

Supplemental Digital Content is available in the text
Keywords: Endometriosis, Non-hormonal therapy, Pelvic pain, Subfertility
Abstract
Objective:
Endometriosis is a common gynecologic disease that frequently leading to chronic pelvic pain, severe dysmenorrhea, and subfertility. As first-line hormonal treatment can interfere with ovulation and may cause recurrent pelvic pain, exploration of new non-hormonal therapeutic approaches becomes increasingly necessary. This review aimed to evaluate the pre-clinical and clinical efficacy and safety of non-hormonal treatment for endometriosis
Data sources:
Databases including PubMed, Embase, Cochrane Library, SINOMED, ClinicalTrials.gov, and Google Scholar were searched up to October 2019, using search terms “endometriosis” and “non-hormonal therapy.”
Study selection:
Twenty-four articles were reviewed for analysis, including nine animal studies and 15 human trials; all were published in English.
Results:
Twenty-four articles were identified, including 15 human trials with 861 patients and nine animal studies. Some agents have been evaluated clinically with significant efficacy in endometriosis-related pelvic pain and subfertility, such as rofecoxib, etanercept, pentoxifylline, N-palmitoylethanolamine, resveratrol, everolimus, cabergoline (Cb2), and simvastatin. Other drugs with similar pharmacological properties, like parecoxib, celecoxib, endostatin, rapamycin, quinagolide, and atorvastatin, have only been tested in animal studies.
Conclusions:
Clinical data about most of the non-hormonal agents are not sufficient to support them as options for replacement therapy for endometriosis. In spite of this, a few drugs like pentoxifylline showed strong potential for real clinical application.
Introduction
Endometriosis is one of the most common benign gynecological diseases in pre-menopausal women, since approximately 10% to 15% of reproductive-aged women experience pelvic endometriosis.[1] It is characterized by pelvic pain, dysmenorrhea, dyspareunia, and infertility. The influence of endometriosis on infertility cannot be ignored, as it is found in 33% of infertile women.[2] As the American Society for Reproductive Medicine proposed, endometriosis should be considered a chronic disease that requires lifelong treatment, with the goal of using medical treatment as much as possible and avoiding invasive procedures such as surgery.[3]
The pharmacological therapy consists of hormonal and non-hormonal agents. The well-known hormonal therapy includes combined oral contraceptives (COC) and the levonorgestrel-releasing intra-uterine system. As a second line, desogestrel progestin-only pills, etonogestrel implants, and gonadotrophin-releasing hormone analogs, and dienogest are available.[4] These agents have been reported to ameliorate pain and reduce disease recurrence. However, because these drugs may interfere with ovulation during the post-operative period that is critical for conception, their use for treating endometriosis has been a controversy. Another shortcoming of hormonal therapy is long-term use and high recurrence rate after discontinuation of treatment. Non-hormonal drugs are receiving attention these days because of their protection of ovulation and the potential to eradicate lesions or alleviate symptoms.
Given the complex pathogenesis of endometriosis, non-hormonal drugs could be categorized into different types. A large number of these non-hormonal drugs target angiogenesis, which is a pre-requisite for endometriosis development according to basic studies. As numerous cytokines and inflammatory factors were suggested to facilitate the development of ectopic endometrial tissues, the therapeutic potential of non-steroidal anti-inflammatory drugs (NSAIDs) and tumor necrosis factor (TNF)-α antagonist has been assessed. Additionally, some natural components have been tested for their potential effects in endometriosis.
The safety and efficacy of most non-hormonal drugs have not been thoroughly evaluated through large clinical trials. The lack of high-quality evidence has left clinicians in the dark when choosing the most suitable treatment. This paper aimed to investigate the effect of non-hormonal therapy approaches on endometriosis that have been tested in clinical trials and explore their value for being implemented in clinical practice or the best combination usage with hormonal drugs.
Literature search strategy
PubMed, Embase, Cochrane Library, SINOMED, ClinicalTrials.gov, and Google Scholar were searched. Additionally, references of each article that met the criteria with regard to the target population and therapy were included. We assessed all studies that evaluated any aspect of non-hormonal therapy for endometriosis using the searched terms “endometriosis” and “non-hormonal therapy.” We included in vitro experiment studies in which animal models were treated with new non-hormonal drug and clinical trials recruiting patients who have been diagnosed with endometriosis according to the criteria of the American Fertility Society and received non-hormonal drug therapy.[5] Then, a final selection was made by FYC and ZXG after reading the full text of included articles. We excluded duplicate studies and removed publications that were not in English. Potentially eligible articles were checked by title and abstract by FYC. Then, a final decision was made by FYC and ZXG after reading the full text of the articles. Studies were independently evaluated by two reviewers (FYC, ZXG). Data on study design, study population, and therapy were extracted. Institutional review board approval was not necessary for this review. The quality of each study was assessed independently by two reviewers (FYC, ZXG), with discussion with a third reviewer (XW) in cases of disagreement. For clinical trials, reviewers used a tool adapted from the Cochrane Risk Of Bias Assessment Tool.[6] The clinical studies consist of randomized controlled trials (RCTs), single intervention study, and retrospective case-control study. Quality assessment measures included evaluation of selection of cohorts, assessment of exposure and outcome, and consideration of confounding variables. Study quality was graded as no risk, moderate risk, high risk, and critical risk of bias using the adapted tool. The outcomes measured varied across the studies, such as endometriotic area or volume, pain scores, and birth rate. Many studies only documented a measure of the targeted index but did not document the odd risk or relative risk. Visual analog score (VAS) of pelvic pain within the confined populations was the most common outcome across studies. During the literature search, 49 articles were identified. After the initial screening, three duplicates, four unrelated documents, and four non-English studies were excluded. In addition, 14 articles with non-available full text were excluded. Twenty-four articles met the inclusion criteria for analysis, including nine animal studies and 15 human studies. Figure 1 shows the selection process. The results are presented by drug category and the related analyses are concluded both in animal studies [Table 1] and clinical trials [Table 2]. The risk of bias for clinical trials is shown in Supplementary Table 1.
Figure 1.
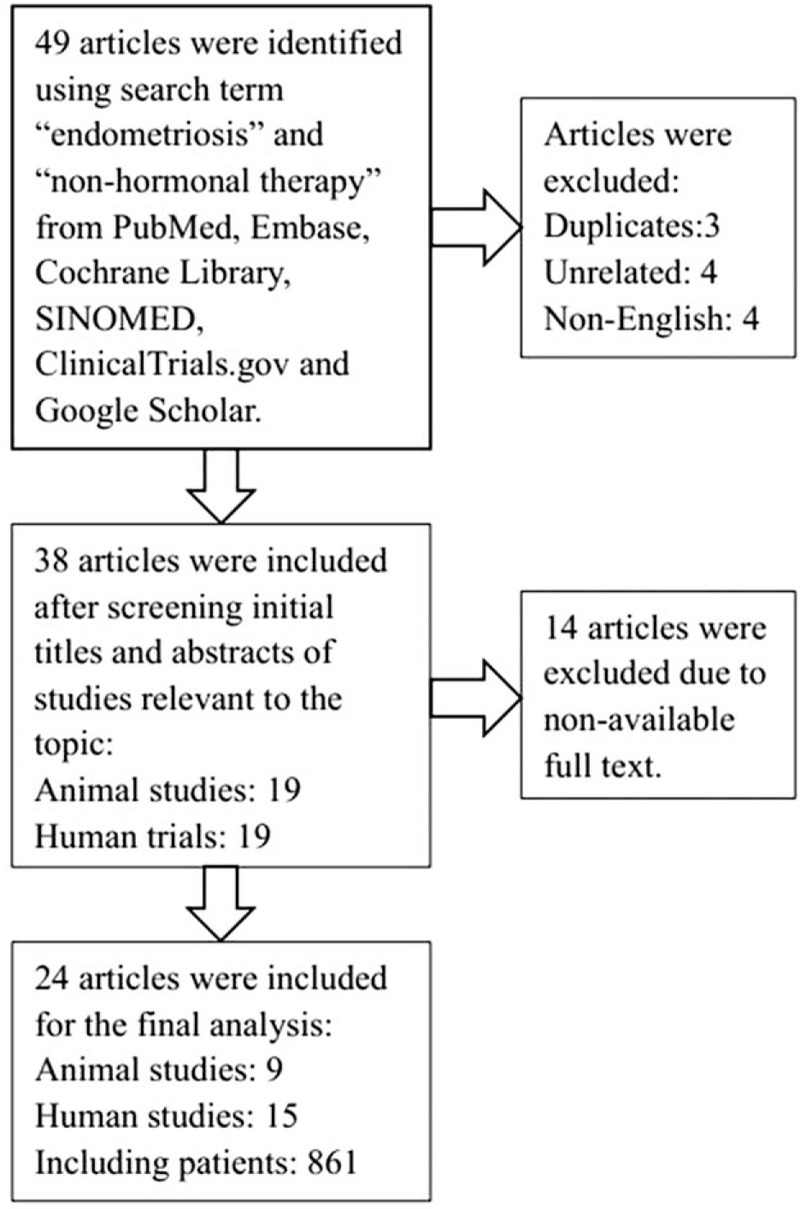
Flow diagram for study selection.
Table 1.
Studies of agents tested in endometriosis induced in animal models but not in humans.

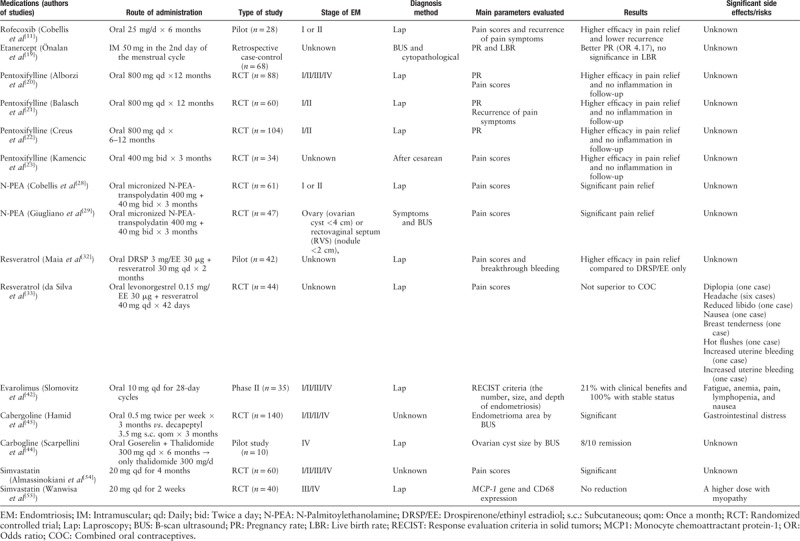
Table 2.
Studies of agents tested in human trials.
NSAIDs
Cyclooxygenase (COX), as a synthetic enzyme for pain mediators, plays a positive role in the development and progression of endometriosis.[7] With additional benefits in relatively sparing the gastrointestinal side effects, COX-2 specific inhibitors were used to alleviate pain and inflammation, such as post-surgery pain, headache, and toothache. The reduction in endometriosis-relevant pain and the anti-proliferative capacity of some COX-2 specific inhibitors have been tested in vivo and in vitro.
Parecoxib
Machado et al[8] have found in an experimental rat model with autotransplanted endometriotic tissue that 3 mg·kg−1·d−1 of parecoxib could inhibit the growth of endometriotic tissue with 80% reduction in volume compared to controls. The decreased expression of vascular endothelial growth factor (VEGF) and polyclonal antibody against VEGF receptor 2 (VEGFR2; Flk-1) and the reduced density of von Willebrand factor-positive vessels in endometriotic tissue indicate that the suppression effect of parecoxib could be achieved through its anti-angiogenic activity.
A mouse model of the endometrium induced by grafting uterine tissue samples to the peritoneum was used to test the effect of telmisartan combined with parecoxib on lesions. Significant reduction in the volume of induced endometrium was observed in the combination therapy compared with single treatment with telmisartan or parecoxib, though they also exhibited inhibitory effect on the growth of endometriotic tissue.[9] In immunohistochemical analysis, the combination therapy was associated with less proliferating Ki67-positive cells and more apoptotic cleaved caspase-3-positive stromal cells as well as decreased microvessel density in the lesions. However, to date, there are limited human studies about the application of parecoxib in clinical environment.
Rofecoxib
Rofecoxib resulted in decreased size of the implanted endometriotic tissue in the same degree compared with leuprolide in a rat model (62.4% vs. 64.3%).[10] The regression and atrophy of induced endometriosis were documented in histologic examination, accompanied by decreased VEGF levels of lesions compared with controls.
A pilot study has evaluated the effect of rofecoxib on endometriosis-induced pelvic pain in 28 women who underwent conservative surgery. Pain symptom scores in 28 patients with stage I or stage II endometriosis were recorded before and after 6 months of treatment, through which rofecoxib demonstrated a higher effect on endometriosis (dysmenorrhea 8:3; dyspareunia 7.5:1.5; and chronic pelvic pain 6:1.5). Additionally, no pain recurrence occurred in the rofecoxib group, while two of 12 in the controls had pain recurrence.[11] However, rofecoxib has been withdrawn from the market because of severe cardiovascular effects in long-term users.[12]
Celecoxib
Y-box-binding protein 1 (YB-1) is a member of DNA- and RNA-binding protein superfamily, which is recently reported to be highly expressed in endometrial epithelial cells of endometriosis. OSU-03012, a celecoxib analog, was demonstrated to inhibit the process of endometriosis by affecting YB-1 related signaling pathway in vitro and in vivo.[13] With exposure to different concentrations of OSU-03012, the proliferation of 12Z human endometriotic epithelial cells was hindered. In the mouse model of Silveira et al,[13] reduced volume of implanted endometriotic lesions was recorded in 100 mg/kg OSU-03012-treated mice, showing 56.4% of shrinking tissue after a 2-week treatment, while the lesion size enlarged by 44.7% in controls. Data on the application of OSU-03012 in humans are still lacking.
A mouse model showed that celecoxib and rosiglitazone, combined or separately, have a therapeutic effect on overall endometriotic growth.[14]
TNF-α antagonist
TNF-α is a secretory factor of active macrophages known to have potent inflammatory cytotoxic and angiogenic characteristics. Several studies have demonstrated higher concentration of TNF-α in the peritoneal fluid of women with endometriosis than those without, as well as a direct correlation between TNF-α level and disease severity.[15,16] Thus, TNF-α blockers were suggested as a promising novel therapy for endometriosis.
Etanercept
A rat model with homologous transplanted endometriotic tissue was used to determine the anti-TNF-α activity of etanercept, a group of immunoglobulin coupled with TNF-α receptor.[17] Moreover, a 31.8% decrease in endometriosis volume was observed in etanercept-treated rats with statistically significant reduction in histologic proliferation scores.
Besides, elevation of TNF-α in peritoneal fluids is associated with infertility induced by endometriosis.[18] A retrospective case-control study was conducted in 68 infertile patients who had endometrioma diagnosed by ultrasound imaging and confirmed by cytopathological examination during oocyte retrieval. Of these patients, 19 patients who were administered with 50 mg of etanercept intramuscularly on the second day of their previous menstrual cycle and then treated by assisted reproduction technique demonstrated statistically higher rate of pregnancy. Although those women did not reach statistically significant elevation in live birth rate (LBR) (P = 0.075), a two-fold increase in LBR was recorded.[19] Another problem in this trial was the lack of information regarding the stages of endometrioma and surgery history.
Pentoxifylline
Pentoxifylline is a methylxanthine with anti-inflammatory property, acting as a phosphodiesterase inhibitor, that has been proposed for treating endometriosis. Cerebrovascular and peripheral vascular diseases, as well as other conditions with defective microcirculation, have been the indication of pentoxifylline treatment for many years.
No statistical significance was observed in overall rates and recurrence rate of pain symptoms in a RCT recruiting 88 infertile patients with endometriosis stages III/IV. The participants received 800 mg pentoxifylline daily and were followed for 12 months. The negative results may be related to high stages of most patients as well as the small sample size.[20] Another study recruited 60 endometriosis-related infertile women with stage I or II and documented that the pentoxifylline-treated group has good results, in which 31% of patients conceived during the 1-year follow-up period compared with 18.5% pregnancy rates in the placebo group. However, the data did not reach statistical significance because of a limited sample size. Furthermore, 40% to 45% of them had additional infertile factors; however, after controlling for all these confounding factors, no significant effect on pregnancy rate was recorded.
Another prospective RCT of the effect of pentoxifylline only comprised infertile women with asymptomatic minimal or mild endometriosis. The results are similar (31% vs. 18.5%), which showed no significant difference in the overall pregnancy rate between the intervention group and the placebo group.[21] To confirm the argument, more rigorous trial eliminating confounding infertile causes was performed, showing a two-fold increase of pregnancy rate in the pentoxifylline group as recorded in controls.[22]
On the basis of anti-inflammatory property of pentoxifylline, a prospective RCT was designed to test the effect of oral pentoxifylline combined with laparoscopic surgery on pelvic pain.[23] Reduction in pain scores was documented most significantly in the second and third months since treatment with 400 mg of pentoxifylline twice a day. No evaluation of pain scores in long-term use was the limitation of the study.
N-palmitoylethanolamine
N-palmitoylethanolamine (N-PEA) is a structural analog of anandamide with anti-inflammatory, immunosuppressive, analgesic, neuroprotective, and antioxidant effects. It inhibits mast cell activation, blocking out the crosstalk between mast cells and nociceptive nerve fibers peripherally. It is also able to downregulate microglial cell behaviors and thus reduces associated central pain hypersensitization.[24,25] Besides endometriosis, N-PEA has been successfully tested for reducing pain due to chronic lumbosciatalgia.[26]
Polydatin, a natural glucoside of resveratrol and a phytoalexin polyphenolic compound found in various plants, such as grapes, berries, and peanuts, downregulates the inflammatory response by inhibiting the synthesis and release of proinflammatory mediators, inducing mast cell degranulation, and modifying eicosanoid synthesis. A nude model has proved its anti-inflammatory activity.[27]
An RCT including 61 patients indicates that the association between micronized N-PEA and transpolydatin is effective in the management of pelvic pain (pelvic pain, dysmenorrhea, and dyspareunia) related to endometriosis after laparoscopy (16/21 vs. 8/20), especially in pelvic pain.[28] Meanwhile, celecoxib decreased pelvic pain more effectively than the association with micronized N-PEA and transpolydatin or placebo (P < 0.001).
In another clinical trial, the efficacy of N-PEA plus transpolydatin was tested in 47 women with endometriosis (ovarian cyst <4 cm or rectovaginal septum nodule <2 cm in instrumental evaluation) before surgery.[29] They were divided into recto-vaginal endometriosis group and ovary endometriosis group. In a 3-month follow-up of their symptoms, chronic pelvic pain, dysmenorrhea, and dyschezia were all ameliorated and significantly associated with time. The effect was more apparent in dysmenorrhea of ovary endometriosis and dyschezia in recto-vaginal endometriosis.
Natural agents
Resveratrol
Resveratrol (3,5,4′-trihydroxystilbene) is a natural phytoestrogen in plants, such as dark grapes and blueberries, synthesized after exposure to ultraviolet radiation. Given its known anti-proliferative activity, various studies were designed to test its effect on endometriosis in vitro and in animal models.[27,30,31]
A mouse model with endometriosis induced by intraperitoneal injection of human endometrial tissue showed an 80% decrease of volume when treated with 6 mg of resveratrol for 18 to 20 days.[27] Ectopic implants by homologous transplantation in mice displayed similar results.[30] In a stepwise manner, some studies showed promising outcomes of the potential usage of resveratrol in women with endometriosis. A pilot open-label trial with 42 patients demonstrated statistically more significant reduction in pelvic pain scores when treated by resveratrol (30 mg/d) combined with drospirenone (DRSP)/ethinyl estradiol (EE) (3 mg/3 μg), compared to the same dose of DRSP/EE treatment alone (pain score: 0.2 vs. 2.1, baseline = 3). Besides, the combination therapy led to complete resolution of dysmenorrhea in 82% of patients, while the single COC group had consistent breakthrough bleeding.[32] After a 2-month treatment, the ectopic endometrium was biopsied via laparoscopic surgery and showed significantly lower expression of aromatase and COX-2 activity, confirming the anti-inflammatory property of resveratrol. No findings about the effect of resveratrol on subsequent pregnancy were reported.
However, a rigorous RCT argued against the benefits of resveratrol. The trial recruited 44 women with endometriosis and was followed for 42 days, indicating no superiority of resveratrol (40 mg/d) + COC therapy (DRSP 3 mg/EE 3 μg) on pain relief compared to COC alone.[33] Despite the negative results, the bias related with the small sample size and short medication time should not be neglected. Some side effects of resveratrol have also been pointed out, such as diplopia (one case), headache (six cases), reduced libido (one case), nausea (one case), breast tenderness (one case), hot flushes (one case), increased uterine bleeding (one case), and increased uterine bleeding (one case). Thus, the safety of resveratrol may need further investigation.
Epigallocatechin-3-gallate (EGCG)
Ricci et al[30] stated that in an endometriosis mice model induced by grafting uterine horns into the peritoneum, treatment with resveratrol or EGCG resulted in shrinkage of endometriotic tissue as well as the inhibited proliferation of endometriotic stromal cells immunochemically. In the same study, human endometrial epithelial cells (EECs) were also cultured in vitro, showing that both resveratrol and EGCG could cause the apoptosis of human EECs through the TdT-mediated dUTP nick-end labeling technique.
Green tea EGCG has been indicated to be effective in inhibition of VEGF expression and thus angiogenesis in endometriosis of an experimental endometriosis model in mice, with significant suppression in the growth of implanted endometriotic tissue.[34,35] Furthermore, EGCG would not affect blood vessel development in ovarian follicles.[34,35] Although there are no data of human trials, a phase II double-blind RCT is currently underway to evaluate the efficacy of 3-month pre-surgical administration of green tea extract (400 mg, twice per day) in patients with endometriosis (NCT02832271). However, poor bioavailability prevented the utilization in humans. A new prodrug, EGCG octaacetate, synthesized to increase the serum level and enhance EGCG stability, may shed light on clinical practice, since it is effective in inhibiting the growth of transplanted endometriosis in a mouse model.[36]
Anti-angiogenesis
Endostatin
Among other anti-angiogenic agents, endostatin, a proteolytic fragment of collagen XVIII, significantly suppressed the growth of endometriotic implants in mice possibly through inhibition of VEGF expression.[37–39] Jiang et al[37] used severe combined immunodeficient mice whose peritoneum was transplanted with human eutopic endometriotic tissue and treated with 2 mg·kg−1·d−1 of recombinant human endostatin YH-16 intraperitoneally. The microscopic examination showed decreased volume of the endometriotic tissue in the endostatin-treated group compared to the control group, with consistent results in hematoxylin-eosin staining and immunochemistry showing decreased microvessel density and lower VEGF expression.[37] A Korean study[40] showed a negative correlation of serum endostatin levels with the development of endometriosis, specifically in early-stage endometriosis patients compared with women without endometriosis, which provides support for the performance of human trials in some degree.
Rapamycin
As a drug targeting the mammalian target of rapamycin pathway to control the cell cycle, cell size, translation initiation, and transcription, rapamycin has aroused interest as a new therapeutic approach in many tumors including endometriosis. The activity of rapamycin in the reduction of implanted endometriosis has been tested and backed by some mice models.[41] Besides, the activity of an oral analog of rapamycin, everolimus, has been assessed in an open-labeled phase 2 study.[42] The study enrolled 35 patients with measurable recurrent endometriosis, who had failed at least one and no more than two prior chemotherapeutic regimens. All these patients had prolonged stable disease status, and 21% of them had a confirmed clinical benefit response at 20 weeks of therapy, indicating an encouraging prospect for clinical administration.
VEGF inhibition
The growth of endometriotic tissue in rich vascularized area implies the role of angiogenesis in the pathogenesis of endometriosis.[43] On the basis of a particularly high VEGF expression in endometriomas, therapy targeting VEGF has been evaluated in a series of recent studies.
Cabergoline
One of the suggestions is that dopamine agonists, such as Cb2, have potential in the inhibition of neoangiogenesis because of its explicit preventive activity in VEGF-VEGF receptor binding.[43] Scarpellini et al[44] recruited ten women with relapsing stage IV endometriosis and provided them with 300 mg/d of thalidomide for 6 to 14 months following 6 months of treatment of goserelin combined with 300 mg/d of thalidomide. None of them complained of endometriosis relapse in the follow-up.
A randomized cohort study with 140 patients was carried out to compare the effect of Cb2 on endometriosis with luteinizing hormone releasing hormone (LHRH).[45] The cut-off value was more than 25% of the reduction in the mean endometrioma diameter. A total of 64.7% of patients who were administered Cb2 met the requirement, compared against only 21.7% in the LHRH group (P < 0.05%). Even with the labels open to both clinicians and patients, ultrasound measures ensured outcomes with some degree of objectivity. Side effects of the new drug therapy should be evaluated before it becomes a new first-line therapy. However, one of the most common adverse events, gastrointestinal symptoms, appeared with higher rates in the Cb2-treated group than in the decapeptyl-treated group (12.5% vs. 0). Other side effects of Cb2, such as cardiac valve regurgitation and metabolic disorders, have largely prevented its clinical usage.
Non-ergot-derived dopamine agonists – quinagolide
Quinagolide is a non-ergot-derived selective D2 dopamine receptor agonist with fewer side effects than Cb2 and does not interfere with pregnancy. Thus, the potential use of quinagolide has been tested in a mouse model with ectopic human endometriotic tissue grafted on peritoneum.[46] The authors found that quinagolide was equally effective as Cb2 in decreasing the size of the endometrioma (39.5% vs. 45.8%, P > 0.05) as well as the expression of VEGF and VEGFR2. As quinagolide is not derived from ergot, it does not produce side effects of ergot derivatives, such as cardiac valve regurgitation. Moreover, it has a much shorter life than carbegoline, making it an attractive alternative to Cb2 in women who wish to become pregnant shortly after the treatment. Notwithstanding, the absence of clinical trials prevents the application of quinagolide in real clinical environment. A phase II clinical trial of 72 patients with endometrioma, deep infiltrating endometriosis, and adenomyosis, which compares the effect of quinagolide in a dose of 1080 μg and placebo, will be finished on November 2020.[47]
Statins
Atorvastatin
Besides the known lipid-lowering activity by inhibition of 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA) reductase, statins are also capable of inhibiting angiogenesis and cell proliferation in the development of endometriosis-like tissue, as tested in vitro and in vivo.[48–50] A rat model study induced by ligation of uterine horns demonstrated 68.2% regression of endometriotic implant area with prescription of atorvastatin at 2.5 mg·kg−1·d−1.[51] A randomized cohort trial with an estimated enrollment of 44 participants in 2008, which determined to compare the effect of atorvastatin, oral contraceptive, or COC and atorvastatin in pain relief and inflammatory status in surgically confirmed endometriosis, is still ongoing.[52]
Simvastatin
Simvastatin is a cholesterol-lowering drug that acts by inhibiting HMG-CoA reductase,[53] resulting in a decrease in mevalonate, a precursor of cholesterol and monocyte chemoattractant protein-1 (MCP-1), which is an important peritoneal inflammatory factor and stimulates the process of endometrial adhesion and proliferation, as well as neovascularization. Bruner-Tran et al[54] also found dose-dependent effect of simvastatin in inhibiting the proliferation of endometrial implants in a nude mouse model that was established by giving external estradiol. Evidence is scarce in clinical environment. However, in a randomized study consisting of only 60 patients with surgically confirmed endometriosis, no significant difference was detected in pain scores of simvastatin-treating patients, relevant to dyspareunia, dysmenorrhea, and pelvic pain, and those of gonadotropin-releasing hormone agonists users in a follow-up of 16 weeks.[55] However, none of the patients accepted second-look laparoscopy to evaluate the size and number of endometriotic lesions after the medication. In a more recent RCT including 40 endometriosis patients, simvastatin was given at a dose of 2 weeks before they received the surgery. The MCP-1 gene and CD68 expression were detected with no significant reduction compared to the no-treated group. It might indicate that a higher dose was needed to take effect, but it would increase the risk of myopathy.[56] To explore further the usage of simvastatin, larger and rigorous clinical trials are awaited.
Rosiglitazone
The peroxisome proliferator-activated receptors (PPARs) ligand rosiglitazone, a known drug for diabetes mellitus, has been shown to have anti-angiogenesis ability through ligand-induced apoptosis in breast cancer.[57] Blitek et al[58] demonstrated that the activation of PPARs affected the expression of genes involved in amino acid and glucose transport, prostaglandin and cytokine synthesis, angiogenesis, and apoptosis in the porcine endometrium. The inhibitory effect for the establishment and development of endometriosis has been illustrated in a rat model with autografted lesions.[59] Besides, another mouse model showed that rosiglitazone did not have any negative effects on reproduction and offspring delivery.[14] Moreover, the safety of rosiglitazone on fertility has been demonstrated in a baboon endometriosis model and it has no effect on the menstrual cycle.[60]
However, Pich et al[61] showed that PPARγ agonist rosiglitazone could activate the proliferation of human metastatic melanoma cells by inducing the intracellular paracrine signaling. Thus, its application potential in real clinical environment was doubted.
Discussion and conclusions
The traditional hormonal therapy for endometriosis has been reported to be ineffective in a group of patients as well as interfering with ovulation. For those who are unresponsive or show unacceptable side effects to hormonal treatment, NSAIDs may be an alternative approach or supplemental therapy. In this review, we discussed the latest non-steroidal therapies for endometriosis categorized by their pharmacological principles.
The most promising one would be pentoxifylline, as this supported by four human trials which showed no negative effects on women's fertility. The adverse events are not reported in these studies, while gastroenterological side effects have been widely mentioned in studies on its use in peripheral vascular diseases. In contrast, most of the other drugs are still restricted to pilot studies or case-control trials, and prospective randomized controlled studies are awaited.
For those currently limited to animal models, EGCG may be the most worthwhile option to be tested in clinical trials because of its significant results and harmlessness on follicles. The effect on fertility needs to be evaluated in animal experiments for the rest of the listed drugs.
One limitation of the study lies in the varied animal models in non-human experiments. In human trials, the heterogeneity of outcome indicators makes comparison between included studies difficult. The time recording pain scores following drug usage varied among human trials. Besides, the evaluating standard, VAS, which depends on participants’ own feelings rather than on objective detecting tools, weakens the credibility of evidence. However, most of the included studies set controls and conformed to strict blinding principles, which provided advantages for our analysis in this sort of topic.
In conclusion, the review exposes the effect of several non-hormonal agents in treating endometriosis, most of which have shown promising results but only been tested in animal models or pilot studies. Randomized controlled studies with more rigorous intervention and homogenous outcomes are needed.
Conflicts of interest
None.
Supplementary Material
Footnotes
How to cite this article: Chen FY, Wang X, Tang RY, Guo ZX, Deng YZJ, Yu Q. New therapeutic approaches for endometriosis besides hormonal therapy. Chin Med J 2019;132:2984–2993. doi: 10.1097/CM9.0000000000000569
References
- 1.Fukunaga M. Uterus-like mass in the uterine cervix: superficial cervical endometriosis with florid smooth muscle metaplasia? Virchows Arch 2001; 438:302–305.. doi: 10.1097/MD.0000000000004961. [DOI] [PubMed] [Google Scholar]
- 2.Thomas MD, Berek JS, Rinehart RD. Berek & Novak's gynecology. 15th ed.2011; Philadelphia: Lippincott Williams & Wilkins, 518–519. [Google Scholar]
- 3.Practice Committee of the American Society for Reproductive Medicine. Treatment of pelvic pain associated with endometriosis: a committee opinion. Fertil Steril 2014; 101:927–935.. doi: 10.1016/j.fertnstert.2014.02.012. [DOI] [PubMed] [Google Scholar]
- 4.Geoffron S, Cohen J, Sauvan M, Legendre G, Wattier JM, Darai E, et al. Endometriosis medical treatment: hormonal treatment for the management of pain and endometriotic lesions recurrence. CNGOF-HAS endometriosis guidelines. Gynecol Obstet Fertil Senol 2018; 46:231–247.. doi: 10.1016/j.gofs.2018.02.011. [DOI] [PubMed] [Google Scholar]
- 5.Michel C, Jacques GD, David SG, Jouko KH, John AR, Robert SC, et al. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril 1997; 67:817–821.. doi: 10.1016/s0015-0282(97)81391-x. [DOI] [PubMed] [Google Scholar]
- 6.Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016; 355:i4919.doi: 10.1136/bmj.i4919. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rudzitis-Auth J, Nickels RM, Menger MD, Laschke MW. Inhibition of cyclooxygenase-2 suppresses the recruitment of endothelial progenitor cells in the microvasculature of endometriotic lesions. Am J Pathol 2018; 188:450–460.. doi: 10.1016/j.ajpath.2017.10.013. [DOI] [PubMed] [Google Scholar]
- 8.Machado DE, Berardo PT, Landgraf RG, Fernandes PD, Palmero C, Alves LM, et al. A selective cyclooxygenase-2 inhibitor suppresses the growth of endometriosis with an antiangiogenic effect in a rat model. Fertil Steril 2010; 93:2674–2679.. doi: 10.1016/j.fertnstert.2009.11.037. [DOI] [PubMed] [Google Scholar]
- 9.Nenicu A, Gu Y, Körbel C, Menger MD, Laschke MW. Combination therapy with telmisartan and parecoxib induces regression of endometriotic lesions. Br J Pharmacol 2017; 174:2623–2635.. doi: 10.1111/bph.13874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Dogan E, Saygili U, Posaci C, Tuna B, Caliskan S, Altunyurt S, et al. Regression of endometrial explants in rats treated with the cyclooxygenase-2 inhibitor rofecoxib. Fertil Steril 2004; 82: Suppl 3: 1115–1120.. doi: 10.1016/j.fertnstert.2004.06.033. [DOI] [PubMed] [Google Scholar]
- 11.Cobellis L, Razzi S, De Simone S, Sartini A, Fava A, Danero S, et al. The treatment with a COX-2 specific inhibitor is effective in the management of pain related to endometriosis. Eur J Obstet Gynecol Reprod Biol 2004; 116:100–102.. doi: 10.1016/j.ejogrb.2004.02.007. [DOI] [PubMed] [Google Scholar]
- 12.Burnier M. The safety of rofecoxib. Expert Opin Drug Saf 2005; 4:491–499.. doi: 10.1517/14740338.4.3.491. [DOI] [PubMed] [Google Scholar]
- 13.Silveira CGT, Marschner G, Canny GO, Klocke S, Hunold P, Köster F, et al. Disrupting Y-box-binding protein 1 function using OSU-03012 prevents endometriosis progression in in vitro and in vivo models. Reprod Sci 2017; 24:67–76.. doi: 10.1177/1933719116649695. [DOI] [PubMed] [Google Scholar]
- 14.Olivares C, Ricci A, Bilotas M, Barañao RI, Meresman G. The inhibitory effect of celecoxib and rosiglitazone on experimental endometriosis. Fertil Steril 2011; 96:428–433.. doi: 10.1016/j.fertnstert.2011.05.063. [DOI] [PubMed] [Google Scholar]
- 15.Chae U, Min JY, Kim SH, Ihm HJ, Oh YS, Park SY, et al. Decreased progesterone receptor B/A ratio in endometrial cells by tumor necrosis factor-alpha and peritoneal fluid from patients with endometriosis. Yonsei Med J 2016; 57:1468–1474.. doi: 10.3349/ymj.2016.57.6.1468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Salmeri FM, Lagana AS, Sofo V, Triolo O, Sturlese E, Retto G, et al. Behavior of tumor necrosis factor-alpha and tumor necrosis factor receptor 1/tumor necrosis factor receptor 2 system in mononuclear cells recovered from peritoneal fluid of women with endometriosis at different stages. Reprod Sci 2015; 22:165–172.. doi: 10.1177/1933719114536472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Yildirim G, Attar R, Ficicioglu C, Karateke A, Ozkan F, Yesildaglar N. Etanercept causes regression of endometriotic implants in a rat model. Arch Gynecol Obstet 2011; 283:1297–1302.. doi: 10.1007/s00404-010-1543-9. [DOI] [PubMed] [Google Scholar]
- 18.Ozcelik K, Capar M, Gazi Ucar M, Cakiotar T, Ozcelik F, Tuyan Ilhan T. Are cytokine levels in serum, endometrial tissue, and peritoneal fluid a promising predictor to diagnosis of endometriosis-adenomyosis? Clin Exp Obstet Gynecol 2016; 43:569–572.. doi: 10.12891/ceoj.3022.2016. [PubMed] [Google Scholar]
- 19.Önalan G, Tohma YA, Zeyneloğlu HB. Effect of etanercept on the success of assisted reproductive technology in patients with endometrioma. Gynecol Obstet Invest 2018; 83:358–364.. doi: 10.1159/000484895. [DOI] [PubMed] [Google Scholar]
- 20.Alborzi S, Ghotbi S, Parsanezhad ME, Dehbashi S, Alborzi S, Alborzi M. Pentoxifylline therapy after laparoscopic surgery for different stages of endometriosis: a prospective, double-blind, randomized, placebo-controlled study. J Minim Invasive Gynecol 2007; 14:54–58.. doi: 10.1016/j.jmig.2006.06.024. [DOI] [PubMed] [Google Scholar]
- 21.Balasch J, Creus M, Fabregues F, Carmona F, Martinez-Roman S, Manau D, et al. Pentoxifylline versus placebo in the treatment of infertility associated with minimal or mild endometriosis: a pilot randomized clinical trial. Hum Reprod 1997; 12:2046–2050.. doi: 10.1093/humrep/12.9.2046. [DOI] [PubMed] [Google Scholar]
- 22.Creus M, Fabregues F, Carmona F, del Pino M, Manau D, Balasch J. Combined laparoscopic surgery and pentoxifylline therapy for treatment of endometriosis-associated infertility: a preliminary trial. Hum Reprod 2008; 23:1910–1916.. doi: 10.1093/humrep/den167. [DOI] [PubMed] [Google Scholar]
- 23.Kamencic H, Thiel JA. Pentoxifylline after conservative surgery for endometriosis: a randomized, controlled trial. J Minim Invasive Gynecol 2008; 15:62–66.. doi: 10.1016/j.jmig.2007.07.018. [DOI] [PubMed] [Google Scholar]
- 24.Skaper SD, Facci L, Fusco M, Della Valle MF, Zusso M, Costa B, et al. Palmitoylethanolamide, a naturally occurring disease-modifying agent in neuropathic pain. Inflammopharmacology 2014; 22:79–94.. doi: 10.1007/s10787-013-0191-7. [DOI] [PubMed] [Google Scholar]
- 25.Mattace Raso G, Russo R, Calignano A, Meli R. Palmitoylethanolamide in CNS health and disease. Pharmacol Res 2014; 86:32–41.. doi: 10.1016/j.phrs.2014.05.006. [DOI] [PubMed] [Google Scholar]
- 26.Jack BD. Aliamides: a new approach to the treatment of inflammation. Drug News Perspect 1996; 9:93–98.. [Google Scholar]
- 27.Bruner-Tran KL, Osteen KG, Taylor HS, Anna S, Kaitlin H, Duleba AJ. Resveratrol inhibits development of experimental endometriosis in vivo and reduces endometrial stromal cell invasiveness in vitro. Biol Reprod 2011; 84:106–112.. doi: 10.1095/biolreprod.110.086744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Cobellis L, Castaldi MA, Giordano V, Trabucco E, De Franciscis P, Torella M, et al. Effectiveness of the association micronized N-palmitoylethanolamine (PEA)-transpolydatin in the treatment of chronic pelvic pain related to endometriosis after laparoscopic assessment: a pilot study. Eur J Obstet Gynecol Reprod Bio 2011; 158:82–86.. doi: 10.1016/j.ejogrb.2011.04.011. [DOI] [PubMed] [Google Scholar]
- 29.Giugliano E, Cagnazzo E, Soave I, Lo Monte G, Wenger JM, Marci R. The adjuvant use of N-palmitoylethanolamine and transpolydatin in the treatment of endometriotic pain. Eur J Obstet Gynecol Reprod Biol 2013; 168:209–213.. doi: 10.1016/j.ejogrb.2013.01.009. [DOI] [PubMed] [Google Scholar]
- 30.Ricci AG, Olivares CN, Bilotas MA, Bastón JI, Singla JJ, Meresman GF, et al. Natural therapies assessment for the treatment of endometriosis. Hum Reprod 2013; 28:178–188.. doi: 10.1093/humrep/des369. [DOI] [PubMed] [Google Scholar]
- 31.Rudzitisauth J, Menger MD, Laschke MW. Resveratrol is a potent inhibitor of vascularization and cell proliferation in experimental endometriosis. Hum Reprod 2013; 28:1339–1347.. doi: 10.1093/humrep/det031. [DOI] [PubMed] [Google Scholar]
- 32.Maia H, Jr, Haddad C, Pinheiro N, Casoy J. Advantages of the association of resveratrol with oral contraceptives for management of endometriosis-related pain. Int J Womens Health 2012; 4:543–549.. doi: 10.2147/IJWH.S36825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.da Silva DM, Gross LA, Neto EPG, Lessey BA, Savaris RF. The use of resveratrol as an adjuvant treatment of pain in endometriosis: a randomized clinical trial. J Endocr Soc 2017; 1:359–369.. doi: 10.1210/js.2017-00053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Laschke MW, Schwender C, Scheuer C, Vollmar B, Menger MD. Epigallocatechin-3-gallate inhibits estrogen-induced activation of endometrial cells in vitro and causes regression of endometriotic lesions in vivo. Hum Reprod 2008; 23:2308–2318.. doi: 10.1093/humrep/den245. [DOI] [PubMed] [Google Scholar]
- 35.Wang J, Man GCW, Chan TH, Kwong J, Wang CC. A prodrug of green tea polyphenol (–)-epigallocatechin-3-gallate (Pro-EGCG) serves as a novel angiogenesis inhibitor in endometrial cancer. Cancer Lett 2018; 412:10–20.. doi: 10.1016/j.canlet.2017.09.054. [DOI] [PubMed] [Google Scholar]
- 36.Wang CC, Xu H, Man GCW, Zhang T, Chu KO, Chu CY, et al. Prodrug of green tea epigallocatechin-3-gallate (Pro-EGCG) as a potent anti-angiogenesis agent for endometriosis in mice. Angiogenesis 2013; 16:59–69.. doi: 10.1007/s10456-012-9299-4. [DOI] [PubMed] [Google Scholar]
- 37.Jiang HQ, Li YL, Jie Z. Effect of recombinant human endostatin on endometriosis in mice. Chin Med J 2007; 120:1241–1246.. doi: 10.1097/00029330-200707020-00007. [PubMed] [Google Scholar]
- 38.Becker CM, Sampson DA, Rupnick MA, Rohan RM, Efstathiou JA, Short SM, et al. Endostatin inhibits the growth of endometriotic lesions but does not affect fertility. Fertil Steril 2005; 84:1144–1155.. doi: 10.1016/j.fertnstert.2005.04.040. [DOI] [PubMed] [Google Scholar]
- 39.Ma Y, He Y. Study of an antiangiogenesis gene therapy with endostatin on endometriosis in the nude mouse model. Clin Exp Obstet Gynecol 2014; 41:328–334.. doi: 10.12891/ceog17172014. [PubMed] [Google Scholar]
- 40.Kim JG, Kim JY, Jee BC, Suh CS, Kim SH, Choi YM. Association between endometriosis and polymorphisms in endostatin and vascular endothelial growth factor and their serum levels in Korean women. Fertil Steril 2008; 89:243–245.. doi: 10.1016/j.fertnstert.2007.02.023. [DOI] [PubMed] [Google Scholar]
- 41.Laschke M, Elitzsch A, Scheuer C, Holstein J, Vollmar B, Menger M. Rapamycin induces regression of endometriotic lesions by inhibiting neovascularization and cell proliferation. Br J Pharmacol 2006; 149:137–144.. doi: 10.1038/sj.bjp.0706857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Slomovitz BM, Lu KH, Johnston T, Coleman RL, Munsell M, Broaddus RR, et al. A phase 2 study of the oral mammalian target of rapamycin inhibitor, everolimus, in patients with recurrent endometrial carcinoma. Cancer 2010; 116:5415–5419.. doi: 10.1002/cncr.25515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Novella-Maestre E, Carda C, Ruiz-Sauri A, Garcia-Velasco JA, Simon C, Pellicer A. Identification and quantification of dopamine receptor 2 in human eutopic and ectopic endometrium: a novel molecular target for endometriosis therapy. Biol Reprod 2010; 83:866–873.. doi: 10.1095/biolreprod.110.084392. [DOI] [PubMed] [Google Scholar]
- 44.Scarpellini F, Sbracia M, Lecchini S, Scarpellini L. Anti-angiogenesis treatment with thalidomide in endometriosis: a pilot study. Fertil Steril 2002; 78:S87.doi: 10.1016/S0015-0282(02)03609-9. [Google Scholar]
- 45.Hamid AMSA, Madkour WA, Moawad A, Elzaher MA, Roberts MP. Does cabergoline help in decreasing endometrioma size compared to LHRH agonist? A prospective randomized study. Arch Gynecol Obstet 2014; 290:677–682.. doi: 10.1007/s00404-014-3242-4. [DOI] [PubMed] [Google Scholar]
- 46.Delgado-Rosas F, Gomez R, Ferrero H, Gaytan F, Garcia-Velasco J, Simon C, et al. The effects of ergot and non-ergot-derived dopamine agonists in an experimental mouse model of endometriosis. Reproduction 2011; 142:745–755.. doi: 10.1530/rep-11-0223. [DOI] [PubMed] [Google Scholar]
- 47. Quinagolide Vaginal Ring on Lesion Reduction Assessed by MRI in Women with Andometriosis/Adenomyosis. ClinicalTrials.gov, 2018. Available from: https://clinicaltrials.gov/ct2/show/NCT03749109?cond=endometriosis&intr=quinagolide&rank=1. [Last accessed on October 24, 2019] [Google Scholar]
- 48.Esfandiari N, Khazaei M, Ai J, Bielecki R, Gotlieb L, Ryan E, et al. Effect of a statin on an in vitro model of endometriosis. Fertil Steril 2007; 87:257–262.. doi: 10.1016/j.fertnstert.2006.06.040. [DOI] [PubMed] [Google Scholar]
- 49.Nasu K, Yuge A, Tsuno A, Narahara H. Simvastatin inhibits the proliferation and the contractility of human endometriotic stromal cells: a promising agent for the treatment of endometriosis. Fertil Steril 2009; 92:2097–2099.. doi: 10.1016/j.fertnstert.2009.06.055. [DOI] [PubMed] [Google Scholar]
- 50.Piotrowski PC, Kwintkiewicz J, Rzepczynska IJ, Seval Y, Cakmak H, Arici A, et al. Statins inhibit growth of human endometrial stromal cells independently of cholesterol availability. Biol Reprod 2006; 75:107–111.. doi: 10.1095/biolreprod.106.051763. [DOI] [PubMed] [Google Scholar]
- 51.Oktem M, Esinler I, Eroglu D, Haberal N, Bayraktar N, Zeyneloglu H. High-dose atorvastatin causes regression of endometriotic implants: a rat model. Hum Reprod 2007; 22:1474–1480.. doi: 10.1093/humrep/del505. [DOI] [PubMed] [Google Scholar]
- 52. Efficacy Study of Atorvastatin in Pelvic Pain Relief in Women With Endometriosis. ClinicalTrials.gov, 2018. Available from: https://clinicaltrials.gov/ct2/show/NCT00675779?titles=Efficacy+study+of+atorvastatin+in+pelvic+pain+relief+in+women+with+endometriosis&rank=1. [Last accessed on October 24, 2019] [Google Scholar]
- 53.Zhang GQ, Tao YK, Bai YP, Yan ST, Zhao SP. Inhibitory effects of simvastatin on oxidized low-density lipoprotein-induced endoplasmic reticulum stress and apoptosis in vascular endothelial cells. Chin Med J 2018; 131:950–955.. doi: 10.4103/0366-6999.229891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Bruner-Tran KL, Osteen KG, Duleba AJ. Simvastatin protects against the development of endometriosis in a nude mouse model. J Clin Endocrinol Metab 2009; 94:2489–2494.. doi: 10.1210/jc.2008-2802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Almassinokiani F, Mehdizadeh A, Sariri E, Rezaei M, Almasi A, Akbari H, et al. Effects of simvastatin in prevention of pain recurrences after surgery for endometriosis. Med Sci Monit 2013; 19:534–539.. doi: 10.12659/msm.883967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Waiyaput W, Pumipichet S, Weerakiet S, Rattanasiri S, Sophonsritsuk A. Effect of simvastatin on monocyte chemoattractant protein-1 expression in endometriosis patients: a randomized controlled trial. BMC Women Health 2017; 17:89.doi: 10.1186/s12905-017-0446-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Yee LD, Williams N, Wen P, Young DC, Lester J, Johnson MV, et al. Pilot study of rosiglitazone therapy in women with breast cancer: effects of short-term therapy on tumor tissue and serum markers. Clin Cancer Res 2007; 13:246–252.. doi: 10.1158/1078-0432.CCR-06-1947. [DOI] [PubMed] [Google Scholar]
- 58.Blitek A, Szymanska M. Regulation of expression and role of peroxisome proliferator-activated receptors (PPARs) in luminal epithelial and stromal cells of the porcine endometrium. Theriogenology 2019; 127:88–101.. doi: 10.1016/j.theriogenology.2019.01.002. [DOI] [PubMed] [Google Scholar]
- 59.Demirturk F, Aytan H, Caliskan AC, Aytan P, Koseoglu DR. Effect of peroxisome proliferator-activated receptor-gamma agonist rosiglitazone on the induction of endometriosis in an experimental rat model. J Soc Gynecol Investig 2006; 13:58–62.. doi: 10.1016/j.jsgi.2005.10.002. [DOI] [PubMed] [Google Scholar]
- 60.Lebovic DI, Mwenda JM, Chai DC, Mueller MD, Santi A, Fisseha S, et al. PPAR-gamma receptor ligand induces regression of endometrial explants in baboons: a prospective, randomized, placebo-and drug-controlled study. Fertil Steril 2007; 88:1108–1119.. doi: 10.1016/j.fertnstert.2006.12.072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Pich C, Meylan P, Mastelic-Gavillet B, Nguyen TN, Loyon R, Trang BK, et al. Induction of paracrine signaling in metastatic melanoma cells by PPARgamma agonist rosiglitazone activates stromal cells and enhances tumor growth. Cancer Res 2018; 78:6447–6461.. doi: 10.1158/0008-5472.can-18-0912. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.