

Abstract
Background/Aims:
Old age is a risk factor of suboptimal bowel preparation. This study aimed to evaluate the efficacy of mosapride citrate with a split dose of polyethylene glycol (PEG) plus ascorbic acid for bowel preparation in elderly patients (aged ≥65 years) before they underwent a colonoscopy.
Materials and methods:
This prospective investigator-blinded randomized study was conducted from November 2017 to October 2018. The patients were randomly divided into 2 groups, a mosapride group (mosapride citrate with a split-dose of PEG plus ascorbic acid) or a non-mosapride group (a split-dose of PEG plus ascorbic acid alone). Mosapride citrate 15 mg (Gastin CR) was administered once with each split-dose of the bowel preparation. The bowel preparation quality was assessed using the Boston Bowel Preparation Scale (BBPS).
Results:
A total of 257 patients were finally included and analyzed in our study. The total BBPS score was significantly higher in the mosapride group than in the non-mosapride group (8.53 vs 8.24, P = .033). The BBPS scores of the right colon and mid-colon were 2.75 vs 2.61 (P = .044) and 2.89 vs 2.79 (P = .030), respectively. The rate of adequate bowel preparation (BBPS ≥ 6) was similar in both groups (98.4% vs 98.5%, P = .968), while the rate of excellent bowel preparation (BBPS = 9) was higher in the mosapride group than in the non-mosapride group (73.8% vs 61.1%, P = .029). The total incidence of adverse events during the administration of the bowel cleansing agent, particularly abdominal fullness, was lower in the mosapride group (11.9% vs 30.5%, P < .001).
Conclusion:
The administration of mosapride citrate with a split-dose of PEG plus ascorbic acid in elderly patients showed an increase in bowel preparation efficacy and reduced adverse events, particularly abdominal fullness, during the administration of a bowel cleansing agent.
Keywords: bowel preparation, colonoscopy, mosapride citrate, prokinetic agent
1. Introduction
Colonoscopy is a standard tool for the screening and diagnosis of colorectal diseases. The prevalence of colorectal adenoma and cancer increases with age, as does the recurrence rate of adenoma.[1–4] Adequate bowel preparation is closely related to the safe and accurate application of colonoscopies. Inadequate bowel preparation can lead to longer and difficult colonoscopy procedures, increased patient discomfort, and a lower adenoma detection rate.[5]
Due to an increasingly elderly population, there is significant interest in performing bowel cleansing and colonoscopy procedures in elderly patients. Old age is considered a major risk factor for inadequate bowel preparation,[6–8] this has been suggested to be caused by a decreased number of bowel movements and an increased incidence of adverse events during the administration of the bowel cleansing agent in elderly patients. Complications associated with bowel cleansing may be increased in elderly patients due to the presence of multiple common comorbidities such as hypertension, diabetes, stroke, and renal failure. Therefore, elderly patients require careful planning and consideration before the performance of a colonoscopy.
Several studies have reported that the administration of a prokinetic agent with a bowel cleansing agent may improve the outcome of bowel preparations.[9–13] Mosapride citrate, a selective 5-hydroxytrptamie-4 (5-HT4) receptor agonist, is widely used to enhance gastrointestinal motility. Tajika et al[10] have shown that the use of mosapride citrate (5 mg immediate-release tablets) with bowel cleansing agents enhance bowel preparation and improve the tolerability to the procedure. However, the dose of mosapride citrate varied among these studies and several tablets were administered orally with the bowel cleansing agents. A new formulation of mosapride citrate 15 mg (Gastin; Korea United Pharm, Seoul, South Korea), that releases the active moiety slowly into the gastrointestinal tract, is expected to boast high compliance rates because it is taken once a day and carries a low risk of adverse events or side effect.[9,10]
This study aimed to evaluate the efficacy of this new formulation of mosapride citrate with a split dose of polyethylene glycol (PEG) plus ascorbic acid for bowel preparation in elderly patients (aged ≥65 years).
2. Methods
2.1. Subjects
This prospective investigator-blinded randomized study was performed from November 2017 to October 2018 at Inje University Haeundae Paik Hospital, Busan, South Korea (CRIS registration number: KCT0002580). This study enrolled consecutive outpatients over 65 years of age who were scheduled to undergo a colonoscopy for routine screening and surveillance. The following exclusion criteria were applied: patient aged under 65 years, the presence of a bowel obstruction, a structural intestinal disorder diagnosis, inflammatory bowel disease diagnosis, and the inability of the patient to provide informed consent. All participants provided written informed consent before enrollment in the study. This study was approved by our facility's institutional review board (HPIRB 2016–11–007–002).
2.2. Study protocol
This study was designed to evaluate the efficacy of mosapride citrate with a split dose of PEG plus ascorbic acid for bowel preparation in elderly patients (aged ≥65 years). The patients were randomly divided into 2 groups: mosapride citrate with a split-dose of PEG plus ascorbic acid (mosapride group) or a split-dose of PEG plus ascorbic acid alone (non-mosapride group). Two liters of Coolprep (PEG solution with 20 g ascorbic acid; Taejoon Pharm, Seoul, Korea) was used as the bowel cleansing agent. The patients ingested 1 liter of the Coolprep solution the evening before the colonoscopy (up to 21:00) and the remaining 1 liter in the morning at least 2 hours before the colonoscopy.
Mosapride citrate 15 mg (Gastin CR; Korea United Pharm) was administered twice with each split-dose of the bowel preparation as a prokinetic agent. This new formulation of mosapride citrate (Gastin CR), a controlled-release double-layer tablet administered once daily, releases the active moiety slowly into the gastrointestinal tract. In the mosapride group, one Gastin CR tablet was administered at 8:00 am the day before the colonoscopy, then another Gastin CR tablet was administered at 8:00 am on the day of the colonoscopy.
All colonoscopy procedures were conducted in the afternoon (between 14:00 pm and 16:30 pm) by 3 endoscopists with significant experience in performing colonoscopies. Prior to the commencement of the study, the endoscopists performed calibration exercises in 20 colonoscopies to ensure a high inter-rater consistency.
2.3. Assessment of outcomes
The primary outcome for both groups was the proportion of bowel preparations graded as adequate or excellent quality according to the total Boston Bowel Preparation Scale (BBPS) score. The secondary outcomes were the rate of adverse clinical events during the administration of the bowel cleansing agent, the patients’ satisfaction with the bowel cleansing, and the patients’ willingness to repeat the bowel cleansing method.
The BBPS was used to assess the bowel preparation quality for the 3 sections of the colon (right, mid, and left). Each section was assigned a segment score from 0 to 3 (excellent: 3; good: 2; fair: 1; poor: 0), and these segment scores were summed to calculate a total BBPS score of 0 to 9. An adequate bowel preparation was defined as a total score of 6 or higher, while an excellent bowel preparation was defined as a total score of 9.
Any adverse events and the patient tolerability during administration of the bowel cleansing agent were assessed with questionnaires before the colonoscopy. The adverse events of bowel cleansing included in this study were abdominal pain, abdominal fullness, nausea, vomiting, headache, dizziness, and sleep disturbance. The presence or absence of adverse events was recorded, and the degree of adverse events was assessed based on a 4-grade scale of 0–3. Patient tolerability and satisfaction were assessed by three questions: “how easy or difficult was it to take the cleansing agent?” (Easy/Tolerable/Difficult); “would you be willing to use the same regimen at the next colonoscopy?” (Strongly agree/Tolerable/Strongly disagree); and “how easy or difficult was it to take this cleansing agent compared with the previous one?” (Easy/Tolerable/Difficult).
2.4. Randomization and blinding
All eligible patients were randomly divided into 2 groups: mosapride citrate with a split-dose of PEG plus ascorbic acid (mosapride group) or a split-dose of PEG plus ascorbic acid alone (non-mosapride group). The patients were randomized into block sizes of two at a ratio of 1:1 using a random number table stored in an envelope. The researchers who generated the random number table did not participate in the subsequent study. The participating endoscopists were blinded to the patients’ assignments before and during the procedure, and before the scoring of the bowel cleansing.
2.5. Statistical analysis
To calculate the sample size, we assumed an adequate bowel preparation rate of 81% in elderly patients and an inter-group difference of 12% in the percentage of patients with an adequate bowel preparation that was based on previous data.[10,14] A sample size of 140 patients for each group was estimated to provide an 80% power at a 2-sided α of 0.05, assuming 10% missing data.
Quantitative data were presented as the mean ± standard deviation and were compared using a Student 2-tailed t test. Qualitative data were presented as percentages and were compared using the chi-square test. A P values <.05 were considered statistically significant. MedCalc Statistical Software version 19.0.7 (MedCalc Software bvba, Ostend, Belgium; https://www.medcalc.org; 2019) was used for the statistical data analysis.
3. Results
3.1. Patient characteristics
The patient allocations and dispositions are presented in Figure 1. A total of 280 patients were randomized in this study. Fourteen patients in the mosapride group were excluded from the outcome measurement (6 for refusing mosapride, eight for cancelling the colonoscopy), while nine patients in the non-mosapride group were excluded for cancelling the colonoscopy after they had provided informed consent. Thus, a total of 257 patients (126 in the mosapride group, 131 in the non-mosapride group) were finally included and analyzed. The mean patient age was 71 years (range, 65–84 years); 110 (42.8%) patients were male and 147 (57.2%) were female. There were no significant intergroup differences. Table 1 summarizes the subjects’ baseline characteristics.
Figure 1.
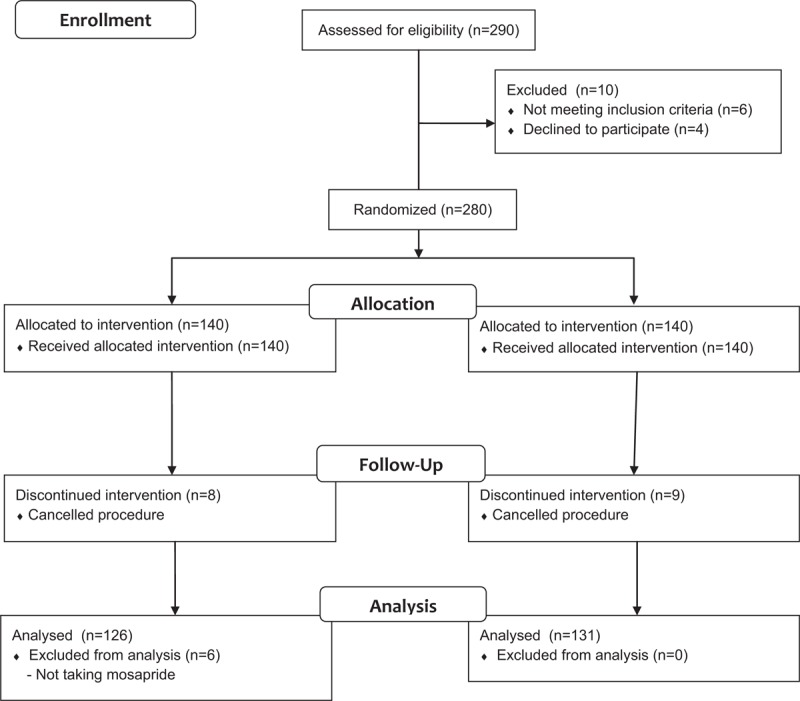
Consort flow diagram.
Table 1.
Patients’ baseline characteristics.

3.2. Bowel preparation quality
The efficacy of bowel cleansing according to the BBPS score is shown in Table 2. The total BBPS score was significantly higher in the mosapride group than in the non-mosapride group (8.53 vs 8.24, P = .033). The BBPS scores for right colon and mid-colon were 2.75 vs 2.61 (P = .044) and 2.89 vs 2.79 (P = .030), respectively, that were higher in the mosapride group than in the non-mosapride group. The rate of adequate bowel preparation (BBPS ≥ 6) was similar in both groups (98.4% vs 98.5%, P = .968), but the rate of excellent bowel preparation (BBPS = 9) was higher in the mosapride group than in the non-mosapride group (73.8% vs 61.1%, P = .029).
Table 2.
Efficacy of bowel cleansing according to BBPS.

3.3. Adverse events and compliance
A total of 87 patients (33 in the mosapride group, 54 in the non-mosapride group) experienced adverse events during the administration of the bowel cleansing agent; the incidence was significantly lower in the mosapride group than in the non-mosapride group (26.2% vs 41.2%, P = .011). Abdominal fullness and nausea were the most common adverse events in both groups. Except for abdominal fullness, the incidence of adverse events did not differ significantly between the two groups. The incidence of abdominal fullness was significantly lower in the mosapride group than in the non-mosapride group (11.9% vs 30.5%, P < .001). Greater than 80% of the patients in both groups ingested 100% of the bowel cleansing agent, more than 95% of the patients ingested 75% of the bowel cleansing agent. The adverse events and compliance rates are described in Table 3.
Table 3.
Compliance and Adverse events during bowel cleansing.

3.4. Patient satisfaction
The Patients’ tolerability of the bowel cleansing is shown in Table 4. The Patients’ satisfaction with the bowel preparation and willingness to repeat the same method did not differ significantly between the 2 groups. No significant difference was observed in the satisfaction with the current bowel cleansing process versus the previous bowel cleansing process in the 119 patients who had undergone a prior colonoscopy.
Table 4.
Satisfaction evaluated by patients.

3.5. Colonoscopic data
The polyp and adenoma detection rates, cecal incubation time, colonoscopy withdrawal time, and cecal intubation rates did not differ significantly between the 2 groups. Colonoscopic data are presented in Table 5.
Table 5.
Outcomes of colonoscopic findings.

4. Discussion
Our study suggests that mosapride citrate (Gastin CR) increased the quality of bowel preparations and reduced the incidence of adverse events during the administration of a bowel cleansing agent in elderly patients. Adequate bowel cleansing is essential to an accurate and safe colonoscopy. Bowel cleansing quality is affected by many factors including age, sex, the presence of co-morbidities, the adherence to the bowel cleansing instructions, the intake time of bowel the cleansing agent, and the appointment wait time.[6–8,15–17] Among them, old age is considered to be one of the major risk factors for inadequate bowel preparations.[6–8] In the elderly, a decreased number of bowel movements, a low compliance with the bowel preparation process, and an increased incidence of comorbidities such as hypertension, diabetes, stroke, and renal failure are considered to be the main causes of poor bowel cleansing.
Prokinetic agents have been studied for the purpose of improving the quality of bowel preparations.[9–13] A randomized controlled study reported that the optimal bowel cleansing rate of the left colon was significantly higher in a group that was administered 2 liters of PEG plus mosapride citrate 15 mg compared with a group that was administered 2 liters of PEG plus a placebo.[10] However, no study has investigated the effect of prokinetic agents on bowel cleansing in elderly patients. The present study evaluated the efficacy of a new formulation of mosapride citrate for bowel preparation in elderly patients (aged ≥65 years) and showed that the addition of mosapride citrate improved bowel preparation in elderly patients.
In the present study, the total BBPS score and the rate of excellent bowel preparations (BBPS = 9) was higher in the mosapride group than in the non-mosapride group, but there was no significant intergroup difference in the rate of adequate bowel preparation (BBPS ≥ 6). A total BBPS score ≥6 and/or an all segment scores ≥2 are considered a standard definition of adequate bowel preparation.[18–22] In a recent prospective study,[22] a BBPS segment score of 2 or 3 was reported as the cut-off value for adequate bowel preparation to detect adenomas larger than 5 mm, while a score of 2 was non-inferior to a score of 3. Furthermore, another study[23] reported that a BBPS score ≥8 was related to an increased polyp detection rate than a BBPS score <8 (44.9% vs 33.0%, P = .042). Calderwood et al[18] also reported that a BBPS segment score was positively correlated with an improved polyp detection rate in the right and left colon, however, this association was not observed in the transverse colon. In real-world clinical practice, higher BBPS scores, including the BBPS segmental score (3 vs 2), are more helpful for ensuring a safe and accurate colonoscopy in terms of a prolonged procedure time because of liquid fluid suction and patient discomfort.
The administration of the bowel cleansing agent was associated with the occurrence of adverse clinical events including nausea, vomiting, headache, abdominal fullness, and sleep disturbance. Requiring patients to drink a large amount of fluid can lower the patient tolerability and compliance to the bowel preparation. Accordingly, we considered the need to reduce the occurrence of adverse events to improve the tolerability to the bowel preparation and increase patient compliance; especially in elderly patients. Prokinetic drugs increase the number of bowel movements and have been used as an adjuvant agent in bowel cleansing. Cisapride has been used in previous studies to improve bowel cleansing[12,13]; however, it is no longer used because of the potential for serious cardiovascular side effects. The efficacy of other prokinetics, including itopride and mosapride, for bowel cleansing has also been studied.[9–11,24] Mishima et al[24] showed a lower incidence of uncomfortable abdominal symptoms in patients who received mosapride or itopride before bowel cleansing compared with those who received placebo. Tajika et al[10] also demonstrated that the patients receiving mosapride before PEG reported easier bowel cleansing than in their previous experience of colonoscopy. In accordance with these studies, this study showed that the total incidence of adverse events during administration of the bowel cleansing agent was lower in the mosapride group, particularly abdominal fullness (11.9% vs 30.5%, P < .001).
The new formulation of mosapride citrate (Gastin CR), a controlled-release double-layer tablet that is taken once daily, releases the active moiety slowly into the gastrointestinal tract. In this study, mosapride citrate 15 mg (Gastin CR; Korea United Pharm) was administered twice with each split-dose of the bowel preparation. Since Gastin CR costs 340 KRW (0.3 USD) per tablet, it is thought to be cost-effective considering the more difficult colonoscopy procedures and the increased patient discomfort caused by poor bowel preparations.
There are several limitations to our study. First, this study was not double-blinded. The enrolled patients knew whether they were in the mosapride or non-mosapride group, this might have acted as a confounding variable in terms of an objective assessment of the adverse events and the overall patient satisfaction. Second, because our study included only patients undergoing colonoscopies in the afternoon, these results may not be applicable to patients undergoing colonoscopies in the morning. Third, the mean age of the enrolled patients was 71 years and the proportion of patients over 75 years was small; thus, it may be difficult to generalize our results to very elderly patients.
In conclusion, this study demonstrated that mosapride citrate when administered with a split-dose of PEG plus ascorbic acid in elderly patients led to a sufficient bowel preparation. Furthermore, the administration of mosapride citrate resulted in a reduced rate of adverse events during bowel preparation such as abdominal fullness during the administration of the bowel cleansing agent. The study results suggest that prokinetic drugs such as mosapride may be an effective adjuvant agent for improving bowel preparation in patients of all ages, particularly in the elderly.
Author contributions
Conceptualization: Jin Lee, Tae Oh Kim.
Data curation: Su Jin Jeong, Tae Hyung Kim.
Formal analysis: Jin Lee, Nae-Yun Heo, Seung Ha Park.
Investigation: Su Jin Jeong, Yong Eun Park.
Methodology: Tae Hyung Kim, Yong Eun Park.
Resources: Joon Hyuk Choi, Nae-Yun Heo, Jongha Park, Young Soo Moon.
Supervision: Tae Oh Kim.
Validation: Joon Hyuk Choi, Jongha Park, Seung Ha Park.
Visualization: Young Soo Moon.
Writing – original draft: Jin Lee.
Writing – review & editing: Jin Lee.
Tae Oh Kim orcid: 0000-0002-7359-1599.
Footnotes
Abbreviations: BBPS = Boston Bowel Preparation Scale, PEG = polyethylene glycol.
How to cite this article: Lee J, Jeong SJ, Kim TH, Park YE, Choi JH, Heo NY, Park J, Park SH, Moon YS, Kim TO. Efficacy of mosapride citrate with a split dose of polyethylene glycol plus ascorbic acid for bowel preparation in elderly patients: A randomized controlled trial. Medicine. 2020;99:2(e18702).
Ethics committee approval was received for this study from the institutional review board.
Informed consent was obtained from all individual participants included in the study.
This study was supported by Korea United Pharm. Inc.
The authors have no conflicts of interest to disclose.
References
- [1].Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2013. Bethesda, MD: National Cancer Institute; 2016. [Google Scholar]
- [2].Martínez ME, Baron JA, Lieberman DA, et al. A pooled analysis of advanced colorectal neoplasia diagnoses following colonoscopic polypectomy. Gastroenterology 2009;136:832–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Park SK, Kim NH, Jung YS, et al. Risk of developing advanced colorectal neoplasia after removing high-risk adenoma detected at index colonoscopy in young patients: a KASID study. J Gastroenterol Hepatol 2016;31:138–44. [DOI] [PubMed] [Google Scholar]
- [4].Lee J, Wan J, Ho S, et al. Predictors of high-risk adenoma occurrence at surveillance colonoscopy in patients who undergo colorectal adenoma removal. Dig Dis 2018;36:354–61. [DOI] [PubMed] [Google Scholar]
- [5].Menees SB, Elliott E, Govani S, et al. The impact of bowel cleansing on follow-up recommendations in average-risk patients with a normal colonoscopy. Am J Gastroenterol 2014;109:148–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Nguyen DL, Wieland M. Risk factors predictive of poor quality preparation during average risk colonoscopy screening: the importance of health literacy. J Gastrointestin Liver Dis 2010;19:369–72. [PMID: 21188326]. [PubMed] [Google Scholar]
- [7].Chung YW, Han DS, Park KH, et al. Patient factors predictive of inadequate bowel preparation using polyethylene glycol: a prospective study in Korea. J Clin Gastroenterol 2009;43:448–52. [DOI] [PubMed] [Google Scholar]
- [8].Cha JM, Kozarek RA, La Selva D, et al. Risks and benefits of colonoscopy in patients 90 years or older, compared with younger patients. Clin Gastroenterol Hepatol 2016;14:80–6.e1. [DOI] [PubMed] [Google Scholar]
- [9].Tajika M, Niwa Y, Bhatia V, et al. Can mosapride citrate reduce the volume of lavage solution for colonoscopy preparation? World J Gastroenterol 2013;19:727–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Tajika M, Niwa Y, Bhatia V, et al. Efficacy of mosapride citrate with polyethylene glycol solution for colonoscopy preparation. World J Gastroenterol 2012;18:2517–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Kim HJ, Kim TO, Shin BC, et al. Efficacy of prokinetics with a split-dose of polyethylene glycol in bowel preparation for morning colonoscopy: a randomized controlled trial. Digestion 2012;86:194–200. [DOI] [PubMed] [Google Scholar]
- [12].Reiser JR, Rosman AS, Rajendran SK, et al. The effects of cisapride on the quality and tolerance of colonic lavage: a double-blind randomized study. Gastrointest Endosc 1995;41:481–4. [PMID: 7615227]. [DOI] [PubMed] [Google Scholar]
- [13].Ueda S, Iishi H, Tatsuta M, et al. Addition of cisapride shortens colonoscopy preparation with lavage in elderly patients. Aliment Pharmacol Ther 1994;8:209–14. [PMID: 8038353]. [DOI] [PubMed] [Google Scholar]
- [14].Day LW, Kwon A, Inadomi JM, et al. Adverse events in older patients undergoing colonoscopy: a systematic review and meta-analysis. Gastrointest Endosc 2011;74:885–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Romero RV, Mahadeva S. Factors influencing quality of bowel preparation for colonoscopy. World J Gastrointest Endosc 2013;5:39–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Johnson DA, Barkun AN, Cohen LB, et al. Optimizing adequacy of bowel cleansing for colonoscopy: recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer. Gastrointest Endosc 2014;80:543–62. [DOI] [PubMed] [Google Scholar]
- [17].Ness RM, Manam R, Hoen H, et al. Predictors of inadequate bowel preparation for colonoscopy. Am J Gastroenterol 2001;96:1797–802. [DOI] [PubMed] [Google Scholar]
- [18].Calderwood AH, Jacobson BC. Comprehensive validation of the Boston Bowel Preparation Scale. Gastrointest Endosc 2010;72:686–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Calderwood AH, Schroy PC, 3rd, Lieberman DA, et al. Boston Bowel Preparation Scale scores provide a standardized definition of adequate for describing bowel cleanliness. Gastrointest Endosc 2014;80:269–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Kluge MA, Williams JL, Wu CK, et al. Inadequate Boston Bowel Preparation Scale scores predict the risk of missed neoplasia on the next colonoscopy. Gastrointest Endosc 2018;87:744–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Johnson DA, Barkun AN, Cohen LB, et al. Optimizing adequacy of bowel cleansing for colonoscopy: recommendations from the US multi-society task force on colorectal cancer. Gastroenterology 2014;147:903–24. [DOI] [PubMed] [Google Scholar]
- [22].Clark BT, Protiva P, Nagar A, et al. Quantification of adequate bowel preparation for screening or surveillance colonoscopy in men. Gastroenterology 2016;150:396–405. quiz e14-e15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Kim EJ, Park YI, Kim YS, et al. A Korean experience of the use of Boston bowel preparation scale: a valid and reliable instrument for colonoscopy-oriented research. Saudi J Gastroenterol 2014;20:219–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Mishima Y, Amano Y, Okita K, et al. Efficacy of prokinetic agents in improving bowel preparation for colonoscopy. Digestion 2008;77:166–72. [DOI] [PubMed] [Google Scholar]