 https://doi.org/10.1371/journal.pone.0199616 10.1371/journal.pone.0199616 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Squeri R, Genovese C, Trimarchi G, Palamara MAR, La Fauci V. An evaluation of attitude toward vaccines among healthcare workers of a University Hospital in Southern Italy. Ann Ig 2017;29:595-606. https://doi.org/10.7416/ai.2017.2188 10.7416/ai.2017.2188 [DOI] [PubMed] [Google Scholar]
- [36].Genovese C, La Fauci V, Squeri A, Trimarchi G, Squeri R. HPV vaccine and autoimmune diseases: systematic review and meta-analysis of the literature. J Prev Med Hyg 2018;59:E194-E199. https://doi.org/10.15167/2421-4248/jpmh2018.59.3.998 10.15167/2421-4248/jpmh2018.59.3.998 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].La Fauci V, Riso R, Facciolà A, Merlina V, Squeri R. Surveillance of microbiological contamination and correct use of protective lead garments. Ann Ig 2016;28:360-6. https://doi.org/10.7416/ai.2016.2116 10.7416/ai.2016.2116 [DOI] [PubMed] [Google Scholar]
- [38].La Fauci V, Costa GB, Arena A, Ventura Spagnolo E, Genovese C, Palamara MA, Squeri R. Trend of MDR-microorganisms isolated from the biological samples of patients with HAI and from the surfaces around that patient. New Microbiol 2018;41:42-6. [PubMed] [Google Scholar]
- [39].La Fauci V, Genovese C, Facciolà A, Palamara MAR, Squeri R. Five-year microbiological monitoring of wards and operating theatres in southern Italy. J Prev Med Hyg 2017;58:E166-E172. [PMC free article] [PubMed] [Google Scholar]
- [40].Genovese C, Picerno IAM, Trimarchi G, Cannavò G, Egitto G, Cosenza B, Merlina V, Icardi G, Panatto D, Amicizia D, Orsi A, Colosio C, Marsili C, Lari C, Palamara MAR, Vitale F, Casuccio A, Costantino C, Azara A, Castiglia P, Bianco A, Currà A, Gabutti G, Stefanati A, Sandri F, Florescu C, Marranzano M, Giorgianni G, Fiore V, Platania A, Torre I, Cappuccio A, Guillari A, Fabiani L, Giuliani AR, Appetiti A, La Fauci V, Squeri A, Ragusa R, Squeri R. Vaccination coverage in healthcare workers: a multicenter cross-sectional study in Italy. J Prev Med Hyg 2019;60:E12-E17. https://doi.org/10.15167/2421-4248/jpmh2019.60.1.1097 10.15167/2421-4248/jpmh2019.60.1.1097 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].La Fauci V, Costa GB, Facciolà A, Conti A, Riso R, Squeri R. Humidifiers for oxygen therapy: what risk for reusable and disposable devices? J Prev Med Hyg 2017;58:E161-E165. [PMC free article] [PubMed] [Google Scholar]
- [42].Squeri R, La Fauci V, Sindoni L, Cannavò G, Ventura Spagnolo E. Study on hepatitis B and C serologic status among municipal solid waste workers in Messina (Italy). J Prev Med Hyg 2006;47:110-3. [PubMed] [Google Scholar]
- [43].La Fauci V, Sindoni D, Grillo OC, Calimeri S, Lo Giudice D, Squeri R. Hepatitis E virus (HEV) in sewage from treatment plants of Messina University Hospital and of Messina City Council. J Prev Med Hyg 2010;51:28-30. [PubMed] [Google Scholar]