

Abstract
Background:
The journey in the field of periodontics has destined from macrodentistry to microdentistry. The success of periodontal therapy always depends on better visual access and debridement which are prerequisites for achieving a clean and smooth root surface in attaining new attachment. Magnification is something which provides good hand-eye coordination resulting in better treatment outcomes. The aim of our study is to assess the effectiveness of magnification variable under a surgical operating microscope while performing root planing procedure.
Materials and Methods:
A randomized clinical trial was conducted on 45 patients who were diagnosed with mild-to-moderate chronic periodontitis and were treated under the surgical operating microscope with three different magnification variables (0.4, 0.6, and 1). Plaque index, gingival index (GI), and probing pocket depths (PPDs) were assessed from baseline to 4 weeks, whereas healing index was assessed after 2 weeks of root planing procedure.
Results:
The results of our study under the three magnification variables (0.4, 0.6 and 1) have shown no significant reduction in plaque or GI after 4 weeks of therapy. However, a significant reduction PPDs was observed after 4 weeks and improved healing index was observed after 2 weeks under all the three magnification variables with the variable 0.6 demonstrating more effective results.
Conclusion:
Even though all the three magnification variables have shown better treatment outcome and ergonomics, 0.6 magnification variable, i.e., ×3.5 – ×5, has demonstrated a more significant effect while performing root planing procedure.
Key words: Magnification, magnification variables, root planing, surgical operating microscope
INTRODUCTION
Periodontal diseases which are one among the various inflammatory conditions affecting the oral cavity happen to be one of the main reasons for tooth loss in the modern era. The literature search clearly states that periodontal disease involves a complex interaction between microorganisms and host responses leading to the destruction of attachment apparatus,[1] the ultimate paradigm of periodontal therapy lies in disrupting this host-microbial destruction and reducing the subgingival pathogens, thereby improving the overall oral health of the individual.[2] Periodontal therapy includes a variety of treatment modalities which are broadly categorized into nonsurgical and surgical phases. Nonsurgical therapy which forms the cornerstone of mechanical plaque control plays a crucial role in the maintenance of periodontal health.[3]
In general, any periodontal procedures are routinely carried out by conventional means that includes the performance of the procedures under a naked eye. Although regularly performed, it is not without limitations. However, its main limitation lies in the patient's position in the dental chair, as the procedures are time taking and require a lot of patience from the operator's side. Furthermore, tooth factors such as improper root anatomy and lack of proper vision to inaccessible areas might also lead to tissue trauma resulting in discomfort to the patient even.[4] It is clearly stated in the literature that diagnostic skills along with good visual access form the key criteria in the success of a periodontal treatment procedure by allowing a magnified view of the interproximal areas between the teeth, thereby resulting in a disease-free tooth surface facilitating new attachment.[5] Not only the success of treatment depends on a successful treatment plan but also the key to it lies in crucial diagnosis. Taking these factors into consideration, dentistry has evolved from conventional to that of advancements in the field wherein procedures are being performed under magnification.
As the literature search has also demonstrated positive outcomes such as less tissue trauma as a result of precise and controlled instrumentation, resulting in a better and faster wound healing, procedures under magnification are the need of the hour.[4,5,6,7] Not only do they account for the above-said benefits but also have tremendous advantages related to the work position of the clinician as the increased time involved in dental procedures subject the clinician to musculoskeletal disorders.[8] Above all, documentation in an accurate and proper way is the most important aspect of today's dentistry due to various medicolegal issues which can be achieved with procedures being done under magnification, especially the surgical operating microscope.[9] Taking these factors into consideration, as there is sparse literature regarding the periodontal procedures done under magnification, especially advocating under the surgical operating microscope, an attempt was made within this study to compare the treatment outcome of different magnification variables under the surgical operating microscope during root planing procedure in chronic periodontitis.
MATERIALS AND METHODS
Source of the data
This is a randomized, double-blind clinical trial wherein patients from the department of periodontics and implantology were recruited in this study. A total of 45 patients with age groups ranging from 25 to 55 years and affected by mild-to-moderate chronic periodontitis were enrolled in this study. Ethical clearance was obtained from the Institutional Ethics and Review Board with informed consent from the patient.
Selection criteria
The inclusion criteria comprised patients diagnosed with chronic moderate periodontitis (probing depth ≥5 mm) and who were systemically healthy with a minimum of 20 teeth in mouth and teeth with Grade I mobility. Patients with uncontrolled systemic diseases, physically and mentally challenged individuals, pregnant women and lactating women, patients with <20 teeth, teeth which are Grade II mobile, and smokers were excluded from the study.
Study design
The study design includes three different groups, namely Group A, Group B, and Group C.
Group A – Root planing under magnification variable 0.4 (×2.5)
Group B – Root planing under magnification variable 0.6 (×3.5)
Group C – Root planing under magnification variable 1 (×5.6).
Forty-five patients were included in the study. Scaling was performed for all the patients without using magnification. Periodontal parameters, i.e., plaque index (PI), gingival index (GI), and probing pocket depths (PPDs), were recorded and compared at the baseline and 4 weeks where early wound healing index was assessed after 2 weeks. However, root planing was performed under magnification assigning each group for each quadrant randomly.
Statistical analysis
All the data obtained after performing the clinical trial were computed and analyzed. Statistical analysis was done using one-way ANOVA test and Chi-square test. P < 0.05 was considered statistically significant for all the comparisons.
RESULTS
Plaque index (Loe and Silness)
The mean change in the PI from the baseline to 1 month was 0.86 ± 0.12 under 0.4 magnification variable. The mean change was 0.93 ± 0.20 and 0.73 ± 0.08 under variables 0.6 and 1, respectively. These reductions in plaque scores did not show any statistically significant difference between different magnifications (P = 0.59) [Table 1].
Table 1.
Comparison of change in plaque index scores under three different magnification variables
| Magnification variables | Mean±SD | P |
|---|---|---|
| 0.4 | 0.86±0.12 | 0.59 |
| 0.6 | 0.93±0.20 | |
| 1 | 0.73±0.08 |
P>0.05 (PI is not statistically significant). SD – Standard deviation; PI – Plaque index; P – Probability value
Gingival index (Silness and Loe)
The mean change in the GI from the baseline to 1 month was 0.89 ± 0.26 under 0.4 magnification variable. The mean change was 0.93 ± 0.06 and 0.93 ± 0.18 under variables 0.6 and 1, respectively. These reductions in scores did not show any statistically significant difference between different magnifications (P = 0.76) [Table 2].
Table 2.
Comparison of changes in the gingival index under three different magnification variables at the baseline and 4 weeks after the root planing
| Magnification variables | Mean difference±SD | P |
|---|---|---|
| 0.4 | 0.89±0.26 | 0.76 |
| 0.6 | 0.93±0.06 | 0.76 |
| 1 | 0.93±0.18 | 0.76 |
P>0.05 (GI is not statistically significant). GI – Gingival index; SD – Standard deviation; P – Probability value
Probing pocket depths
The mean change in the GI from the baseline to 1 month was 0.89 ± 0.26 under 0.4 magnification variable [Figure 1]. The mean change was 0.93 ± 0.06 and 0.93 ± 0.18 under variables 0.6 and 1, respectively. These reductions in probing depths showed a statistical significant difference between different magnifications (P = 0.037) [Table 3] and [Figure 2].
Figure 1.
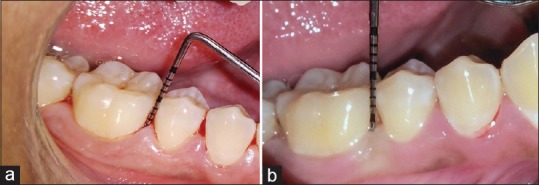
(a) Preoperative photograph of 46 with a pocket depth of 7 mm measured under magnification variable 0.4; (b) Postoperative photograph of 46 with reduction of probing depth to 3mm after 4 weeks of root planning
Table 3.
Comparison of changes in probing depths under three different magnification variables at the baseline and 4 weeks after the root planing
| Magnification variables | Mean difference±SD | P |
|---|---|---|
| 0.4 | 0.22±0.02 | 0.03 |
| 0.6 | 0.71±0.06 | 0.03 |
| 1 | 0.48±0.08 | 0.03 |
P<0.05 (PPDs are statistically significant). PPDs – Probing pocket depths; SD – Standard deviation; P – Probability Value
Figure 2.
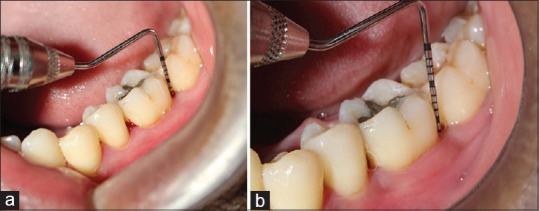
(a) Preoperative photograph showing probing pocket depth of 7 mm in the distal aspect of 36 under magnification variable 0.6; (b) Preoperative photograph showing the reduction of probing pocket depth of 3 mm in the distal aspect of 36; 4 weeks after root planing procedure under magnification variable 0.6
Intergroup comparisons in the reduction of PPDs between 0.4 and 0.6 show the mean difference of 0.15, between 0.4 and 1, it shows 0.07, and between 1 and 0.6, it shows the mean difference of 0.07 [Figure 3]. A significant reduction was observed under the magnification variable 0.6 with significant P = of 0.28 [Table 4].
Figure 3.
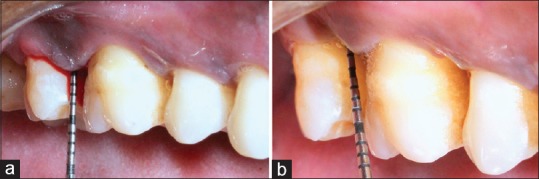
(a) Preoperative photograph showing probing depth of 7 mm of 16 under magnification variable 1; (b) Postoperative photograph showing probing depth of 3mm under magnification variable 1; 4 weeks after root planning
Table 4.
Intercomparison of probing depths under three different magnification variables at the baseline and 4 weeks after the root planing
| Dependent variable | Magnification variables | Magnification variables | Mean difference | P |
|---|---|---|---|---|
| Probing depth | 0.4 | 0.6 | 0.15208 | 0.028 |
| 0.4 | 1 | 0.07708 | 0.388 | |
| 0.6 | 1 | 0.07500 | 0.408 |
P<0.05. P – Probability value
Wound healing index (watchell)
Healing index was measured 2 weeks after root planing. About 42.2% of the individuals have shown the healing index score of 1 under magnification 0.4. Better healing score, i.e., Score 1, was observed under magnification variable 0.6 in 55.5% of the individuals and 24.4% showed Score 1 under variable 1. The healing index is statistically significant under magnification variable 0.6 with P = 0.023 [Table 5].
Table 5.
Distribution of the Early Healing Index at the treated sites after 2 weeks of treatment
| Magnification variable | Score 1 (%) | Score 2 (%) |
|---|---|---|
| 0.4 | 19 (42.2) | 26 (57.7) |
| 0.6 | 25 (55.5) | 20 (44.4) |
| 1 | 11 (24.4) | 34 (75.5) |
P<0.05 (P - 0.023). P – Probability value
DISCUSSION
Periodontal diseases which are a result of the host-microbial complexes are the most common cause of tooth loss. Over decades, literature has shown that the elimination of necrosed cementum and bacterial endotoxins from the root surface are the key factors for a successful periodontal treatment outcome. Even though complete elimination of these endotoxins from the root surface has always remained as a matter of debate, adequately planed root surface has shown the change in the root topography which affects the attachment of bacteria followed by positive treatment outcome.[3] The success of periodontal therapy always depends on better visuality for proper debridement which is a prerequisite in achieving a clean and smooth surface that is essentially required for new attachment to take place.[3,5]
Periodontics, a rapidly evolving field of dentistry, has shown its transition from macrodentistry to a high precision microdentistry wherein the tissue trauma is precise and comfort of the patient as well as the clinician is the subject of interest. Advanced research has left today's periodontist with wide varieties of magnification systems to choose which range from simple to compound loupes and a vast variety of surgical microscopes. The literature has shown few limitations while performing procedures under loupes such as eyestrain, as a result of which eyes are subjected to fatigue as they need to converge to view an image.[9]
The measures of magnification are the power of the eyepiece, magnification changing factor, focal length of binoculars, and focal length of the objective lens. The power of eyepiece ranges from ×6 to ×12 wherein a surgical operating microscope of ×10, with the variable focal length of objective lens ranging from 300 to 400 mm was used in this study. The binocular focal length of surgical operating microscope used in this study was 170 mm. Our total magnification ranged from ×1.7 to ×10, wherein magnification increases with increase in the magnification factor and a decrease in the field of view. An interesting factor that needs to be taken into consideration is that the magnification increases with decreased field of view when the focal length is increased which holds good for the procedures that require more focus which is usually the case in isolated teeth.[9]
A good periodontal treatment could be achieved at a total magnification range of ×2.5–×6.8. A magnification of ×2 (magnification variable of 0.4) provides more field of vision which will be almost similar to a conventional procedure, whereas ×6 (magnification variable 1) shows a restricted field which will be more comfortable for localized treatment procedures such as localized gingival recessions, crown lengthening, and localized flap surgeries. An average magnification of ×3.5 (magnification variable 0.6) provides a good working field wherein a complete quadrant can be viewed along with the interproximal areas and even the field of view is not restricted to a fixed point. Thus, the magnification variable should be the dictum of the clinician during various types of periodontal procedures.[9]
To our knowledge, there is only one study evaluating the efficacy of root planing done under the surgical microscope, although the literature on scaling and root planing under magnifying loupes with a magnification ranging from ×2.5 to ×3.4 exist. Hence, our present study aimed to evaluate the efficacy of root planing and operators' ergonomic benefit under the surgical microscope with different magnifications ranging from ×2.5 (magnification variable 0.4) to ×5.6 (magnification variable 1).
Fifteen patients were assigned to each group of three different magnification variables. The results of the present study have shown the reduction of PI with a mean difference of 0.9 under magnification variable 0.6 and reduction of GI with a mean difference of 0.9 under magnification variables 0.6 from the baseline to 4 weeks of reevaluation which showed no clinical significance. This result obtained in the study was similar to the results obtained in a study conducted by Mohammed, Nandini in 2018, and Corbella et al. in 2018 which showed no clinical significance in reduction of plaque and GI between the groups treated with magnification (×2.5 loupes) and without magnification.[5,10]
On the other hand, the evaluation of PPDs after root planing under the surgical microscope was the first attempt made from our side. The reduction of probing depths has shown clinical significance after 4 weeks of therapy. As it is clearly stated in the literature that better the magnification better will be the visual acuity and treatment outcome.[9] These results in our present study, wherein the probing depth reduction showed much clinical significance under magnification variable 1 (×5.6) than 0.4 (×2.5) 0.6 (×3.4), were in accordance to the above statement.
When the use of a surgical microscope was taken into consideration, the magnification levels of ×10 with a variable of 0.6 (×3.5) have shown as a significant improvement in the quality of treatment [Figure 1 and 2]. However, we can very well infer from the findings of our study that among the three magnification variables that were implicated in our study, 0.4 has more field of vision and 1 provides a restricted vision. On the other hand, ×0.6 variable is effective in terms of ergonomics, the comfort of operator as well as the quality of treatment outcome [Figure 4].
Figure 4.

(a) Postoperative photograph showing probing depth of 3 mm under magnification variable 1; 4 weeks after root planning; (b) Photograph showing the straight posture of the operator while performing the procedure resulting in improved ergonomics
As well stated in the literature that surgical operating microscope has the advantage of operator comfortability, thereby saving time. One of the interesting features of our study is, the operator felt that procedure under the microscope is a steep learning curve, thereby demanding time and patience more as the operator needs to get habituated to a fixed position while working.[10] Hence, the superior effects of magnification could be best achieved when the usage of magnification is advocated in clinical practice as early as possible.
CONCLUSION
As ergonomics is one of the most important principles that needs to be implicated in dental practice, the use of a surgical microscope can definitely overcome the limitations encountered in performing the procedures in a conventional way.[11] However, more randomized clinical trials could help to better understand the benefits of a surgical microscope than a loupe in performing scaling and root planing with improved visual acuity and better ergonomics to the clinician along with less pain perception, thereby enhancing the comfort levels of the patient.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Page RC, Kornman KS. The pathogenesis of human periodontitis: An introduction. Periodontol 2000. 1997;14:9–11. doi: 10.1111/j.1600-0757.1997.tb00189.x. [DOI] [PubMed] [Google Scholar]
- 2.Claffey N, Polyzois I, Ziaka P. An overview of nonsurgical and surgical therapy. Periodontol 2000. 2004;36:35–44. doi: 10.1111/j.1600-0757.2004.00073.x. [DOI] [PubMed] [Google Scholar]
- 3.Tanwar J, Hugund SA, Dodani K. Non surgical periodontal therapy: A review. J Oral Res Rev. 2016;8:39–44. [Google Scholar]
- 4.Low SB. Clinical considerations in nonsurgical mechanical therapy. Periodontol 2000. 1995;9:23–6. doi: 10.1111/j.1600-0757.1995.tb00053.x. [DOI] [PubMed] [Google Scholar]
- 5.Parvez MF, Manjunath N. Comparative evaluation of conventional scaling with and without magnification loupes. IOSR J Dent Med Sci. 2018;17:73–6. [Google Scholar]
- 6.Yadav VS, Salaria SK, Bhatia A, Yadav R. Periodontal microsurgery: Reaching new heights of precision. J Indian Soc Periodontol. 2018;22:5–11. doi: 10.4103/jisp.jisp_364_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kapadia JA, Bhedasgoankar SY, Bhandari SD. Periodontal microsurgery: A case report. J Indian Soc Periodontol. 2013;17:790–2. doi: 10.4103/0972-124X.124511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Valachi B, Valachi K. Preventing musculoskeletal disorders in clinical dentistry: Strategies to address the mechanisms leading to musculoskeletal disorders. J Am Dent Assoc. 2003;134:1604–12. doi: 10.14219/jada.archive.2003.0106. [DOI] [PubMed] [Google Scholar]
- 9.Tibbetts LS, Shanelec DA. A review of the principles and practice of periodontal microsurgery. Tex Dent J. 2007;124:188–204. [PubMed] [Google Scholar]
- 10.Farook SA, Stokes RJ, Davis AK, Sneddon K, Collyer J. Use of dental loupes among dental trainers and trainees in the UK. J Investig Clin Dent. 2013;4:120–3. doi: 10.1111/jicd.12002. [DOI] [PubMed] [Google Scholar]
- 11.Mamoun J. Use of high-magnification loupes or surgical operating microscope when performing prophylaxes, scaling or root planing procedures. N Y State Dent J. 2013;79:48–52. [PubMed] [Google Scholar]