

Abstract
Purpose: Tumor markers that are related to hypoxia, proliferation, DNA damage repair and stem cell-ness, have a prognostic value in advanced stage HNSCC patients when assessed individually. Here we aimed to evaluate and validate this in a multifactorial context and assess interrelation and the combined role of these biological factors in determining chemo-radiotherapy response in HPV-negative advanced HNSCC.
Methods: RNA sequencing data of pre-treatment biopsy material from 197 HPV-negative advanced stage HNSCC patients treated with definitive chemoradiotherapy was analyzed. Biological parameter scores were assigned to patient samples using previously generated and described gene expression signatures. Locoregional control rates were used to assess the role of these biological parameters in radiation response and compared to distant metastasis data. Biological factors were ranked according to their clinical impact using bootstrapping methods and multivariate Cox regression analyses that included clinical variables. Multivariate Cox regression analyses comprising all biological variables were used to define their relative role among all factors when combined.
Results: Only few biomarker scores correlate with each other, underscoring their independence. The different biological factors do not correlate or cluster, except for the two stem cell markers CD44 and SLC3A2 (r = 0.4, p < 0.001) and acute hypoxia prediction scores which correlated with T-cell infiltration score, CD8+ T cell abundance and proliferation scores (r = 0.52, 0.56, and 0.6, respectively with p < 0.001). Locoregional control association analyses revealed that chronic (Hazard Ratio (HR) = 3.9) and acute hypoxia (HR = 1.9), followed by stem cell-ness (CD44/SLC3A2; HR = 2.2/2.3), were the strongest and most robust determinants of radiation response. Furthermore, multivariable analysis, considering other biological and clinical factors, reveal a significant role for EGFR expression (HR = 2.9, p < 0.05) and T-cell infiltration (CD8+T-cells: HR = 2.2, p < 0.05; CD8+T-cells/Treg: HR = 2.6, p < 0.01) signatures in locoregional control of chemoradiotherapy-treated HNSCC.
Conclusion: Tumor acute and chronic hypoxia, stem cell-ness, and CD8+ T-cell parameters are relevant and largely independent biological factors that together contribute to locoregional control. The combined analyses illustrate the additive value of multifactorial analyses and support a role for EGFR expression analysis and immune cell markers in addition to previously validated biomarkers. This external validation underscores the relevance of biological factors in determining chemoradiotherapy outcome in HNSCC.
Keywords: HNSCC, chemoradiotherapy, radiation resistance, hypoxia, immune cell infiltration, expression profile analysis, head and neck cancer, radiation oncology
Introduction
In this study we set out to perform multifactorial analyses to gain understanding of the role and dependence of biological factors that have shown to influence tumor radiation response in preclinical studies and to be associated with radiotherapy response in clinical studies (1, 2). Chemo-radiotherapy is the primary treatment option for advanced head and neck squamous cell carcinoma (HNSCC). Cure and locoregional failure rates of around 50 and 25%, respectively, facilitate the evaluation of biological determinants of radiation response. Using biological characteristics of the tumors, outcome association studies revealed many potential determinants of prognosis and treatment response in HNSCC (3–7). This study evaluates complementarity and hierarchy of radiation response determining “HNSCC biology.”
Head and neck squamous cell carcinoma (HNSCC) is the 6th most common cancer in the world, with smoking, alcohol and HPV infection as the main risk factors. Around two thirds of the patients present with advanced stage disease and have a poor prognosis with 5 year overall survival rates around 50% (8, 9). Allowing for organ preservation, curative treatment for advanced stage hypopharyngeal, laryngeal and HPV-negative oropharyngeal carcinomas shifted from extensive surgery to concomitant cisplatin-based chemo-radiotherapy in the last decades (10). Around two third of all HNSCC patients receive radiotherapy as part of their treatment. Among these, those with HPV-positive oropharyngeal tumors have a particularly good prognosis, reason to consider them as a new entity in the new TNM staging (11). As revealed by gene expression and mutational analyses, these tumors are also biologically very different (12, 13). HPV-negative HNSCC, in contrast, are characterized by poor prognosis. They exhibit frequent amplifications and mutations in proto-oncogenes (EGFR, MYC, HRAS) and in cell cycle genes that drive and support tumor proliferation (14–16). p53 is affected in almost all HPV-negative HNSCC.
Early radiobiology studies revealed determinants of tumor radiation response. Hypoxia, repopulation, driven by tumor cell proliferation, tumor stem cell density (i.e., clonogenic cell density) and cellular radiosensitivity (as for example determined by cellular DNA damage repair capacity) were shown to be among the most relevant biological factors that affect radiation or fractionated radiotherapy response in preclinical models of different cancers (1, 2). In recent years, increased interest emerged in immune response related markers and immune cells due to novel immunotherapeutic options (17–21). A series of preclinical and clinical studies highlight the potential relevance of immune-related markers in HNSCC [reviewed in (5, 6, 19, 22–24)].
HNSCC outcome association studies using many different biomarkers, demonstrated the clinical importance of some of these pre-clinically assessed tumor biology parameters (1, 5–7). HPV and hypoxia are indeed the best studied biology related prognostic markers in HNSCC. Within the HPV-negative patients, tumor hypoxia marks patients with a poor prognosis (25–29). Confirming its role above marking poor prognosis patients, hypoxia biomarkers also predict response to hypoxia modification therapy (25, 30–33). Elaborating on a gene expression profile that captures the cellular changes caused by acute hypoxia, we recently showed the relevance of acute hypoxia in addition to chronic hypoxia (29). As predicted by the process they capture, these two classifications did not necessarily overlap in the samples and also reveal different outcome associations in HNSCC that result from a prominent role of acute hypoxia.
While the success of accelerated radiotherapy schedules (34) highlight the important role of tumor repopulation in HNSCC, there is a lack of biomarker data showing a link to cellular proliferation (35). Based on genetic mutation data, we find a small role for co-occurring CCND1 and CDKN2A mutations in HPV-negative chemo-radiotherapy treated HNSCC that was however not visible in the locoregional control endpoints (36). Yet, the combination of radiotherapy with the epidermal growth factor receptor (EGFR) binding antibody cetuximab has shown efficacy and EGFR expression has been associated with poor survival, preferentially in non-accelerated schedules arguing for a role in tumor repopulation (37–40). The role of EGFR and cellular proliferation in radiotherapy response needs to be further elaborated (41–43). However proliferation, as determined by the proliferation marker by Starmans et al. has been linked to aggressive disease or disease progression in multiple cancer types; unfortunately this was not assessed in HNSCC (44).
Originated from CD44 expression data from de Jong et al. (45) in laryngeal cancer and confirmed in resected and chemo-radiotherapy treated HNSCC for CD44 and SLC3A2 (27, 46) in subsequent studies, it also became clear that tumor “stem cell-ness” is important in radiotherapy outcomes since these stem cell related biomarkers were associated with poor prognosis (35, 47–49).
The consistent effect of CD8+ T cell depletion on radiation induced tumor growth delays in preclinical studies expose the relevance of certain immune cell populations in radiation response and resistance (50, 51). Evidence in clinic of a possible interaction is less strong and current studies focus on strategies to optimize combinations with immune response modulators to improve radiotherapy outcomes (6, 18, 20, 21, 23, 27, 52–55). Interestingly, Mandal et al. recently showed that markers for regulatory Tcells (Treg), NK cells and CD8+ T cells are prognostic in head and neck cancer (56) in the TCGA dataset. Despite these interesting initial reports, the prognostic value of these gene expression based immune markers is still unknown for chemo-radiotherapy treated patients since all patients in the TCGA dataset have been treated with primary surgery. Immunohistochemically (IHC) determined high CD8+ T-cell counts are associated with good prognosis in postoperative chemo-radiotherapy treated patients, further indicating its relevance for HNSCC (57). A good prognosis association with IHC CD8+ TIL density was found in patients with oropharyngeal squamous cell carcinoma treated with surgery or (chemo) radiotherapy and in a similarly mixed treatment cohort of hypopharyngeal SCC patients (58–60).
Our previous studies emphasized the important role of functional and genetic DNA crosslink repair defects in HNSCC (61, 62) and provided the basis for machine learning generated models that predicted such DNA repair defects in clinical samples (63). The expression based DNA repair defect prediction models revealed an association with metastasis in HNSCC and linked DNA repair defects to migratory and invasive behavior in HNSCC cell lines (63). Given the relevance of Epithelial to Mesenchymal Transition (EMT) in many cancer types, we also developed a HNSCC-specific EMT model that classifies HNSCC according to epithelial or mesenchymal characteristics (64). The strong prognostic value of this HNSCC-EMT model also suggests an important role in radiation response.
Taken together, the individual roles of some of these biological factors important in radiation response have not been validated and the interrelation of these biological factors has not been investigated in the clinical setting. We therefore studied the role of the aforementioned biological factors in the context of head and neck cancer and chemo-radiotherapy. Previously published gene expression based signatures were used to detect these factors. In a set of nearly 200 patients with advanced stage HPV-negative HNSCC treated with chemo-radiotherapy, we used univariate and multivariate outcome analyses to examine these factors while also considering correlation and dependence to delineate their relative roles.
Materials and Methods
Patient Data and Material
This retrospective study included material and data from patients that were diagnosed between 2001 and 2014 and treated with definitive cisplatin-based chemo-radiotherapy within three centers: the Netherlands Cancer Institute (Amsterdam, NL), the Amsterdam University Medical Center (Amsterdam, NL) or the MAASTRO clinic/MUMC+ (Maastricht, NL). Selection criteria for this gene expression study cohort were (i) concomitant radiotherapy and cisplatin treatment of unresected HNSCC, (ii) hypopharyngeal, laryngeal or HPV-negative oropharyngeal (iii) no prior treatment with chemotherapy or radiotherapy in the head and neck area. To minimize the number of variables, AJCC disease staging, summarizing TNM stage, was used to classify HNSCC patients after determining whether this classification also represented N-staging and its known association with survival well (Supplementary Figure 1). Received radiotherapy regimens were 70 Gy over 35 fractions (up to 77 Gy in ARTFORCE patients) in 7 or 6 weeks (DAHANCA scheme). All patients were treated with either of four different cisplatin regimens: daily [25 × 6 mg/m2 Body Surface Area (BSA)], weekly (7 × 40 mg/m2 BSA) or 3-weekly (3 × 100 mg/m2 BSA) intravenous administration or weekly intra-arterial administration [4 × 150 mg/m2 BSA, for 8 patients according to the RADPLAT trial protocol (65)]. Not all patients completed the full chemotherapy scheme. Therefore, cumulative cisplatin doses were calculated and patients were classified into < or ≥ or 200 mg/m2 BSA cisplatin, according to literature (66, 67). Survival data was calculated from the start of treatment until the first event was detected. The primary outcome measure is loco-regional control (LRC) and implies absence of recurrences in the radiotherapy targeted regions of the head and neck area. Patient characteristics are provided in Supplementary Table 1. Institutional Review Boards at the Netherlands Cancer Institute, the Amsterdam University Medical Center and the MAASTRO clinic/MUMC+ approved biopsies and collection of fresh-frozen HNSCC tumor material and the use of genetic and clinical data from patients at their respective centers after anonymization. All patients granted written informed consent for biopsy, material use and data use. Pre-treatment tumor biopsy material available for the DESIGN study or collected from the NKI ARTFORCE (68) or RADPLAT trial patients were used for RNA preparation and sequencing. HPV-status of all oropharyngeal carcinomas was determined by immunohistochemical assessment of p16 by a dedicated head and neck pathologist (69) followed by a HPV DNA test on the p16-immunopositive cases and/or confirmed using RNA-sequencing data.
Material Preparation and RNA-Sequencing
Fresh-frozen tumor samples were sectioned, collected for RNA preparation and in part subjected to tumor percentage evaluation by revision of HE stained coupes by senior head and neck pathologist Dr. S.M. Willems. Only samples with a tumor percentage of >40% proceeded to RNA-sequencing. RNA was isolated using the AllPrep DNA/RNA mini kit (Qiagen). Quality and quantity of total RNA was assessed by the 2100 Bioanalyzer using a Nano chip (Agilent, Santa Clara, CA). Only total RNA samples having RIN>7 were used for library preparation. Strand-specific libraries were generated using the TruSeq Stranded mRNA sample preparation kit (Illumina Inc., San Diego, RS-122-2101/2) according to the manufacturer's instructions (Illumina, Part # 15031047 Rev. E). The libraries were analyzed on a 2100 Bioanalyzer using a 7500 chip (Agilent, Santa Clara, CA), diluted and pooled equimolar into a 10 nM multiplex sequencing pool and sequenced with 65 base single reads on a HiSeq2500 using V4 chemistry (Illumina Inc., San Diego). Reads were mapped against the GRCh38 human genome using TopHat2.1 (70), with options “fr-firststrand,” “transcriptome-index,” and “prefilter multi-hits.” Read counts were determined using HTSeq-count (71) with options “stranded” and mode “union.”
Expression and Patient Outcome Analyses
All analyses were performed in R 3.4.3 using Rstudio 1.1. Samples were classified and scored for the different analyzed biological characteristics using different gene expression profiles according to the protocols described in the original publication. If not possible due to the lack of original reference data, GSVA, a Bioconductor package for R, was used on raw read counts to calculate gene expression profile scores (72). Transcripts per million (TPM) was used for individual gene expression analyses. Patient outcome analyses were performed using Cox proportional hazard model. Time to event was defined as the time between the first day of treatment and the day the event was detected. Events in the locoregional control data (LRC) were defined by recurrences in the radiotherapy targeted region. Distant metastasis (DM) events were defined by tumors detected outside the head and neck area. A patient's death prior to a possible event led to censoring in the LRC and DM data and no event was recorded. Progression free survival (PFS) was defined as the time from the start of treatment to the day the patient died, had a locoregional recurrence or distant metastasis. Tests were considered significant when p < 0.05. A spearman correlation coefficient was computed between continuous variables.
In order to obtain a robust cut-off when transforming a continuous variable into a dichotomous variable we used the bootstrap procedure as described in Linge et al. (28). In brief, 197 sample values were randomly assigned into one bootstrap cohort (from the cohort of 197 patients) while data from the same patient could be chosen multiple times. This procedure was repeated to obtain 10.000 randomized cohorts. At each possible cut-off value of the marker of interest, the individual cohorts were split into a “low” and “high” group and Cox proportional hazards models were fit based on these splits. These models included, next to the newly grouped marker of interest, all clinical variables that were found to be significantly associated with the outcome of interest [Locoregional Control (LRC), Distant Metastasis (DM), Overall Survival (OS) or Progression Free Survival (PFS)]. The fraction of cohorts for which the marker of interest was significantly associated with survival (p < 0.05) was recorded for each cutoff. The values of nine adjacent cutoffs were averaged to smoothen the data. The cutoff with the highest fraction of significant associations was chosen for further analysis. Cutoffs that would result in patient subgroups with <10% of the patients were not considered to maintain statistical power. Note that, this analysis was repeated for each endpoint resulting in different cut-offs.
To reduce the number of possible variables included in multivariable analysis we used a backward selection procedure. The most frequent level of each variable was used as the reference level for this analysis. A Cox proportional hazard model was fit containing all biological markers and clinical variables. Then, each individual variable was removed from the model and improvements in model performance by this process were assessed using the Akaike Information Criterion (AIC) from the “stats” package in R. The best model (lowest AIC) was selected for further analysis in the multivariate Cox regression analysis. This process was repeated until removing variables from the model did no longer result in an improved model.
Results
Role of Clinical Factors and Patient Characteristics in Chemo-Radiotherapy Outcome
In this retrospective multicenter study, 197 patients met all inclusion criteria and had sufficient tumor material available. All patients were treated with definitive cisplatin-based chemo-radiotherapy for advanced stage HPV-negative oropharyngeal, hypopharyngeal, or laryngeal carcinoma. Patient characteristics are shown in Table 1. The median age in this patient cohort is 62 years and there is a male: female ratio of 3:1. Most patients reported ongoing or a history of alcohol and/or tobacco use. The largest subsite representation is oropharyngeal tumors with 85 patients, then hypopharyngeal with 78 and laryngeal carcinoma with 34 patients. Except for two patients, all patients had stage III/IV classified tumors. As expected, outcomes and survival curves differ according to stage (Supplementary Figure 2). Tumor volume data as determined by delineation on RT planning CT images were available for 166 patients with a median volume of 23.2 cm3. Not all patients finished chemotherapy, but 126 patients (63%) received a cumulative dose of and above 200 mg/m2 body surface area. Locoregional recurrences occurred in 23.8% (N = 49) of cases and distant metastasis in 19.8% (N = 39).
Table 1.
HNSCC patients and tumor characteristics.
| Variable | #Patients (total 197) | |
|---|---|---|
| Median Age at diagnosis (Range) | 61 years (40–80.23) | |
| Sex | Female | 55 |
| Male | 142 | |
| Alcohol | No | 22 |
| Former alcoholic | 22 | |
| Yes | 146 | |
| Missing | 7 | |
| Tobacco | Never | 5 |
| Former smoker | 30 | |
| Yes | 156 | |
| Missing | 6 | |
| Tumor subsite | Larynx | 34 |
| Hypopharynx | 78 | |
| Oropharynx | 85 | |
| Median tumor volume (Range) | 23.2 cm3 (1.03–752.2) | |
| Missing | 31 | |
| Stage | IVB | 20 |
| III | 40 | |
| II | 2 | |
| IVA | 135 | |
| Cumulative cisplatin dose | <200 mg/cm2 | 67 |
| ≥200 mg/cm2 | 126 | |
| Missing | 4 | |
| Median Follow-up | 5.24 years (4.59–5.86) | |
| Locoregional Recurrences | 49 | |
| Distant Metastasis | 39 | |
Clinical factors were tested for their association with locoregional control and other survival outcomes (Supplementary Figure 1, Supplementary Table 1). Consistent with previous reports we find that locoregional control (LRC) is influenced by cumulative cisplatin dose levels (66, 67). The cumulative cisplatin dose of < 200 mg/m2 BSA was significantly associated with LRC failure (HR = 2.57, p = 0.0012). Female sex shows a trend toward better locoregional control (HR = 0.52, p = 0.072). This could however been confounded by the less prominent alcohol consumption characteristics or other differences in lifestyle in this particular patient group. More female patients reported to abstain from alcohol compared to male patients (21.8 vs. 7.4%, p = 0.019), which was however not the case for tobacco use (p = 0.66). Heavy past or ongoing alcohol consumption was associated with an increased risk for LRC failure (HR = 2.16, p = 0.041). Interestingly, age, tobacco, tumor subsite and AJCC stage is not significantly associated with LRC in our patient cohort. The other clinical outcomes (DM, PFS or OS) showed significant associations with sex, tumor volume, stage and cisplatin (Supplementary Figure 1, Supplementary Table 1).
Tumor Biology Assessment and (in)Dependence in HPV-Negative HNSCC
Preclinical radiobiology studies and clinical biomarker studies exposed many different determinants of radiation response. The number of variables that can be included in statistical analyses are however limited by the cohort size and number of events. Thus, in order to evaluate the relative role of different tumor biology parameters in clinic, we prioritized those with a reported clinical outcome association. The following 12 gene expression signatures were therefore selected to characterize the clinical samples using pretreatment HNSCC transcriptomic data: The Toustrup (1) and Seigneuric (2) expression signatures were used to assess the level of chronic (1) and acute (2) hypoxia, respectively (25, 73). Linked to tumor stem cell richness SLC3A2 (3) and CD44 (4) gene expression values (in TPM) were included since both have been reported to be associated with outcome in chemo-radiotherapy treated patients (74). Economopoulou et al. (5) EGFR expression (in TPM) and (6) the Starmans et al. “proliferation” expression signature (44) were selected as cellular proliferation markers which could influence tumor repopulation between radiotherapy fractions. To cover immune-related factors we further included expression signatures from Senbabaoglu et al. (75) that originated from Bindea et al. (76) and assess (7) ‘T-cell infiltration score' (TIS), (8) CD8+ T-cells, (9) CD56dim natural killer (NK) cells abundance while considering the (10) CD8+ vs. T regulatory (Treg) cell ratios. This immune status gene expression signature selection is based on the reported outcome association in resected HNSCC (56). Our own studies conducted in HPV-negative advanced HNSCC revealed an important role for EMT and DNA crosslink (CL) repair defects in treatment outcome and these prediction models for mesenchymal characteristics and tumor cell DNA crosslink repair defects (11). “HNSCC-EMT” and (12) “MMConly,” were therefore included in this analysis and are referred to as “EMT” and “DNA CL repair” in this manuscript (63, 64). Most of these biological factors have been tested individually, predominantly in univariable analyses and in different settings in previous studies; however their mutual correlations and possible dependence between them are unknown.
The goal of this study is to pinpoint biological factors that are important for (chemo)-radiotherapy treatment failure and thus might validate their independent role in radioresistance. We therefore calculated scores for all aforementioned markers. Supplementary Figure 3 shows the frequency of the scores and their distribution over the patient cohort. Next, we performed hierarchical clustering to investigate the presence of HNSCC subsets as defined by these characteristics. Tumor volume was included in this analysis as it promotes chronic hypoxia or may be associated with high proliferation scores. Despite the coexistence and correlation of some factors this does however not reveal any prominent clusters (Figures 1A,B). Surprisingly, we find that the acute hypoxia profile score correlates with the Starmans proliferation score (r = 0.58, p < 0.001) (Figure 1C) but also with the T-cell Infiltration Score (TIS) and the CD8+ T cell scores (r = 0.51 and r = 0.54, p < 0.001).
Figure 1.

Interrelation and dependence of biological markers. (A) Heatmap showing hierarchical clustering of patients based on the selected biological markers. Tumor volume and EGFR expression were log-transformed to prevent clustering to be dominated by few samples with high values. (B) Correlation plot with spearman's ranked correlation values between all biological marker scores. Markers were grouped by tumor biology class where appropriate. *p < 0.05, **p < 0.01, *** p < 0.001, not corrected for multiple testing. (C) Scatterplots with Spearman's coefficients and p-values for correlations of interest.
Within their own category, stem cell related markers, CD44 and SLC3A2 (r = 0.57, p < 0.001), and the immune cell related markers correlate with each other. While the correlation of acute and chronic hypoxia is significant, it is fairly weak (R = 0.26, p < 0.001) and was in line with previous reports (29). EGFR expression and the proliferation score are correlated to some extent (r = 0.26, p < 0.01). The CD8+ T cell to regulatory T cell ratio (CD8+/Treg) as determined by the expression signature scores is negatively associated with the abundance of CD56dim natural killer (NK) cells and the TIS signature. While the link between tumor volume and chronic hypoxia (R = 0.23, p < 0.01) is expected, tumor volume is also associated with EMT (R = 0.23, p < 0.05). With a maximum variance inflation factor value of 3.3, correlations were not strong enough to exclude parameters from subsequent analyses. None of these markers show strong associations with any of the clinical factors. Among all, we find that the most independent tumor characteristics are the presence of DNA CL repair defects and tumor EMT status (and tumor volumes).
Role of Individual Biological Factors in Locoregional Control by Chemo-Radiotherapy in HNSCC
Since we aimed to evaluate tumor characteristics with respect to radiation resistance and response, we initially focused on locoregional control outcome values that are mainly determined by the success of the “local” radiotherapy treatment. Given the lack of strong correlations, all markers were individually tested for their association with locoregional failure. A 10.000 times bootstrapping method was employed to (a) determine a potential role for the biomarker across different cutoffs and (b) to identify a clinically robust cut-off for each so to compare the biomarkers among each other. In brief, each marker was tested for their association with the selected survival outcome for all possible cutoffs. This analysis was performed using a multivariable Cox proportional hazard model with all relevant clinical factors included, as determined above. Consequently, clinical variables were included according to outcome type: sex and cumulative cisplatin dose for LRC; sex, subsite and cumulative cisplatin dose for OS; stage, subsite and cisplatin dose for PFS; and sex and alcohol use for DM. Based on the results of these 10.000 bootstrap repeats (Figure 2A), we find that the hypoxia and stem cell related markers are most robustly associated with LRC across different score cut-offs. Proliferation, EGFR and immune cell signatures merely provide significant associations with LRC in a fraction of the randomly created cohorts and tested cut-offs.
Figure 2.

Role of individual biological factors for locoregional control. (A) Results of individual bootstrap analysis (see methods) including important clinical factors. The fraction of randomized cohorts with a significant association with locoregional control is shown for each cut-off and biological marker. Markers are ordered by the magnitude of the maximum fraction of significant Cox proportional hazard tests at the best cut-off. The best cutoff is indicated with dotted red lines. (B) For each marker, the cohort was split into a high and low group at the best cutoff determined in A. Hazard ratios for recurrences and corresponding p-values were obtained with a multivariate Cox proportional hazard analysis using the same variables as those used to determine the cutoff.
Cut-offs with the most stable clinical association were selected for each biomarker for further analysis as depicted in Figure 2A and listed in Supplementary Table 2. These analyses confirm that both, chronic and acute hypoxia, are strongly associated with locoregional control. Using these calculated cut-offs in multivariable analyses with clinical factors, we find that among all chronic hypoxia is most strongly associated with a failure of locoregional control (HR = 3.95, p = 0.0038) followed by acute hypoxia (HR = 1.9, p = 0.03) and stem cell related, SLC3A2 (HR = 2.31, p = 0.026) and CD44 (HR = 2.03, p = 0.043; Figures 2B, 3; Supplementary Table 3). Although not significantly, larger tumor volumes showed a trend toward worse locoregional control with a hazard ratio (HR = 1.63, p = 0.11) that is comparable to those previously reported by others (27). It should be however noted that most tumors in this cohort are relatively large and stage III/IV. This and the fact that the LRC measure also includes regional recurrences, may together affect the specific HR values. Trends toward a worse LRC prognosis were observed in patient groups with tumors with high proliferation and CD8+ T cell scores (HR = 1.89, p = 0.067 and HR = 2.35, p = 0.071, respectively) (Supplementary Figure 4 and Supplementary Table 3).
Figure 3.

Relevance of biological markers for HNSCC chemo-radiotherapy outcomes. Forest plots comparing individual biological markers across different outcome endpoints are shown. Hazard Ratios for locoregional recurrences, distant metastasis, disease progression and death are from multivariate Cox proportional hazard analyses of the dichotomized cohorts using bootstrap analysis defined cut-offs for all outcomes analyzed in this study. For each marker the “low” score or low expression group was used as reference. Each individual model contained the same clinical variables as those used to determine the cut-off. Only the biological markers are shown.
To delineate this from general poor prognosis pattern and to investigate the radiation response link further, we repeated these analyses and compared the role of these biomarkers for overall survival, progression free survival and distant metastasis (Figure 3). Cut-off values were defined by the bootstrapping method described above for each biomarker; and multivariable Cox proportional hazard analyses with clinical factors were performed. Notably, gene expression signature scores or expression value cut-offs, as determined by their potential relevance in the 10,000x bootstrapping method, resulted to be different in some of the biomarkers such as “acute hypoxia,” “chronic hypoxia,” “EGFR,” “TIS,” “NK CD56dim.” and “CD8+/Treg” (Supplementary Figures 4–6 and Supplementary Table 2).
Most markers show an association with several of the outcome parameters. We find that distant metastasis is associated with EMT (HR = 3.14, p = 0.0086), acute hypoxia score (HR = 2.44, p = 0.0086), NK CD56dim score (HR = 2.47, p = 0.019) and EGFR expression (HR = 2.07, p = 0.032) (Supplementary Figure 5, Supplementary Table 3). Poor overall survival is associated with increased tumor volume (HR = 2.12, p = 0.00054), EMT score (HR = 2.15, p = 0.002), DNA CL repair defect (HR = 1.97, p = 0.0043), acute hypoxia (HR = 1.62, p = 0.023) and EGFR expression (HR = 1.68, p = 0.014) (Supplementary Figure 6, Supplementary Table 3). High EMT (HR = 2.19, p = 0.0014), EGFR (HR = 1.82, p = 0.0038), acute hypoxia (HR = 1.64, p = 0.017), DNA CL repair defect (HR = 1.8, p = 0.0085) and chronic hypoxia scores (HR = 1.7, p = 0.015) and tumor volumes (HR = 1.72, p = 0.036) are associated with a worse progression free survival (PFS) (Supplementary Figure 7; Supplementary Table 3). Interestingly, when comparing the distant metastasis and locoregional control failure data, locoregional control is increased in tumors with higher EGFR expression or containing few CD56dim NK cells while high values in both result in an increased risk of DM. It should be noted, however, that the bootstrapping defined cut-offs were different in both. Yet, as evident from the bootstrapping data chronic hypoxia was not linked to DM but LRC at many cut-offs. On the contrary, the similar shape of the results from the acute hypoxia bootstrapping supports its relevance in both, LRC and DM (Figure 2 and Supplementary Figure 5).
Taken together, for biomarkers which have been previously reported to be prognostic in HNSCC these analyses validate their role in an independent data set. Most biological factors as determined by the selected biomarkers are significantly associated with PFS thereby confirming their relevance. Overall, we find a prominent role for acute and chronic hypoxia and CD44 and SCL3A2 in our cohorts. We show that, from all, chronic hypoxia appears to be the most specific to LRC. In contrast, HR values from EMT and proliferation based splits are greater when assessing DM. Furthermore, these data reveal a role for the immune cell and proliferation related biomarkers in HNSCC outcome after definitive chemo-radiotherapy.
The Relative Role of Biological Factors in Chemo-Radiotherapy Outcomes in HNSCC
The biological markers have been tested independently of each other and most are significantly associated with patient outcome thereby supporting their role in HNSCC and treatment response. However, tumor biology and determinants of radioresistance are multifactorial and may depend on the context and relation to each other. We therefore aimed to identify the most relevant markers in a multivariable analysis. To this end we used a backward selection method. This method creates a Cox proportional hazard model using all available factors. It then iteratively eliminates the least relevant factor until no further decrease in AIC, a measure of model performance, is possible. From these analyses (Supplementary Table 4), we conclude that chronic hypoxia, EGFR expression, CD8+/Treg, T-cell infiltration, and CD44 are the most relevant biological factors that are associated with locoregional control. Multivariable analyses (Figure 4) also demonstrate that they are independent from relevant clinical factors such as cumulative cisplatin dose or sex. Cisplatin dose, age and sex are the clinical factors most associated with locoregional control in this cohort (Figure 4 and Supplementary Table 4). Broadly consistent with the results from the multivariate analyses that were performed on the biomarkers on an individual basis, EGFR and immune cell related factors remain important in instituting an increased risk for distant metastasis, while chronic hypoxia and CD44 are less relevant. Instead, tumor EMT and proliferation affects progression free survival most profoundly and independent of other important factors such as tumor volume or cisplatin dose (Supplementary Figure 8 and Supplementary Table 4). The consistent worse prognosis and distant metastasis association of patients with tumors that score high in the CD8+ T cells and related gene expression signatures is remarkable. High CD8+ T cell scores, as determined by these signatures or by immunohistochemistry, have been reported to be linked to good prognosis in other heterogeneous HNSCC cohorts (6, 56, 77) and prompted us to analyze this further (Supplementary Figures 9, 10). These analyses suggest that the lack of a good prognosis association could be based on the absence of HPV-positive HNSCC which show overall higher CD8 expression and CD8+ T-cell signature scores in the TCGA cohort (Supplementary Figure 9A). Within the HPV-positive group, high CD8 expression is strongly associated with good prognosis (Supplementary Figure 9B). Notably, CD8A/B expression and CD8+ T-cell signature values do not correlate well (Supplementary Figure 10). Interestingly, the observed outcome associations in HPV-negative HNSCC appear to be dependent on cumulative cisplatin dose (Supplementary Figure 10).
Figure 4.
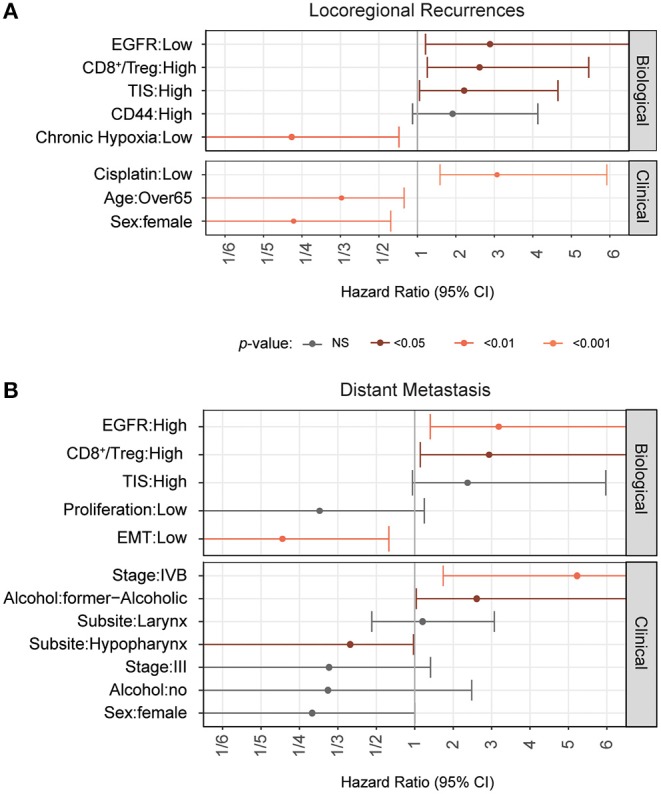
Relative role of biological markers in combined analyses. Forest plots with results from full multivariate Cox Proportional Hazards models are shown. The model was generated using a backward selection procedure. The most frequent level was used as the reference level for this analysis. A Cox proportional hazard model was fit that included all biological markers and clinical variables. Then, each variable was individually eliminated from the model and improvements in model performance were assessed. This process was repeated with the best performing models until the removal of variables did no longer improve the models. Hazard ratios for locoregional recurrences (A) and distant metastasis (B) as determined by the final model are shown.
The obvious divergence in the biomarker associations with local treatment outcomes compared to DM development risks prompted us to investigate this further. Unable to classify patients according to “true” biological parameter classes, we relied on bootstrapping methods to provide cut-offs for each outcome endpoints. As described above those resulted to be largely different in some cases such as for EGFR expression and pointed to a different influence in the respective biological mechanisms. We therefore compared the biological markers with respect to their influence in locoregional control or DM risk in a less cutoff-dependent manner by computing the AUC of the hazard ratio plots from multivariable regression analysis with clinical variables (Supplementary Figure 11). Figure 5 shows an overview of the impact of the individual biological parameters on locoregional control or distant metastasis risk. This analysis highlights the difference in the collection of the most relevant survival determinants for each outcome endpoint. Notably, locoregional control is mainly determined by chronic hypoxia, but also acute hypoxia. CD44 expression and CD8+ T-cell/Treg ratio are more relevant to LRC than DM, whereas distant metastasis is predominantly influenced by EMT, acute hypoxia, proliferation and EGFR status.
Figure 5.
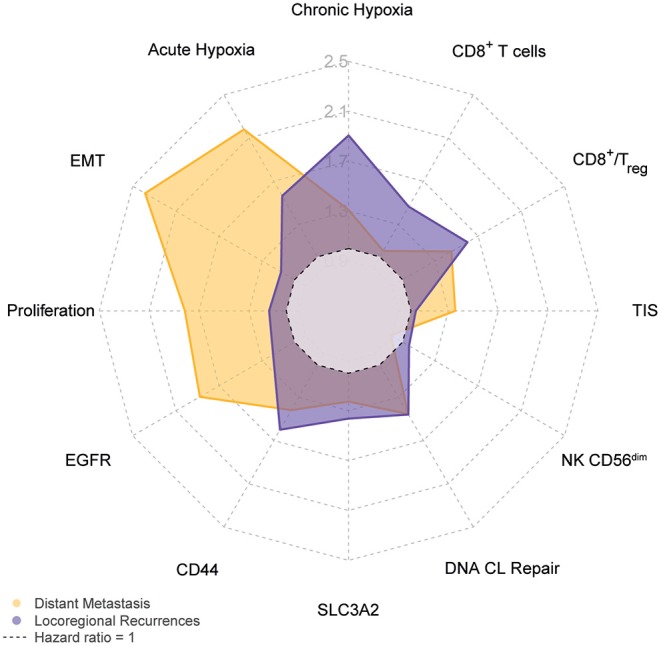
Divergence in biological parameter role for locoregional or distant control. The spider plot depicts the average hazard ratio as obtained after testing all possible cutoffs in a multivariable Cox proportional hazard analysis that included relevant clinical factors as shown in Supplementary Figure 8 and described in Materials and Methods. Hazard ratios for locoregional recurrences are shown in purple and distant metastasis hazard ratios in yellow.
Discussion
Here, we aimed to evaluate the relevance and interrelation of biological factors known to influence radiation response as determined in preclinical studies. Limited by the size of the study cohort, we restricted the study to markers for which discriminative power has been reported in clinical data in HNSCC and added clinical or biological factors that have shown an important association with radiotherapy outcomes. Using RNA-sequencing data from a large and relative uniform cohort of 197 HPV-negative advanced stage HNSCC patients that were all treated with cisplatin-based chemo-radiotherapy, we find an important role of immune cell (T cell) markers in locoregional control which suggests a role in radiation response. We also show that chronic and acute hypoxia are robustly associated with locoregional control. Similarly, we validated the equally important role of CD44 and SCL3A2, in part related to stem cells, in our study cohort. When assessed in combination, hypoxia, immune cells, EGFR are the most discriminating independent factors in LRC. For DM, those also include EMT. Overall, considered in the context of clinical factors and each other, our study underscores the relevance of many of these biological factors in HNSCC chemo-radiotherapy outcomes.
To advance previous findings on determinants of chemo-radiotherapy outcomes and to prioritize prognostic markers for multi-parametric prediction models, we focused on (i) the validation of expression-based prognostic markers in the chemo-radiotherapy setting and (ii) the evaluation of their complementarity and (iii) the assessment of any dependence to important clinical or other biologic factors. Many HNSCC studies highlight the role of biology for outcome (3–6, 78). A major drawback however for many of such studies is the heterogeneity of the HNSCC patient cohorts or a lack of contextual analyses (78). If focused on tumor site they often encompass many different treatments or if focused on treatment they combine different tumor sites, HPV-negative and positive. Large multicentric studies are therefore valuable contributions to the field (12, 13, 15, 16, 57) that provide insights to the biology of HNSCC and its link to patient outcome (5, 6, 27, 28, 79, 80). Clinical factors are important (81, 82) but are often not considered in multivariable analyses (78, 83). A lack of tumor volume data for example, even though clearly linked to LRC (81, 84–86), impedes the assessment of a role for or a bias from tumor volumes in such analyses. To minimize such treatment or tumor site related bias due to possible interactions; we deliberately excluded the biologically distinct oral cavity and HPV-positive oropharyngeal HNSCC (14, 16, 87–90) in our study. Our cohort also solely comprises definitive chemo-radiotherapy-treated advanced HNSCC. In contrast to predetermined gene sets in nanostring technologies, the availability of full transcriptomic data by RNA-Seq allowed us to test selected gene expressions and signatures related to the biological processes that we queried. Together we were able to show that most of the selected markers or marker categories are not related, are independently linked to outcome and that outcome associations are not based on links with known important clinical factors. Overall, we observed little or no influence or interactions with clinical factors, with the notable exception of tumor volume and cumulative cisplatin dose, factors often not accounted for in other biomarker studies. While correlations within the immune markers were expected, here we reveal an association with acute hypoxia scores which in turn appears to be linked to proliferation. Such relations or complementarities can alter the prognostic value or impede a discrimination of the true source of the observed outcome relevance. It however highlights the importance to study such markers in the context of each other and within the same cohort. Overall, our study pinpoints expression markers that should be considered as valuable contributors of future multi-parametric prediction models that combine clinical, radiologic, pathological and genetic variables for improved prognosis in advanced HPV-negative HNSCC (91, 92).It is difficult to discern factors that determine tumor radioresistance (83). A comparison of similar patient cohorts treated without or with different doses of radiotherapy would be required to strengthen such a link. Since cisplatin-based chemo-radiotherapy has become a standard treatment for HNSCC to improve quality of life by achieving organ preservation, surgically resected HNSCC patients with similar clinical tumor characteristics are rare, impeding such comparisons. However, in the absence of a comparable but non-radiotherapy treated study cohort, differences in LRC (mostly achieved by radiotherapy) as defined by the biomarker classification, can suggest a role in radiation response. In our study, we assured that important clinical factors that impact patient outcomes have been considered to limit bias or dependence. DM events may have occurred prior to LRC events and could have masked a greater impact in radiation response, such as in the case of acute hypoxia that also shows a strong association with DM. The comparison of LRC with DM further helped to discern a more radiation response specific role from a role in metastasis. Our data here and those reported by us and others do indeed confirm the role of hypoxia in determining radiation response as reflected by the LRC rates (25, 27, 29). In addition, hypoxia has been also implicated in tumor cell invasiveness, facilitating dissemination, and has been therefore associated with metastasis formation, a role that is also evident from our DM analyses. Similarly, we have recently shown that HNSCC cell lines with DNA crosslink repair defects are more migratory and invasive (63), a feature that may explain the association with DM prognosis but could also result in a greater regional spread and failure of locoregional control.
After the initial EGFR studies in clinic and the success of cetuximab combinations (40, 93, 94), cetuximab in HNSCC and the role of EGFR amplification and expression have been disputed since then (95). Most of these studies focused on the very high expressing or used a median cut-off to detect an association with the clinical endpoints analyzed. Here we see a clear role for EGFR in the outcome data when also considering hypoxia and other factors in multivariable analyses. Average to high EGFR expression, is linked to improved LRC when analyzed individually. The association of a low EGFR expressing group with poor LRC however becomes much clearer in the combined multivariable analyses that integrated all relevant biomarkers. It epitomizes the importance of combined analysis, as the prevalence of other, also clinical, factors in the different EGFR expression classified groups may have shifted or masked a possible influence in other studies if not accounted for, as revealed here. Given its role in promoting cell cycle progression, it is conceivable that increased EGFR levels mediate an increase in tumor repopulation between fractions; a radiotherapy response determining process that is counteracted by radiotherapy treatment acceleration or concurrent chemotherapy. This process is therefore limited in our patient population in contrast to some earlier studies that analyzed the influence of EGFR (96). Notably, the association with improved LRC is still discernible (HR = 0.57, p = 0.067) when reanalyzing the data using the higher EGFR expression cut-off that was used for the DM data. DM HR values however drop to 0.57 (p = 0.2) showing a DM link only in the top 25% EGFR expression group (HR = 3.19, p = 0.0056). This more aggressive nature of highly EGFR expressing tumors is consistent with other reports in HNSCC and other cancer types (97).
Our study is limited by statistical constraints due to the cohort size. This enforced us to limit the biological variables and apply selection processes such as the bootstrapping analyses. Yet, it becomes evident that the prognostic value of many of the factors could be validated in our cohort and withstood multivariable analyses with the important clinical variables. Among the clinical variables, we observe a trend toward poor outcomes in current smokers, however this does not reach significance in our cohort. Low numbers in the former smoker category but also the lack of more accurate smoking status values may have decreased the power to reveal the reported association with smoking (79, 98, 99). Since we focused on known determinants of radiation response, other biomarkers were not included despite their relevance or prognostic value in HNSCC (5, 6, 16, 100–106). Some, such as tumor mutational burden (TMB) are prevalent in laryngeal and HPV-negative pharyngeal HNSCC (14) but require DNA sequencing data. TMB was found to be associated with poor prognosis in HPV-negative chemo-radiotherapy treated patients in our previous study (36) and more strongly so in a cohort of patients that also included oral cavity cancers and HPV-positive oropharyngeal (107). Interestingly, low immune cell infiltration or CD8+ T cell values, as assessed by gene expression, have been assigned to HNSCC high in TMB or mutational signatures related to smoking (56, 107).
Other limitations result from technical challenges. Here we detect different biological processes and factors in clinical samples by using published and validated expression signatures—that are linked to these processes. These gene expression signatures may not be perfect identification tools for the specific biology in question (83); however they often reflect the abundance of certain biological elements well (108, 109). The DNA CL repair defect prediction model has for example been generated using functional endpoints and then validated in independent cell line panels or by genetic modification. On the other hand, markers such as CD44 are less clear defined. CD44 expression is associated with stem cell-ness in tumor cells (110), but it is also expressed under hypoxic conditions or in epithelial cells and is a marker for effector memory T cells (45). Therefore, it is particularly interesting to observe the correlation with SLC3A2 another stem cell related marker in our samples which confirms its link to tumor stem cell abundance. Notably, we find a correlation between acute hypoxia and TIS or CD8+ T-cell scores, suggesting a higher T-cell content in acute hypoxic areas or tumors which could be proposed to be driven by hypoxia induced inflammatory cytokine release (111). This T-cell/acute hypoxia correlation may in part also be responsible for the consistent poor outcome association of the CD8+ T-cell gene expression signatures. Reiterating the role of technical limitations, it should be noted that these gene expression signatures were based on transcriptional profiles of purified immune cell subsets. Through multiple adaptation steps, they evolved to markers that allowed further discrimination in the context of colorectal carcinoma and HNSCC (56, 75, 76). In terms of identification accuracy there are potential challenges with such technical approaches that can also explain discrepancies with immunohistochemistry determined factors. It is evident that the tumor context affects gene expression of the immune cells and, on the other hand, tumor gene expression features, if present in these signatures, can compound the identification. For instance, the CD8+ T cell signature includes ZEB1 expression, a protein involved in EMT and a poor prognostic factor in HNSCC (56, 76, 112–115). We therefore assessed CD8A and B gene expression in our samples as a simple surrogate for CD8+ T cells and show its limited complementarity with the CD8+ T cell signature score and associations with outcome. The better LRC outcome of patients with CD8 positive tumors in the low cumulative cisplatin patient category is in line with previous report based on IHC (116) The lack of an association with outcome in patients that received high cisplatin doses however demonstrates treatment dependence and explains the discrepancy to other studies (6, 77) when considering this clinical variable in our cisplatin treated cohort. Despite a significant but weak correlation with CD8A expression, high CD8+ T cell signature values are associated with poor outcomes, demonstrating the influence of the other features in this discriminating signature. Immune cell identification by gene expression may not be flawless. Yet, together, our data indicate a prognosis association that is linked to this particular patient treatment. One could speculate that hematologic toxicities associated with cisplatin administration could contribute to this pattern by abolishing the benefit from an immune cell rich tumor status in these individuals. On the other hand, recent studies suggest an enhancement of antitumor immunity by cisplatin that could also diminish the impact of the pre-treatment immune status (117, 118). While the primary emphasis for prognostic biomarkers lays in the discriminatory power to predict patient outcome, the focus of biomarkers for targeting opportunities is the achievement of an accurate representation of the marked biological process or elements. The signatures used here were selected based on their reported association with both immune cell infiltration and prognosis in HNSCC (56, 76). Yet the question remains whether they reflect CD8+ T cell infiltration well.
Interestingly, we did find a seemingly independent and consistent role for CD8+, non-regulatory, T cells in our study cohort. Observed for resected HNSCC in overall survival outcome data before, here we show an association with both, LRC and DM, in chemo-radiotherapy treated HNSCC patients indicating those with a high abundance of such T cells to have a worse prognosis. To our knowledge this poor prognosis association with radiation response has not been reported previously (6, 77, 119). As detailed above, this discrepancy with other studies is only in part explained by the used technology (116, 120) (IHC CD8 expression vs. gene expression signatures) since the signatures showed a good prognosis association in the Mandal et al. (56). Careful inspection of the TCGA data revealed increased CD8+ T-cell gene expression signature scores in the HPV-positive oropharyngeal that drive the good prognosis association. A pattern observed in other studies as well (56, 77, 121–124). Mandal et al. adjusted for HPV-associated outcome differences, which does not account for a possible interaction between the two variables (56). The CD8A and B expression HR plots in our analyses however suggest a stronger effect in the HPV-positive subgroup. Despite obvious evaluation challenges when using the different techniques and associated cut-offs, a similar argument applies to other studies based on immunohistochemistry determined CD8+ T cell infiltration values. A significant HPV status association got lost in multivariable analyses that indicated a good prognosis association of CD8+ T cells in oropharyngeal squamous cell carcinoma patients (59). Yet, some studies also show a good prognosis association with TIS or CD8+ T cells in HPV-negative patients using other scorings, cut offs and expression signatures (125). Since the effect size can be small, patient treatment associations with survival are often not significant in small studies. Treatment could however alter prognosis in subsets of patients. For instance, patients with tumors with DNA crosslink repair defects benefit most from a high cumulative cisplatin dose (63). Similarly, possible immune cell infiltration links could depend on treatment. Despite worse PFS in cases that lack or show minimal CD8A or CD8B expression, we cannot observe the previously reported poor prognosis link in CD8+ T cell signature low patients in our cohort. No associations between TIS or CD8+ scores and clinical variables were found; and outcome association links derived from the correlation with acute hypoxia should have been accounted for by the multivariable analyses. Together, our data suggest a role for HNSCC treatment, in particular cisplatin, in immune cell infiltration determined outcomes. Early cancer immunotherapy trials in HNSCC with immune checkpoint inhibitors demonstrate a benefit and underscore the potential value of immune response and chemo-radiotherapy relevant biomarkers to identify patients that will benefit from such treatments (24, 126–134). Larger comparative studies are therefore needed to disentangle the role of CD8+ T cells in the individual genetic HNSCC context and the important clinical variables connected to its role in patient outcome (78, 83, 135).
Our patient cohort is fairly unique in that it consists of definitive chemoradiotherapy treated advanced HNSCC patients. Based exclusively on resected HNSCC, these cases are unfortunately not present in the TCGA data. Supported by the detailed clinical data and follow up, this allowed us to elaborate on the role of biological determinants of chemoradiotherapy response. A quarter of the patients suffered from loco regional recurrences after treatment; a treatment success rate that further stresses the relevance of the biological factors found to determine treatment failure. This study does not provide or test clinically applicable prognostic markers. It was designed to compare the individual factors in relation to each other to assess and understand their influence in HNSCC outcome. Optimal cutoffs identified by the bootstrapping method and illustrated in the hazard ratio plots require validation for further development into true prognostic markers. Based on our results, future studies should focus on the elaboration of prognostic models that incorporate these biological markers together with important clinical factors. The multivariable outcome association results and the lack of correlations suggest that these future models should include all biological factors. Discrepancy in the optimal cutoff values further points to the value of non-dichotomized variables in such efforts and also reveals a possible cause of incongruent outcome associations in previous studies. The value of the clinical factors is exemplified by the fact that some biological markers (i.e., DNA CL repair or CD8+ T cells) lose their strength in patients groups with a high cumulative cisplatin dose.
While tumor stem cell targeting agents are still under development, some of the other biological factors are targetable. Next to high-dose alkylating agents, PARP inhibitors may help to exploit DNA CL repair defects (62) and different immunotherapy options are currently being tested in the HNSCC setting (136). The value of such biological markers in personalized treatments remains to be determined; however our study demonstrates that those patients are in need of improved therapy options.
In conclusion, this multicentric external validation study confirms the important and independent role of biological factors that embody hypoxia, stem cell-ness, tumor growth, EMT and DNA repair for locoregional control in chemoradiotherapy treated patients. The multifactorial analyses results highlight the need to consider these biomarkers in the context of each other and also revealed an important role for immune cell abundance in HNSCC treatment outcome.
Data Availability Statement
The data in this study is available the European Genome-phenome Archive (https://www.ebi.ac.uk/ega/) with the accession numbers: EGAD00001005721, EGAD00001005715, EGAD00001005716, EGAD00001005717, and study number EGAS00001004090.
Ethics Statement
The studies involving human participants were reviewed and approved by Institutional Review Board The Netherlands Cancer Institute, Amsterdam, The Netherlands; Institutional Review Board VuMC, Amsterdam, The Netherlands; Institutional Review Board Maastro, Maastricht, The Netherlands. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
CVen, MH, PE, and MJ contributed to the conception and design of the study. MH, RR, CVer, OH-V, FH, PL, HB, CL, MV, RB, and MB contributed to the acquisition of data. MH, RR, and FH established and/or curated databases. PE, MH, and SS performed data analysis. MH, CVen, PE, and MJ contributed to data interpretation. CVen, MH, and PE wrote the first draft of the manuscript. All authors contributed to manuscript revisions and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors are grateful for financial support from Brunel and Verwelius and would like to thank the NKI Genomics Core Facility for performing RNA sequencing, the NKI RHPC facility for providing computational resources and the Core Facility-Molecular Pathology and Biobank (CFMPB) for collecting and preparing tissue samples.
Footnotes
Funding. Authors acknowledge financial support from the Dutch Cancer Society (KWF-A6C7072, acronym DESIGN), from the EU 7th framework program (no 257144, acronym ARTFORCE) and the ERC advanced grant (no 694812, acronym Hypoximmuno).
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2019.01470/full#supplementary-material
References
- 1.Baumann M, Krause M, Overgaard J, Debus J, Bentzen SM, Daartz J, et al. Radiation oncology in the era of precision medicine. Nat Rev Cancer. (2016) 16:234–49. 10.1038/nrc.2016.18 [DOI] [PubMed] [Google Scholar]
- 2.van der Kogel A. Basic Clinical Radiobiology, 4th edn. London: CRC Press; (2009). 10.1201/b13224 [DOI] [Google Scholar]
- 3.Alsahafi E, Begg K, Amelio I, Raulf N, Lucarelli P, et al. Clinical update on head and neck cancer: molecular biology and ongoing challenges. Cell Death Dis. (2019) 10:540. 10.1038/s41419-019-1769-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Leemans CR, Braakhuis BJM, Brakenhoff RH. The molecular biology of head and neck cancer. Nat Rev Cancer. (2011) 11:9–22. 10.1038/nrc2982 [DOI] [PubMed] [Google Scholar]
- 5.Economopoulou P, de Bree R, Kotsantis I, Psyrri A. Diagnostic tumor markers in head and neck squamous cell carcinoma (HNSCC) in the clinical setting. Front Oncol. (2019) 9:827. 10.3389/fonc.2019.00827 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Budach V, Tinhofer I. Novel prognostic clinical factors and biomarkers for outcome prediction in head and neck cancer: a systematic review. Lancet Oncol. (2019) 20:e313–26. 10.1016/S1470-2045(19)30177-9 [DOI] [PubMed] [Google Scholar]
- 7.Kang H, Kiess A, Chung CH. Emerging biomarkers in head and neck cancer in the era of genomics. Nat Rev Clin Oncol. (2015) 12:11–26. 10.1038/nrclinonc.2014.192 [DOI] [PubMed] [Google Scholar]
- 8.Petersen JF, Timmermans AJ, van Dijk BAC, Overbeek LIH, Smit LA, Hilgers FJM, et al. Trends in treatment, incidence and survival of hypopharynx cancer: a 20-year population-based study in the Netherlands. Eur Arch Oto Rhino Laryngol. (2018) 275:181–9. 10.1007/s00405-017-4766-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Timmermans AJ, van Dijk BAC, Overbeek LIH, van Velthuysen M-LF, van Tinteren H, Hilgers FJM, et al. Trends in treatment and survival for advanced laryngeal cancer: a 20-year population-based study in The Netherlands. Head Neck. (2015) 38 (Suppl. 1):E1247–55. 10.1002/hed.24200 [DOI] [PubMed] [Google Scholar]
- 10.Price KAR, Cohen EE. Current treatment options for metastatic head and neck cancer. Curr Treat Options Oncol. (2012) 13:35–46. 10.1007/s11864-011-0176-y [DOI] [PubMed] [Google Scholar]
- 11.Huang SH, O'Sullivan B. Overview of the 8th Edition TNM classification for head and neck cancer. Curr Treat Options Oncol. (2017) 18:40. 10.1007/s11864-017-0484-y [DOI] [PubMed] [Google Scholar]
- 12.Lawrence MS, Sougnez C, Lichtenstein L, Cibulskis K, Lander E, Gabriel SB, et al. Comprehensive genomic characterization of head and neck squamous cell carcinomas. Nature. (2015) 517:576–82. 10.1038/nature14129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Stransky N, Egloff AM, Tward AD, Kostic AD, Cibulskis K, Sivachenko A, et al. The mutational landscape of head and neck squamous cell carcinoma. Science. (2011) 333:1157–60. 10.1126/science.1208130 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Vossen DM, Verhagen CVM, Verheij M, Wessels LFA, Vens C, van den Brekel MWM. Comparative genomic analysis of oral versus laryngeal and pharyngeal cancer. Oral Oncol. (2018) 81:35–44. 10.1016/j.oraloncology.2018.04.006 [DOI] [PubMed] [Google Scholar]
- 15.Agrawal N, Frederick MJ, Pickering CR, Bettegowda C, Chang K, Li RJ, et al. Exome sequencing of head and neck squamous cell carcinoma reveals inactivating mutations in NOTCH1. Science. (2011) 333:1154–7. 10.1126/science.1206923 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Dogan S, Xu B, Middha S, Vanderbilt CM, Bowman AS, Migliacci J, et al. Identification of prognostic molecular biomarkers in 157 HPV-positive and HPV-negative squamous cell carcinomas of the oropharynx. Int J Cancer. (2019) 145:3152–62. 10.1002/ijc.32412 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Theelen WSME, Peulen HMU, Lalezari F, van der Noort V, de Vries JF, Aerts JGJV, et al. Effect of pembrolizumab after stereotactic body radiotherapy vs pembrolizumab alone on tumor response in patients with advanced non–small cell lung cancer. JAMA Oncol. (2019) 5:1276–82. 10.1001/jamaoncol.2019.1478 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ngwa W, Irabor OC, Schoenfeld JD, Hesser J, Demaria S, Formenti SC. Using immunotherapy to boost the abscopal effect. Nat Rev Cancer. (2018) 18:313–22 10.1038/nrc.2018.6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tinhofer I, Budach V, Johrens K, Keilholz U. The rationale for including immune checkpoint inhibition into multimodal primary treatment concepts of head and neck cancer. Cancers Head Neck. (2016) 1:8. 10.1186/s41199-016-0009-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bristow RG, Alexander B, Baumann M, Bratman SV, Brown JM, Camphausen K, et al. Combining precision radiotherapy with molecular targeting and immunomodulatory agents: a guideline by the American Society for Radiation Oncology. Lancet Oncol. (2018) 19:e240–51. 10.1016/S1470-2045(18)30096-2 [DOI] [PubMed] [Google Scholar]
- 21.Swart M, Verbrugge I, Beltman JB. Combination approaches with immune-checkpoint blockade in cancer therapy. Front Oncol. (2016) 6:233. 10.3389/fonc.2016.00233 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Canning M, Guo G, Yu M, Myint C, Groves MW, Byrd JK, Cui Y. Heterogeneity of the head and neck squamous cell carcinoma immune landscape and its impact on immunotherapy. Front Cell Dev Biol. (2019) 7:52. 10.3389/fcell.2019.00052 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Economopoulou P, Agelaki S, Perisanidis C, Giotakis EI, Psyrri A. The promise of immunotherapy in head and neck squamous cell carcinoma. Ann Oncol Off J Eur Soc Med Oncol. (2016) 27:1675–85. 10.1093/annonc/mdw226 [DOI] [PubMed] [Google Scholar]
- 24.Solomon B, Young RJ, Rischin D. Head and neck squamous cell carcinoma: genomics and emerging biomarkers for immunomodulatory cancer treatments. Semin Cancer Biol. (2018) 52:228–40. 10.1016/j.semcancer.2018.01.008 [DOI] [PubMed] [Google Scholar]
- 25.Toustrup K, Sørensen BS, Nordsmark M, Busk M, Wiuf C, Alsner J, Overgaard J. Development of a hypoxia gene expression classifier with predictive impact for hypoxic modification of radiotherapy in head and neck cancer. Cancer Res. (2011) 71:5923–31. 10.1016/S0167-8140(11)70012-3 [DOI] [PubMed] [Google Scholar]
- 26.Tawk B, Schwager C, Deffaa O, Dyckhoff G, Warta R, Linge A, et al. Comparative analysis of transcriptomics based hypoxia signatures in head- and neck squamous cell carcinoma. Radiother Oncol. (2016) 118:350–8. 10.1016/j.radonc.2015.11.027 [DOI] [PubMed] [Google Scholar]
- 27.Linge A, Lohaus F, Löck S, Nowak A, Gudziol V, Valentini C, et al. HPV status, cancer stem cell marker expression, hypoxia gene signatures and tumour volume identify good prognosis subgroups in patients with HNSCC after primary radiochemotherapy: A multicentre retrospective study of the German Cancer Consortium Radiation. Radiother Oncol. (2016) 121:364–73. 10.1016/j.radonc.2016.11.008 [DOI] [PubMed] [Google Scholar]
- 28.Linge A, Lock S, Gudziol V, Nowak A, Lohaus F, von Neubeck C, et al. Low cancer stem cell marker expression and low hypoxia identify good prognosis subgroups in HPV(-) HNSCC after postoperative radiochemotherapy: a multicenter study of the DKTK-ROG. Clin Cancer Res. (2016) 22:2639–49. 10.1158/1078-0432.CCR-15-1990 [DOI] [PubMed] [Google Scholar]
- 29.van der Heijden M, de Jong MC, Verhagen CVM, de Roest RH, Sanduleanu S, Hoebers F, et al. Acute hypoxia profile is a stronger prognostic factor than chronic hypoxia in advanced stage head and neck cancer patients. Cancers. (2019) 11:E583. 10.3390/cancers11040583 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rademakers SE, Hoogsteen IJ, Rijken PF, Oosterwijk E, Terhaard CH, Doornaert PA, et al. Pattern of CAIX expression is prognostic for outcome and predicts response to ARCON in patients with laryngeal cancer treated in a phase III randomized trial. Radiother Oncol. (2013) 108:517–22. 10.1016/j.radonc.2013.04.022 [DOI] [PubMed] [Google Scholar]
- 31.Thomson D, Yang H, Baines H, Miles E, Bolton S, West C, et al. NIMRAD - A phase III trial to investigate the use of nimorazole hypoxia modification with intensity-modulated radiotherapy in head and neck cancer. Clin Oncol. (2014) 26:344–7. 10.1016/j.clon.2014.03.003 [DOI] [PubMed] [Google Scholar]
- 32.Kaanders JHAM, Bussink J, Van der Kogel AJ. ARCON: a novel biology-based approach in radiotherapy. Lancet Oncol. (2002) 3:728–37. 10.1016/S1470-2045(02)00929-4 [DOI] [PubMed] [Google Scholar]
- 33.Overgaard J. Hypoxic modification of radiotherapy in squamous cell carcinoma of the head and neck - A systematic review and meta-analysis. Radiother Oncol. (2011) 100:22–32. 10.1016/S0167-8140(11)70167-0 [DOI] [PubMed] [Google Scholar]
- 34.Overgaard J, Hansen HS, Specht L, Overgaard M, Grau C, Andersen E, et al. Five compared with six fractions per week of conventional radiotherapy of squamous-cell carcinoma of head and neck: DAHANCA 6&7 randomised controlled trial. Lancet. (2003) 362:933–40. 10.1016/S0140-6736(03)14361-9 [DOI] [PubMed] [Google Scholar]
- 35.Bentzen SM, Thames HD. Clinical evidence for tumor clonogen regeneration: interpretations of the data. Radiother Oncol. (1991) 22:161–6. 10.1016/0167-8140(91)90019-D [DOI] [PubMed] [Google Scholar]
- 36.Vossen DM, Verhagen CVM, Van Der Heijden M, Essers PBM, Bartelink H, Verheij M, et al. Genetic factors associated with a poor outcome in head and neck cancer patients receiving definitive chemoradiotherapy. Cancers. (2019) 11:E445. 10.3390/cancers11040445 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ang KK. Multidisciplinary management of locally advanced SCCHN: optimizing treatment outcomes. Oncologist. (2008) 13:899–910. 10.1634/theoncologist.2007-0157 [DOI] [PubMed] [Google Scholar]
- 38.Bonner JA, Harari PM, Giralt J, Cohen RB, Jones CU, Sur RK, et al. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer. Lancet Oncol. (2010) 11:21–8. 10.1016/S1470-2045(09)70311-0 [DOI] [PubMed] [Google Scholar]
- 39.Bentzen SM, Atasoy BM, Daley FM, Dische S, Richman PI, Saunders MI, et al. Epidermal growth factor receptor expression in pretreatment biopsies from head and neck squamous cell carcinoma as a predictive factor for a benefit from accelerated radiation therapy in a randomized controlled trial. J Clin Oncol. (2005) 23:5560–7. 10.1200/JCO.2005.06.411 [DOI] [PubMed] [Google Scholar]
- 40.Bossi P, Resteghini C, Paielli N, Licitra L, Pilotti S, Perrone F. Prognostic and predictive value of EGFR in head and neck squamous cell carcinoma. Oncotarget. (2016) 7:74362–79. 10.18632/oncotarget.11413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Xu MJ, Johnson DE, Grandis JR. EGFR-targeted therapies in the post-genomic era. Cancer Metastasis Rev. (2017) 36:463–73. 10.1007/s10555-017-9687-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Juergens RA, Bratman SV, Tsao M-S, Laurie SA, Sara Kuruvilla M, Razak ARA, Hansen AR. Biology and patterns of response to EGFR-inhibition in squamous cell cancers of the lung and head & neck. Cancer Treat Rev. (2017) 54:43–57. 10.1016/j.ctrv.2017.01.003 [DOI] [PubMed] [Google Scholar]
- 43.Taberna M, Oliva M, Mesia R. Cetuximab-containing combinations in locally advanced and recurrent or metastatic head and neck squamous cell carcinoma. Front Oncol. (2019) 9:383 10.3389/fonc.2019.00383 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Starmans MHW, Krishnapuram B, Steck H, Horlings H, Nuyten DSA, Van De Vijver MJ, et al. Robust prognostic value of a knowledge-based proliferation signature across large patient microarray studies spanning different cancer types. Br J Cancer. (2008) 99:1884–90. 10.1038/sj.bjc.6604746 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.De Jong MC, Pramana J, Van Der Wal JE, Lacko M, Peutz-Kootstra CJ, De Jong JM, et al. CD44 expression predicts local recurrence after radiotherapy in larynx cancer. Clin Cancer Res. (2010) 16:5329–38. 10.1158/1078-0432.CCR-10-0799 [DOI] [PubMed] [Google Scholar]
- 46.Linge A, Schmidt S, Lohaus F, Krenn C, Bandurska-Luque A, Platzek I, et al. Independent validation of tumour volume, cancer stem cell markers and hypoxia-associated gene expressions for HNSCC after primary radiochemotherapy. Clin Transl Radiat Oncol. (2019) 16:40–7. 10.1016/j.ctro.2019.03.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Baumann M, Krause M, Hill R. Exploring the role of cancer stem cells in radioresistance. Nat Rev Cancer. (2008) 8:545–54. 10.1038/nrc2419 [DOI] [PubMed] [Google Scholar]
- 48.Krause M, Dubrovska A, Linge A, Baumann M. Cancer stem cells: radioresistance, prediction of radiotherapy outcome and specific targets for combined treatments. Adv Drug Deliv Rev. (2017) 109:63–73. 10.1016/j.addr.2016.02.002 [DOI] [PubMed] [Google Scholar]
- 49.Krause M, Yaromina A, Eicheler W, Koch U, Baumann M. Cancer stem cells: targets and potential biomarkers for radiotherapy. Clin Cancer Res. (2011) 17:7224–9. 10.1158/1078-0432.CCR-10-2639 [DOI] [PubMed] [Google Scholar]
- 50.Chen H-Y, Xu L, Li L-F, Liu X-X, Gao J-X, Bai Y-R. Inhibiting the CD8 + T cell infiltration in the tumor microenvironment after radiotherapy is an important mechanism of radioresistance. Sci Rep. (2018) 8:11934. 10.1038/s41598-018-30417-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Gupta A, Probst HC, Vuong V, Landshammer A, Muth S, Yagita H, et al. Radiotherapy promotes tumor-specific effector CD8 + T cells via dendritic cell activation. J Immunol. (2012) 189:558–66. 10.1158/1538-7445.TUMIMM2012-B1 [DOI] [PubMed] [Google Scholar]
- 52.Ran X, Yang K. Inhibitors of the PD-1/PD-L1 axis for the treatment of head and neck cancer: current status and future perspectives. Drug Des Devel Ther. (2017) 11:2007–14. 10.2147/DDDT.S140687 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Moskovitz J, Moy J, Ferris RL. Immunotherapy for head and neck squamous cell carcinoma. Curr Oncol Rep. (2018) 20:22. 10.1007/s11912-018-0654-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Economopoulou P, Kotsantis I, Psyrri A. Checkpoint inhibitors in head and neck cancer: rationale, clinical activity, and potential biomarkers. Curr Treat Options Oncol. (2016) 17:40. 10.1007/s11864-016-0419-z [DOI] [PubMed] [Google Scholar]
- 55.Van Limbergen EJ, De Ruysscher DK, Pimentel VO, Marcus D, Berbee M, Hoeben A, et al. Combining radiotherapy with immunotherapy: the past, the present and the future. Br J Radiol. (2017) 90:20170157. 10.1259/bjr.20170157 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Mandal R, Senbabaoglu Y, Desrichard A, Havel JJ, Dalin MG, Riaz N, et al. The head and neck cancer immune landscape and its immunotherapeutic implications. JCI Insight. (2016) 1:e89829. 10.1172/jci.insight.89829 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Balermpas P, Rodel F, Rodel C, Krause M, Linge A, Lohaus F, et al. CD8+ tumour-infiltrating lymphocytes in relation to HPV status and clinical outcome in patients with head and neck cancer after postoperative chemoradiotherapy: a multicentre study of the German cancer consortium radiation oncology group (DKTK-ROG). Int J Cancer. (2016) 138:171–81. 10.1002/ijc.29683 [DOI] [PubMed] [Google Scholar]
- 58.Ono T, Azuma K, Kawahara A, Akiba J, Kakuma T, Chitose S, et al. Pre-treatment CD8(+) tumour-infiltrating lymphocyte density predicts distant metastasis after definitive treatment in patients with stage III/IV hypopharyngeal squamous cell carcinoma. Clin Otolaryngol. (2018) 43:1312–20. 10.1111/coa.13171 [DOI] [PubMed] [Google Scholar]
- 59.De Meulenaere A, Vermassen T, Aspeslagh S, Deron P, Duprez F, Laukens D, et al. Tumor PD-L1 status and CD8(+) tumor-infiltrating T cells: markers of improved prognosis in oropharyngeal cancer. Oncotarget. (2017) 8:80443–52. 10.18632/oncotarget.19045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.De Meulenaere A, Vermassen T, Aspeslagh S, Zwaenepoel K, Deron P, Duprez F, et al. Prognostic markers in oropharyngeal squamous cell carcinoma: focus on CD70 and tumour infiltrating lymphocytes. Pathology. (2017) 49:397–404. 10.1016/j.pathol.2017.02.002 [DOI] [PubMed] [Google Scholar]
- 61.Verhagen CVM, Vossen DM, Borgmann K, Hageman F, Grénman R, Verwijs-Janssen M, et al. Fanconi anemia and homologous recombination gene variants are associated with functional DNA repair defects in vitro and poor outcome in patients with advanced head and neck squamous cell carcinoma. Oncotarget. (2018) 9:18198–213. 10.18632/oncotarget.24797 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Verhagen CVM, De Haan R, Hageman F, Oostendorp TPD, Carli ALE, O'Connor MJ, et al. Extent of radiosensitization by the PARP inhibitor olaparib depends on its dose, the radiation dose and the integrity of the homologous recombination pathway of tumor cells. Radiother Oncol. (2015) 116:358–65. 10.1016/j.radonc.2015.03.028 [DOI] [PubMed] [Google Scholar]
- 63.Essers PBM, van der Heijden M, Verhagen CVM, Ploeg EM, de Roest RH, Leemans CR, et al. Drug sensitivity prediction models reveal link between DNA repair defects and poor prognosis in HNSCC. Cancer Res. (2019) 79:5597–611. 10.1158/0008-5472.CAN-18-3388 [DOI] [PubMed] [Google Scholar]
- 64.Van der Heijden M, Essers P, Verheij M, Van den Brekel M, Vens C. OC-0487: EMT signatures as a prognostic marker for metastasis in HPV-negative HNSCC. Radiother Oncol. (2018) 127:S250–1. 10.1016/S0167-8140(18)30797-7 [DOI] [Google Scholar]
- 65.Balm AJM, Rasch CRN, Schornagel JH, Hilgers FJM, Keus RB, Schultze-Kool L, et al. High-dose superselective intra-arterial cisplatin and concomitant radiation (radplat) for advanced head and neck cancer. Head Neck. (2004) 26:485–93. 10.1002/hed.20006 [DOI] [PubMed] [Google Scholar]
- 66.Al-Mamgani A, de Ridder M, Navran A, Klop WM, de Boer JP, Tesselaar ME. The impact of cumulative dose of cisplatin on outcome of patients with head and neck squamous cell carcinoma. Eur Arch Oto Rhino Laryngol. (2017) 274:3757–65. 10.1007/s00405-017-4687-4 [DOI] [PubMed] [Google Scholar]
- 67.Spreafico A, Huang SH, Xu W, Granata R, Liu CS, Waldron JN, et al. Impact of cisplatin dose intensity on human papillomavirus-related and -unrelated locally advanced head and neck squamous cell carcinoma. Eur J Cancer. (2016) 67:174–82. 10.1016/j.ejca.2016.08.013 [DOI] [PubMed] [Google Scholar]
- 68.Heukelom J, Hamming O, Bartelink H, Hoebers F, Giralt J, Herlestam T, et al. Adaptive and innovative Radiation Treatment FOR improving Cancer treatment outcomE (ARTFORCE); a randomized controlled phase II trial for individualized treatment of head and neck cancer. BMC Cancer. (2013) 13:84. 10.1186/1471-2407-13-84 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Lewis JS, Chernock RD, Ma XJ, Flanagan JJ, Luo Y, Gao G, et al. Partial p16 staining in oropharyngeal squamous cell carcinoma: extent and pattern correlate with human papillomavirus RNA status. Mod Pathol. (2012) 25:1212–20. 10.1038/modpathol.2012.79 [DOI] [PubMed] [Google Scholar]
- 70.Kim D, Pertea G, Trapnell C, Pimentel H, Kelley R, Salzberg SL. TopHat2: accurate alignment of transcriptomes in the presence of insertions, deletions and gene fusions. Genome Biol. (2013) 14:R36. 10.1186/gb-2013-14-4-r36 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Anders S, Pyl PT, Huber W. HTSeq-A Python framework to work with high-throughput sequencing data. Bioinformatics. (2015) 31:166–9. 10.1093/bioinformatics/btu638 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Hänzelmann S, Castelo R, Guinney J. GSVA: gene set variation analysis for microarray and RNA-Seq data. BMC Bioinform. (2013) 14:7. 10.1186/1471-2105-14-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Seigneuric R, Starmans MHW, Fung G, Krishnapuram B, Nuyten DSA, van Erk A, et al. Impact of supervised gene signatures of early hypoxia on patient survival. Radiother Oncol. (2007) 83:374–82. 10.1016/j.radonc.2007.05.002 [DOI] [PubMed] [Google Scholar]
- 74.Lohaus F, Linge A, Tinhofer I, Budach V, Gkika E, Stuschke M, et al. HPV16 DNA status is a strong prognosticator of loco-regional control after postoperative radiochemotherapy of locally advanced oropharyngeal carcinoma: results from a multicentre explorative study of the German Cancer Consortium Radiation Oncology Group. Radiother Oncol. (2014) 113:317–23. 10.1016/j.radonc.2014.11.011 [DOI] [PubMed] [Google Scholar]
- 75.Senbabaoglu Y, Winer AG, Gejman RS, Liu M, Luna A, Ostrovnaya I, et al. The landscape of {T} cell infiltration in human cancer and its association with antigen presenting gene expression. bioRxiv. (2015). 10.1101/025908 [DOI] [Google Scholar]
- 76.Bindea G, Mlecnik B, Tosolini M, Kirilovsky A, Waldner M, Obenauf AC, et al. Spatiotemporal dynamics of intratumoral immune cells reveal the immune landscape in human cancer. Immunity. (2013) 39:782–95. 10.1016/j.immuni.2013.10.003 [DOI] [PubMed] [Google Scholar]
- 77.De Meulenaere A, Vermassen T, Aspeslagh S, Vandecasteele K, Rottey S, Ferdinande L. TILs in head and neck cancer: ready for clinical implementation and Why (Not)? Head Neck Pathol. (2017) 11:354–63. 10.1007/s12105-016-0776-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Kim KY, McShane LM, Conley BA. Designing biomarker studies for head and neck cancer. Head Neck. (2014) 36:1069–75. 10.1002/hed.23444 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Lassen P, Lacas B, Pignon J-P, Trotti A, Zackrisson B, Zhang Q, et al. Prognostic impact of HPV-associated p16-expression and smoking status on outcomes following radiotherapy for oropharyngeal cancer: The MARCH-HPV project. Radiother Oncol. (2018) 126:107–15. 10.1016/j.radonc.2017.10.018 [DOI] [PubMed] [Google Scholar]
- 80.O'Sullivan B, Huang SH, Su J, Garden AS, Sturgis EM, Dahlstrom K, et al. Development and validation of a staging system for HPV-related oropharyngeal cancer by the International Collaboration on Oropharyngeal cancer Network for Staging (ICON-S): a multicentre cohort study. Lancet Oncol. (2016) 17:440–51. 10.1016/S1470-2045(15)00560-4 [DOI] [PubMed] [Google Scholar]
- 81.Hoebers F, Rios E, Troost E, van den Ende P, Kross K, Lacko M, et al. Definitive radiation therapy for treatment of laryngeal carcinoma: impact of local relapse on outcome and implications for treatment strategies. Strahlentherapie und Onkol Organ der Dtsch Rontgengesellschaft. (2013) 189:834–41. 10.1007/s00066-013-0414-2 [DOI] [PubMed] [Google Scholar]
- 82.Silva P, Homer JJ, Slevin NJ, Musgrove BT, Sloan P, Price P, et al. Clinical and biological factors affecting response to radiotherapy in patients with head and neck cancer: a review. Clin Otolaryngol. (2007) 32:337–45. 10.1111/j.1749-4486.2007.01544.x [DOI] [PubMed] [Google Scholar]
- 83.Lucs A, Saltman B, Chung CH, Steinberg BM, Schwartz DL. Opportunities and challenges facing biomarker development for personalized head and neck cancer treatment. Head Neck. (2013) 35:294–306. 10.1002/hed.21975 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Welch ML, McIntosh C, Haibe-Kains B, Milosevic MF, Wee L, Dekker A, et al. Vulnerabilities of radiomic signature development: The need for safeguards. Radiother Oncol. (2019) 130:2–9. 10.1016/j.radonc.2018.10.027 [DOI] [PubMed] [Google Scholar]
- 85.Strongin A, Yovino S, Taylor R, Wolf J, Cullen K, Zimrin A, et al. Primary tumor volume is an important predictor of clinical outcomes among patients with locally advanced squamous cell cancer of the head and neck treated with definitive chemoradiotherapy. Int J Radiat Oncol Biol Phys. (2012) 82:1823–30. 10.1016/j.ijrobp.2010.10.053 [DOI] [PubMed] [Google Scholar]
- 86.Knegjens JL, Hauptmann M, Pameijer FA, Balm AJ, Hoebers FJ, de Bois JA, et al. Tumor volume as prognostic factor in chemoradiation for advanced head and neck cancer. Head Neck. (2011) 33:375–82. 10.1002/hed.21459 [DOI] [PubMed] [Google Scholar]
- 87.Gopinath D, Kunnath Menon R. Unravelling the molecular signatures in HNSCC: is the homogenous paradigm becoming obsolete? Oral Oncol. (2018) 82:195. 10.1016/j.oraloncology.2018.05.011 [DOI] [PubMed] [Google Scholar]
- 88.Pai SI, Westra WH. Molecular pathology of head and neck cancer: implications for diagnosis, prognosis, and treatment. Annu Rev Pathol. (2009) 4:49–70. 10.1146/annurev.pathol.4.110807.092158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.van Monsjou HS, Balm AJM, van den Brekel MM, Wreesmann VB. Oropharyngeal squamous cell carcinoma: a unique disease on the rise? Oral Oncol. (2010) 46:780–5. 10.1016/j.oraloncology.2010.08.011 [DOI] [PubMed] [Google Scholar]
- 90.Dogan V, Rieckmann T, Münscher A, Busch CJ. Current studies of immunotherapy in head and neck cancer. Clin Otolaryngol. (2018) 43:13–21. 10.1111/coa.12895 [DOI] [PubMed] [Google Scholar]
- 91.Caudell JJ, Torres-Roca JF, Gillies RJ, Enderling H, Kim S, Rishi A, et al. The future of personalised radiotherapy for head and neck cancer. Lancet Oncol. (2017) 18:e266–73. 10.1016/S1470-2045(17)30252-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Lambin P, Zindler J, Vanneste BGL, Van De Voorde L, Eekers D, Compter I, et al. Decision support systems for personalized and participative radiation oncology. Adv Drug Deliv Rev. (2017) 109:131–53. 10.1016/j.addr.2016.01.006 [DOI] [PubMed] [Google Scholar]
- 93.Cripps C, Winquist E, Devries MC, Stys-Norman D, Gilbert R. Epidermal growth factor receptor targeted therapy in stages III and IV head and neck cancer. Curr Oncol. (2010) 17:37–48. 10.3747/co.v17i3.520 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Grandis JR, Melhem MF, Gooding WE, Day R, Holst VA, Wagener MM, et al. Levels of TGF-α and EGFR protein in head and neck squamous cell carcinoma and patient survival. J Natl Cancer Inst. (1998) 90:824–32. 10.1093/jnci/90.11.824 [DOI] [PubMed] [Google Scholar]
- 95.Hutchinson L. Drug therapy: cetuximab or cisplatin in HNSCC? Nat Rev Clin Oncol. (2016) 13:66 10.1038/nrclinonc.2015.235 [DOI] [PubMed] [Google Scholar]
- 96.Ang KK, Berkey BA, Tu X, Zhang HZ, Katz R, Hammond EH, et al. Impact of epidermal growth factor receptor expression on survival and pattern of relapse in patients with advanced head and neck carcinoma. Cancer Res. (2002) 62:7350–6. [PubMed] [Google Scholar]
- 97.Nicholson R, Gee JM., Harper M. EGFR and cancer prognosis. Eur J Cancer. (2001) 37:(Suppl. 4):S9–15. 10.1016/S0959-8049(01)00231-3 [DOI] [PubMed] [Google Scholar]
- 98.Gillison ML, Zhang Q, Jordan R, Xiao W, Westra WH, Trotti A, et al. Tobacco smoking and increased risk of death and progression for patients with p16-positive and p16-negative oropharyngeal cancer. J Clin Oncol. (2012) 30:2102–11. 10.1200/JCO.2011.38.4099 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Gronhoj C, Jensen JS, Wagner S, Dehlendorff C, Friborg J, Andersen E, et al. Impact on survival of tobacco smoking for cases with oropharyngeal squamous cell carcinoma and known human papillomavirus and p16-status: a multicenter retrospective study. Oncotarget. (2019) 10:4655–63. 10.18632/oncotarget.27079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Hess J, Unger K, Maihoefer C, Schuttrumpf L, Wintergerst L, Heider T, et al. A five-MicroRNA signature predicts survival and disease control of patients with head and neck cancer negative for HPV infection. Clin Cancer Res. (2019) 25:1505–16. 10.1158/1078-0432.CCR-18-0776 [DOI] [PubMed] [Google Scholar]
- 101.Glorieux M, Dok R, Nuyts S. Novel DNA targeted therapies for head and neck cancers: clinical potential and biomarkers. Oncotarget. (2017) 8:81662–78. 10.18632/oncotarget.20953 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Bossi P, Alfieri S, Strojan P, Takes RP, Lopez F, Makitie A, et al. Prognostic and predictive factors in recurrent and/or metastatic head and neck squamous cell carcinoma: a review of the literature. Crit Rev Oncol Hematol. (2019) 137:84–91. 10.1016/j.critrevonc.2019.01.018 [DOI] [PubMed] [Google Scholar]
- 103.Foy J-P, Bazire L, Ortiz-Cuaran S, Deneuve S, Kielbassa J, Thomas E, et al. A 13-gene expression-based radioresistance score highlights the heterogeneity in the response to radiation therapy across HPV-negative HNSCC molecular subtypes. BMC Med. (2017) 15:165. 10.1186/s12916-017-0929-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Scott JG, Berglund A, Schell MJ, Mihaylov I, Fulp WJ, Yue B, et al. A genome-based model for adjusting radiotherapy dose (GARD): a retrospective, cohort-based study. Lancet Oncol. (2017) 18:202–11. 10.1016/S1470-2045(16)30648-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Hsieh JC-H, Wang H-M, Wu M-H, Chang K-P, Chang P-H, Liao C-T, et al. Review of emerging biomarkers in head and neck squamous cell carcinoma in the era of immunotherapy and targeted therapy. Head Neck. (2019) 41 (Suppl. 1):19–45. 10.1002/hed.25932 [DOI] [PubMed] [Google Scholar]
- 106.Lim SM, Cho SH, Hwang IG, Choi JW, Chang H, Ahn M-J, et al. Investigating the feasibility of targeted next-generation sequencing to guide the treatment of head and neck squamous cell carcinoma. Cancer Res Treat. (2019) 51:300–12. 10.4143/crt.2018.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Eder T, Hess AK, Konschak R, Stromberger C, Johrens K, Fleischer V, et al. Interference of tumour mutational burden with outcome of patients with head and neck cancer treated with definitive chemoradiation: a multicentre retrospective study of the German Cancer Consortium Radiation Oncology Group. Eur J Cancer. (2019) 116:67–76. 10.1016/j.ejca.2019.04.015 [DOI] [PubMed] [Google Scholar]
- 108.Hoogsteen IJ, Marres HAM, Bussink J, van der Kogel AJ, Kaanders JHAM. Tumor microenvironment in head and neck squamous cell carcinomas: predictive value and clinical relevance of hypoxic markers. A review. Head Neck. (2007) 29:591–604. 10.1002/hed.20543 [DOI] [PubMed] [Google Scholar]
- 109.Spiegelberg L, Houben R, Niemans R, de Ruysscher D, Yaromina A, Theys J, et al. Hypoxia-activated prodrugs and (lack of) clinical progress: The need for hypoxia-based biomarker patient selection in phase III clinical trials. Clin Transl Radiat Oncol. (2019) 15:62–9. 10.1016/j.ctro.2019.01.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Baumann M, Krause M. CD44: a cancer stem cell-related biomarker with predictive potential for radiotherapy. Clin Cancer Res. (2010) 16:5091–3. 10.1158/1078-0432.CCR-10-2244 [DOI] [PubMed] [Google Scholar]
- 111.Eltzschig HK, Carmeliet P. Hypoxia and Inflammation. N Engl J Med. (2011) 364:656–65. 10.1056/NEJMra0910283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.Zhang P, Sun Y, Ma L. ZEB1: at the crossroads of epithelial-mesenchymal transition, metastasis and therapy resistance. Cell Cycle. (2015) 14:481–7. 10.1080/15384101.2015.1006048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Schmalhofer O, Brabletz S, Brabletz T. E-cadherin, beta-catenin, and ZEB1 in malignant progression of cancer. Cancer Metastasis Rev. (2009) 28:151–66. 10.1007/s10555-008-9179-y [DOI] [PubMed] [Google Scholar]
- 114.Chen C, Zimmermann M, Tinhofer I, Kaufmann AM, Albers AE. Epithelial-to-mesenchymal transition and cancer stem(-like) cells in head and neck squamous cell carcinoma. Cancer Lett. (2013) 338:47–56. 10.1016/j.canlet.2012.06.013 [DOI] [PubMed] [Google Scholar]
- 115.Smith A, Teknos TN, Pan Q. Epithelial to mesenchymal transition in head and neck squamous cell carcinoma. Oral Oncol. (2013) 49:287–92. 10.1016/j.oraloncology.2012.10.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.De Meulenaere A, Vermassen T, Creytens D, Aspeslagh S, Deron P, Duprez F, et al. Importance of choice of materials and methods in PD-L1 and TIL assessment in oropharyngeal squamous cell carcinoma. Histopathology. (2018) 73:500–9. 10.1111/his.13650 [DOI] [PubMed] [Google Scholar]
- 117.Tran L, Allen CT, Xiao R, Moore E, Davis R, Park S-J, et al. Cisplatin alters antitumor immunity and synergizes with PD-1/PD-L1 inhibition in head and neck squamous cell carcinoma. Cancer Immunol Res. (2017) 5:1141–51. 10.1158/2326-6066.CIR-17-0235 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Kroon P, Frijlink E, Iglesias-Guimarais V, Volkov A, van Buuren MM, Schumacher TN, et al. Radiotherapy and cisplatin increase immunotherapy efficacy by enabling local and systemic intratumoral T-cell activity. Cancer Immunol Res. (2019) 7:670–82. 10.1158/2326-6066.CIR-18-0654 [DOI] [PubMed] [Google Scholar]
- 119.de Ruiter EJ, Ooft ML, Devriese LA, Willems SM. The prognostic role of tumor infiltrating T-lymphocytes in squamous cell carcinoma of the head and neck: a systematic review and meta-analysis. Oncoimmunology. (2017) 6:e1356148. 10.1080/2162402X.2017.1356148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Hendry S, Salgado R, Gevaert T, Russell PA, John T, Thapa B, et al. Assessing tumor-infiltrating lymphocytes in solid tumors: a practical review for pathologists and proposal for a standardized method from the international immuno-oncology biomarkers working group: part 2: TILs in melanoma, gastrointestinal tract carcinom. Adv Anat Pathol. (2017) 24:311–35. 10.1097/PAP.0000000000000161 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Spector ME, Bellile E, Amlani L, Zarins K, Smith J, Brenner JC, et al. Prognostic value of tumor-infiltrating lymphocytes in head and neck squamous cell carcinoma. JAMA Otolaryngol Head Neck Surg. (2019) 145:1012–19. 10.1001/jamaoto.2019.2427 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Balermpas P, Rodel F, Krause M, Linge A, Lohaus F, Baumann M, et al. The PD-1/PD-L1 axis and human papilloma virus in patients with head and neck cancer after adjuvant chemoradiotherapy: a multicentre study of the German Cancer Consortium Radiation Oncology Group (DKTK-ROG). Int J Cancer. (2017) 141:594–603. 10.1002/ijc.30770 [DOI] [PubMed] [Google Scholar]
- 123.Ward MJ, Thirdborough SM, Mellows T, Riley C, Harris S, Suchak K, et al. Tumour-infiltrating lymphocytes predict for outcome in HPV-positive oropharyngeal cancer. Br J Cancer. (2014) 110:489–500. 10.1038/bjc.2013.639 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Oguejiofor K, Hall J, Slater C, Betts G, Hall G, Slevin N, et al. Stromal infiltration of CD8 T cells is associated with improved clinical outcome in HPV-positive oropharyngeal squamous carcinoma. Br J Cancer. (2015) 113:886–93. 10.1038/bjc.2015.277 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 125.Hess A-K, Johrens K, Zakarneh A, Balermpas P, Von Der Grun J, Rodel C, et al. Characterization of the tumor immune micromilieu and its interference with outcome after concurrent chemoradiation in patients with oropharyngeal carcinomas. Oncoimmunology. (2019) 8:1614858. 10.1080/2162402X.2019.1614858 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Ghanizada M, Jakobsen KK, Grønhøj C, von Buchwald C. The effects of checkpoint inhibition on head and neck squamous cell carcinoma: a systematic review. Oral Oncol. (2019) 90:67–73. 10.1016/j.oraloncology.2019.01.018 [DOI] [PubMed] [Google Scholar]
- 127.Seiwert TY, Burtness B, Mehra R, Weiss J, Berger R, Eder JP, et al. Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): an open-label, multicentre, phase 1b trial. Lancet Oncol. (2016) 17:956–65. 10.1016/S1470-2045(16)30066-3 [DOI] [PubMed] [Google Scholar]
- 128.Alfieri S, Cavalieri S, Licitra L. Immunotherapy for recurrent/metastatic head and neck cancer. Curr Opin Otolaryngol Head Neck Surg. (2018) 26:152–6. 10.1097/MOO.0000000000000448 [DOI] [PubMed] [Google Scholar]
- 129.Cohen EEW, Soulieres D, Le Tourneau C, Dinis J, Licitra L, Ahn M-J, et al. Pembrolizumab versus methotrexate, docetaxel, or cetuximab for recurrent or metastatic head-and-neck squamous cell carcinoma (KEYNOTE-040): a randomised, open-label, phase 3 study. Lancet. (2019) 393:156–67. 10.1016/S0140-6736(18)31999-8 [DOI] [PubMed] [Google Scholar]
- 130.Lee YS, Johnson DE, Grandis JR. An update: emerging drugs to treat squamous cell carcinomas of the head and neck. Expert Opin Emerg Drugs. (2018) 23:283–99. 10.1080/14728214.2018.1543400 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131.Sato K, Ono T, Sato F, Kawahara A, Azuma K, Kawaguchi T, et al. Different responses to nivolumab therapy between primary and metastatic tumors in a patient with recurrent hypopharyngeal squamous cell carcinoma. Oral Oncol. (2019). [Epub ahead of print]. 10.1016/j.oraloncology.2019.07.009 [DOI] [PubMed] [Google Scholar]
- 132.Ferris RL, Blumenschein GJ, Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med. (2016) 375:1856–67. 10.1056/NEJMoa1602252 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133.Zandberg DP, Algazi AP, Jimeno A, Good JS, Fayette J, Bouganim N, et al. Durvalumab for recurrent or metastatic head and neck squamous cell carcinoma: results from a single-arm, phase II study in patients with >/= 25% tumour cell PD-L1 expression who have progressed on platinum-based chemotherapy. Eur J Cancer. (2019) 107:142–52. 10.1016/j.ejca.2018.11.015 [DOI] [PubMed] [Google Scholar]
- 134.Chow LQM, Haddad R, Gupta S, Mahipal A, Mehra R, Tahara M, et al. Antitumor activity of pembrolizumab in biomarker-unselected patients with recurrent and/or metastatic head and neck squamous cell carcinoma: results from the phase Ib KEYNOTE-012 expansion cohort. J Clin Oncol. (2016) 34:3838–45. 10.1200/JCO.2016.68.1478 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Bedognetti D, Hendrickx W, Ceccarelli M, Miller LD, Seliger B. Disentangling the relationship between tumor genetic programs and immune responsiveness. Curr Opin Immunol. (2016) 39:150–8. 10.1016/j.coi.2016.02.001 [DOI] [PubMed] [Google Scholar]
- 136.Ferris RL. Immunology and immunotherapy of head and neck cancer. J Clin Oncol. (2015) 33:3293–304. 10.1200/JCO.2015.61.1509 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data in this study is available the European Genome-phenome Archive (https://www.ebi.ac.uk/ega/) with the accession numbers: EGAD00001005721, EGAD00001005715, EGAD00001005716, EGAD00001005717, and study number EGAS00001004090.