

Abstract
Objectives:
To estimate the prevalence of chronic pain (CP) and high-impact chronic pain (HICP) in a sample of the general adult population in Saudi Arabia.
Methods:
This is a cross-sectional online survey (N=24,265). Forty data collectors from 5 regions of Saudi Arabia approached people to complete the questionnaires through different social media applications, using a validated survey in Arabic language.
Results:
Chronic pain and HICP prevalences in the Saudi adult population were found to be 46.4% (CP) and 4% (HICP), with a higher prevalence among women and elderly. Chronic back pain was the most reported pain location. Half of the respondents reported dissatisfaction with pain services. Greater prevalence of HICP was found among women, elderly, unemployed, and those with low-income status. Patients with HICP were more likely to have more healthcare utilization and have more negative impacts on their physical and psychological wellbeing.
Conclusion:
Chronic pain and HICP are common in Saudi Arabia, especially among females and elderly, suggesting a public health problem. This calls for collaborative efforts at various levels of the social hierarchy to ensure the provision of effective management of CP in Saudi Arabia.
Pain is an extremely common health-related condition.1 It is defined by the International Association for the Study of Pain (IASP) as an “unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage”.2 If pain lasts for 3 months or more, whether persistent or recurrent, it is considered chronic pain (CP). Chronic pain is a major global health issue with a prevalence of 20%-50% worldwide.3-6 This wide range is probably explained by the subjective definition of pain, the lack of appropriate instruments to assess pain, and data collection variability among studies.6 Chronic pain exerts a heavy toll on an individual’s life (example, the association with depression and anxiety), community (example, the opioids epidemic), and the healthcare system.4 It is one of the most costly health conditions, with a total estimated economic cost of $560-$635 billion per annum for medical care and disability programs in the United States (US).7
The traditional definition of CP focuses on the pain duration without considering its multidimensional consequences (physical and psychological negative sequelae).8 Many patients with CP find that the pain negatively impacts their daily life activities, and these impacts vary from one individual to another, and therefore, the utilization of healthcare services may differ accordingly.9 In 2015, the US National Pain Strategy (USNPS) proposed a new concept under the name of “High-Impact Chronic Pain” (HICP), which helps to identify CP patients who live with activity limitations and restricted participation (example, in work and self-care activities).7,10,11
To date, published epidemiological studies regarding CP prevalence in Saudi Arabia are either limited to certain cities (for instance, Al-Kharj),12 or certain CP subset disorders (example, low back pain).13 The aim of this study is to estimate the prevalence of CP and HICP in Saudi Arabia.
Methods
A literature review of previous publications was conducted using Google Scholar and PubMed search engines, as well as through citation chasing. An Arabic questionnaire was developed that examined the 3 following topics: 1) demographic information (gender, age, nationality, region, marital status, average income, education level, nature of work, smoking, and exercise); 2) pain aspects (location, onset, course, duration, intensity, frequency, timing, activity of daily living, most aggravating factors, and relieving factors); 3) pain management and consequences (presence of diagnosis, most frequent pain medication used, response to medications, number of doctor visits [over the last year], number of emergency department visits [over the last year], number of hospitalizations [over the last year], number of radiological tests [over the last year], number of interventional pain procedures or surgical interventions, number of visits to traditional practitioners, seeking health services outside the country, mental-health and work-performance impact, and patient satisfaction with pain services).
The questionnaire’s reliability and validity was tested afterwards. First, face validity was examined by 3 pain physicians and one reviewer, and an agreement of good face validity was established. Secondly, a pilot test was conducted on a subset comprising 249 individuals, of which, the complete response of 50 individuals was used for testing the reliability and validity of the questionnaire. Regarding reliability, the internal consistency of the questionnaire was examined using Cronbach’s alpha, and test-retest reliability was assessed by a second administration after at least 3 days of the first administration, after which, the stability of the responses between the 2 administrations were estimated using Pearson’s correlation coefficients (r). Results demonstrated adequate internal consistency and good test-retest reliability. Regarding validity, construct validity of the “pain intensity” part of the questionnaire was examined via the association with the numerical pain rating scale (NPRS). Concurrent validity of the questionnaire, testing the extent to which the “pain aspects” part is correlated with a validated measure of pain, the Arabic Brief Pain Inventory (BPI), was also assessed. Pearson’s correlation coefficient (r) was used for the evaluation of the associations; where r <0.3 was considered weak, moderate if r ≥0.3 but <0.5, and strong if r ≥0.5. Results showed a strong association with the NPRS, and moderate to strong association with the Arabic BPI.
This cross-sectional online survey in the Arabic language was sent to people via different types of social media (WhatsApp, Snapchat, and Twitter), to evaluate CP and HICP characteristics and prevalence in Saudi Arabia. Data was gathered between August and September 2018. Researchers have divided the country into 5 main regions: northern, southern, eastern, western, and central regions, and 40 data collectors, 8 for each region, approached people online to complete the questionnaires. This study was approved by the Institution Review Board, Al-Taif University, Taif, Saudi Arabia.
In this study, CP was defined as continuous or intermittent pain that affects daily life activities, having lasted 3 months or more. High-impact chronic pain describes CP patients who have difficulties executing daily life activities. The criteria of HICP in this study included all the following: 1) pain frequency must be daily or once or more in a week but not daily (excluding once or more in a month but not weekly); 2) pain intensity must be severe (7-10/10) using a 0-10 numerical pain score (excluding mild (1-3/10) and moderate (4-6/10) pain);14 3) the individual must need help, anything from the least to the highest amount of help, to perform their daily life activities, or the individual must be completely dependent on others (excluding those who do not need help to perform their daily life activities). The study excluded all incomplete responses, non-Saudis, and participants under 18 years of age.
The sample size was calculated from a cross-sectional study conducted in Al Kharj, Saudi Arabia. Raosoft software (Seattle, Inc. 2004) was used to calculate the number of people required to be surveyed to detect a 19% prevalence of pain, with a 1% margin of error and 99% confidence interval (CI). The total number of 10,202 respondents were required to complete this study. A total of 32,631 respondents were achieved to correct for non-Saudis, participants under 18 years and incomplete responses within the allotted data-gathering period of one month.
Statistical analysis
We used JMP®, Version 13 (Statistical Analysis System Institute Inc, Cary, NC, 1989-2019) fro data analysis. Data were tested for representativeness, where one-sample Chi-square goodness of fit was used to compare between the population proportions and sample proportions of each of the strata. There was no significant difference between age of the sample and age in the Saudi population (p=0.95). However, the gender and education showed significant difference. To correct for the sampling proportions in each of the strata defined by gender, age, and education, data were weighted based on the 2018 Saudi census.15 Then descriptive analysis of demographics and characteristics of CP was developed for the respondents in the sample. Next, a best-fitting binary logistic regression model was developed to adjust for the HICP confounders including demographic factors with p-value less than 0.05. A CI at level of 99% was calculated for demographic probabilities.
Results
Of the 32,631 participants in the cross-sectional online survey, 26,372 met the study’s criteria, with the majority of the participants being female (63.3%) (Table 1). After the statistical adjustment of all the demographic factors (gender-weighting) except education (adjusted independently) based on the Saudi census,15 a total of 24,265 respondents depicted our sample size. Seventy percent of the respondents were younger than 40 years of age, and the majority were from the eastern or western regions of Saudi Arabia and married. Before the statistical adjustment, most participants had a university degree (71.7%), and half were unemployed (51%). However, participants with “high school or less” education became the majority (54%), while the unemployed remained (45%) after the statistical adjustment. Three-quarters of participants (76.8%) were non-smokers, and a similar fraction had a sedentary lifestyle or performed walking at most (75.7%). A summary of the demographic factors of the sample and the weighted sample is shown in Table 1.
Table 1.
Demographic factors of the sample, weighted sample, and prevalences of chronic pain and high impact chronic pain.
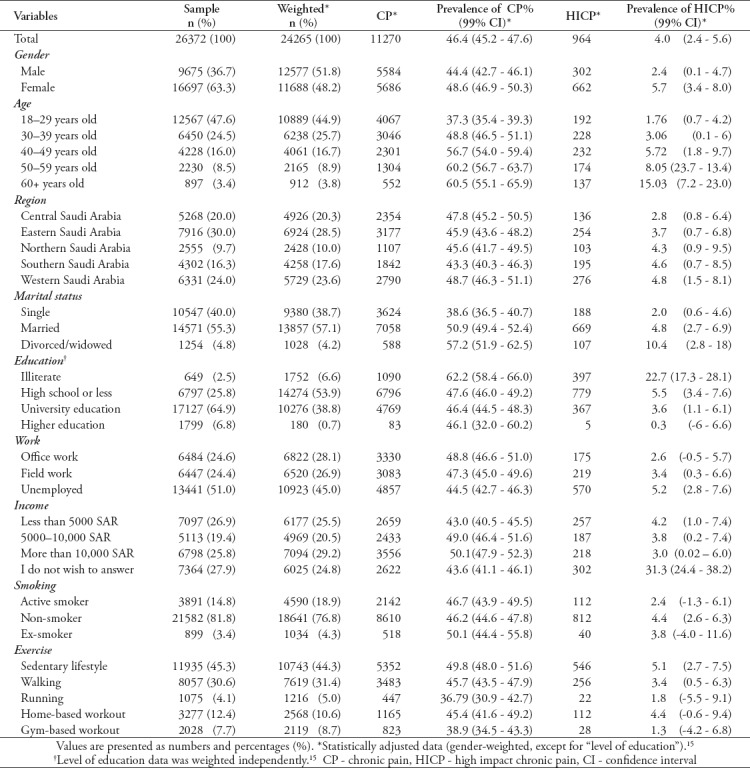
A total of 11,270 participants (46.4%) met the criteria for CP, with the majority being female, younger than 40 years of age, married, having “high school or less” education, unemployed, non-smoker, and from the eastern region of Saudi Arabia. Close to half of the participants with CP reported a sedentary lifestyle (47.4%), and walking was the most reported form of physical activity (30.9%). The prevalence of CP was higher among women (48.6%), divorced or widowed (57.2%), illiterate (62.2%), those with office work (48.8%), ex-smokers (50.1%), those with higher income (50.1%) and a sedentary lifestyle (49.8%), and increased as the population got older. When comparing the prevalence of CP among the 5 Saudi-Arabian regions, the western region had the highest prevalence (48.7%), despite the higher number of CP patients from the eastern region. A summary of the demographic factors of CP patients, and CP prevalence for each factor is depicted in Table 1.
The lower extremities, followed by the lower back and the head, were the most commonly reported pain locations (Figure 1). Over half of the participants (55.7%) reported moderate pain severity and pain that lasted for more than 2 years (50.9%) (Table 2). Close to one third of participants (30.6%) reported daily pain, and pain episodes were continuous or lasted for more than one hour in 53.5% of patients. Physical activities and psychological stressor (anger and anxiety) were the most frequently reported aggravating factors, while resting was the most reported relieving factor. A summary of pain characteristics of patients with CP is depicted in Table 2. Interestingly, 45.2% of participants with CP did not take any medication for their pain, and 71.6% required no help in performing their daily activities (Table 3). Paracetamol was the most commonly used medication, while opioids were the least used among our participants (Figure 2), with a remarkable 69.5% of them reporting pain relief with medications. The majority of the CP patients reported no emergency department pain-related visits (63.1%), required no hospitalization (85.5%) or invasive interventions (86.4%), and over one third (35.2%) had no medical providers for their pain. Half of the participants experiencing CP (49.2%) had no imaging studies to evaluate the pain, more than half (51.6%) reported a “bad” or “very bad” grading for the local pain services, while only 12.5% sought medical providers outside the country for their chronic pain. More than two thirds (69.5%) of CP patients reported that the pain negatively impacted their physical and psychological wellbeing. A summary of the healthcare characteristics of patients with CP, CP without limitations (CPWL), and HICP are shown in Table 3.
Figure 1.
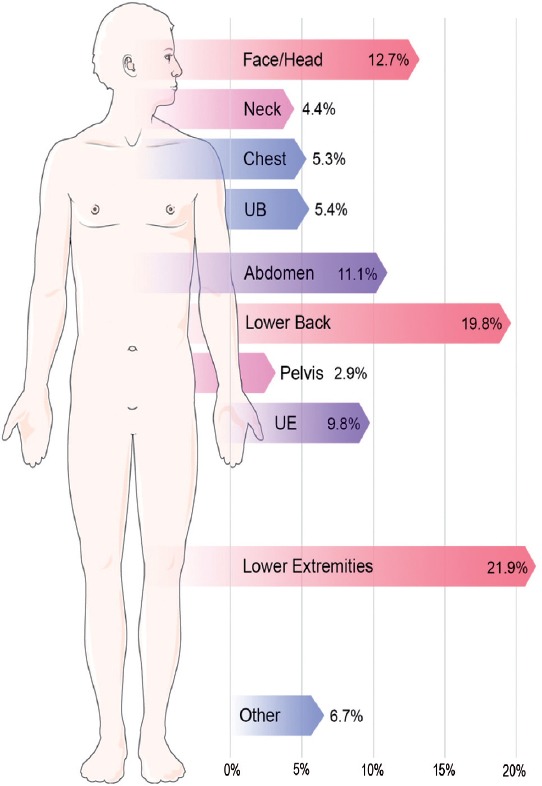
Chronic pain locations (humanoid figure obtained from smart.servier.com) UB - upper back, UE - upper extremities
Table 2.
Pain characteristics of patients with chronic pain (N=11270).
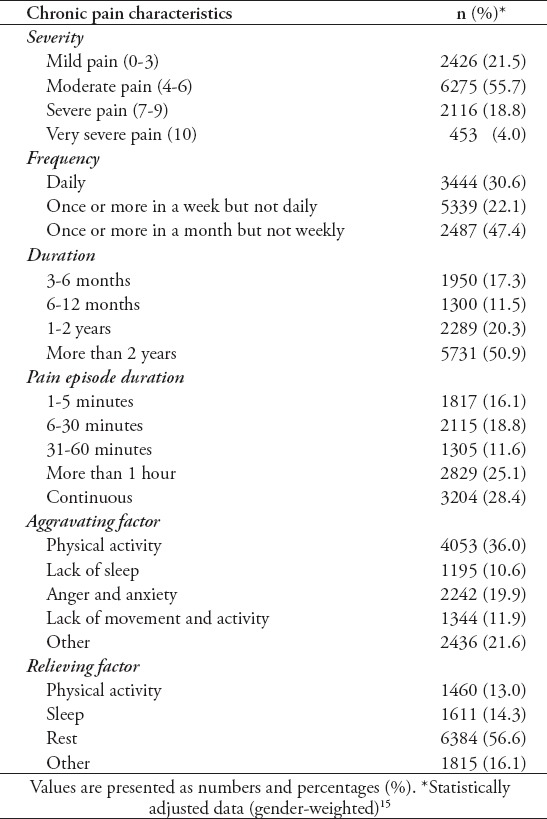
Table 3.
Health care characteristics of patients with chronic pain and high impact chronic pain.
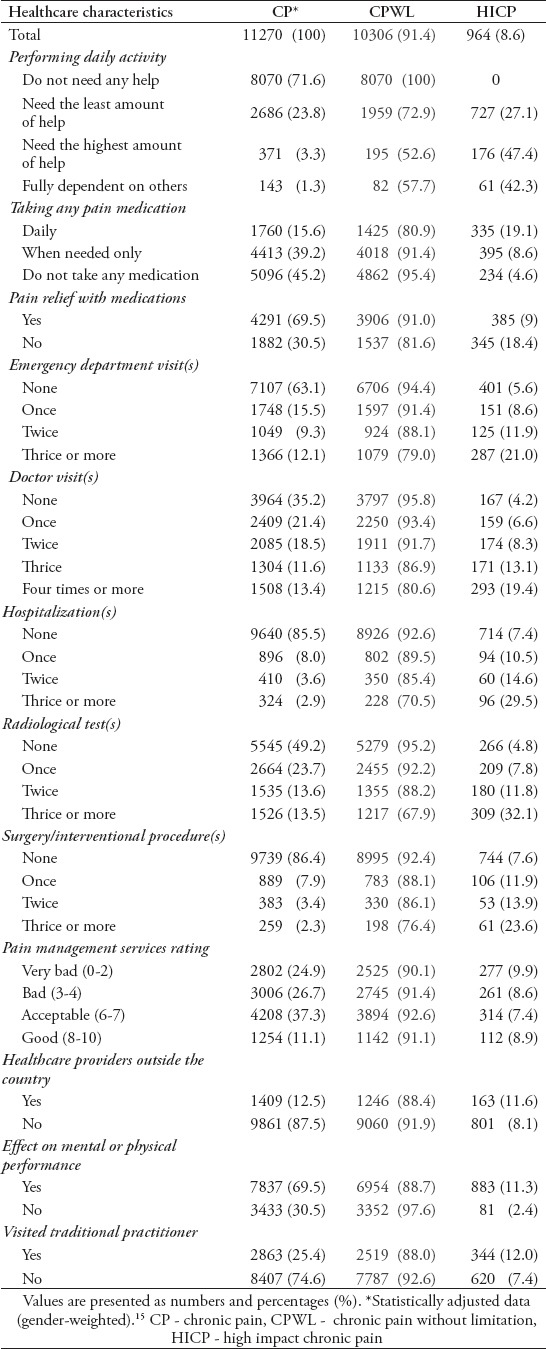
Figure 2.
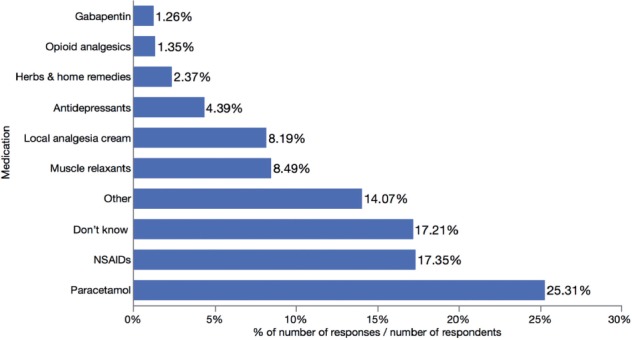
Percentage of chronic pain patients taking medication. Percentage responses were calculated using 6,172 as a denominator (number of chronic pain patients who received medications). NSAIDs - non steroidal anti-inflammatory drugs
A total of 964 (8.6%) participants with CP met the criteria for HICP, which gave a HICP prevalence of 4% among adults in Saudi Arabia (Table 1). The prevalence of HICP was higher among women (5.7%), divorced (10.4%), illiterate (22.7%), unemployed (5.2%), non-smokers (4.4%), those with lower income (4.2%) and a sedentary lifestyle (5.1%), and increased as the population got older (Tables 1 & 4). Similar to the prevalence of CP among the 5 Saudi-Arabian regions, the western region of Saudi Arabia had the highest prevalence of HICP (4.8%). Nominal logistic regression analysis for HICP patients revealed that age and gender had the most impact on HICP, while education, exercise, income and work had a slight impact (Figure 3). Marital status (p=0.213) and smoking (p=0.499) were not significant factors, since they did not add any effect to the model (Figure 3). A summary of the OR of HICP according to different demographic factors is provided in Table 4.
Table 4.
Odds ratio of high impact chronic pain according to different demographic factors.
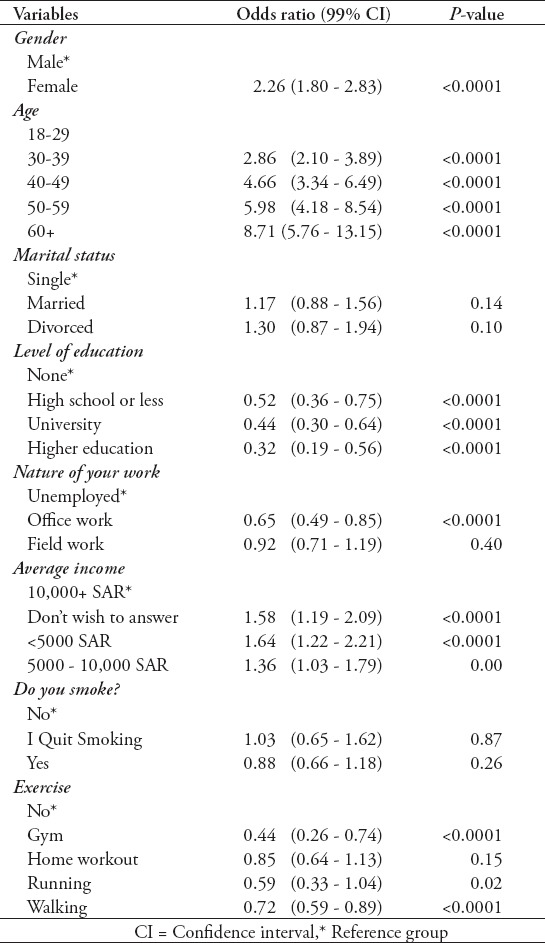
Figure 3.
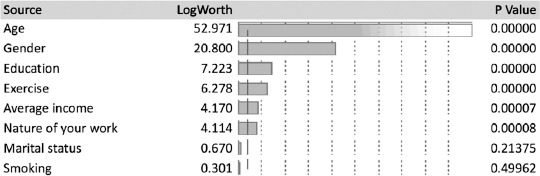
Nominal logistic fit for high impact chronic pain patients. Effect summary: how much each variable compacted the model. Age and gender the real effect on the model, while education, exercise, income, and work have the slight effect. Marital status and smoking are not significant factors, they do not add effect to the model.
Compared to CPWL, patients with HICP were more likely to take daily pain medications, and need the highest amount of help in performing their daily activities. They were also more likely to have more emergency department visits, follow-ups with medical providers, hospitalizations for pain-related complaints, imaging studies, and invasive interventions. In addition, HICP patients were more likely to have more negative impacts on their physical and psychological wellbeing, and be treated by international or traditional medical providers (Table 3).
Discussion
The aim of this study is to estimate the prevalence of CP in the Kingdom of Saudi Arabia adding on to previous prevalence studies that were either limited to certain cities (like Al-Kharj) within Saudi Arabia, or shedding light only on certain subsets of chronic pain (lower back pain).12,13 The prevalence of CP in the Saudi adult population was found to be 46.4%. This was higher than the worldwide weighted mean prevalence of CP (30.30% ± 11.7%) depicted in a systematic review involving 19 studies, 65 surveys, 34 countries, and 182,019 participants.5 It was also higher than that of the Middle East and North Africa (28% ± 9.2%),5 however, lower than the estimate in regional neighboring countries (like Kuwait), where a limited survey estimated CP prevalence of up to 56% among participants attending a large medical center.16 Similar results were seen when comparing the prevalence of CP in Saudi Arabia with that of several developing countries with a human development index (HDI) below 0.9. Saudi Arabia is viewed as a developing country with an HDI of 0.853 (2017).17 Its estimated prevalence was higher than that of India (19.3%, HDI = 0.640),18 and Mexico (24.1%, HDI = 0.774),4 whilst similar to that of South Africa (48.3%, HDI = 0.699).4 Compared to the developed countries, the Saudi estimated CP prevalence was higher than that of France (31.7%)19 and the US (18.4%),11 and similar to that of the United Kingdom (48%).20
Pain duration has traditionally been used to define CP.1,21,22 However, this approach does not consider the multidimensional aspects of CP, such as functional disability, which was accounted for by USNPS’s concept of HICP.8,10 Despite the substantial burden inflicted on an individual by pain lasting 3 months or more, exercising the concept of factoring in disability (activity limitations and participation restrictions) into the definition of CP is important to distinguish between HICP patients dealing with significant limitations in self-care, recreation, work, or social activities, and those with less impact forms of CP.8,10,23,24 This is vital in identifying populations in desperate need of pain services.
The prevalence of HICP among adults in Saudi Arabia was found to be 4% (8.6% of those with CP). This was lower than the 8% reported adults with HICP in the US.14 Interestingly, when separating pain experience from its impact, using general disability scores without referencing pain while assessing activity limitations and participation restrictions, the prevalence of HICP in US adults fell to 4.8%, representing the most impacted segment of the CP population, as demonstrated by a later US study.11
The results of our subgroup analyses were consistent with findings in a similar study showing a high prevalence of HICP among women, the elderly, the unemployed, and those with low educational level.14 A well-defined association is observable between socioeconomic factors (example, low educational levels and poverty) and the overall wellbeing of an individual, in part due to impacting the effective reach for needed healthcare services.25 High-impact chronic pain patients tended to report more negative effects on their physical and psychological wellbeing, more need of help when performing their daily activities, more healthcare usage and hospitalizations, and more reliance on daily or as-needed pain medications, compared to patients experiencing CP without limitations-findings that were inline with those of a similar study.11 This highlights the need to identify and prioritize populations at risk, for the appropriate development and steering of quality pain services.
Chronic pain occurs in various bodily locations and is linked with many different clinical diagnoses, including neurogenic, musculoskeletal, connective tissue, postsurgical, posttraumatic, and cancer. In this study, chronic back pain (25.2%) was the most reported location, followed by the lower limbs (21.9%) and the head (12.7%), which mirrored findings in similar studies.3,4,19 Lower back pain affected 19.6% of the respondents, which was lower than the previously estimated lower-back CP mean prevalence of 66.2% in Saudi Arabia.13
Saudi women exhibited a higher prevalence of CP than men, a universal trend demonstrated by several publications,3,4 evidencing a strong gender predisposition for CP. Specifically, the risk of having CP in Saudi women was higher than that of men with an OR of 1.19 (99% CI 1.11 to 1.27). This was lower than WHO’s worldwide OR (1.69),26 Libya (1.9),27 China (1.57),28 and France (1.41).19 Research supports the evidence of differences in pain perception between genders, with women tending to report greater pain frequency, intensity, and duration than men.29,30 Additionally, psychological differences in pain perception between genders have been noted; namely, greater pain-related catastrophic thinking among women,29,31 defined as the tendency to exaggerate the impact of pain,32 which might explain the heightened emotional distress and physical disability shared by women with CP.31 This could be attributed to features unique to women, such as hormonal (estrogen) or psychosocial (gender role) factors.29,33
A strong association exists between increasing age and the prevalence of CP, as evident in many epidemiological studies,3,4 including ours. Patients aged 50+ years appeared more likely to experience CP than the rest of the age groups, despite their smaller sample size. The higher prevalence of CP among the aging population could be partially attributed to differences in pain perception (decreased tolerance), attitude toward pain (the belief that pain is age normative), coping mechanisms (narrower range or less frequent use of coping strategies), and social context (less social support) between the elderly and the young.34
Besides the observed associations of increased CP prevalence in certain demographic factors such as women and elderly, unemployment was less likely in patients with CP in our study. This observation could be attributed to several reasons, including the higher sample size of patients in the age group of 18-29 years (lowest CP prevalence in the age subgroup), wherein individuals often seek higher education, and therefore are unemployed. In addition and given the strong gender predisposition for CP, the unemployment rate of Saudi women (18.7%) is significantly higher than that of men (2.9%);35 therefore, the prevalence of CP among the unemployed might be partially attributed to the higher prevalence of CP among female participants. Furthermore, the unemployment of affected patients could potentially be a manifestation of their experiences with CP. These could explain why unemployment is viewed as a weak risk factor for developing CP in the current study.
Over half (54.8%) of CP patients reported taking daily or as-needed pain medications in our study, with paracetamol (acetaminophen) being the most commonly used analgesic, followed by NSAIDs (anti-inflammatory medications), while opioids were the least commonly used. This finding differed from that of similar surveys conducted elsewhere, where NSAIDs (followed by weak opioids in one study)3 surpassed paracetamol (acetaminophen) as the most commonly used class of analgesic medication.36 As with the majority of the world, paracetamol and NSAIDs are commonly available over the counter in Saudi Arabia and do not require a medical prescription. Access to analgesic opioids, on the other hand, is very difficult in this country, obtained through an extensive process and requiring a specific medical prescription.
When comparing our results to other related studies conducted in developed countries with a high prevalence of CP (example US, Canada, and Europe), it is evident that analgesic opioids are under-prescribed for CP in Saudi Arabia.3,36,37 In fact, the average consumption of opioids in Saudi Arabia, conveyed in defined daily doses for statistical purposes (S-DDD) per one million inhabitants per day for a 3-year period (2015-2017), was just 308 S-DDD compared with 40,240 S-DDD in the US, 28,862 S-DDD in Germany, and 26,029 S-DDD in Canada.38 Unfortunately, many countries in the Middle East and the developing world share figures similar to those of Saudi Arabia when it comes to opioid prescriptions due to concerns and fears regarding tolerance, dependence, and abuse of opioids.27,39,40 A study conducted in a major tertiary care hospital in Saudi Arabia reported the prevalence of opioid misuse (12.8%), abuse (9.1%), and dependence (3.2%) among CP patients attending the pain clinic.41
While the risks associated with opioid use are clearly evident in the literature and opioid prescriptions must remain controlled, appropriate medical use of opioids should not be impeded, especially given their well-documented efficacy and established guidelines in CP treatment.42 The under-prescription of analgesic opioids in Saudi Arabia could be attributed to several factors including; severe restrictions and regulations on prescribing and supplying narcotics, under-procurement of narcotics due to strict laws and the complexity governing international purchases, clinicians’ concerns regarding complications and legislations surrounding opioid use, and the public’s cultural misbeliefs and fear of addiction.43,44 These issues call for much-needed efforts in public information and awareness, physician education and training, and policy making regarding opioid use, to encourage the effective and safe management of CP.
A minority of patients with CP resorted to non-pharmacological approaches, where 2.4% of respondents reported taking herbal supplements and other home remedies. Furthermore, a quarter (25.4%) reported visiting traditional practitioners, commonly utilizing practices such as religious healings (Quran reciting), herbal medicine, cupping (Hijama), and cauterization (Kai) for pain relief.45,46 Despite the limited evidence on the efficacy of some complementary and alternative medicines (CAM) in the treatment of CP,47 it remains consistently intertwined with the healthcare of CP patients in the world and in Saudi Arabia.47-49 This is apparent given the burden of an expanding population coupled with the demand of free services on the Saudi healthcare system,50 translating into long waiting times to receive appropriate healthcare. Higher treatment costs, the perceived success of CAM in the management of pain conditions,45 and patient dissatisfaction with pain services-where over half (51.6%) of CP patients in the current study rated local pain services as “bad” or “very bad”-are also an issue. Consequently, efforts to educate the affected population on the presence of such CAM modalities should not preclude seeking conventional medical treatment, instead be viewed as a collaborative approach to pain management, must be commenced. Additionally, the availability of pain centers and pain physicians who are well updated and qualified in the management of CP is important, and aligns with the objectives of the IASP and the Saudi Society of Pain Medicines.51,52
Based on the literature, there an insufficient amount of reliable epidemiological statistics on the prevalence of CP in the developing world, especially countries in the Gulf Cooperation Council.6 The majority of prevalence studies have been conducted and funded by developed countries that tend to embrace data from countries with similar affluence.6 This highlights the issue that epidemiologic data on pain is often neglected and not considered a public health priority in the developing countries, despite its huge socioeconomic burden. This in turn calls for collaborative efforts at government, healthcare, and public levels to ponder pain when developing national laws, regulations, and economic plans. Future studies are needed to adjust for factors such as comorbidities, smoking, and body mass index, and to establish causality for associated factors in order to develop an effective approach to prevention, management and improving quality of life of CP patients.
Study limitations
The strengths of this study are the large sample size, the national coverage of Saudi regions, and the use of a uniform Arabic questionnaire. The study has a few limitation including some forms of selection bias such as non-probability sampling, and non-coverage. While probability sampling is often considered the most appropriate method for generating estimates that could be generalized to a fixed population and generally subject to lower biases, non-probability sampling may be a better choice in certain situations. Brick53 explained these situations in 3 conditions including lower cost, unnecessary extremely accurate estimates for requirement satisfaction, and a stable well-understood target population even when higher accuracy is needed. Attempts to compensate for the bias in our study, such as statistical weighting, has been made. Non-coverage discloses the access bias towards respondents in our study who use social media applications (WhatsApp, Snapchat, and Twitter) driven by the internet. Although internet usage has soared in recent years in Saudi Arabia, reaching 91% of the population in 2018, only 3 quarters (75%) have active social media accounts, with WhatsApp (73%) being the most commonly used application, followed by Twitter (52%) and Snapchat (39%), many are still not connected to any social media platform.54 This could also explain why the elderly population is underrepresented in this study, where only 3.4% of respondents were aged 60 years or older, compared to the estimated 6.5% elderly (60+ years of age) of the general Saudi population.15 This was the case despite our efforts in encouraging the respondents to help their elder family members and friends who did not have access to or could not fill in the survey on their own. Other limitations include the nature of self-reported data, which is subject to recall bias, and the lack of assessment of some confounding variables, such as clinical diagnoses and psychiatric comorbidity.
In conclusion, CP and HICP are very common in Saudi Arabia, with prevalence estimates of 46.4% (CP) and 4% (HICP) in the Saudi adult population, suggesting a high public-health burden. The most common location of CP was the back, while the major associated risk factors included gender (female) and age (elderly). High-impact chronic pain patients were the most affected subgroup of CP patients with the highest impact on physical and psychological wellbeing, amount of help in performing their activities, healthcare usage and hospitalizations, and reliance on pain medications, compared to patients having CP without limitations.
There is need for multifaceted efforts at government, healthcare, and public levels to consider pain when developing national laws, regulations, and economic plans. In addition, the wide availability of qualified pain centers and pain physicians for efficient CP prevention and management is important, and aligns with IASP objectives.
Acknowledgment
We gratefully acknowledge Roba M. Aldossary, Sara I. Alshahwan, Zahra M. Alyousef, Arwa A. Althubaity, Rand F. Alsaif, Alhassan M. AlSalem, Intesar H. Alshammari, Hadi A. Alshehri, Faisal A. Alsamiri, Ghadah A. Albalawi, Jawaher H. AL-Lugbi, Bayan A. Alatawi, Bashaer A. Alazhari, Musab S. Alabeesy, Rawan M. Alharthi, Ranin M. Masarit, Zainab A. Atufayyif, Aishah Z. Alanazi, Maha Y. Alahmari, Maryam A. Alhussain, Halah M. Alrasheedi, Anwar S. Alkhalifah, Faisal K. Almugrin, Hanan I. Alhassani, Yahya H. Dighriri, Rawabi T. Aljayani, Abdulkarim F. Aldhubayi, Rawabi W. Alghbban, Moudhi M. Aladwani, Reema S. ALQahtani, Mohamed A. Majrashi, Abdulkhaleq O. Almotiri G. Almutiri, Khloud A. Alshehri, Abdulkhaliq O. Almotiri, Renda A. Alhabib, Mohanned M. Alraddadi, Abdullah Z. Malaka, Shomokh F. Alharbi, Ebtihal M. Albeshri and Jehad A. Alzahrani for their help with the data collection. The authors would also like to thank Scribendi (www.scribendi.com) for English language editing.
Footnotes
References
- 1.Goldberg DS, McGee SJ. Pain as a global public health priority. BMC Public Health. 2011;11:770. doi: 10.1186/1471-2458-11-770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Turk DC, Rudy TE. IASP taxonomy of chronic pain syndromes:preliminary assessment of reliability. Pain. 1987;30:177–189. doi: 10.1016/0304-3959(87)91073-6. [DOI] [PubMed] [Google Scholar]
- 3.Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe:Prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10:287–333. doi: 10.1016/j.ejpain.2005.06.009. [DOI] [PubMed] [Google Scholar]
- 4.Tsang A, Von Korff M, Lee S, Alonso J, Karam E, Angermeyer MC, et al. Common chronic pain conditions in developed and developing countries:gender and age differences and comorbidity with depression-anxiety disorders. J Pain. 2009;10:553. doi: 10.1016/j.jpain.2008.05.005. [DOI] [PubMed] [Google Scholar]
- 5.Elzahaf RA, Tashani OA, Unsworth BA, Johnson MI. The prevalence of chronic pain with an analysis of countries with a Human Development Index less than 0.9:a systematic review without meta-analysis. Curr Med Res Opin. 2012;7:1221–1229. doi: 10.1185/03007995.2012.703132. [DOI] [PubMed] [Google Scholar]
- 6.Johnson MI, Elzahaf RA, Tashani OA. The prevalence of chronic pain in developing countries. Pain Manag. 2013;3:83–86. doi: 10.2217/pmt.12.83. [DOI] [PubMed] [Google Scholar]
- 7.Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13:715–724. doi: 10.1016/j.jpain.2012.03.009. [DOI] [PubMed] [Google Scholar]
- 8.Von Korff M, Scher AI, Helmick C, Carter-Pokras O, Dodick DW, Goulet J, et al. United states national pain strategy for population research:concepts, definitions, and pilot data. J Pain. 2016;17:1068–1080. doi: 10.1016/j.jpain.2016.06.009. [DOI] [PubMed] [Google Scholar]
- 9.IOM (Institute of Medicine) Relieving pain in America:a blueprint for transforming prevention, care, education, and research. Washindton (DC): National Academics Press; 2011. [PubMed] [Google Scholar]
- 10.Interagency Pain Research Coordinating Committee. National pain strategy:A comprehensive population healthlevel strategy for pain. 2015. Cited 2019 April 25. Available from: https://www.iprcc.nih.gov/National-Pain-Strategy/Objectives-Updates .
- 11.Pitcher MH, Von Korff M, Bushnell MC, Porter L. Prevalence and profile of high-impact chronic pain in the United States. J Pain. 2019;20:146–160. doi: 10.1016/j.jpain.2018.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.El-Metwally A, Shaikh Q, Aldiab A, Al-Zahrani J, Al-Ghamdi S, Alrasheed AA, et al. The prevalence of chronic pain and its associated factors among Saudi Al-Kharj population;a cross sectional study. BMC Musculoskelet Disord. 2019;20:177. doi: 10.1186/s12891-019-2555-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Awaji M. Epidemiology of low back pain in Saudi Arabia. J Adv Med Pharm Sci. 2016;6:1–9. [Google Scholar]
- 14.Dahlhamer J, Lucas J, Zelaya C, Nahin R, Mackey S, DeBar L, et al. Prevalence of chronic pain and high-impact chronic pain among adults-United States, 2016. Morb Mortal Wkly Rep. 2018;67:1001–1006. doi: 10.15585/mmwr.mm6736a2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.General Authority for Statistics. Population by Gender, Age Groups and Nationality (Saudi/Non-Saudi), 2018. Udpated 2019. Cited 2019 April 25. Available from: https://www.stats.gov.sa/en/43 .
- 16.Zghoul N, Ross EL, Edwards RR, Ahmed A, Jamison RN. Prevalence of chronic pain with neuropathic characteristics:A randomized telephone survey among medical center patients in Kuwait. J Pain Res. 2017;10:679–87. doi: 10.2147/JPR.S123966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Human Development Indices and Indicators:2018 Statistical Update. Updated 2018. Cited 2019 May 1. Available from: http://hdr.undp.org/sites/all/themes/hdr_theme/country-notes/SAU.pdf .
- 18.Saxena AK, Jain PN, Bhatnagar S. The prevalence of chronic pain among adults in India. Indian J Palliat Care. 2018;24:472. doi: 10.4103/IJPC.IJPC_141_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bouhassira D, Lantéri-Minet M, Attal N, Laurent B, Touboul C. Prevalence of chronic pain with neuropathic characteristics in the general population. Pain. 2008;136:380–387. doi: 10.1016/j.pain.2007.08.013. [DOI] [PubMed] [Google Scholar]
- 20.Torrance N, Smith BH, Bennett MI, Lee AJ. The epidemiology of chronic pain of predominantly neuropathic origin. Results from a general population survey. J Pain. 2006;7:281–289. doi: 10.1016/j.jpain.2005.11.008. [DOI] [PubMed] [Google Scholar]
- 21.Landis S. Chronic pain:Symptoms, diagnosis, and treatment. NIH Medlin Plus. Cited 2019 May 1. Available from: https://magazine.medlineplus.gov/pdf/MLP_Spring_2011.pdf .
- 22.Merskey H, Bogduk N. Classification of chronic pain;description of chronic pain syndromes and definition of pain terms. Seattle (WA): International Association for the Study of Pain (IASP) Press; 1994. [Google Scholar]
- 23.Von Korff M. Assessment of chronic pain in epidemiological and health services research. In: Turk D, Melzack R, editors. Handbook pain assessment. 3rd ed. New York: Guilford Publ Inc; 2011. pp. 455–473. [Google Scholar]
- 24.Von Korff M, Jensen MP, Karoly P. Assessing global pain severity by self-report in clinical and health services research. Spine (Phila Pa 1976) 2000;25:3140–3151. doi: 10.1097/00007632-200012150-00009. [DOI] [PubMed] [Google Scholar]
- 25.Ver Ploeg M, Perrin E. Washington, DC: National Academies Press; 2004. Eliminating health disparities. [PubMed] [Google Scholar]
- 26.Gureje O, Von Korff M, Simon GE, Gater R. Persistent pain and well-being:a World Health Organization Study in Primary Care. JAMA. 1998;280:147–151. doi: 10.1001/jama.280.2.147. Erratum: in JAMA 1998;280:1142. [DOI] [PubMed] [Google Scholar]
- 27.Elzahaf RA, Johnson MI, Tashani OA. The epidemiology of chronic pain in Libya :a cross-sectional telephone survey. BMC Public Health. 2016;776:1–14. doi: 10.1186/s12889-016-3349-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Chen B, Li L, Donovan C, Gao Y, Ali G, Jiang Y, et al. Prevalence and characteristics of chronic body pain in China:a national study. Springerplus. 2016;5:938. doi: 10.1186/s40064-016-2581-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Marcus D. Chronic Pain:A primary care guide to practical management. Totowa (NJ): Humana Press; 2009. [Google Scholar]
- 30.de Moraes Vieira ÉB, Garcia JBS, Silva AAM da, Araújo RLTM, Jansen RCS, Bertrand ALX. Chronic pain, associated factors, and impact on daily life:are there differences between the sexes? Cad Saude Publica. 2012;28:1459–1467. doi: 10.1590/s0102-311x2012000800005. [DOI] [PubMed] [Google Scholar]
- 31.Keefe FJ, Lefebvre JC, Egert JR, Affleck G, Sullivan MJ, Caldwell DS. The relationship of gender to pain, pain behavior, and disability in osteoarthritis patients:The role of catastrophizing. Pain. 2000;87:325–334. doi: 10.1016/S0304-3959(00)00296-7. [DOI] [PubMed] [Google Scholar]
- 32.Quartana PJ, Campbell CM, Edwards RR. Pain catastrophizing:a critical review. Expert Rev Neurother. 2009;9:745–758. doi: 10.1586/ERN.09.34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Smitherman TA, Ward TN. Psychosocial factors of relevance to sex and gender studies in headache. Headache. 2011;51:923–931. doi: 10.1111/j.1526-4610.2011.01919.x. [DOI] [PubMed] [Google Scholar]
- 34.Molton IR, Terrill AL. Overview of persistent pain in older adults. Am Psychol. 2014;69:197–207. doi: 10.1037/a0035794. [DOI] [PubMed] [Google Scholar]
- 35.General Authority for Statistics, Labor Market 2018, Third Quarter. Updated 2018. Cited 2019 May 01. Available from: https://www.stats.gov.sa/sites/default/files/labour_market_3q_2018_0.pdf .
- 36.Moulin DE, Clark AJ, Speechley M, Morley-Forster PK. Chronic pain in Canada - prevalence, treatment, impact and the role of opioid analgesia. Pain Res Manag. 2002;7:179–184. doi: 10.1155/2002/323085. [DOI] [PubMed] [Google Scholar]
- 37.Hudson TJ, Edlund MJ, Steffick DE, Tripathi SP, Sullivan MD. Epidemiology of regular prescribed opioid use:results from a national, population-based survey. J Pain Symptom Manage. 2008;36:280–288. doi: 10.1016/j.jpainsymman.2007.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.International Narcotics Control Board. Estimated world requirements for 2019 - Statistics for 2017. Updated 2019. Cited 2019 May 021. Available from: https://www.incb.org/documents/Narcotic-Drugs/Technical-Publications/2018/INCB-Narcotics_Drugs_Technical_Publication_2018.pdf .
- 39.Soyannwo OA. Obstacles to pain management in low-resource settings. In: Kopf A, Patel N, editors. Guide to pain management in low-resource settings. Washington (DC): International Association for the Study of Pain; 2010. pp. 9–11. [Google Scholar]
- 40.Cleary J, Silbermann M, Scholten W, Radbruch L, Torode J, Cherny NI. Formulary availability and regulatory barriers to accessibility of opioids for cancer pain in the Middle East:a report from the Global Opioid Policy Initiative (GOPI) Ann Oncol. 2013;24:xi51–xi59. doi: 10.1093/annonc/mdt503. [DOI] [PubMed] [Google Scholar]
- 41.Al Maharbi S, Abolkhair A, Al Ghamdi H, Haddara M, Valtysson B, Tolba Y, et al. Prevalence of opioid misuse, abuse and dependence among chronic pain patients on opioids followed in chronic pain clinic in a tertiary care hospital Riyadh, Saudi Arabia. Hamdan Med J. 2019:12–15. [Google Scholar]
- 42.World Health Organization. Cancer pain relief:With a guide to opioid availability. World Health Organization technical report series. Geneva (CH): 1996. Cited 2019 May 05. Available from; https://apps.who.int/iris/bitstream/handle/10665/37896/9241544821.pdf;jsessionid=9DE9FD41D877BB13170E05F05D34∧?sequence=1 . [Google Scholar]
- 43.Nuessle S, Gray A, Lambert G, Boyar A, Ba-Hatheq A, Adloni S, et al. Pain control with morphine:Evaluation of prescriptions for oral morphine for outpatients at King Faisal Specialist Hospital and Research Centre. Ann Saudi Med. 1996;16:371–376. doi: 10.5144/0256-4947.1996.371. [DOI] [PubMed] [Google Scholar]
- 44.Alqarni A, Alghsoon S, Alawlah A, Alhinti N, Aljulaihm A, Alolah YH. Trends of opioid consumption for cancer patients during the last week of their life in a tertiary care center. Int J Acad Sci Res. 2017;5:165–170. [Google Scholar]
- 45.Al-Faris EA, Al-Rowais N, Mohamed AG, Al-Rukban MO, Al-Kurdi A, Balla Al-Noor MA, et al. Prevalence and pattern of alternative medicine use:The results of a household survey. Ann Saudi Med. 2008;28:4–10. doi: 10.5144/0256-4947.2008.4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.AlBedah AM, Khalil MK, Elolemy AT, Al Mudaiheem AA, Al Eidi S, Al-Yahia OA, et al. The use of and out-of-pocket spending on complementary and alternative medicine in Qassim province, Saudi Arabia. Ann Saudi Med. 2013;33:282–289. doi: 10.5144/0256-4947.2013.282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Bauer BA, Tilburt JC, Sood A, Li GX, Wang SH. Complementary and alternative medicine therapies for chronic pain. Chin J Integr Med. 2016;22:403–411. doi: 10.1007/s11655-016-2258-y. [DOI] [PubMed] [Google Scholar]
- 48.Aldahash FD, Marwa AMK, Alkhamees MA, Alsulaiman HM, Aledan AK, Alkahtani SM, et al. Attitude towards the use of complementary and alternative medicine by patients in Saudi Arabia. Biomedica. 2012;28:1–6. [Google Scholar]
- 49.Khalil MKM, Al-Eidi S, Al-Qaed M, AlSanad S. The future of integrative health and medicine in Saudi Arabia. Integr Med Res. 2018;7:316–321. doi: 10.1016/j.imr.2018.06.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Almalki M, Fitzgerald G, Clark M. Health care system in Saudi Arabia:an overview. East Mediterr Heal J. 2011;17:784–793. doi: 10.26719/2011.17.10.784. [DOI] [PubMed] [Google Scholar]
- 51.International Association for the Study of Pain (IASP) Updated 2018. Cited 2019 May 015. Available from: https://www.iasp-pain.org/AboutIASP/?navItemNumber=506 .
- 52.Saudi Society of Pain Medicines (SSPM) Cited 2019 May 05. Available from: https://sspm.sa/mission-vision-2/
- 53.Brick JM, editor. Proceedings of Statistics Canada Symposium 2014. Rockville, MD: Westat and JPSM; 2015. Explorations in non-probability sampling using the web. [Google Scholar]
- 54.We Are Social, Saudi Arabia Digital 2019. Updated 2019. Cited 2019 May 05. Available from: https://datareportal.com/reports/digital-2018-saudi-arabia .