

Abstract
Extra-gonadal pure yolk sac tumor of the ear is very rare. We report a case of a yolk sac tumor of the ear and review the English literature in PubMed. The initial complaint was a mass protruding out of the external auditory canal. Computed tomography (CT) showed a large irregularly enhancing isodense mass lesion measuring 42*16 mm in the right external auditory canal, the right mastoid process, and extending to the right back parapharyngeal space with unclear border. Laboratory studies revealed that serum alpha fetoprotein (AFP) was significantly elevated at 664.60 ng/ml (range, 0 to 25 ng/ml), and neuron-specific enolase (NSE) was 28.3 ng/ml (range, 0 to 16.3 ng/ml). After finishing 6 cycles of chemotherapy, the patient underwent a total resection of yolk sac tumor of the ear. In addition, we review the English literature of the yolk sac tumor of the ear.
Keywords: Yolk sac tumor, ear, external auditory canal
Yolk sac tumors, also known as endodermal sinus tumors are one of the common malignant germ cell tumors which account for 3% of all childhood malignant tumors. Yolk sac tumors often arise in gonadal sites such as ovary and testis. Yolk sac tumors of the extra-gonadal region are rare. It has been reported that extra-gonadal occurrence of Yolk sac tumors are involved in the spinal cord [1], urachal [2], abdominal wall [3], mediastinum [4], vagina [5], gluteus [6], the brain [7,8], the liver [9], head and neck region [10], etc. Yolk sac tumor of the ear is rare [11-13]. To our knowledge, there are only 9 cases reported about the yolk sac tumor of the ear. We aimed to report another case of primary yolk sac tumor of external auditory canal and review the previous cases in the literature.
Case report
A 18-month-year old male child presented to the Department of Otorhinolaryngology, The First Affiliated Hospital of Sun Yat-sen University. His parents found a mass in his right side of the external auditory canal approximately measuring 5*3 mm.
One month later, the mass growth to 30*20 mm with a little bleeding. The parents took the patient to the Department of Otorhinolaryngology, Sun Yat-sen Memorial Hospital of Sun Yat-sen University. Endoscopic examination revealed a dark red mass blocked and protruding out of the right external auditory canal. Laboratory studies revealed that serum alpha fetoprotein (AFP) was significantly elevated at 664.60 ng/ml (range, 0 to 25 ng/ml), and neuron-specific enolase (NSE) was 28.3 ng/ml (range, 0 to 16.3 ng/ml). Other tumor biomarkers including b-HCG, carcinoembryonic antigen (CA125, CA15-3, CA19-9, CA211, CA72-4), and other serum examination were normal. Temporal bone computed tomography scan showed a large irregularly enhancing isodense mass lesion measuring 42*16 mm in the right external auditory canal, the right mastoid process, and extending to the right back parapharyngeal space with unclear border. There were several enlarged lymph nodes in the II level of the bilateral neck region. Biopsy of the mass was then performed.
Microscopically, the tumor was located underneath the epidermis with partially ulceration. The loose meshwork of interconnected spaces and small cysts were lined by round or ovarian tumor cells with primitive appearance. The papillary fibrovascular core lined by a single layer of tumor cells which pathognomonic Schiller-Duval bodies were poorly formed. Hyaline globules could be found in the stroma (Figure 1). Immunohistochemistry staining showed that tumor cells were positive for cytokeratin, SALL4, glypican-3, focal positive for EMA, vimentin, CD10, and CD34, and negative for AFP, HCG, PLAP, p63, SMA, CD30, CD31, CD56, S-100 protein, synaptophysin, chromogranin A, RCC, androgen receptor, and GCDFP-15. According to the histopathological findings and elevated serum AFP level, the pathologist diagnosed as a yolk sac tumor. However, the parents refused the chemotherapy due to the economic condition.
Figure 1.
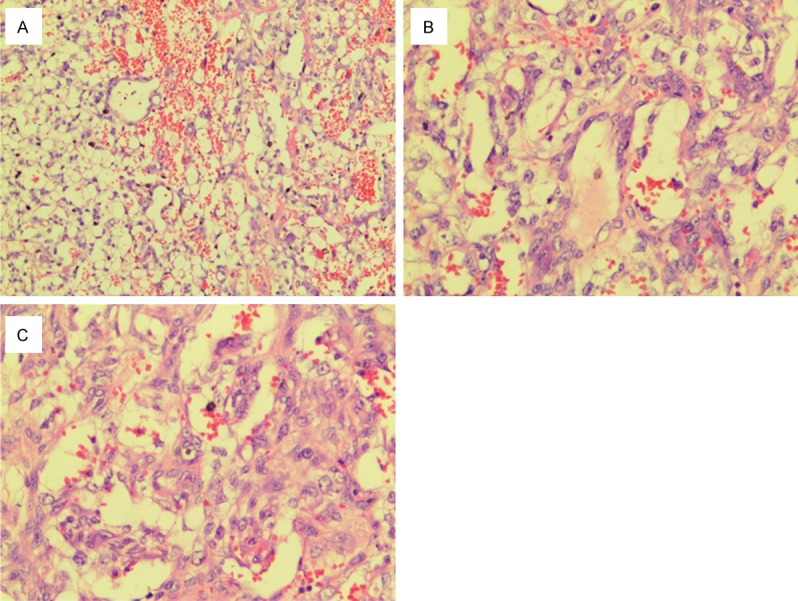
(A, B) The tumor located underneath the epidermis with partially ulceration. The loose meshwork of interconnected spaces and small cysts were lined by round or ovary tumor cells with the primitive appearance. The papillary fibrovascular core lined by a single layer of tumor cells. (C) Pathognomonic Schiller-Duval bodies were poorly formed. Hyaline globules could be found in the stroma. (The magnification of the (A-C) are 100, 200, and 200, respectively).
Four months later, with the rapid growth, the tumor reached about 87*66 mm (Figure 2). The patient was admitted to Sun Yat-sen University Cancer Center and Guangzhou Red Cross Hospital for the chemotherapy. Temporal bone computed tomography scan showed a large irregularly enhancing isodense mass lesion measuring 87*66 mm in the right external auditory canal, the right mastoid process, and extending to the right back parapharyngeal space with unclear border (Figure 3). Fortunately, abdominal, thoracic, and pelvic CT scanning did not identify any metastases. The child accepted BEP regimen chemotherapy for 6 cycles, consisting of bleomycin (6.4 mg; first day), VP-16 (42 mg; five days), DDP (8.4 mg; five days). After finishing the 6 cycles of chemotherapy, the tumor dramatically reduced to a small soft mass in the external auditory canal.
Figure 2.

The tumor before chemotherapy measured 87*66 mm.
Figure 3.
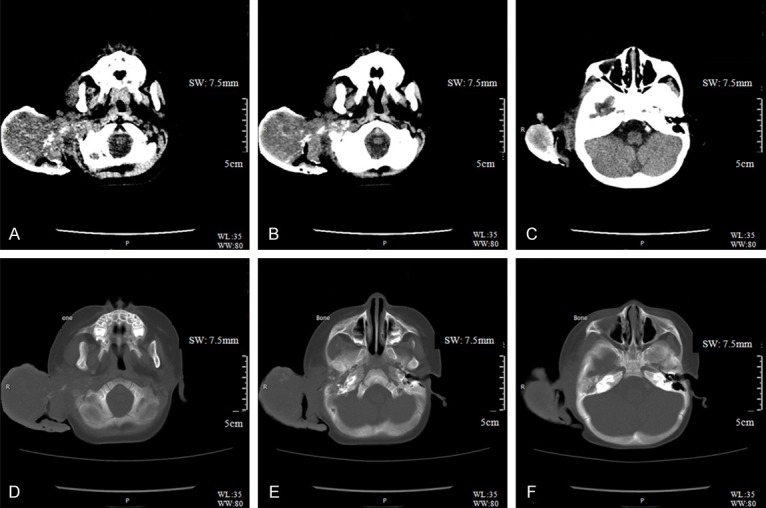
Temporal bone computed tomography scan showed a large irregularly enhancing isodense mass lesion measuring 87*66 mm in the right external auditory canal, the right mastoid process, and extending to the right back parapharyngeal space with unclear border. (Illustration: Diao Zehong, 14 months, M.0877639; Head examination; Sep/05/2015; Patient’s position: HFS; Exammination #: 201511050252; Series: 7.5 mm Stnd (A-C), 7.5 mm Stnd (D-F); GE MEDICAL SYSTEMS Optima; 100 KV, 9 mAs (A), 55 mAs (B-F), Sweep range: 320.00 mm; 100% pixel; Orginal resolution).
The patient presented to our hospital for advanced therapy. Temporal bone computed tomography scan revealed there still remained a soft mass in the right external auditory canal. The patient underwent a total resection: (1) The shape of the mass was irregular and the texture of the mass was harder than the temporal bone. (2) The tumor with a wide base of anterior, superior and posterior bone wall of external acoustic meatus. Otherwise, there was not an obvious boundary between them. The peripheral blood supply was not abundant. (3) Margins of resection, lymph node, the mass were deemed free of tumor.
Six months after the surgery, temporal bone computed tomography scan showed no mass in both the right middle ear and external auditory canal (Figure 4). The patient was still alive during the 13 months follow up period.
Figure 4.

Temporal bone computed tomography scan showed no mass in both the right middle ear and external auditory canal.
Discussion
Yolk sac tumors of the ear are rare and predominantly occur in early-childhood and pediatric patients. English literature from PubMed was surveyed to found the cases with yolk sac tumor of the ear. There were only 10 cases including our current case have been reported [11-19] (Table 1).
Table 1.
Report of cases of yolk sac tumor of the ear
| No. | Sex | Age (months) | Position | Serum α-feto protein level | Treatment (months) | Follow up | References |
|---|---|---|---|---|---|---|---|
| 1 | Female | 11 | Left external auditory canal | Elevated | Partial resection | 15 m, alive | [14] |
| Chemotherapy | |||||||
| 2 | Female | 21 | Left temporal bone | Elevated | Surgical resection | 16 m, alive | [15] |
| Chemotherapy | |||||||
| 3 | Female | 8 | Left external auditory canal | Elevated | Surgical resection | 13 m, alive | [16] |
| Chemotherapy | |||||||
| 4 | Female | 26 | Left external auditory canal | Elevated | Surgical removeal | 3 m, dead | [17] |
| 5 | Female | 18 | Left temporal bone | Elevated | Surgical resection | 36 m, alive | [18] |
| Chemotherapy | |||||||
| 6 | Male | 60 | Left external auditory canal | Elevated | Surgical resection | - | [16] |
| Chemotherapy | |||||||
| 7 | Female | 24 | Left postauricular region | Elevated | Surgical resection | 9 m, alive | [13] |
| 8 | Male | 30 | Left temporal bone | Elevated | Surgical resection | 9 m, alive | [12] |
| Chemotherapy | |||||||
| 9 | Male | 9 | Right external auditory canal | Elevated | Partical resection | 3 m, alive | [11] |
| 10 | Male | 18 | Right external auditory canal | Elevated | Surgical resection | 13 m, alive | Our case |
| Chemotherapy |
Yolk sac tumors often arise in gonadal sites such as ovary and tetis. Yolk sac tumors of the extra-gonadal region are reported in 20% of the cases. The exact etiology of the extra-gonadal germ cell tumors is still not well understood. Filho provided 4 hypothesis: (1) Detachment of germ cell during migration from the vitelline sac to gonadal crest during embryogenesis and their subsequent malignant transformation. (2) Germ cells present in extragonadal tissues. (3) Pluripotent cells that escape from the influence of primary development. (4) The tumors have a genetic origin arising through somatic cells or germ cell mitoses [20,21].
Yolk sac tumors, also known as endodermal sinus tumors, account for 3% of all childhood malignant tumors. Only 5% of germ cell tumors are found in the head and neck region (except for the central nervous system). There are a few cases reported in the head and neck including ear [11], nasal cavity and sinus [20,21], nasopharynx [22], orbit [23], parotid gland [24], and submandibular gland [25]. According to previous studies, yolk sac tumor of the head and neck show a highly aggressive behavior which might be attributed to the difficulty of tumor approach and excision. The poor prognosis is related to incomplete resection and anterior skull base involvement. Therefore, what should we do to monitor the recurrence and metastasis status of extra-gonadal and gonadal yolk sac tumors?
The diagnosis of yolk sac tumors mainly depends on the histological findings and serum biomarkers. Both the yolk sac tumor derived from gonad and extra-gonadal regions have similar characteristics, such as specific growth patterns and AFP immunoreactivity. Yolk sac tumor cells display vacuolated cytoplasm, a single large nucleolus, and some small eosinophilic hyaline globules. The tumor cells commonly forma a meshwork of microcystic, labyrinthine loose, eosinophilic, reticular stroma [26]. In addition, almost all the patients with yolk sac tumors are reported with serum elevated AFP level. There are different patterns under the microscopy, such as pseudopapillary, polyvesicular, glandular, hepatoid, and solid patterns [27,28]. In our case, we observed poly-vesicular patterns and Schiller-Duval body which has a characteristic pseudopapillary pattern.
Conclusion
Current therapies for yolk sac tumors are chemotherapy and surgical resection. Extra-gonadal yolk sac tumors have a strong relationship to poor prognosis, owing to the tumor position and total resection of the tumor. However, all the reported cases in the literature were still alive during the follow-up period. In our case, the child received chemotherapy and subsequent surgical resection, and was alive at the time of this writing. Therefore, we can closely test the serum level of AFP to monitor the status of yolk sac tumors.
Acknowledgements
The research was supported by National Natural Science Foundation of China (81700908), Natural Science Foundation of Guangdong Province-free application (2015A030313094) and Natural Science Foundation of Guangdong Province (2016A030310148).
Disclosure of conflict of interest
None.
References
- 1.Mukasa A, Yanagisawa S, Saito K, Tanaka S, Takai K, Shibahara J, Ikegami M, Nakao Y, Takeshita K, Matsutani M, Saito N. Successful treatment of mixed yolk sac tumor and mature teratoma in the spinal cord: case report. J Neurosurg Spine. 2017;26:319–324. doi: 10.3171/2016.8.SPINE16465. [DOI] [PubMed] [Google Scholar]
- 2.Suma TL, Ramanathan S, Padma M, Appaji L, Suma MN. A case of urachal yolk sac tumor with spontaneous rupture in a child. J Pediatr Hematol Oncol. 2017;39:e82–e84. doi: 10.1097/MPH.0000000000000615. [DOI] [PubMed] [Google Scholar]
- 3.van den Akker M, Vervloessem D, Huybrechs A, Declercq S, van der Werff Ten Bosch J. Yolk sac tumor in the abdominal wall of an 18-month-old girl: a case report. J Med Case Rep. 2017;11:47. doi: 10.1186/s13256-017-1216-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hirakawa H, Nakashima C, Nakamura T, Masuda M, Funakoshi T, Nakagawa S, Horimatsu T, Matsubara K, Muto M, Kimura S, Sueoka-Aragane N. Chemotherapy for primary mediastinal yolk sac tumor in a patient undergoing chronic hemodialysis: a case report. J Med Case Rep. 2017;11:43. doi: 10.1186/s13256-017-1213-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fang X, Du W, Wang Q, Zhao X. Endoscopic surgery combining chemotherapy for vaginal yolk-sac tumor: a case report. Eur J Gynaecol Oncol. 2015;36:335–338. [PubMed] [Google Scholar]
- 6.Li B, Jiang Q, Zhang S, Zhou Y, Zhang QF, OuYang L. Primary yolk sac tumor of the gluteus: a case report and literature review. Onco Targets Ther. 2016;9:4715–4719. doi: 10.2147/OTT.S106924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shenoy AS, Desai HM, Tyagi DK, Savant HV, Kavishwar VS, Balasubramaniam M. Primary yolk sac tumor of the cerebellar vermis: a case report. Indian J Pathol Microbiol. 2014;57:278–280. doi: 10.4103/0377-4929.134711. [DOI] [PubMed] [Google Scholar]
- 8.Nakamura T, Kanamori M, Sonoda Y, Watanabe M, Kumabe T, Tominaga T. [Primary yolk sac tumor in the cerebellar vermis. Case report] . No Shinkei Geka. 2009;37:173–177. [PubMed] [Google Scholar]
- 9.Reznichenko AA, Klingbeil LR, Shah SA. Giant primary yolk sac tumor of the liver. J Gastrointest Surg. 2016;20:1669–1670. doi: 10.1007/s11605-016-3123-1. [DOI] [PubMed] [Google Scholar]
- 10.Roy M, Agarwal S, Gupta A, Bakhshi S, Bhalla AS. Extragonadal yolk sac tumor of the head and neck region: a report of two cases. J Cancer Res Ther. 2015;11:1000–1002. doi: 10.4103/0973-1482.157305. [DOI] [PubMed] [Google Scholar]
- 11.Shi H, Tang Q, Zhen T, Li H, Zhang F, Han A. Yolk sac tumor of the external auditory canal: a case report and literature review. Int J Clin Exp Pathol. 2015;8:15001–15006. [PMC free article] [PubMed] [Google Scholar]
- 12.Rozbahany NA, Hasanzadazar M, Latifi H, Mohammadi A, Ilkhanizadeh B, Ghasemi-Rad M. Yolk-sac tumor of the postauricular region: case report and review of the literature. J Oral Maxillofac Surg. 2012;70:1891–1895. doi: 10.1016/j.joms.2011.08.009. [DOI] [PubMed] [Google Scholar]
- 13.Kaveti V, Sanjay R, Ganeshula S. Yolk sac tumor of the ear: uncommon presentation of a rare tumor. J. Clin. Oncol. 2010;28:e349–350. doi: 10.1200/JCO.2009.25.7337. [DOI] [PubMed] [Google Scholar]
- 14.Stanley RJ, Scheithauer BW, Thompson EI, Kispert DB, Weiland LH, Pearson BW. Endodermal sinus tumor (yolk sac tumor) of the ear. Arch Otolaryngol Head Neck Surg. 1987;113:200–203. doi: 10.1001/archotol.1987.01860020092020. [DOI] [PubMed] [Google Scholar]
- 15.Kebudi R, Ayan I, Darendeliler E, Agaoglu L, Kinay M, Olgac V, Bilge N. Non-midline endodermal sinus tumor in the head and neck region: a case report. Med Pediatr Oncol. 1993;21:685–689. doi: 10.1002/mpo.2950210915. [DOI] [PubMed] [Google Scholar]
- 16.Fukunaga M, Miyazawa Y, Harada T, Ushigome S, Ishikawa E. Yolk sac tumour of the ear. Histopathology. 1995;27:563–567. doi: 10.1111/j.1365-2559.1995.tb00328.x. [DOI] [PubMed] [Google Scholar]
- 17.Choufani G, Saussez S, Detemmerman D, Salmon I, Tainmont J, Louryan S, Remmelink M, Hassid S. Yolk sac tumor of the ear in a child. Am J Otol. 1998;19:298–300. [PubMed] [Google Scholar]
- 18.Frank TC, Anand VK, Subramony C. Yolk sac tumor of the temporal bone: report of a case. Ear Nose Throat J. 2000;79:183, 187–188, 191–192 passim. [PubMed] [Google Scholar]
- 19.Narula V, Meher R, Rana K, Sura JH, Nigam J, Tandon S, Sharma D. Extragonadal primary yolk sac tumour of temporal bone. Int J Pediatr Otorhinolaryngol. 2014;78:1416–1418. doi: 10.1016/j.ijporl.2014.06.016. [DOI] [PubMed] [Google Scholar]
- 20.Filho BC, McHugh JB, Carrau RL, Kassam AB. Yolk sac tumor in the nasal cavity. Am J Otolaryngol. 2008;29:250–254. doi: 10.1016/j.amjoto.2007.09.001. [DOI] [PubMed] [Google Scholar]
- 21.Chuang HC, Kang CJ, Lee LY. Sinonasal pure yolk sac tumor: a case report and literature review. Fetal Pediatr Pathol. 2014;33:127–134. doi: 10.3109/15513815.2013.839013. [DOI] [PubMed] [Google Scholar]
- 22.Arumugam D, Thandavarayan P, Chidambaram L, Boj S, Marudasalam S. Primary nasopharngeal yolk sac tumor: a case report. J Clin Diagn Res. 2016;10:ED06–07. doi: 10.7860/JCDR/2016/17620.7760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ahmad Z, Khurshid A, Qureshi A. Primary orbital yolk sac tumour in a 14-year-old girl. BMJ Case Rep. 2009:2009. doi: 10.1136/bcr.04.2009.1821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sredni ST, da Cunha IW, de Carvalho Filho NP, Magrin J, Pinto CA, Lopes LF. Endodermal sinus tumor of the parotid gland in a child. Pediatr Dev Pathol. 2004;7:77–80. doi: 10.1007/s10024-003-4048-8. [DOI] [PubMed] [Google Scholar]
- 25.Tsuji T, Nagai N. Production of alpha-fetoprotein by human submandibular gland. Int J Dev Biol. 1993;37:497–498. [PubMed] [Google Scholar]
- 26.Nogales-Fernandez F, Silverberg SG, Bloustein PA, Martinez-Hernandez A, Pierce GB. Yolk sac carcinoma (endodermal sinus tumor): ultrastructure and histogenesis of gonadal and extragonadal tumors in comparison with normal human yolk sac. Cancer. 1977;39:1462–1474. doi: 10.1002/1097-0142(197704)39:4<1462::aid-cncr2820390418>3.0.co;2-4. [DOI] [PubMed] [Google Scholar]
- 27.Dehner LP. Gonadal and extragonadal germ cell neoplasia of childhood. Hum Pathol. 1983;14:493–511. doi: 10.1016/s0046-8177(83)80004-5. [DOI] [PubMed] [Google Scholar]
- 28.Bao J, Ohlemiller KK. Age-related loss of spiral ganglion neurons. Hear Res. 2010;264:93–97. doi: 10.1016/j.heares.2009.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]