

Abstract
Work stress and burnout have become important issues. Changes in work patterns frequently, long working hours, and too much pressure among workers in high-tech companies may result in the chronic fatigue symptoms and increase the risk of cardiovascular diseases, even leading to sudden death. Changes of heart rate variability (HRV) can be treated as a warning from the autonomic nervous systems and as a long-term monitoring method for chronic disease, for example, cardiovascular diseases and sudden death. The purpose of this study was to explore the association between occupational burnout and HRV.
Proportional stratified convenient sampling was performed and in total, 120 individuals participated in this study. Questionnaires and the “occupational burnout inventory” were used to collect biographical and burnout information. A novel wrist physiological monitor was used to measure autonomic nervous system-related data, including HRV, low-frequency (LF) %, high-frequency (HF) %, and LF/HF ratio. Descriptive statistics and logistic regressions were computed using SPSS 17.0 (Chinese version, IBM Corp., New York, NY).
The results show that participants who were 20 to 25 years old, work overtime because of onerous personal tasks, had a medical history, and recently felt unwell have higher “personal burnout.” “Participants with a graduate degree, with onerous tasks, who were indirect staff, and with a regular-hour job tended to overcommit to their work.” Significant associations were found among medical history, recently feeling unwell, and “work-related burnout.” There was a positive association between HRV and job seniority. LF%, HF%, and LF/HF ratio were significantly correlated with job category. “Work overcommitment” was related to LF/HF ratio among men. Some items in “personal burnout” and “work overcommitment” were also associated with HRV among women.
The findings suggest that the measurement of HRV can be applied in occupational settings to assess burnout. It not only allows administrators to quickly select the colleagues who need health care, but also provides timely and appropriate care, thereby promoting the health of the worker.
Keywords: burnout, heart rate variability, occupational burnout inventory, high-tech company
1. Introduction
Health is a fundamental right of human beings. Each year, 38 million people die as a result of non-communicable diseases, with cardiovascular diseases (17.5 million) accounting for most of them.[1] The causes of these non-communicable diseases, such as cardiovascular diseases, are multidimensional and complex; Leischik et al[2] developed a 3D model of risk factors on the issue of health plasticity. These factors include environmental settings,[1,3] inequalities,[4] behaviors,[5–7] social/mental problems,[4,8] etc. The risk factors causing cardiovascular diseases should be similar to those factors mentioned above.[1–9] Among those risk factors, work-related factors are of concern in the occupational safety and health fields.
In the last decade, work stress and burnout have become important issues all over the world.[10–20] Moreover, several sudden deaths because of overwork (also known as “Karoshi”) have drawn public concern and been a major health issue in Taiwan. These cases of sudden death were related to cerebrovascular disease.[21] From 1994 to 2004, the Institute of Occupational Safety and Health conducted national surveys relevant to job stress; the results revealed that the percentage of workers who reported “always feeling job stress” increased substantially from 6.5% to 19.0%.[22–24] Furthermore, the changes in job requirements, particularly in high-tech companies, for example, prolonged working hours and excessive workload, resulted in increased job stress. Research has shown that long-term exposure to high job stress may lead to chronic fatigue, anxiety symptoms, irritability, depersonalization, and health issues such as hypertension, cardiovascular diseases, and increased low density of cholesterol.[25,26] Prolonged working hours was one of the factors that could also increase the risk of cardiovascular diseases, even leading to sudden death.[27] Therefore, the Ministry of Labor has issued the “The Guideline to Identify Cerebrovascular and Heart Diseases Induced by Jobs (Excluding the Acute Injuries)” in 2010 and specified that the major cause of such disease is excessive workload. Although a particular job is usually not the risk factor causing the cerebrovascular diseases, it is one of the precipitating factors of these diseases.[28]
Many organs in the body function because of the sympathetic and parasympathetic nervous systems under the final equilibrium state of the interaction between these systems, such as heartbeat, digestion, urination, and glycogen conversion. Heart rate variability (HRV) can be used to assess the overall activity of the autonomic nervous system (ANS).[29,30] The sudden decrease of HRV can be treated as a warning from the body systems and has been used as a long-term monitoring method for chronic disease, for example, cardiovascular diseases, diabetes, depression, arrhythmia, and sudden death.[29,31] The purpose of this study was to investigate the association between the occupational burnout inventory and HRV in a high-tech company.
2. Methods
2.1. Study design
This was a descriptive, cross-sectional study. The study participants were recruited using proportional stratified convenient sampling from a local display manufacturing company in Central Taiwan (6000 employees). There are 3 major departments in this company: engineering (38%), manufacturing (48%), and administration/logistics (14%). One unique characteristics of this type of company is that the technicians in the manufacturing department usually work for 12 hours either in day shift or night shift in consecutive days and then take 2-day off. In total, 120 participants completed the questionnaires and HRV measurement because of the time constraints and limited resources. All participants were recruited based on the percentage of the 3 departments: engineers (46 participants), manufacturing (57 participants), and administration (17 participants). Those who were pregnant, had dysautonomia, or had cancer were excluded from the study.
After reading the informed consent, all of the voluntary participants completed a biographic information questionnaire and occupational burnout inventory questionnaire in the physical examination room, office, or rest room. After completing these questionnaires, the researcher measured the physiological parameters of the ANS with a patient wrist monitor. If the measurement failed, the participant needed to rest for an additional 15 minutes before the next trial. The whole process took approximately 30 to 45 minutes. The China Medical University and Hospital Research Ethic Committee (CMUH REC) approved the research protocol (CMUH REC No. CMUH103-REC3-064). The recruiting period was from July 20 to November 30 in 2014.
2.2. Questionnaire and occupational burnout inventory
The questionnaire used in this study included 3 main parts: demographic information and personal medical history, working conditions, and the Chinese version of the Copenhagen Burnout Inventory (C-CBI). Demographic information included age, gender, height, weight, educational level, marital status, medical history, current prescription drug use, current health status (e.g., headache, insomnia), diet, physical activities per week, and smoking status and these factors might affect the HRV results. Medical history included hypertension, heart disease (minor mitral valve prolapse), hepatitis, and gout. The category of “others” in the medical history included asthma, allergic rhinitis, gastroesophageal reflux, migraine, anemia, and hyperthyroidism. Current prescription drug use included for heart diseases, hypertension, thyroid disease, Chinese medicine, and others e.g., Tylenol). Current health status included headache, insomnia, exhaustion, and others (e.g., tired). Because the numbers of participants in some categories in the medical history, prescription drug use, and current health status were too small, we recategorized the data into dichotomous groups: yes/no or good/unwell for statistical analysis. Working conditions included job title, length of employment in current position, work shift, number of hours of overtime in the past month, and reasons that might be relevant to the occupational fatigue.
In this study, the “occupational burnout inventory” was used to assess the burnout status. This inventory consists of 2 major domains: the C-CBI and overcommitment to work. The C-CBI, modified based on the Copenhagen Burnout Inventory with good validity and reliability, consists of 16 items in 3 dimensions.[24,32–34] There are 5 items for personal burnout, 5 items for work-related burnout, and 6 items for client-related burnout. However, client-related burnout was excluded because of the job characteristics; the chosen departments did not interact with customers. A 5-point Likert scale was used for the C-CBI. To assess the overcommitment to work, a modified Chinese version, Job-Content Questionnaire from Siegrist's Effort-Reward Imbalance Questionnaire, was used. There were five 5-point Likert scale items in this questionnaire, with a good validity and reliability with respect to the untranslated version.[26,35–38]
2.3. Heart rate variability
A patient wrist monitor (ANSWatch Model TS-0411, Taiwan Scientific Corp., New Taipei City, Taiwan) was used to measure the heart rate (HR) and ANS parameters, that is, heart rate variability (HRV). The cuff with piezoelectric sensors in it was placed on the radial artery on the left wrist for 7 minutes and recorded the blood pressure and pulse waveforms. Peak-to peak intervals were determined and calculated by time and frequency analyses. The HRV analysis followed the standard measurement proposed by the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology.[29,39] Irregular heartbeats, as caused by arrhythmia or body movement, were excluded. The parameters of the ANS used in this study and the associated physiological meanings and units follow the suggestions provided by the instrument user manual[40] and are listed below:
-
1.
HR: heart rate (beat/min).
-
2.
HRV: total ANS activity index (millisecond) defined as the standard deviation of all normal-to-normal intervals. The normal range is from 25 to 100 milliseconds.
-
3.
HF (%): high frequency (normal unit) representing the contribution of parasympathetic nervous activity; the normal range is from 30% to 55% with the mean equaled to 40.
-
4.
LF (%): low frequency (normal unit) representing the contribution of sympathetic nervous activity; the normal range is from 40% to 70% with the mean equaled to 60.
-
5.
LF/HF: ratio of LF to HF, representing the sympathetic-parasympathetic balance index; the normal range is from 0.5 to 2.5 with the mean equaled to 1.5.
The purpose of the HRV data collections was not used for disease diagnosis, and we categorized the data of HF and LF into 5 groups for statistical analysis reasons: less than 20, 20 to 39, 40 to 59, 60 to 79, and equal to or greater than 80.
2.4. Data analysis
Statistical analyses were performed using SPSS 17 (Chinese version 17.0, IBM Corp., New York, NY), with a level of significance of P < .05. Demographic data, including gender, age, level of education, marital status, as well as the work condition data such as position, hours of overtime in the last week, and work shifts, are presented as numbers and percentages. A one-way analysis of variance was used for the analysis of occupational burnout inventory and HRV associated with demographic information, medical history information, and work conditions. Logistic regression analysis was performed to identify the factors of the occupational burnout inventory influencing HRV.
3. Results
Table 1 shows the demographic variables, job characteristics, and medical history information of the participants. Of the 120 participants, 66 (55%) were male and 54 (45%) were female. In terms of education, there was a significant difference in the education level between genders (P = .003). Further, there were significant differences in occupations between the gender groups (P < .0001). Forty-six of the participants (38.3%) were engineers, and 41 of them were males (89%). Ninety-one percent of the female participants were technicians. There were significant differences in work shifts between the gender groups (P < .0001). Fifty-nine percent of the males worked the night shift. However, 61% of the females worked the day shift. In terms of the number of hours of overtime in the past month, the results revealed that 74 participants (61.7%) were in the group with overtime hours between 1 and 46 hours, and 53 (71.6%) of them were males. Furthermore, the company's request (46.7%) was the main reason for working overtime. In terms of medical history, 4 participants had heart disease. All of them had minor mitral valve prolapse; none of them had symptoms or were routinely visiting a clinic. Therefore, the authors did not exclude these 4 participants from the study.
Table 1.
Demographic information, work characteristics, and health status characteristics.
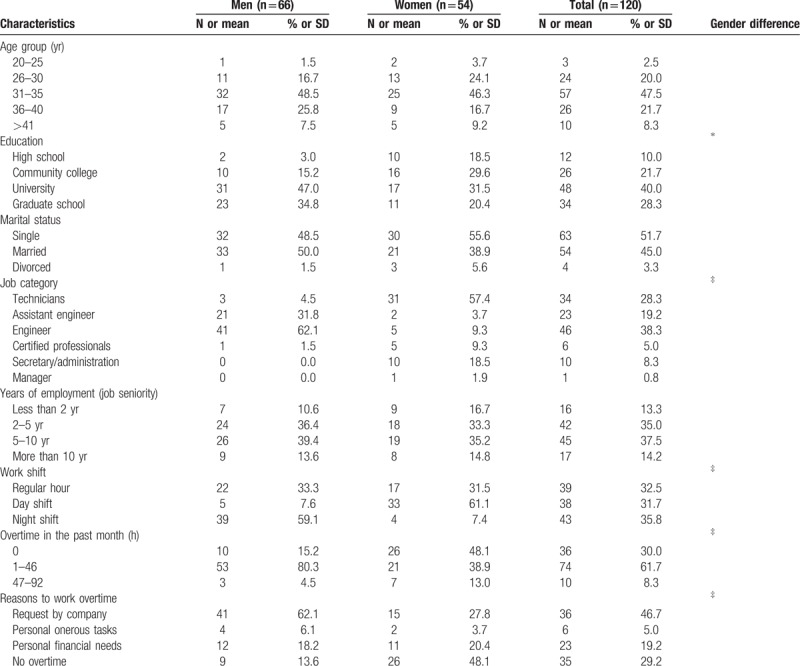
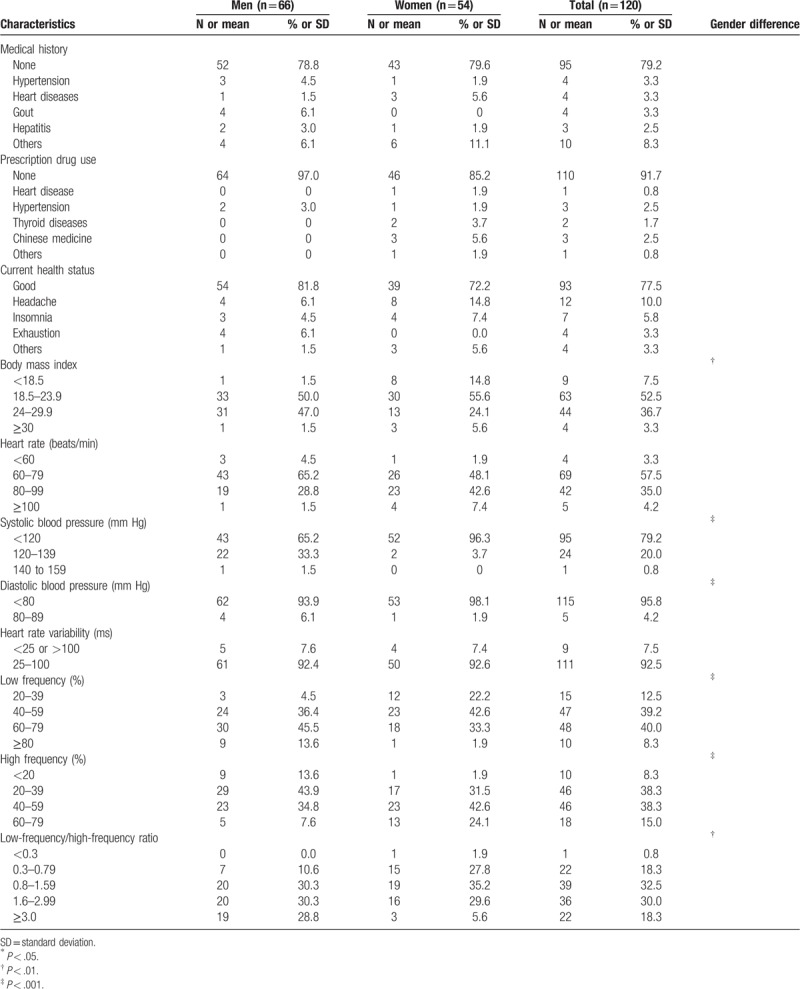
In terms of body mass index (BMI), there was a statistical difference on the gender (P = .004). Among the 44 participants who were overweight, 31 (70.5%) were males. Eight (88.9%) of the 9 underweight participants were females. In terms of blood pressure, 95 (79.2%) had a normal systolic blood pressure (90–119 mm Hg), and 52 (54.7%) of these 95 participants were females. One (1.5%) male participant had stage-1 hypertension (140–159 mm Hg). Regarding the diastolic blood pressure, 115 (95.8%) had the desired diastolic blood pressure (60–79 mm Hg), and 5 (4.2%) were in the prehypertension group (80–89 mm Hg). Four (80%) of these 5 participants were males. There were significant gender differences in the blood pressure categories.
In terms of the ANS parameters, the results revealed that there were significant gender differences among the parameters of LF/HF ratio, LF(%), and HF(%) (P < .001). However, there was no significant difference in HRV between males and females (P = .887). Fifty-eight (48.3%) of the participants had a higher value (>60%) of LF (%), representing the contribution of sympathetic nervous activity, and 39 (66.1%) of these 58 participants were males. Fifty-six (46.6%) of the participants had a lower value (<39%) of HF (%), and 38 (67.9%) of these 56 participants were males. In terms of the value of LF/HF ratio, 58 (48.3%) were higher than the normal value (>1.6), and 39 (32.5%) were in the normal range (0.8–1.59). For those with a higher value of LF/HF ratio, 39 (67.2%) were males.
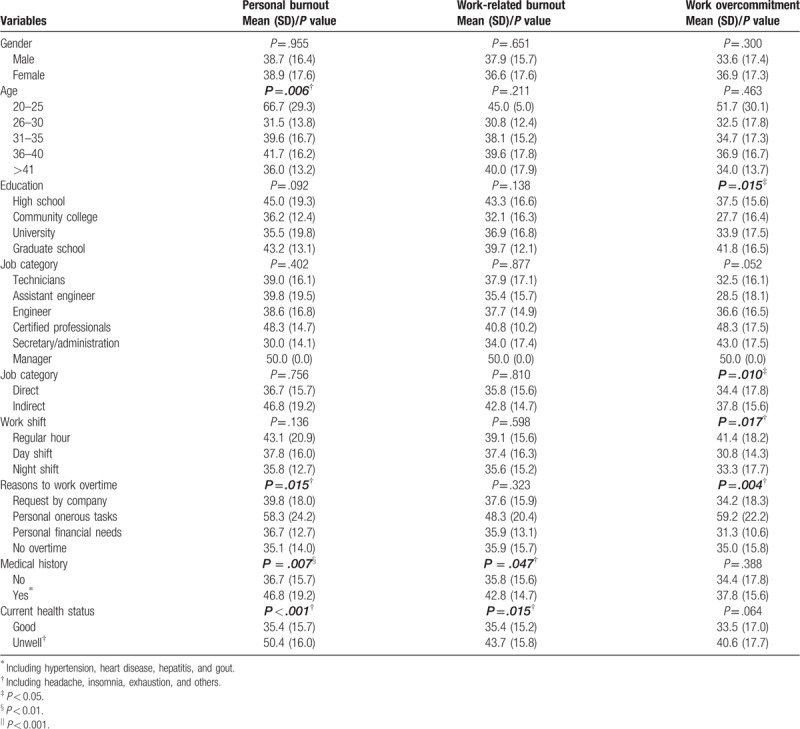
The results of 3 dimensions in the occupational burnout inventory are shown in Table 2. No statistically significant association was found between the gender and the scores of the 3 dimensions in the occupational burnout inventory (P = .300–.955).
Table 1 (Continued).
Demographic information, work characteristics, and health status characteristics.
In the dimension of personal burnout, it was significantly associated with age (F(4;115) = 3.794; P = .006), reasons to work overtime (F(3;116) = 3.630; P = .015), medical history (2 levels: yes/no, F(1;118) = 7.486; P = .007), and current health status (2 levels: good/unwell, F(1;118) = 18.824; P < .001). Post hoc test results revealed that participants between the ages of 20 and 25 years had significantly higher personal burnout scores than participants in the other age group (66.7 ± 29.3), and the age group of 36 to 40 years followed (41.7 ± 16.2). Regarding the reasons for working overtime, the results showed that participants with onerous tasks had significantly higher personal burnout scores (58.3 ± 24.2) than other reasons or without overtime participants. Participants with a medical history (46.8 ± 19.2) had scores 10 points higher than those without any major diseases (36.7 ± 15.7). Participants with good health status (35.4 ± 15.7) had lower personal burnout scores (35.4 ± 15.7) than those with at least 1 symptom among headache, insomnia, exhaustion, or others (50.4 ± 16.0).
Regarding work-related burnout, it was significantly associated with medical history (2 levels: yes/no, F(1;118) = 4.026; P = .047) and current health status (2 levels: good/unwell, F(1;118) = 6.121; P = .015). Participants with a medical history (42.8 ± 14.7) had 7 more points in the work-related burnout scores than those without any major diseases (35.8 ± 15.6). Participants with good health status (35.4 ± 24.2) had lower work-related burnout scores than those with at least 1 symptom among headache, insomnia, serious fatigue, and others (43.7 ± 24.2).
The score of “work overcommitment” was significantly associated with education level (F(3;116) = 3.649; P = .015). Participants with graduate degrees were overcommitted to work in comparison with others. Furthermore, participants who were indirect staff (engineers, managers, certified professionals, secretary/administrators) tended to overcommit to their work in comparison with direct staff members (technicians and assistant engineers) (37.8 ± 15.6 vs 34.4 ± 17.8; F(1;118) = 6.847; P = .010). For participants who worked during the regular hours, the score of “work overcommitment” was significantly higher than for those participants who work either in the day shift or in the night shift (F(2;117) = 4.223; P = .017). In comparison with the reasons for overtime, those who had onerous tasks tended to overcommit to their work in comparison with participants with other reasons, such as no overtime, working overtime because of the company's request or because of personal finance requirements (F(3;116) = 4.674; P = .004).
In general, participants with a medical history and feeling unwell tended to have higher personal and work-related burnout. Participants with onerous tasks, a graduate degree, an indirect position, and regular-hour work tended to overcommit to their work.
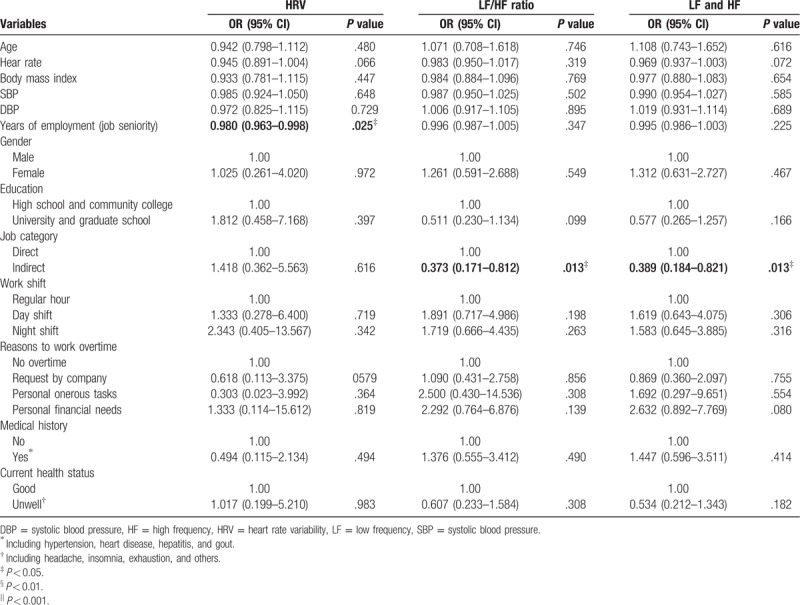
The associations between ANS parameters and demographic and health information are shown in Table 3. Most of the biographic, health-related variables were not significantly associated with HRV, LF/HF ratio, HF(%), or LF(%). Job seniority was found to be associated with HRV (odds ratio [OR] = 0.980, 95% confidence interval [95% CI]: 0.963–0.998, P = .025). LF% (OR = 0.389, 95% CI: 0.184–0.821, P = .013), HF% (OR = 0.389, 95% CI: 0.184–0.821, P = .013), and LF/HF ratio (OR = 0.373, 95% CI: 0.171–0.812, P = .013) were significantly correlated with job category (direct vs indirect). The associations between heart rate and HRV (OR = 0.945, 95% CI: 0.891–1.004, P = .066), LF% (OR = 0.969, 95% CI: 0.937–1.003, P = .072), and HF% (OR = 0.969, 95% CI: 0.937–1.003, P = .072) were borderline.
Table 2.
Association between occupational burnout inventory and information, work characteristics, and health status characteristics.
The correlation between the ANS parameters and the scores of occupational burnout inventory is shown in Table 4. None of any ANS parameters was significantly correlated with the 3 dimensions in the occupational burnout inventory in general or among women. The dimension of “work overcommitment” tended to poorly correlate with HF(%), LF(%), and LF/HF ratio among men.
Table 3.
Logistical regression analysis of factors associated with HRV, LF/HF Ratio, LF, and HF.
Taking further steps to investigate the correlation between the ANS parameters and each item in the occupational burnout inventory (data not shown), the results revealed that 1 item (“how often are you physically exhausted?”) in the “personal burnout” was correlated with HRV (Spearman correlation coefficients = 0.187, P = .041). Another item (“are you exhausted in the morning at the thought of another day at work?”) in the “work-related burnout” was correlated with HRV (Spearman correlation coefficients = 0.187, P = .047). Regarding the gender difference, all items in the occupational burnout inventory were not correlated with HRV for men. For female participants, 1 item (“are you exhausted in the morning at the thought of another day at work?”) in the “work-related burnout” and another item (“when I get home, I am still thinking about work problems”) in the subscale of “work overcommitment” were correlated with HRV (Spearman correlation coefficients = 0.341, P = .012; Spearman correlation coefficients = 0.287, P = .035, respectively). “Work overcommitment” was also poorly related to LF/HF ratio among male participants (Spearman correlation coefficients = 0.274, P = .026). In addition, the item “as soon as I get up in the morning, I start thinking about work problems” was significantly correlated with the LF/HF ratio (Spearman correlation coefficients = 0.262, P = .034). Two items in the dimension of “work overcommitment” were significantly associated with HF(%) and LF(%) among men. These items were “as soon as I get up in the morning, I start thinking about work problems” (Spearman correlation coefficients = 0.291, P = .018) and “when I got to bed, I am still thinking about work problems” (Spearman correlation coefficients = 0.266, P = .031).
After adjusting for possible confounding factors, such as job category, job seniority, HR, age, BMI, education, medical history, economics condition, and extra working hours in the past month, all parameters of ANS (HRV, LF/HF ratio, HF[%], and LF[%]) were not significantly associated with any of the dimensions of the occupational burnout inventory (P = .13–.79) (Table 5). The dimension of “work overcommitment” was somewhat associated with HRV (P = .13).
Table 4.
The correlation between occupational burnout inventory and HRV, LF, HF, and LF/HF ratio.
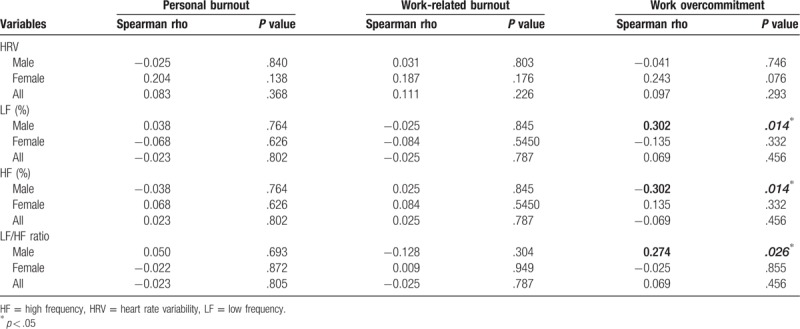
Table 5.
Logistical regression analysis of subscales of occupational burnout inventory factors associated with the normality of HRV, LF/HF ratio, LF, and HF.

4. Discussion
Generally, participants who were young (20–25 years old), who worked overtime because of onerous personal tasks, who had a medical history, and feeling unwell tended to report higher personal burnout scores. Higher work-related burnout was associated with medical history and feeling unwell. Participants with a graduate degree, with onerous tasks, who were indirect staff, and with a regular-hour job tended to overcommit to their work. The results showed that gender was not significantly associated with the 3 dimensions of the occupational burnout inventory. In addition, the occupational burnout inventory is not correlated with the parameters of ANS function. Furthermore, there was no significant association among the occupational burnout inventory and the normality of the ANS parameters after adjusting for confounding factors.
The effects of the reasons for working overtime on burnout, the association between current health status and burnout, and the association with work overcommitment for those with graduate degrees and indirect positions reported in this study had not been reported in earlier studies. The results were comparable to the results from previous studies in which young, junior employees with regular-hour work had higher burnout scores.[20,41,42]
The results in this study revealed that there were no significant gender differences in personal or work-related burnout; this is in conflict with the results from previous studies.[34,43] Job characteristics of the study population, the differences of definitions in job title, and small sample size may contribute to the different results in comparison with other studies.
The authors categorized the jobs into 6 different categories in order to investigate the effects of job category on burnout. Because of the small sample size, it was difficult to conduct a statistical analysis. Therefore, the authors recategorized the participants into 2 major groups: direct and indirect. The participants in the direct-position group were technicians, and assistant engineers who usually work on the production line. The characteristics of direct staff included labor intensive, routine task execution, high school and community college degrees, and usually work either the day shift or the night shift with 12 working hours for 2 consecutive days and resting for 2 days. Engineers, certified professionals, secretary/administrators, and managers were classified in the indirect position group. The characteristics in this group included higher education, working regularly in the daytime with occasional night duty, policy and project planning, and decision-making. After adjusting for the job category, the indirect staff were significantly more committed to their work than those who were direct staff. Although there were no significant differences, the scores for personal and work-related burnout of indirect staff were higher than the scores of direct staff. These findings were similar to the results from Yeh et al.[34]
Regarding the association between health status and occupational burnout, the results from previous studies showed that work under high job stress conditions might result in hypertension, cardiovascular disease, depression, and chronic fatigue syndrome.[25,26] Prochalska et al[25] suggested that in order to diagnose chronic fatigue syndrome, physicians should exclude factors, such as obesity (BMI > 25) and those diseases that would result in fatigue. Hsiao[42] also suggested that health problems would result in burnout, such as viral and respiratory infections, diabetes, cardiovascular diseases, obesity, and liver diseases. This study suggested that participants with a past medical problem and who subjectively reported feeling unwell had higher scores of personal and work-related burnout, confirming results from previous studies.[25,26] However, no significant associations among BMI, HR, blood pressure, and the 3 dimensions of occupation burnout inventory in this study contradicted the findings from the earlier study.
Research has shown that age, gender, HR, blood pressure, obesity, health status, psychological stress, respiration rate, regular exercise, air pollutants, PM2.5, household sprays, and scented products will affect the HRV.[29,30,44–46] Among these factors, HR and age were inversely correlated to HRV. However, obesity and work stress were positively correlated to the ratio of LF/HF. Regular exercise increased HRV and the parasympathetic nerve system activity, suggesting a decreased risk of cardiovascular disease.[45,46] In this study, the results revealed that HRV significantly decreased as years of employment increased (P = .025), and LF(%), HF(%), and LF/HF ratio were significantly associated with job category (P = .013). However, there was no significant association between HRV and age, gender, HR, or blood pressure; this result was different from those of previous studies. The possible reason may be because of the study purpose. In earlier studies, researchers tried to investigate the linear association between HRV and correlated variables. In contrast, the main purpose of this study was to identify the high risk of cardiovascular diseases and the abnormalities of HRV, LF(%), HF(%), and LF/HF ratio. Therefore, the results of the OR represented the association between the abnormalities of ANS function indices and the demographic and health characteristics. Regarding the significant association of HRV with years of employment, a previous study showed that job seniority was a risk factor for high job stress, and was also associated with “work overcommitment.” Although “work overcommitment” is not the direct factor resulting in fatigue, it may be an important factor related to occupational burnout and may worsen the health condition. Previous studies have identified that worse health status resulted in decreased HRV, increasing the risk of heart diseases.[20,29,34,47] In addition, most of the indirect staff reported that they did not have extra energy to exercise, gained weight every year, and usually did not have dinner at a regular time (most after 8 PM). These can explain the association between HRV and job seniority, and the associations between LF (%), HF (%), and LF/HF ratio and position.
In general, the occupational burnout inventory is not correlated with the parameters of ANS function indices. However, there were 2 items in each subscales of the occupational burnout inventory that were correlated with one of the indices. LF (%), HF (%), and LF/HF ratio were significantly correlated with “work overcommitment” for men. In contrast, “personal burnout” and “work overcommitment” were significantly correlated to HRV for women. Tseng and Cheng[26] mentioned that employees with higher “work overcommitment” scores had a higher job stress. Yeh et al[34] showed that employees with higher “work overcommitment” scores usually sacrificed their leisure time and spent more time on these jobs voluntarily. The situation of “overcommitment” may not result in burnout, but it was correlated with those “Karoshi” cases. This can be explained by the fact that “work overcommitment” tended to result in occupational burnout and worsen the health status. High job stress is associated with decreases in HRV that will affect the HPA feedback and result in the increase of cardiovascular diseases.[48]
After adjusting for age, HR, BMI, education, medical history, job category (direct/indirect), job seniority, and extra working hours in the previous month, there was no significant association among the 3 dimensions of occupational burnout inventory and the normality of the ANS parameters. One of the possible reasons to explain the insignificant association in the occupational burnout inventory is the conservativeness of the participants, leading to lower scores in the 3 dimensions when compared to other studies.[24,32,34] Another reason is the small sample size of the participants.
Although the HRV was not significantly associated with the score from the occupational burnout inventory, the scales in the domain of “work overcommitment” were found to be associated with HRV in comparison with the domains of “personal burnout” and “work-related burnout.” The result showed that the ratio of LF to HF was statistically significant for male participants. In addition, high-tech employees were found to be in a high-risk group for burnout, overcommitment, and abnormalities in the ANS function. Therefore, health care professionals should focus on the results of physical exams among these employees, especially those with high blood pressure and HRV. An intervention should be given in advance to those with chronic fatigue or metabolic issues resulting from overcommitment and working overtime in order to reduce the risk of any diseases.
Regarding ANS parameters, the authors recommend that HRV can be applied to work places, especially to employees with existing diseases, who are obese, who work overtime, have an excess workload, and have a high score for occupational burnout or stress, although there was a weak association between HRV and these factors. However, the results from earlier studies showed that there were associations between HRV and cardiovascular diseases, obesity, and even Karoshi. By measuring HRV and monitoring the HRV trend, health care professionals can screen out possible cases with arrhythmias and/or ANS function abnormalities in order to provide early medical treatment and promote regular health education. Furthermore, this can reduce the risks of cardiovascular diseases resulting from occupational fatigue, work stress, and burnout.
This study has some limitations. This was a cross-sectional study that represents a snapshot in time limited to the participants herein. In the study tools, the occupational burnout inventory is a subjective method to collect data. Although the researchers already explained confidentiality of the study, it was hard to appease the concerns of the participants, especially with respect to the leakage of information to the managers of the company. Regarding the biographic and health status information, the data were collected using questionnaires, not from physical examination records. The subjective method also may affect the study results if the participants did not provide the correct responses. In addition, we did not include noise or other environmental factors in our study. Therefore, it is difficult to discuss the association between HRV and noise exposure; thus, the effect of work-related burnout on HRV cannot be investigated with the noise effect.
In the HRV measurement, the authors use a wrist-band HR and blood pressure monitor. This instrument has passed the ISO 13485 and European Union CE marking requirement. The precision and accuracy should be acceptable. However, the measurement was easily affected by body or extremity movements and respiration in a sitting position, resulting from the limited test space. The researchers checked the data immediately after the measurement and redid it, if there were any interferences, after a 15-minute resting period. This may induce psychological stress because the examination duration may pass the regular break period given by the company.
This study was the first to investigate the association between occupational burnout and HRV in the high-tech industry, a unique industry in Taiwan. There were only 120 study participants in this cross-sectional study; this may limit the statistical power and interpretation of the results. We recommend increasing the sample size, including the health examination records, and conducting a follow-up study that can clearly analyze the association between occupational burnout and HRV in the future study.
Cardiovascular diseases are a multifactor problem, from the environmental setting to inequalities and from personal behavior to organizations. In this study, our focus was on the investigation of the association between occupational burnout and HRV for early intervention. Therefore, factors, such as green cities, inequalities, and physical inactivity, will remain for future studies.
This study concluded that participants who were young (20–25 years) and junior and who worked overtime because of onerous personal tasks reported a higher personal burnout score. Participants with graduate degrees, who were indirect staff, with a regular-hour job, and who worked overtime because of onerous personal tasks tended to overcommit to their work. Participants with a past medical problem and unhealthy status were at a high risk for personal and work-related burnout. Junior employees had higher HRVs. The abnormality in LF(%), HF(%), or the ratio of LF/HF for indirect employees was lower than the direct staff. Male participants with “work overcommitment” status tended to be positively correlated with LF(%) and the LF/HF ratio and tended to be negatively correlated with HF(%), indicating over-functioning of the sympathetic nervous system. Overall, HRV is an objective method to evaluate occupational burnout and can be used to screen out employees at a higher risk for cardiovascular problems. With early intervention and/or health education and promotion to these employees, the prevalence of burnout and even cardiovascular diseases can be prevented.
Acknowledgments
The authors would like to thank all of the participants in the high-tech company.
Author contributions
Conceptualization: Ei-Wen Victor Lo, Yin-Hsuan Wei, Bing-Fang Hwang.
Data curation: Ei-Wen Victor Lo, Yin-Hsuan Wei, Bing-Fang Hwang.
Formal analysis: Ei-Wen Victor Lo, Yin-Hsuan Wei, Bing-Fang Hwang.
Investigation: Ei-Wen Victor Lo, Yin-Hsuan Wei, Bing-Fang Hwang.
Methodology: Ei-Wen Victor Lo, Yin-Hsuan Wei, Bing-Fang Hwang.
Project administration: Yin-Hsuan Wei, Bing-Fang Hwang.
Resources: Ei-Wen Victor Lo, Yin-Hsuan Wei, Bing-Fang Hwang.
Software: Yin-Hsuan Wei.
Supervision: Ei-Wen Victor Lo, Bing-Fang Hwang.
Validation: Ei-Wen Victor Lo, Yin-Hsuan Wei, Bing-Fang Hwang.
Writing – original draft: Ei-Wen Victor Lo, Yin-Hsuan Wei, Bing-Fang Hwang.
Writing – review & editing: Ei-Wen Victor Lo, Yin-Hsuan Wei, Bing-Fang Hwang.
Ei-Wen Victor Lo orcid: 0000-0001-6859-2100.
Footnotes
Abbreviations: 95% CI = 95% of confidence interval, ANS = autonomic nervous system, BMI = body mass index, C-CBI = Chinese version of the Copenhagen Burnout Inventory, HF (%) = high frequency (normal unit), HR = heart rate, HRV = heart rate variability, LF (%) = low frequency (normal unit), OR = odds ratio.
How to cite this article: Lo EWV, Wei YH, Hwang BF. Association between occupational burnout and heart rate variability–a pilot study in a high-tech company in Taiwan. Medicine. 2020;99:2(e18630).
The authors report no conflicts of interest.
References
- [1].WHO. World Health Report 2013: Research for Universal Health Coverage. Geneva, Switzerland: WHO; 2013. [Google Scholar]
- [2].Leischik R, Dworrak B, Strauss M, et al. Plasticity of health. German J Med 2016;1:1–7. [Google Scholar]
- [3].WHO. Urban Green Spaces and Health. Copenhagen, Denmark: WHO Regional Office Europe; 2016. [Google Scholar]
- [4].Lee HE, Kim HR, Chung YK, et al. Mortality rates by occupation in Korea: a nationwide, 13-year follow-up study. Occup Environ Med 2016;73:329–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Strauß M, Foshag P, Przybylek B, et al. Occupation and metabolic syndrome: is there correlation? A cross sectional study in different work activity occupations of German firefighters and office workers. Diabetol Metab Syndr 2016;8:57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Leischik R, Foshag P, Strauß M, et al. Aerobic capacity, physical activity and metabolic risk factors in firefighters compared with police officers and sedentary clerks. PLoS One 2015;10:e0133113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Edwardson CL, Gorely T, Davies MJ, et al. Association of sedentary behaviour with metabolic syndrome: a meta-analysis. PLoS One 2012;7:e34916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Maslach C, Leiter MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry 2016;15:103–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Rootman I, Goodstadt M, Hyndman B, et al. Evaluation in Health Promotion: Principles and Perspectives. Copenhagen, Denmark: WHO Regional Office Europe; 2001. [Google Scholar]
- [10].Bagaajav A, Myagmarjav S, Nanjid K, et al. Burnout and job stress among Mongolian doctors and nurses. Ind Health 2011;49:582–8. [DOI] [PubMed] [Google Scholar]
- [11].Bjorner JB, Pejtersen JH. Evaluating construct validity of the second version of the Copenhagen psychosocial questionnaire through analysis of differential item functioning and differential item effect. Scand J Public Health 38D 2010:90–105. [DOI] [PubMed] [Google Scholar]
- [12].Collin V, Toon M, O'Selmo E, et al. A survey of stress, burnout and well-being in UK dentists. Br Dent J 2019;226:40–9. [DOI] [PubMed] [Google Scholar]
- [13].Creedy DK, Sidebotham M, Gamble J, et al. Prevalence of burnout, depression, anxiety and stress in Australian midwives: a cross-sectional survey. BMC Pregnancy Childbirth 2017;17:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Dreher A, Theune M, Kersting C, et al. Prevalence of burnout among German general practitioners: comparison of physicians working in solo and group practices. PLoS One 2019;14:e0211223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Fong TC, Ho RT, Ng SM. Psychometric properties of the Copenhagen Burnout Inventory–Chinese version. J Psychol 2014;148:255–66. [DOI] [PubMed] [Google Scholar]
- [16].Ilić IM, Arandjelović MŽ, Jovanović JM, et al. Relationships of work-related psychosocial risks, stress, individual factors and burnout–questionnaire survey among emergency physicians and nurses. Med Pr 2017;68:167–78. [DOI] [PubMed] [Google Scholar]
- [17].Schooley B, Hikmet N, Tarcan M, et al. Comparing burnout across emergency physicians, nurses, technicians, and health information technicians working for the same organization. Medicine (Baltimore) 2016;95:e2856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Shoorideh FA, Ashktorab T, Yaghmaei F, et al. Relationship between ICU nurses’ moral distress with burnout and anticipated turnover. Nurs Ethics 2015;22:64–76. [DOI] [PubMed] [Google Scholar]
- [19].Walters JE, Brown AR, Jones AE. Use of the Copenhagen Burnout Inventory with social workers: a confirmatory factor analysis. Hum Serv Organ Manag Leadersh Gov 2018;42:437–56. [Google Scholar]
- [20].Wu P-C, Chen S-H, Huang C-Y. Work stress and related risk factors among high tech male workers in southern Taiwan [in Chinese]. Chin J Occup Med 2013;20:215–25. [Google Scholar]
- [21].Bureau of Labor Insurance. 2018. Statistical data–annual report. Available at: https://www.bli.gov.tw/en/0009555.html. Accessed August 10, 2019. [Google Scholar]
- [22].Institute of Occupational Safety and Health. Survey of Employee's Perception of Safety and Health in the Work Environment. Taipei, Taiwan: The Council of Labor Affairs Institute of Occupational Safety and Health; 1994. [Google Scholar]
- [23].Institute of Occupational Safety and Health. Taiwan Labor's Job-Burnout and Related Psychosocial Factor Survey in 2004. Taipei, Taiwan: The Council of Labor Affair Institute of Occupational Safety and Health; 2004. [Google Scholar]
- [24].Yeh WY, Cheng Y, Chen CJ, et al. Psychometric properties of the Chinese version of Copenhagen Burnout Inventory among employees in two companies in Taiwan. Int J Behav Med 2007;14:126–33. [DOI] [PubMed] [Google Scholar]
- [25].Prochalska C, Gressier F, Corruble E. Chronic fatigue syndrome: an update for psychiatrists. Open J Psychiatry 2012;2:40–8. [Google Scholar]
- [26].Tseng H-P, Cheng Y. Reliability and validity of the Chinese demand-control-support model and effort-reward imbalance model questionnaires: a study among employees of the microelectronic industry. Taiwan J Public Health 2002;21:420–32. [Google Scholar]
- [27].Cleland JG, Chattopadhyay S, Khand A, et al. Prevalence and incidence of arrhythmias and sudden death in heart failure. Heart Fail Rev 2002;7:229–42. [DOI] [PubMed] [Google Scholar]
- [28].Ministry of Labor. 2010. The identification reference of occupation precipitating cerebrovascular and heart diseases guideline (revised). Taiwan, ROC. Available at: https://www.osha.gov.tw/1106/1119/1136/1138/12664/. Assessed September 17, 2019 [Google Scholar]
- [29].Camm AJ, Malik M, Bigger JT, et al. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur Heart J 1996;17:354–81. [PubMed] [Google Scholar]
- [30].Borchini R, Ferrario MM, Bertu L, et al. Prolonged job strain reduces time-domain heart rate variability on both working and resting days among cardiovascular-susceptible nurses. Int J Occup Med Environ Health 2015;28:42–51. [DOI] [PubMed] [Google Scholar]
- [31].Chang C-F, Chung Y-W, Lin C-S, et al. Analysis natural heart rate variability using photoplethysmography. J Adv Eng 2010;5:235–43. [Google Scholar]
- [32].Yeh W-Y, Cheng Y, Chen M-J, et al. Development and validation of an occupational burnout inventory. Taiwan J Public Health 2008;27:349–64. [Google Scholar]
- [33].Kristensen TS, Borritz M, Villadsen E, et al. The Copenhagen Burnout Inventory: a new tool for the assessment of burnout. Work Stress 2005;19:192–207. [Google Scholar]
- [34].Yeh W-Y, Cheng Y, Chen M-J, et al. Factors associated with workers’ burnout and “over-commitment to work”: a survey among employees of 36 companies in Taipei City. Taiwan J Public Health 2008;27:463–77. [Google Scholar]
- [35].Siegrist J, Peter R, Junge A, et al. Low status control, high effort at work and ischmic-heart-disease–prospective evidence from blue-collar men. Soc Sci Med 1990;31:1127–34. [DOI] [PubMed] [Google Scholar]
- [36].Siegrist J, Starke S, Chandola T, et al. The measurement of effort-reward imbalance at work: European comparisons. Soc Sci Med 2004;58:1483–99. [DOI] [PubMed] [Google Scholar]
- [37].Cheng YW, Luh WN, Guo YL. Reliability and validity of the Chinese version of the job content questionnaire in Taiwanese workers. Int J Behav Med 2003;10:15–30. [DOI] [PubMed] [Google Scholar]
- [38].Li J, Yang WJ, Cheng YW, et al. Effort-reward imbalance at work and job dissatisfaction in Chinese healthcare workers: a validation study. Int Arch Occup Environ Health 2005;78:198–204. [DOI] [PubMed] [Google Scholar]
- [39].Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996;93:1043–65. [PubMed] [Google Scholar]
- [40].Taiwan Scientific Corp. 2010. ANSWatch® Wrist Monitor–user's manual. Available at: https://www.sunscientific.com/files/ANSWatch_Users_Manual_English.pdf Accessed September 17, 2019. [Google Scholar]
- [41].Tzeng M-T. A Research of Burnout Associated with Physical and Mental Health. Taipei City, Taiwan: Department of Business Management, National Taipei University of Technology; 2011. [Google Scholar]
- [42].Hsiao C-W. Investigation of Work Stress, Shiftwork, Fatigue and Health Status among Manufacturing Workers. Tainan City, Taiwan: Department of Occupational Safety and Health, Chang-Jung Christian University; 2010. [Google Scholar]
- [43].Chou LP, Li CY, Hu SSC. Job stress and burnout in hospital employees: comparisons of different medical professions in a regional hospital in Taiwan. BMJ Open 2014;4:7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [44].Liang W-C, Yuan J, Sun DC, et al. Changes in physiological parameters induced by indoor simulated driving: effect of lower body exercise at mid-term break. Sensors (Basel) 2009;9:6913–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [45].Wu Y-H, Wu J-S. The influence of exercise training on heart rate variability (HRV) [in Chinese]. J Phys Educ Fu Jen Catholic Univ 2008;7:239–52. [Google Scholar]
- [46].Mehta AJ, Adam M, Schaffner E, et al. Heart rate variability in association with frequent use of household sprays and scented products in SAPALDIA. Environ Health Perspect 2012;120:958–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Palatini P, Julius S. The role of cardiac autonomic function in hypertension and cardiovascular disease. Curr Hypertens Rep 2009;11:199–205. [DOI] [PubMed] [Google Scholar]
- [48].Borchini R, Ferrario M. Job strain and heart rate variability. New evidence and new prospects. G Ital Med Lav Ergon 2012;34: 3 Suppl: 174–6. [PubMed] [Google Scholar]