

Abstract
Purpose
To report our findings in a case of bilateral Mooren's ulcer that developed after filtering surgeries using the EX-PRESS glaucoma filtering device (EX-PRESS surgery).
Patients and methods
A 71-year-old Japanese man with primary open angle glaucoma underwent EX-PRESS surgery first in his left eye and 1 month later in his right eye. He developed Mooren's ulcer in his right eye at 7 months and in his left eye at 10 months after the initial EX-PRESS surgery. Systemic examinations showed no collagen vascular disease, and he did not have a history of bacterial or viral infections. He was not allergic to metallic materials. Before the EX-PRESS surgery, he had underdone cataract surgery combined with trabeculotomy in both eyes, and a reoperation of trabeculotomy in his left eye. He had not developed Mooren's ulcer after these surgeries. The Mooren's ulcer after the EX-PRESS surgery was treated with oral prednisolone (30 mg tapering) in combination with topical 0.1% betamethasone sodium. The ulcers were responsive and healed well in three months.
Conclusions
The EX-PRESS devices were most likely the cause of the Mooren's ulcers considering that they were located close to the site of EX-PRESS insertion and no peripheral corneal ulcer developed after prior intraocular surgeries.
Keywords: Mooren's ulcer, Glaucoma implant surgery, EX-PRESS glaucoma filtering device, Autoimmune reaction, Surgical injury
1. Introduction
Mooren's ulcer is a rare, painful ulceration of the peripheral cornea with conjunctival and episcleral injection.1,2 The course is progressive, and the entire cornea can be involved. A wide variety of systemic diseases including herpes zoster,3 hepatitis C,4 and parasitic infection5 have been associated with Mooren's ulcers. In addition, there have been other causes associated with Mooren's ulcer, e.g., physical trauma,6 cataract surgery,7 pterygium surgery,8 penetrating keratoplasty,9,10 and epikeratoplasty.11
We report our findings in a case of bilateral Mooren's ulcers that developed following filtering surgery using the EX-PRESS glaucoma filtering device.
2. Case report
A 71-year-old Japanese man underwent EX-PRESS surgery for primary open angle glaucoma first in his left eye and 1 month later in his right eye. The bleb size was small in the left eye and moderate in the right eye, and the intraocular pressures were well controlled bilaterally. Seven months after the EX-PRESS surgery, he complained of redness and a foreign body sensation in his right eye. A corneal ulcer with epithelial defect was detected near the site of the EX-PRESS insertion, and limbitis with severe scleral injection was observed (Fig. 1). An allergic reaction to the nylon sutures was suspected, and they were removed. Then, 0.5% levoflaxin and 0.1% fluorometholone were applied topically, and there was a slight reduction in the size of the ulcer and infiltration, however a complete resolution was not observed. Topical 1% betamethasone sodium phosphate was started, and the corneal ulcer, limbitis, and scleral injection gradually decreased.
Fig. 1.
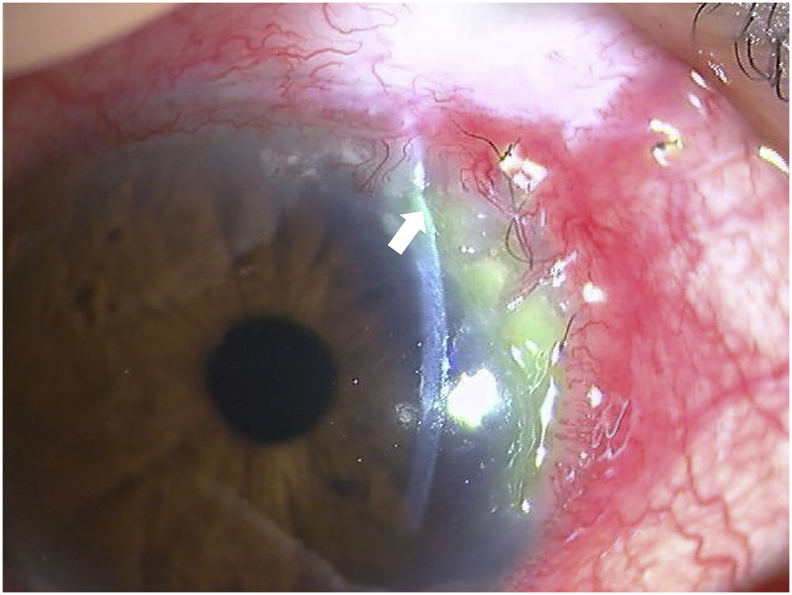
Slit-lamp photograph of the right eye at 7 months after the EX-PRESS surgery. A marginal corneal ulcer can be seen close to the site of the EX-PRESS implantation with severe conjunctival injection. Arrow indicates the site of EX-PRESS implantation.
Ten months after the surgery in his left eye, a similar corneal ulcer developed near the site of EX-PRESS insertion (Fig. 2). After the sutures around the limbus were removed, topical 0.1% betamethasone sodium phosphate was applied to his left eye and continued in his right eye. However, the corneal ulcers in both eyes responded less favorably, and they progressed with thinning and a steep undermined leading edge (Fig. 3).
Fig. 2.
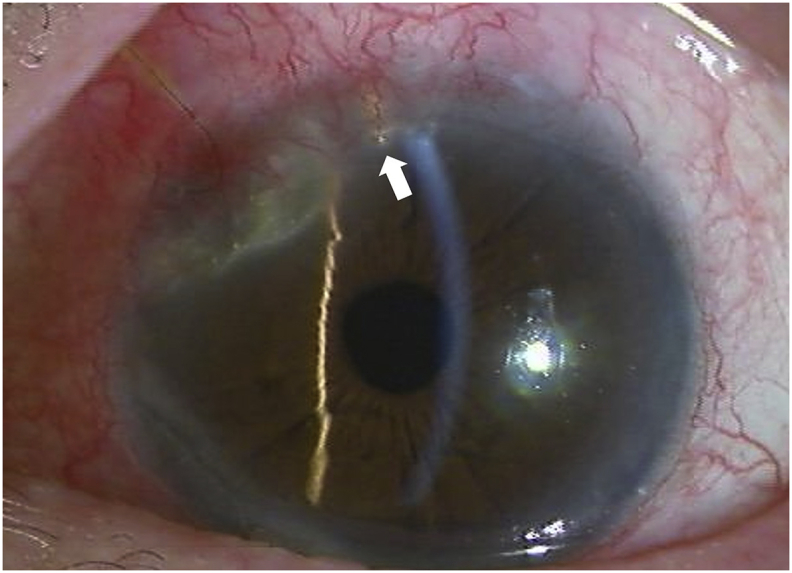
Slit-lamp photograph of the left eye at 10 months after the EX-PRESS surgery. A marginal corneal ulcer close to the site of the EX-PRESS implantation with conjunctival and scleral injection. Arrow indicates the site of EX-PRESS insertion.
Fig. 3.

Slit-lamp photograph of the right eye (3a) and left eye (3b) taken during topical steroid therapy. Bilateral progressive thinning of the ulcers with a steep undermined leading edge can be seen.
Gram staining of corneal scrapings did not show any microorganisms. Cultures for bacteria and fungi were negative, and there was no mucopurulent eye discharge. We diagnosed this case with Mooren's ulcers bilaterally.
Then, 30 mg of oral prednisolone combined with topical 0.1% betamethasone sodium was started and tapered gradually as the signs and symptoms decreased. The corneal ulcers were responsive and healed well in three months. The 0.1% topical betamethasone sodium has been continued to prevent recurrences. There have been no recurrences of the ulcerations in either eye during the 2-year follow-up (Fig. 4).
Fig. 4.

Slit-lamp photograph of the right eye (3a) and left eye (3b) of the patient at 2 years after the onset of the ulcer in the right eye. The corneal epithelium has healed with thinning of corneal stroma after the systemic steroid therapy. Betamethasone sodium phosphate 0.1% is being continued.
Nine years before the EX-PRESS surgery, he had cataract surgery combined with trabeculotomy bilaterally, and a reoperation of trabeculotomy four years previously in his left eye. He had not developed any complications after these surgeries. He was being treated with conventional medications for the diabetes mellitus and hypertension.
His laboratory data showed that he had mild liver dysfunction, and the hepatitis C antibody was negative. He had no history of allergy including that to metallic materials. Blood tests, including complete blood cell, platelet count, antinuclear antibodies, rheumatoid factor, C-reactive protein, liver function tests, blood urea nitrogen and creatinine tests, fasting blood sugar tests, revealed no abnormal findings associated with collagen vascular disease. Patch testing for metallic allergy was negative for the metal components of the EX-PRESS glaucoma filtering device.
3. Discussion
Although EX-PRESS surgery has a minimum insult to the cornea, it has been recently shown that there is a decrease in the corneal endothelial cell density after the EX-PRESS surgery.12, 13, 14 Our report is the first to show Mooren's ulcers developing following the EX-PRESS surgery. The differential diagnoses for Mooren's ulcer are bacterial corneal ulcer, rheumatoid arthritis (RA), scleritis, and delle associated with conjunctival chemosis. The patient had no mucopurulent eye discharge. He also did not show the common symptoms of RA such as joint inflammation and abnormal laboratory finding associated with RA. Although scleritis sometimes accompanies corneal peripheral ulcer in the late phase, he had no history of scleritis. As for a delle, it represents an area of localized corneal thinning without epithelial defect. Thus, we diagnosed his condition as Mooren's ulcers developing following the EX-PRESSS surgery.
Mooren's ulcer is believed to be caused by an autoimmune mechanism15 with both humoral- and cell-mediated autoimmune phenomena associated with it.2,10,11,15, 16, 17, 18, 19 The triggers for the hyperactive immune reactions might be trauma, surgery, and systemic or local infections.2, 3, 4, 5, 6, 7, 8, 9, 10, 11
Gottsch et al. suggested that prior corneal surgery may play a role in the pathogenesis of Mooren's ulcer.10 In addition, some studies have implied that the epithelial basement membrane of corneal epithelium and especially the corneal stem cells are the specific target of this disease.20 The limbal epithelium may be a more specific target.21 We suggest that the glaucoma implant device may have increased the risk of an autoimmune reaction against the peripheral cornea. The question remains, however, whether the implanted device material or the surgical trauma was the cause of the Mooren's ulcers. It must also be considered that Mooren's ulcer might be a multifactorial disorder.
We recommend that clinicians pay special attention to marginal ulcer or limbal injection after EX-PRESS surgery.
Patient consent
Consent to perform the surgery and to publish this case report was obtained. This report does not contain any personal information that could lead to the identification of the patient.
Authors’ contributions
All authors agree to be accountable for all aspects of the work, have drafted and revised the manuscript critically, and have final approval of the final version.
Funding
No funding was received for this work.
Declaration of competing interest
No conflict of interest exists.
Acknowledgements and Disclosures
The authors thank Professor Emeritus Duco Hamasaki of the Bascom Palmer Eye Institute for his critical discussion and final manuscript version.
Footnotes
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ajoc.2020.100588.
Appendix A. Supplementary data
The following is the Supplementary data to this article:
References
- 1.Brown S.I. Mooren's ulcer. Treatment by conjunctival excision. Br J Ophthalmol. 1975;59:675–682. doi: 10.1136/bjo.59.11.675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Chow C.Y.C., Foster C.S. Mooren's ulcer. Int Ophthalmol Clin. 1996;36:1–13. doi: 10.1097/00004397-199603610-00003. [DOI] [PubMed] [Google Scholar]
- 3.Mondino B.J., Brown S.I. Peripheral corneal ulcers with herpes zoster ophthalmicus. Am J Ophthalmol. 1978;86(5):611–614. doi: 10.1016/0002-9394(78)90176-9. [DOI] [PubMed] [Google Scholar]
- 4.Wilson S.E., Lee W.M., Murakami C., Weng J., Moninger G.A. Mooren-type hepatitis C virus-associated corneal ulceration. Ophthalmology. 1994;101:736–745. doi: 10.1016/s0161-6420(94)31291-7. [DOI] [PubMed] [Google Scholar]
- 5.Zelefsky J.R., Srinivasan M., Kundu A. Hookworm infestation as a risk factor for Mooren's ulcer in South India. Ophthalmology. 2007;114(3) doi: 10.1016/j.ophtha.2006.08.014. [DOI] [PubMed] [Google Scholar]
- 6.Zegans M.E., Srinivasan M., Mchugh T. Mooren ulcer in south India: serology and clinical risk factors. Am J Ophthalmol. 1999;128:205–210. doi: 10.1016/s0002-9394(99)00162-2. [DOI] [PubMed] [Google Scholar]
- 7.Arentsenn J.J., Christansen J.M., Maumense A.E. Marginal ulceration after intracapsular cataract extraction. Am J Ophthalmol. 1976;81:194–197. doi: 10.1016/0002-9394(76)90730-3. [DOI] [PubMed] [Google Scholar]
- 8.Kim E.C., Jun A.S., Kim M.S., Jee D. Mooren ulcer occurring at donor site after conjunctivolimbal autograft for recurrent pterygium. Cornea. 2012;31:1357–1358. doi: 10.1097/ICO.0b013e31824d7041. [DOI] [PubMed] [Google Scholar]
- 9.Mondino B.J., Hofbauer J.D., Foos R.Y. Mooren's ulcer after penetrating keratoplasty. Am J Ophthalmol. 1987;103:53–56. doi: 10.1016/s0002-9394(14)74169-8. [DOI] [PubMed] [Google Scholar]
- 10.Gottsch J.D., Liu S.H., Stark W.J. Mooren's ulcer and evidence of stromal graft rejection after penetrating keratoplasty. Am J Ophthalmol. 1992;113:412–417. doi: 10.1016/s0002-9394(14)76164-1. [DOI] [PubMed] [Google Scholar]
- 11.Teichmann K.D., Wagoner M.D. Mooren ulcer following epikeratoplasty for keratoconus. Arch Ophthalmol. 1998;116:1381–1382. [PubMed] [Google Scholar]
- 12.Konopinska J., Deniziak M., Saeed E. Prospective randomized study comparing combined phaco-ExPress and phacotrabeculectomy in open angle glaucoma treatment: 12-month follow-up. J Ophthalmol. 2015;2015:720109. doi: 10.1155/2015/720109. E-Pub Jun 7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ishida K., Moroto N., Murata K., Yamamoto T. Effect of glaucoma implant surgery on intraocular pressure reduction, flare count, anterior chamber depth, and corneal endothelium in primary open-angle glaucoma. Jpn J Ophthalmol. 2017;61:334–346. doi: 10.1007/s10384-017-0512-2. [DOI] [PubMed] [Google Scholar]
- 14.Toyokawa N., Araki-Sasaki K., Kimura H., Kuroda S. Changes of corneal endothelial cell density after Ex-PRESS glaucoma shunt implantation: 2-year follow-up study. J Clin Ophthalmol. 2018;2:38–43. [Google Scholar]
- 15.Brown S.I., Mindino B.J., Rabin B.S. Autoimmune phenomenon in Mooren’s ulcer. Am J Ophthalmol. 1976;82:835–840. doi: 10.1016/0002-9394(76)90058-1. [DOI] [PubMed] [Google Scholar]
- 16.Mondino B.J., Brown S.I., Rabin B.S. Cellular immunity in Mooren's ulcer. Am J Ophthalmol. 1978;85:788–791. doi: 10.1016/s0002-9394(14)78106-1. [DOI] [PubMed] [Google Scholar]
- 17.Foster C.S., Kenyon K.R., Greier J. The immunopathology of Mooren's ulcer. Am J Ophthalmol. 1979;88:149–159. doi: 10.1016/0002-9394(79)90459-8. [DOI] [PubMed] [Google Scholar]
- 18.Gottsch J.D., Liu S.H., Minkovitz J.B. Autoimmunity to a cornea-associated stromal antigen in patients with Mooren's ulcer. Investig Ophthalmol Vis Sci. 1995;45:1541–1547. [PubMed] [Google Scholar]
- 19.Shinoyama K., Ueta M., Sotozono C. Immunohistochemical analysis of inflammatory limbal conjunctiva adjacent to Mooren's ulcer. Br J Ophthalmol. 2013;97:362–366. doi: 10.1136/bjophthalmol-2012-302631. [DOI] [PubMed] [Google Scholar]
- 20.van der Gaag R., Abdillahi H., Stilma J.S., Vetter J.C.M. Circulation antibodies against corneal epithelium and hookworm in patients with Mooren's ulcer from Sierra Leone. Br J Ophthalmol. 1983;67:623–628. doi: 10.1136/bjo.67.9.623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cotsarelis G., Cheng S.Z., Dong G., Sun T.T., Lavker R.M. Existence of slow- cycling limbal epithelial basal cells that can be preferentially stimulated to proliferate: implications on epithelial stem cells. Cell. 1989;57(2):201–209. doi: 10.1016/0092-8674(89)90958-6. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.