

Abstract
Purpose:
Nonsuicidal self-injury (NSSI) is associated with increased risk of suicide attempts. Theories of NSSI assert interpersonal stress as a common risk factor for, and perhaps consequence of, NSSI. Prior research has not examined reciprocal associations between chronic interpersonal stress and NSSI. This study used a multiwave, prospective design to address this gap in a sample of adolescent girls, a group with elevated risk for both chronic interpersonal stress and NSSI. Pubertal development was examined as a moderator of the reciprocal associations.
Methods:
Adolescent girls (N = 220; ages 12–16, M age = 14.69 years) at heightened risk for NSSI completed a baseline assessment and follow-up assessments over 18 months, divided into two 9-month epochs (Time 1 and 2). Pubertal development was assessed via self- and parent-report. Chronic interpersonal stress was assessed using a semistructured interview at the end of each time period. NSSI was measured using a semistructured clinical interview every 3 months within both time periods to enhance accurate reporting.
Results:
Path models revealed that chronic romantic stress during Time 1, but not peer or parent–child stress, predicted NSSI during Time 2 among girls with more advanced pubertal development. Moreover, NSSI during Time 1 predicted higher levels of chronic romantic and parent–child stress during Time 2.
Conclusions:
Results revealed a reciprocal relationship between chronic romantic stress and engagement in NSSI. Further, this association may be best understood in the context of pubertal development.
Keywords: NSSI, Self-injury, Romantic stress, Adolescent dating, Pubertal development
Nonsuicidal self-injury (NSSI) is the direct, intentional harm to one’s own body performed without the intent to die. Meta-analytic work indicates that pooled lifetime prevalence estimates are around 17% for nonclinical samples and substantially higher (40%–80%) among clinical samples of adolescents [1–3]. Adolescent girls report higher rates of NSSI than boys [4], and NSSI prospectively predicts suicide attempts [5]. A recent meta-analysis reveals few prospective, multiwave studies of commonly purported risk factors for NSSI, such as interpersonal stress [4]. The present study addresses this gap by examining the reciprocal association between NSSI and chronic interpersonal stress over 18 months.
NSSI is purported to reduce emotional distress triggered by episodic (e.g., fight with friend) or chronic (e.g., low social support) interpersonal stress [6,7]. However, this association is unlikely to be unidirectional. From a developmental psychopathology perspective, youth not only react to environmental stressors, but engage in behavior that contributes to their social environment [8]. Whereas interpersonal stress may contribute to NSSI engagement, NSSI also may lead to subsequent interpersonal stress. Surprisingly, the reciprocal association between NSSI and interpersonal stressors has not been examined, perhaps because relatively few longitudinal studies of NSSI and its psychosocial correlates exist.
Prior work suggests that chronic and episodic interpersonal stress is associated with NSSI, perhaps especially for girls. Indeed, compared to boys, girls experience more internalizing reactions, such as rumination, subsequent to interpersonal stress [9]. Past cross-sectional work suggests that low social support [10] and peer victimization [11,12] are associated with NSSI. Longitudinal studies suggest that negative life events [13] and harsh parental discipline [14] predict NSSI. Further, both peer victimization and low friend support distinguished youth drawn from the community with high versus moderate and low-risk trajectories of NSSI over 2 years [15]. Finally, low perceived parent support longitudinally predicts NSSI onset [16] and engagement [14]. Thus, existing evidence supports the link between peer and parent-child stress and NSSI.
Fewer studies have examined the role of chronic romantic relationship stress in adolescent NSSI. This is surprising given that nearly 70% of all US adolescents report a romantic relationship by age 17 [17]. These relationships are associated with more distress among girls more than boys [18], which is linked with mental health problems during adolescence [19]. A recent cross-sectional study demonstrated that high levels of chronic peer and romantic stress were associated with presence of NSSI, but only among those with a genetic vulnerability (short allele 5-HTTLPR gene) [20]. Among adults, victimization [21] and lack of support [22] from romantic partners are associated with NSSI.
Considerable research supports a reciprocal association between psychopathology and interpersonal stress [23]. From a stress-generation perspective, an individual with depression may engage in behaviors (e.g., excessive reassurance seeking) that inadvertently cause additional interpersonal stress [24]. Similarly, an adolescent’s engagement in NSSI may be viewed unfavorably by relationship partners who then may distance themselves from the adolescent. Initial evidence from a 6-month prospective study suggests that baseline NSSI predicts stressful interpersonal life events for late adolescent girls [25]. However, Burke and colleagues did not examine the reciprocal association between interpersonal stress and NSSI [5]. From this study it remains unclear if NSSI predicts interpersonal stress over and above previous interpersonal stress.
The reciprocal link between interpersonal stress and NSSI may be especially relevant in the context of advanced pubertal development. Brain development during puberty increases social sensitivity [25,26]. Simultaneously, the development of reward circuitry outpaces critical frontal control regions resulting in a period of increased risk taking [27], exacerbated by interpersonal stress [28]. Thus, adolescents who are advanced in pubertal development may be biologically primed to engage in risky behaviors, such as NSSI, as a result of chronic interpersonal stress. Together, prior theory and research suggests that the transactional relationship between NSSI and chronic interpersonal stressors may be moderated by pubertal development.
This study examined multiple domains of girls’ chronic interpersonal stress, including stress within peer, family, and romantic relationships, which has been remarkably understudied with respect to NSSI. Addressing limitations in prior work that has predominantly relied on checklist-style stress assessments or perceptions of stress, measures of chronic interpersonal stress were obtained from objectively coded responses to semistructured interviews. To facilitate accurate reporting of NSSI over two 9-month periods, participants completed a semistructured interview of self-injurious thoughts and behaviors every 3 months. It was hypothesized that NSSI and interpersonal stress would be associated reciprocally and that these associations would be strongest among girls with more advanced pubertal development. Given the importance of differentiation among self-injury constructs, and evidence that NSSI [5] and interpersonal stress [29] are associated with suicidal self-injurious thoughts and behaviors, we ran sensitivity models with suicidal ideation as a predictor and covariate to explore the specificity of our findings.
Method
Participants
Participants were 220 females between 12 and 16 years old (M age = 14.69 years, SD = 1.37), with at least one mental health concern (e.g., affective, anxiety, or disruptive behavior disorders or substance use) in the 2 years prior to the study. Participants were born mostly in the United States (92%); 24% identified as African American, 64% as Caucasian, 10% as mixed or other, 1% as Asian American, and 1% as Latino/a. Six percent of the sample identified as being Hispanic.
Procedures
Data for the present study were collected from 2010 to 2015 as part of an 18-month longitudinal study examining the development of self-injurious thoughts and behaviors among youth [15] in a rural town in the southeastern US. Previously [30], we have focused on suicidal ideation and behavior. Here we focus on NSSI. Participants were recruited from a wide range of referral sources, including local inpatient units, outpatient facilities, local advertisements, and mass emails to university employees (~60% of eligible individuals enrolled in the study). Inclusion criteria were: female gender; 12–16 years old; caregiver (parent or legal guardian) willing to take part in the study. Exclusion criteria were: active psychosis or any developmental disorder.
At baseline, participants completed a battery of assessments lasting approximately 2 h. Youth were assessed at 3 (91% retained), 6 (88% retained), 9 (91% retained), 12 (84% retained), 15 (84% retained), and 18 (80% retained) months post-baseline. A trained research assistant administered a structured clinical interview at each time point to assess self-injurious thoughts and behaviors. At the 9- and 18-month follow-up assessments, a trained research assistant administered a semi-structured interview assessing interpersonal stress. Hereafter, we refer to the time between baseline and 9 months as Time 1 and the time between 9 and 18 months as Time 2. Missing data rates are presented in Table 1. All procedures were approved by the university human subjects board.
Table 1.
Bivariate correlations and descriptive statistics
| 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | |
|---|---|---|---|---|---|---|---|---|---|
| 1. Pubertal development – baseline | – | ||||||||
| 2. Peer stress – Time 1 | .13 | – | |||||||
| 3. Peer stress – Time 2 | .08 | .55** | – | ||||||
| 4. Parent–child stress – Time 1 | .17* | .30** | .29** | – | |||||
| 5. Parent–child stress – Time 2 | .15 | .19* | .36** | .56** | – | ||||
| 6. Romantic stress – Time 1 | .07 | .40** | .26** | .25** | .14 | – | |||
| 7. Romantic stress – Time 2 | .19* | .17* | .32** | .05 | .28** | .36** | – | ||
| 8. NSSI – Time 1 | .16* | .22* | .16* | .15 | .24** | .03 | .18* | – | |
| 9. NSSI – Time 2 | .11 | .08 | .15 | .08 | .14 | .01 | .16 | .43** | – |
| N | 220 | 163 | 151 | 163 | 151 | 163 | 150 | 212 | 161 |
| Mean | 3.38 | 2.55 | 2.43 | 2.73 | 2.49 | 2.36 | 2.40 | 2.21 | 1.05 |
| Standard deviation | .46 | 1.15 | 1.15 | 1.13 | 1.10 | .87 | .87 | 9.73 | 2.69 |
| Range | 1.70–4.00 | 1–5 | 1–5 | 1–5 | 1–5 | 1–5 | 1–5 | 0–103 | 0–28 |
| Percentage missing | 0% | 25.9% | 31.4% | 25.9% | 31.4% | 25.9% | 31.8% | 3.6% | 26.8% |
Note. NSSI: nonsuicidal self-injury.
p < .05.
p < .01.
Measures
Non-suicidal self-injury and suicidal ideation.
NSSI and suicidal ideation were assessed with the Self-Injurious Thoughts and Behaviors Interview (SITBI; [31]) completed with the adolescent at baseline and each follow-up assessment. The SITBI is a structured clinical interview designed to assess the presence or absence and frequency of suicidal ideation and NSSI. The current study focused on the frequency of NSSI (“How many times since the last follow-up did you purposefully hurt yourself without wanting to die?”). For the sensitivity analysis with suicidal ideation, we assessed the frequency (“How many days”), duration (“How long did they last”), and intensity (“How intense were the thoughts”) of suicidal thoughts. At each follow-up assessment, participants were asked these questions regarding the previous 3 months. We standardized the responses to each of these questions and combined responses into a severity of suicidal ideation index score. To match the time period covered by the stress assessment described below, we created a summed score across the 3-, 6-, and 9-month follow-ups and the 12-, 15-, and 18-month follow-ups (using censoring for missing data),1 resulting in two scores for each outcome (i.e., Time 1 and 2). We also included lifetime NSSI frequency as assessed at the baseline interview. The SITBI has strong convergent validity, inter-rater reliability (K =.90), and test–retest reliability (K = .70) [31].
Chronic interpersonal stress.
The Youth Life Stress Interview [32] was conducted with youth to assess their exposure to chronic life stress during Time 1 and 2. This semistructured interview gathers information about the nature and intensity of chronic and episodic stress experienced by youth. This study focused on chronic stress in peer, parent–child, and romantic relationship domains.
Trained interviewers asked standardized questions about stressful aspects of peer (e.g., difficulty making/retaining friends, social exclusion, isolation, arguments, fights, exposure to relational aggression, and poor-quality friendships), parent–child (e.g., arguments, low trust, and lack of availability), and romantic relationships (e.g., romantic rejection, getting asked out less than peers, having fewer romantic relationships than peers, arguments). In addition to a series of structured prompts, interviewers asked follow-up questions to gain a complete, detailed picture of each youth’s degree of chronic stress in each domain.
Interviewers presented narrative information to a team of independent, trained coders who had no knowledge of the youth’s history of NSSI or SI or the youth’s subjective response to the stress (e.g., felt sad). Coders engaged in group discussions, guided by codebooks with exemplars, until they all arrived at a consensus rating for stress severity, based on the youth’s report to the interviewer. Each chronic stress domain over Time 1 and 2 was rated on a 5-point scale: 1 = no stress, 2 = mild stress, 3 = isolated stress, 4 = serious stress, 5 = severe stress. For each interpersonal stress domain, higher chronic stress ratings reflect higher levels of stressful conditions (e.g., significant fights/arguments) and lower levels of positive conditions (e.g., lack of emotional support, fewer positive shared activities). Thus, adolescents with differing profiles (e. g., an adolescent with frequent or intense arguments with romantic partner and an adolescent with frequent unreciprocated romantic interest) may receive a similar score given that overt conflict and social isolation/low-quality relationships may be similarly stressful. To determine reliability, 41 interview narratives were presented to two teams of coders, who gave independent ratings (single measures ICC = .93, average measures ICC = .97).
Pubertal development.
Using the Pubertal Development Scale [33] administered at baseline, girls and their mother rated the adolescent’s level of pubertal development on various indicators [body growth spurt, pubic hair, changes in skin (pimples), breast growth, and start of menstruation] using a 4-point scale, “not yet started” (0), “barely started” (1), “definitely underway” (2), “seems completed” (3). Mean scores were computed for girls (alpha = .68) and mothers (alpha = .70) separately (r = .52, p < .001), then averaged together to reflect a composite pubertal development scale.
Data analysis
Descriptive statistics and bivariate correlations were conducted with the SPSS statistical package (IBM SPSS Statistics, version 24.0). Path analysis models were conducted with AMOS (AMOS Statistics, version 24.0). To account for missing data, model testing was conducted with full maximum likelihood estimation. Results from Little’s [34] missing completely at random test, X2 (44) = 44.36; p = .46, provided evidence that data were missing at random. Further, attrition analyses suggested that individuals missing data at Time 2 did not significantly differ on Time 1 NSSI, t(91) = −1.92, p =. 06,1 or interpersonal stressors, t(161) = .58, p = .57. Individuals missing data at Time 1 did not significantly differ on Time 2 NSSI t (159) = .66, p = .51 or interpersonal stressors, t(17) = −1.89, p = .08.2
First, we examined an initial model that included concurrent relationships among NSSI, peer stress, parent-child stress, and romantic stress at Time 1 and each of these variables predicting the same variables at Time 2. Additionally, this initial model included pubertal development (measured at baseline) and interaction terms (N = 4, pubertal development × each form of interpersonal stress predicting NSSI at Time 2; and pubertal development × NSSI predicting each form of interpersonal stress at Time 2). This allowed us to examine (a) the reciprocal associations between NSSI and interpersonal stress and (b) whether puberty moderates these reciprocal associations. Second, based on results from our initial model, we tested a more parsimonious model including only significant predictors (Figure 1). This model also included baseline NSSI predicting both NSSI during Time 1 and 2. Finally, we tested the sensitivity of our findings by testing two alternative models. One sensitivity model replaced NSSI with suicidal ideation. A second model included suicidal ideation along with NSSI. Following accepted guidelines [35], predictors were mean centered prior to forming their interaction terms. We probed significant interactions in the reduced model using simple slopes analyses.
Figure 1.
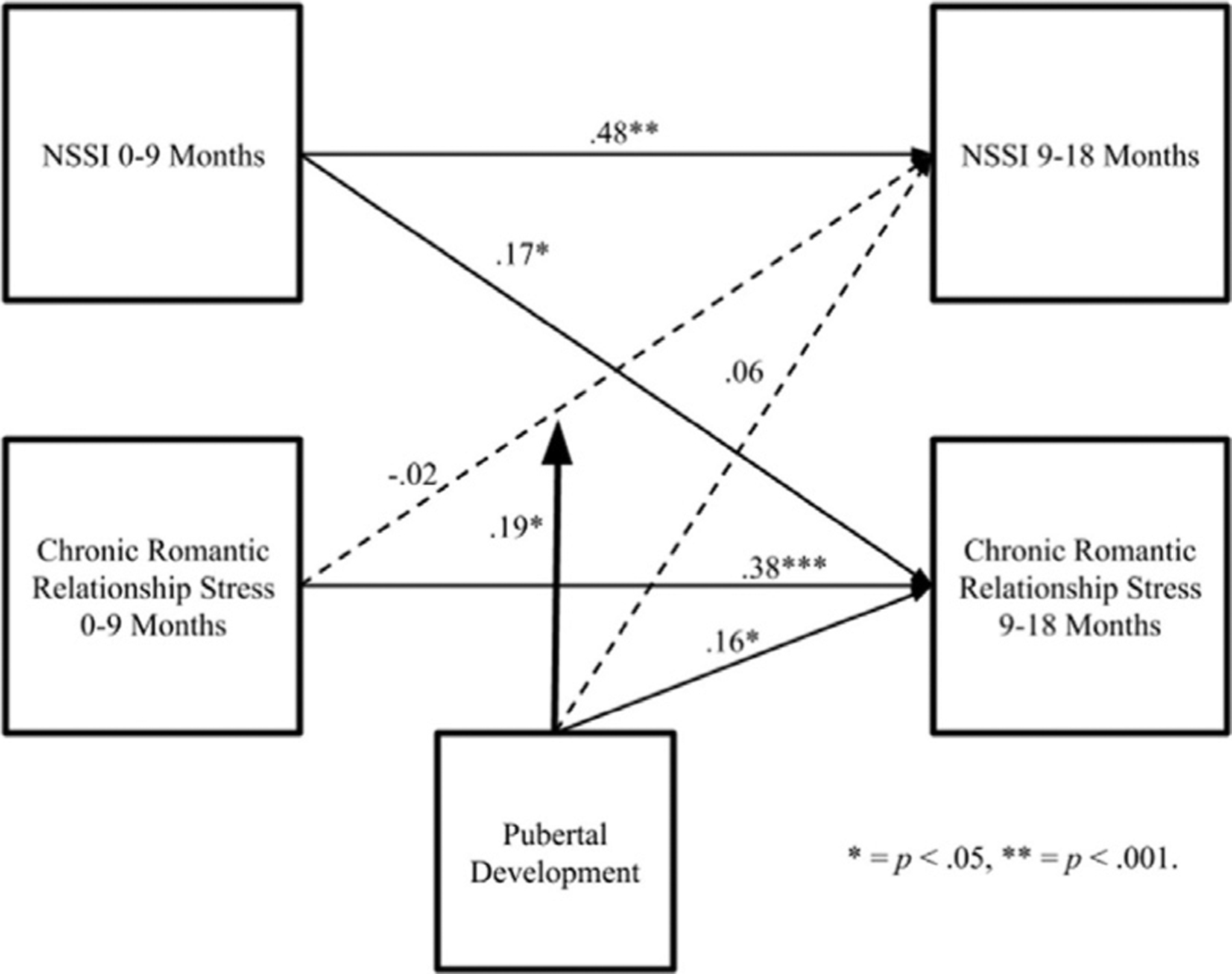
NSSI, chronic romantic relationship stress, and pubertal development. Concurrent relationships between NSSI and chronic romantic relationship stress were allowed to covary. Path coefficients are standardized. Dashed lines are nonsignificant paths.
Results
Descriptive statistics and bivariate associations
Descriptive statistics are presented in Table 1. All variables were normally distributed except for frequency of NSSI, which was log transformed for use in all path models to reduce its significant skew and kurtosis. Each Time 1 and 2 variable was significantly, positively correlated with itself. Pubertal development was associated with higher Time 1 parent-child stress and NSSI and higher Time 2 romantic stress. Time 1 NSSI was significantly associated with higher Time 1 and 2 peer stress and higher Time 2 parent-t–child and romantic stress.
Full model
The initial model demonstrated adequate fit, X2(25) = 41.16, p = .02; CFI = .96; RMSEA = .05,90% CI [.02, .08]. In this initial model, the cross-lagged effects from both Time 1 parent-child, β = .04, p = .66, and peer stress, β = .03, p = .73, on Time 2 NSSI were nonsignificant (see Supplemental Figure 1). Further, there were no significant interactions between either Time 1 parent-child, β = −.06, p = .45, or peer stress, β = .02, p = .69, and pubertal development predicting Time 2 NSSI or between Time 1 NSSI and pubertal development predicting Time 2 interpersonal stressors (see Supplemental Figure 1). The cross-lagged paths from Time 1 NSSI were significantly associated with greater Time 2 romantic stress, β=.16, p < .05, and parent–child stress, β = .15, p < .05, but not peer stress, β = .03, p = .66. The interaction between pubertal development and Time 1 romantic stress was significantly associated with Time 2 NSSI, β = .18, p < .05 (Supplementary Figure 1). We retained romantic stress in the reduced model.
Reduced model
The reduced model (Figure 1) provided excellent fit to the data, X2(4) = 3.35, p = .50; CFI = 1.00; RMSEA = .00, 90% CI [.00, .09]. As shown in Figure 1, there was significant stability in both NSSI, β = .48, p < .001, and romantic stress, β = .38, p < .001. Higher pubertal status at baseline did not directly predict Time 2 NSSI, β = .06, p = .39, but was associated with greater Time 2 romantic stress, β = .16, p < .05.3 Consistent with hypotheses, there was a significant interaction between Time 1 romantic stress and pubertal development predicting Time 2 NSSI, b = .19, p < .05. The simple slopes analysis revealed that Time 1 romantic stress predicted higher Time 2 NSSI only for girls more advanced in pubertal development, slope = .07, p = .045. Further, Time 1 romantic stress predicted significantly lower Time 2 NSSI for girls less advanced in pubertal development, slope = −.08, p = .01 (see Figure 2). Consistent with hypotheses, the cross-lagged relationship between Time 1 NSSI and greater Time 2 romantic stress was significant, β = .17, p < .05.4 However, this relationship was not moderated by puberty.
Figure 2.
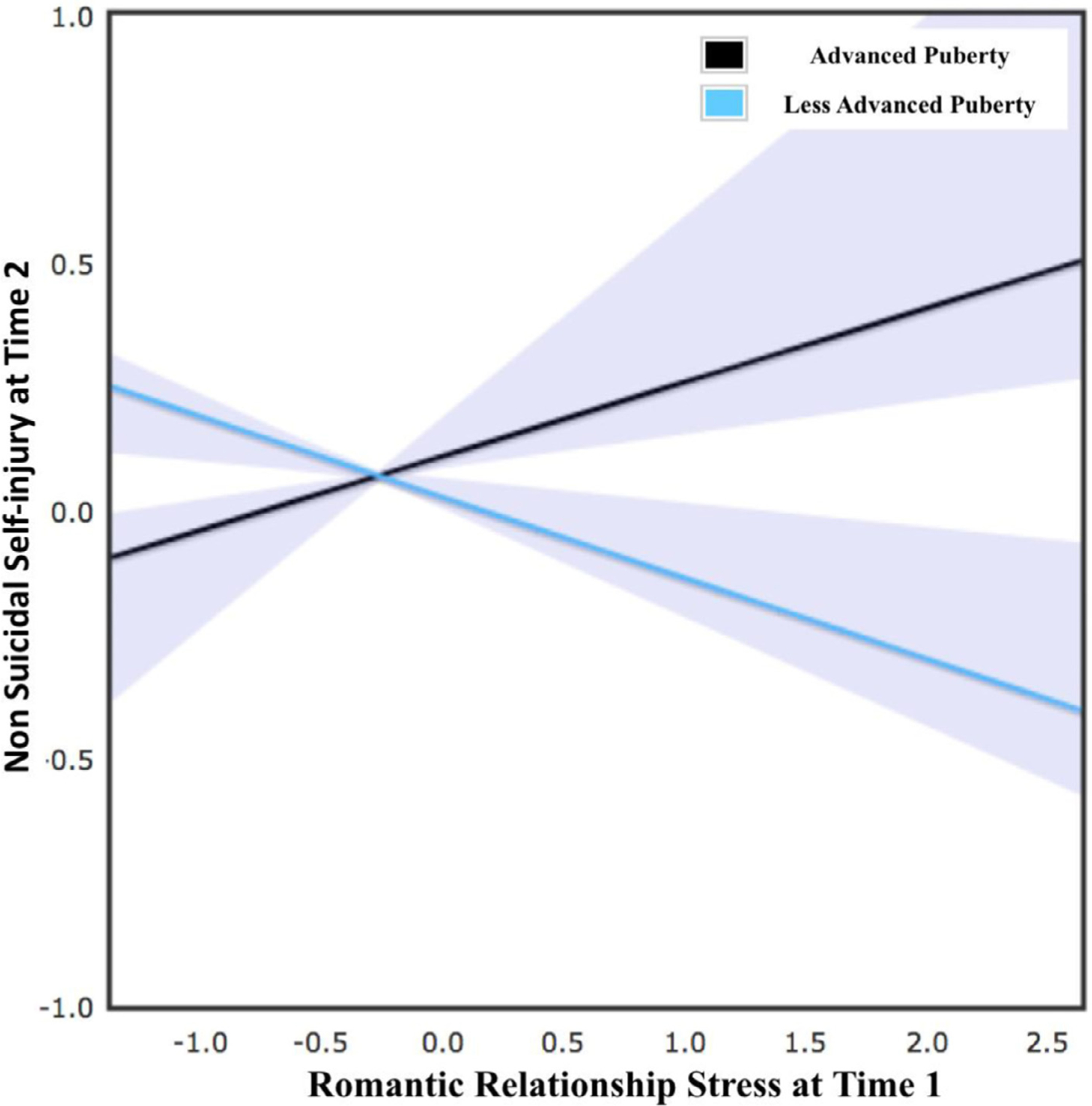
Effect of chronic romantic relationship stress from Time 1 on risk for nonsuicidal self-injury at Time 2 by level of pubertal development. Higher romantic relationship stress at Time 1 was associated with higher NSSI at Time 2 for those more advanced in pubertal development, b = .07 (SE = .04), p = .045. Higher romantic relationship stress at Time 1 was associated with lower NSSI at Time 2 for those less advanced in pubertal development, b = −.08(SE = .04), p = .01.
Sensitivity analyses/alternative model
Sensitivity models were examined to determine whether results were relevant to self-injury more generally, or specifically to NSSI by examining suicide ideation in two ways. The first sensitivity model that replaced Time 1 and 2 NSSI with Time 1 and 2 suicidal ideation demonstrated excellent fit, X2(3) = 3.77, p = .29; CFI = .99; RMSEA = .03, 90% CI [.00, .06]. However, there were no significant cross-lagged effects of Time 1 suicidal ideation predicting Time 2 romantic stress, β = .12, p = .10, or Time 1 romantic stress predicting Time 2 suicidal ideation, β = −.004, p = .95. Further, the interaction between Time 1 romantic stress and pubertal development predicting Time 2 suicidal ideation was nonsignificant, β = .08, p = .28. The second sensitivity model that included suicidal ideation as a covariate (in addition to NSSI) demonstrated acceptable fit, X2(12) = 21.94, p = .01; CFI = .95; RMSEA = .06, 90% CI [.01, .10]. Again, there were no significant cross-lagged effects of Time 1 suicidal ideation predicting Time 2 romantic stress, β = .08, p = .40, or Time 1 romantic stress predicting Time 2 suicidal ideation, β = – .005, p = .94. Further, the interaction between Time 1 romantic stress and pubertal development predicting Time 2 suicidal ideation was nonsignificant, β = .08, p = .24.
Discussion
The purpose of this preliminary study was to examine the reciprocal association between interpersonal stressors and NSSI in a multi-wave study of adolescent girls. Results partially supported our hypotheses and suggest that NSSI is associated prospectively with romantic and parent–child stress. Further, romantic relationship stress was associated with later NSSI among girls more advanced in pubertal development.
Romantic stress was uniquely associated with risk for NSSI in the context of advanced pubertal development. Our initial model included all forms of interpersonal stress, but only romantic stress emerged as a significant predictor of NSSI. Previous studies with youth have rarely included chronic stress across multiple domains in the same model, and in particular, studies have neglected romantic stress as a predictor of NSSI. However, these results are consistent with findings from adult samples, which show significant associations between romantic stress and NSSI [36]. Although we found a concurrent correlation between Time 1 peer stress and NSSI, it is surprising that peer and parent–child stress did not independently predict Time 2 NSSI. In the current analyses, Time 1 and 2 each included information collapsed over a 9-month period. It is possible that a more fine-grained assessment schedule of both NSSI and stress would reveal stronger associations between peer and parent–child stress and NSSI. Given research documenting significant associations between peer and parent–child stress and NSSI [15], our findings should be replicated in future studies.
Our findings suggest that the contribution of romantic stress to NSSI is best understood in the context of pubertal development. Specifically, romantic stress predicted higher subsequent NSSI among girls with more advanced pubertal development but lower subsequent NSSI among girls with less advanced pubertal development. This finding can be understood in terms of a social-contextual model, which suggests that puberty amplifies the associations between stress and maladjustment [37]. For example, experiences of family stress and exposure to maternal depression more strongly predicted subsequent depression among youth with more advanced pubertal maturation [38]. It is also possible that more physically advanced girls are drawn into romantic relationships without adequate socioemotional skills, such as positive coping or cognitive reappraisal, to handle romantic stress [39]. Our results are consistent with these perspectives, suggesting an interplay between social contexts and physical vulnerabilities contribute risk for NSSI. This pattern highlights an exciting potential for future research to explore risk factors for NSSI within a dynamic, multilevel framework.
We also found that NSSI predicted subsequent stress in romantic and parent–child relationships. This finding is consistent with a recent study in which NSSI at baseline predicted stressful interpersonal life events across 6 months for adolescent females [25]. Research within a developmental psychopathology framework views the association between interpersonal stress and psychopathology as a transactional process, consistent with a recent cognitive neuroscience model of NSSI offered by Liu [40]. A portion of this model suggests that NSSI becomes fixed through operant conditioning [6,40] wherein NSSI temporarily relieves distress from romantic stress but contributes to future romantic stress and subsequent NSSI. Future research with a larger sample and more assessment waves would allow for in-depth exploration of the reciprocal effects of NSSI and interpersonal stress.
There are important clinical implications of our findings, which highlight that romantic stress is risky for girls with more advanced pubertal development, thus warranting careful assessment and monitoring in this group. Furthermore, helping youth find alternative, healthy coping skills rather than NSSI may have some beneficial downstream effects on subsequent interpersonal stress.
The strengths of this study include a rigorous assessment of interpersonal stress by an independent team of coders, clinical interviews, and the use of a longitudinal, multiwave design. Nevertheless, our findings should be replicated with studies addressing some limitations. First, our study assessed chronic interpersonal stress at two timepoints using a retrospective approach. Although this is a significant improvement upon self-report checklists, future work would benefit from more frequent assessments to counteract recall bias and to enable an examination of trajectories of stress over time. Although youth with incomplete data on the life stress interview at Time 2 did not significantly differ on Time 1 variables, 31.8% of the sample did not complete this time intensive interview at Time 2, suggesting that caution is needed in interpretation until results are replicated. Second, our assessment of pubertal development was limited to baseline. Repeated assessments of puberty would help identify specific periods of development that confer the greatest risk and would allow estimation of whether pubertal tempo serves as a potential risk or protective factor. Third, our sample included only females with increased clinical risk. It is unclear how our findings would generalize to males or a community-based sample.
Our findings encourage research that examines the reciprocal association between NSSI and interpersonal stress within the context of pubertal development. Romantic stress was associated with future NSSI among those more advanced in pubertal development, and NSSI was associated with increases in stress. Broadly, our results underscore the dynamic interplay between commonly purported risk factors for NSSI.
Supplementary Material
IMPLICATIONS AND CONTRIBUTION.
This study investigates the longitudinal, reciprocal relationship between chronic interpersonal stress and non-suicidal self-nonjury (NSSI). Results suggest that chronic romantic stress and engagement in NSSI may be most strongly related among those more advanced in pubertal development. Evidence shows that NSSI increases risk for romantic and parent–child stress.
Acknowledgement
This research was supported by grants from the National Institute of Mental Health (R01MH085505, R01MH107479, F32MH108238).
Footnotes
Supplementary Data
Supplementary data related to this article can be found at https://doi.org/0.1016/j.jadohealth.2018.06.033.
We reran our models including only individuals with complete SITBI data across all waves and obtained the same results.
Levene’s test indicated unequal variances (Time 1 NSSI, F =14.92, p < .001, and Time 2 interpersonal stressors, F =22.71, p < .001) resulting in adjusted degrees of freedom.
To test the robustness of this interaction, we bootstrapped this parameter estimate. Results from 1,000 bootstrap resamples suggests that the interaction effect remained significant, b = .16, p < .05,95% CI [.03—.27].
We also tested a main effects only model to ensure that the relationship between Time 1 NSSI and Time 2 romantic stress Time 2 remained significant without the interaction term present. The direct relationship was unchanged.
References
- [1].Swannell SV, Martin GE, Page A, et al. Prevalence of nonsuicidal self-injury in nonclinical samples: systematic review, meta-analysis and meta-regression. Suicide Life Threat Behav 2014;44:273–303. [DOI] [PubMed] [Google Scholar]
- [2].Adrian M, Zeman J, Erdley C, et al. Emotional dysregulation and interpersonal difficulties as risk factors for nonsuicidal self-injury in adolescent girls. J Abnorm Child Psychol 2011;39:389–400. [DOI] [PubMed] [Google Scholar]
- [3].DiClemente RJ, Ponton LE, Hartley D. Prevalence and correlates of cutting behavior: risk for HIV transmission. J Am Acad Child Adolesc Psychiatry 1991;30:735–9. [PubMed] [Google Scholar]
- [4].Fox KR, Franklin JC, Ribeiro JD, et al. Meta-analysis of risk factors for nonsuicidal self-injury. Clin Psychol Rev 2015;42:156–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Ribeiro JD, Franklin JC, Fox KR, et al. Self-injurious thoughts and behaviors as risk factors for future suicide ideation, attempts, and death: a meta-analysis of longitudinal studies. Psychol Med 2016;46:225–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Nock MK, Prinstein MJ. A functional approach to the assessment of self-muti-lative behavior. J Consult Clin Psychol 2004;72:885–90. [DOI] [PubMed] [Google Scholar]
- [7].Chapman AL, Gratz KL, Brown MZ. Solving the puzzle of deliberate self-harm: the experiential avoidance model. Behav Res Therapy 2006;44:371–94. [DOI] [PubMed] [Google Scholar]
- [8].Caldwell MS, Rudolph KD, Troop-Gordon W, et al. Reciprocal influences among relational self-views, social disengagement, and peer stress during early adolescence. Child Dev 2004;75:1140–54. [DOI] [PubMed] [Google Scholar]
- [9].Rose AJ, Rudolph KD. A review of sex differences in peer relationship processes: potential trade-offs for the emotional and behavioral development of girls and boys. Psychol Bull 2006;132:98–131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Muehlenkamp J, Brausch A, Quigley K, et al. Interpersonal features and functions of nonsuicidal self-injury. Suicide Life Threat Behav 2013;43:67–80. [DOI] [PubMed] [Google Scholar]
- [11].Giletta M, Scholte RHJ, Engels RCME, et al. Adolescent non-suicidal self-injury: a cross-national study of community samples from Italy, the Netherlands and the United States. Psychiatry Res 2012;197:66–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].van Geel M Goemans A, Vedder P. A meta-analysis on the relation between peer victimization and adolescent non-suicidal self-injury. Psychiatry Res 2015;230:364–8. [DOI] [PubMed] [Google Scholar]
- [13].Liu RT, Frazier EA, Cataldo AM, et al. Negative life events and non-suicidal self-injury in an adolescent inpatient sample. Arch Suicide Res 2014;18:251–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Keenan K, Hipwell AE, Stepp SD, et al. Testing an equifinality model of nonsuicidal self-injury among early adolescent girls. Dev Psychopathol 2014;26:851–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Giletta M, Prinstein MJ, ZR, et al. Trajectories ofsuicide ideation and nonsuicidal self-injury among adolescents in mainland China: peer predictors, joint development, and risk for suicide attempts. J Consult Clin Psychol 2015;83:265–79. [DOI] [PubMed] [Google Scholar]
- [16].Tatnell R, Kelada L, Hasking P, et al. Longitudinal analysis of adolescent NSSI: the role of intrapersonal and interpersonal factors. J Abnorm Child Psychol 2014;42:885–96. [DOI] [PubMed] [Google Scholar]
- [17].Collins WA, Welsh DP, Furman W. Adolescent romantic relationships. Annu Rev Psychol 2009;60:631–52. [DOI] [PubMed] [Google Scholar]
- [18].Hankin BL, Mermelstein R, Roesch L. Sex differences in adolescent depression: stress exposure and reactivity models. Child Dev 2007;78:279–95. [DOI] [PubMed] [Google Scholar]
- [19].La Greca AM, Harrison HM. Adolescent peer relations, friendships, and romantic relationships: do they predict social anxiety and depression? J Clin Child Adolesc Psychol 2005;34:49–61. [DOI] [PubMed] [Google Scholar]
- [20].Hankin BL, Barrocas AL, Young JF, et al. 5-HTTLPRxinterpersonal stress interaction and nonsuicidal self-injury in general community sample ofyouth. Psychiatry Res 2015;225:609–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Rizzo CJ, Esposito-Smythers C, Swenson L, et al. Dating violence victimization, dispositional aggression, and nonsuicidal self-injury among psychiatrically hospitalized male and female adolescents. Suicide Life Threat Behav 2014;44:338–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Turner BJ, Wakefield MA, Gratz KL, et al. Characterizing interpersonal difficulties among young adults who engage in nonsuicidal self-injury using a daily diary. Behav Therapy 2017;48:366–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Hammen C Generation of stress in the course of unipolar depression. J Abnorm Psychol 1991;100:555–61. [DOI] [PubMed] [Google Scholar]
- [24].Stroud CB, Sosoo EE, Wilson S. Rumination, excessive reassurance seeking, and stress generation among early adolescent girls. J. Early Adolesc 2018;38: 139–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Burke TA, Hamilton JL, Abramson LY, et al. Non-suicidal self-injury prospectively predicts interpersonal stressful life events and depressive symptoms among adolescent girls. Psychiatry Res 2015;228:416–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Somerville LH. Special issue on the teenage brain: sensitivity to social evaluation. Curr Dir Psychol Sci 2013;22:121–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Somerville LH, Jones RM, Casey BJ. A time of change: behavioral and neural correlates of adolescent sensitivity to appetitive and aversive environmental cues. Brain Cogn 2010;72:124–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Telzer EH, Miernicki ME, Rudolph KD. Chronic peer victimization heightens neural sensitivity to risktaking. Dev Psychopathol 2017:1–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Liu RT, Miller I. Life events and suicidal ideation and behavior: a systematic review. Clin Psychol Rev 2014;34:181–92. [DOI] [PubMed] [Google Scholar]
- [30].Miller AB, Eisenlohr-Moul T, Giletta M, et al. A within-person approach to risk for suicidal ideation and suicidal behavior: examining the roles of depression, stress, and abuse exposure. J Consult Clin Psychol 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Nock MK, Holmberg EB, Photos VI, et al. Self-injurious thoughts and behaviors interview: development, reliability, and validity in an adolescent sample. Psychol Assess 2007;19:309–17. [DOI] [PubMed] [Google Scholar]
- [32].Rudolph KD, Flynn M. Childhood adversity and youth depression: influence of gender and pubertal status. Dev Psychopathol 2007;19:497–521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Petersen AC. Adolescent development. Annu Rev Psychol 1988;39:583–607. [DOI] [PubMed] [Google Scholar]
- [34].Little RJA. A test of missing completely at random for multivariate data with missing values. J Am Stat Assoc 1988;83:1198–202. [Google Scholar]
- [35].Cohen J, Cohen P, West SG, et al. Applied multiple regression/correlation analysis for the behavioral sciences. 3rd ed Mahwah, NJ: Erlbaum; 2003. [Google Scholar]
- [36].Silva E, Machado BC, Moreira CS, et al. Romantic relationships and nonsuicidal self-injury among college students: the mediating role of emotion regulation. J Appl Dev Psychol 2017;50:36–44. [Google Scholar]
- [37].Natsuaki MN, Biehl MC, Ge X. Trajectories of depressed mood from early adolescence to young adulthood: the effects of pubertal timing and adolescent dating.JRes Adolesc 2009;19:47–74. [Google Scholar]
- [38].Rudolph KD, Troop-Gordon W. Personal-accentuation and contextual-amplifi-cation models of pubertal timing: predicting youth depression. Dev Psychopathol 2010;22:433–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Szwedo DE, Chango JM, Allen JP. Adolescent romance and depressive symptoms: the moderating effects of positive coping and perceived friendship competence. J Clin Child Adolesc Psychol 2015;44:538–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Liu RT. Characterizing the course of non-suicidal self-injury: a cognitive neuroscience perspective. Neurosci Biobehav Rev 2017;80:159–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.