

Abstract
Nance–Horan syndrome (NHS) or X-linked cataract dental syndrome is an extremely rare condition affecting multiple systems. It is characterized by ophthalmological, dental, and facial anomalies. Individuals display facial dysmorphism, mandibular prognathism, congenital cataract, and strabismus. Common dental findings include notching of incisors, supernumerary teeth, and mulberry molars. This article aims to provide an update on NHS while reporting previously unreported findings such as talon's cusp and taurodontism.
Keywords: Dental anomalies, genetics, Nance–Horan syndrome, talons cusp, X-linked syndrome
Introduction
Most genetic syndromes are multifactorial, displaying signs that may involve various systems of the body. An accurate recognition of unusual dental findings may prove to be pivotal in the diagnosis of such conditions. Such an unusual multisystemic syndrome was first described by Nance et al. and Horan and Bilson in Australia in the year 1974 and was referred to as the Nance–Horan syndrome (NHS).[1,2] Its dental manifestations were reported later by Seow et al., which are now established diagnostic indicators of NHS.[3] It has also been termed by various authors as X-linked congenital cataracts and microcornea,[4] X-linked cataract–dental syndrome,[5] cataracts-oto-dental syndrome,[6] cataract–dental syndrome,[2] or mesiodens–cataract syndrome.[1]
NHS is an extremely rare X-linked genetic disorder (OMIM 302350), which is inherited in a co-dominant fashion, with heterozygous females seemingly less affected than affected males.[7,8,9] NHS results in semi-dominant transmission from truncated mutations, occurring in NHS genes of male gametes.[10,11]
NHS is usually characterized by ocular abnormalities, facial dysmorphism, and dental anomalies. The ocular abnormalities include congenital cataracts, microcornea, microphthalmia, strabismus and, frequently, severe nystagmus as well.[12] Dental anomalies are present in nearly 100% of cases and include findings such as Hutchinson's incisors, mulberry molars, supernumerary teeth, and pulp-space pathologies. This case report seeks to highlight the characteristic dental findings present in NHS and to advocate the presence of such findings as a diagnostic aid in its early detection and timely management.
Case Report
A 10-year-old male patient reported to the department of pedodontics and preventive dentistry with the chief complaint of irregularly placed front teeth. Medical history revealed that the patient was born with bilateral congenital cataracts, which were operated at 6 months of age. He wore corrective spectacles for the same, and his medical history was otherwise insignificant. Family history was nonsignificant. Extraoral examination revealed mild features of facial dysmorphism such as long narrow face, mandibular prognathism, large narrow nose with a high narrow nasal bridge, and large protruding anteverted ears [Figure 1]. No signs of any intellectual impairment were noticed, and the patient was capable of performing all activities in school and responded well to instructions.
Figure 1.

Anterior facial view
On intraoral examination, multiple dental anomalies were noticed. The incisors were of unusual morphology, displaying conical or screwdriver shape, along with the presence of notched incised edges (Hutchinson's incisors) [Figure 2a]. Prominent Talon's cusps were observed on both the upper lateral incisors [Figure 2b]. The molars displayed unusual morphology due to the presence of central supernumerary cusps and a globular appearance (mulberry molars). Generalized spacing was present and a predominantly permanent dentition was noticed, with the exception of unerupted permanent canines. Numerous carious lesions were noticed in the permanent molars.
Figure 2.
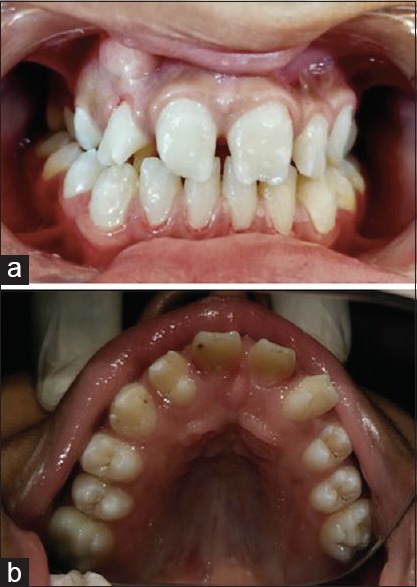
(a) Anterior view. (b) Maxillary occlusal view
A blood serological investigation was carried out to rule out the presence of congenital syphilis.
Radiological examination revealed the presence of impacted supernumerary teeth in relation to 46 and 36 [Figure 3A]. Pulpal pathologies such as multiple pulp stones in relation to 16 and 26 [Figure 3B] and enlarged pulp chambers suggestive of taurodontism in relation to 13 [Figure 3C] were also evident.
Figure 3.
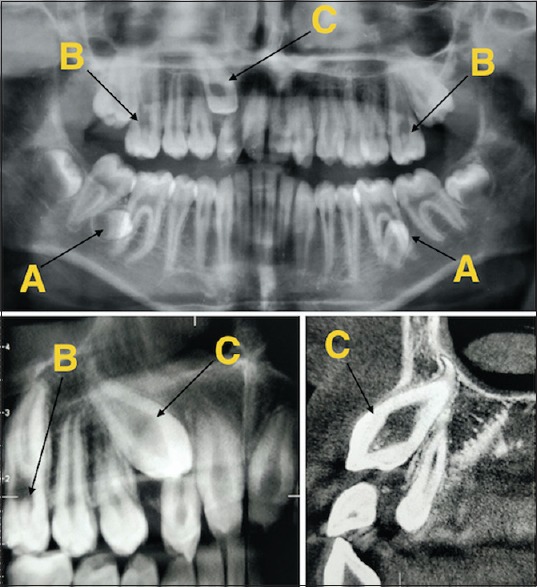
Orthopantomograph and cone-beam computed tomography images showing: (A) Impacted supernumerary teeth.(B) Pulpal calcifications/stones. (C) Taurodontism
A team of pediatric dentists, orthodontists, and oral surgeons were consulted to finalize a treatment plan. The treatment plan consisted of short- and long-term plans. The short-term plan constituted restorations of the multiple carious teeth and preventive restorations for the other molars.
The patient and his parents were explained about the elaborate orthodontic treatment required to assess their compliance and consent. The long-term plan constituted orthodontic intervention involving slow maxillary expansion using a bonded jack screw appliance with posterior bite plane to correct the transverse maxillary discrepancy manifesting as a posterior cross bite bilaterally. Postexpansion, a retention protocol of 3 months would have to be followed. This would be followed by orthodontic treatment with fixed mechanotherapy (0.022 slot McLaughlin Benett Trevisi). Since the 13 is bucally impacted [Figure 4a–d], space creation for 13 would be required, followed by surgical exposure under local anesthesia and traction into the arch. It was decided that the supernumerary teeth would be maintained in their current position, as their removal would necessitate removal of large amount of bone. However, regular follow-ups to check on any root resorption would be essential. Following treatment, permanent retention, not dependent on patient cooperation, would be required.
Figure 4.
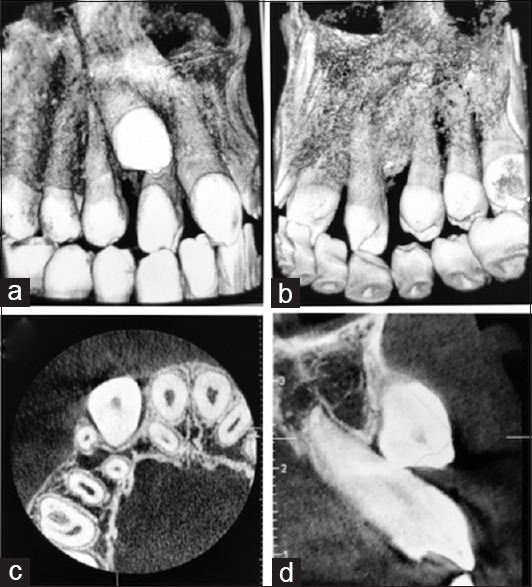
Three-dimensional images showing facially impacted 13. (a) Facial view. (b) Palatal view. (c) Occlusal view. (d) Lateral view
Composite adhesive restorations were carried out for 16, 26, 36, and 46, while preventive sealant restorations were carried out for 17, 27, 37, and 46. In addition, topical fluoride application was also done and oral hygiene instructions were given. The patient is being followed up at 3-month intervals.
Discussion
NHS is an extremely rare condition, which was first described simultaneously by Nance et al. and Horan and Bilson in two separate studies conducted in the year 1974. The initial studies failed to highlight the dental abnormalities associated with NHS, though until 1985 when Seow et al. listed multiple dental findings such as taurodontism, hyperdontia, pulpal abnormalities, and notched incisors.[3]
Most of the earlier studies reported characteristic facial dysmorphic features as displayed in our report such as large protruding anteverted ears, long narrow nose with high nasal bridge, long narrow face, and mandible prognathism. NHS is characterized by ocular defects such as congenital cataracts as shown in this report as well with a documented medical history of cataract removal at the age of 1 year. Unlike most studies, this patient did not display any signs of postoperative complications such as glaucoma, loss of vision, or intellectual impairment, as reported in few earlier cases.
NHS is characterized by distinct dental features which can be used for its accurate diagnosis. The syndrome manifests in the primary and permanent dentitions in all cases.[3,13,14,15] The molars are anatomically more rounded and globular, resembling a lotus flower. There is also the presence of a central supernumerary cusp that makes them appear like mulberry molars. The incisors are tapered and “screwdriver” shaped with notched or serrated edges, similar to Hutchinson's incisors that are found in congenital syphilis. These findings were also present in our patient.
Other findings such as supernumerary teeth, conical teeth, retained primary teeth, taurodontism, pulpal calcifications, and pulp stones have also been reported; however, retained primary teeth and supernumerary teeth were not found in our patient.[1,2,3,7,8,13,14,15,16] The occurrence of mesiodens has been reported in 65% of all cases.[17,18] Yellow-gray discoloration and caries are generally seen on teeth, and many patients get partial- or full-mouth dental extractions carried out between the third and fifth decades of life.[19]
Conclusion
Dentofacial findings can be a strong indicator of an underlying systemic condition. This case report seeks to highlight the importance of dental professionals in identifying any previously undetected systemic conditions by proper awareness and early detection of prominent dentofacial features. This report also seeks to highlight previously undetected dental findings such as talons cusp and taurodontism, not commonly associated with NHS. A multidisciplinary approach involving various medical and dental specialties such as pediatricians, ophthalmologists, genetic counselors, pediatric dentists, prosthodontists, orthodontists, and oral surgeons is the key to ensuring a better standard of life for the patient.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Horan M, Billson F. X-linked cataract and Hutchinsonian teeth. Aust Paediatr J. 1974;10:98–102. [Google Scholar]
- 2.Nance WE, Warburg M, Bixler D, Helveston EM. Congenital X-linked cataract, dental anomalies and brachymetacarpalia. Birth Defects Orig Artic Ser. 1974;10:285–91. [PubMed] [Google Scholar]
- 3.Seow WK, Brown JP, Romaniuk K. The Nance-Horan syndrome of dental anomalies, congenital cataracts, microphthalmia, and anteverted pinna: Case report. Pediatr Dent. 1985;7:307–11. [PubMed] [Google Scholar]
- 4.Lewis RA, Nussbaum RL, Stambolian D. Mapping X-linked ophthalmic diseases. IV. Provisional assignment of the locus for X-linked congenital cataracts and microcornea (the Nance-Horan syndrome) to xp22.2-p22.3. Ophthalmology. 1990;97:110–20. doi: 10.1016/s0161-6420(90)32644-1. [DOI] [PubMed] [Google Scholar]
- 5.Stambolian D, Lewis RA, Buetow K, Bond A, Nussbaum R. Nance-Horan syndrome: Localization within the region xp21.1-xp22.3 by linkage analysis. Am J Hum Genet. 1990;47:13–9. [PMC free article] [PubMed] [Google Scholar]
- 6.Sonoda T. Cataracts-oto-dental defects (Nance-Horan syndrome) Ryoikibetsu Shokogun Shirizu. 2001;33:344–5. [PubMed] [Google Scholar]
- 7.Toutain A. Philadelphia, PA: Lippincott Williams & Wilkins; 2003. NanceHoran syndrome. NORD Guide to Rare Disorders; pp. 654–5. [Google Scholar]
- 8.NanceHoran Syndrome. National Organization for Rare Disorders. 2011. Available from: https://www.rarediseases.org/rarediseases/nancehoransyndrome/
- 9.Tug E, Dilek NF, Javadiyan S, Burdon KP, Percin FE. A Turkish family with Nance-Horan syndrome due to a novel mutation. Gene. 2013;525:141–5. doi: 10.1016/j.gene.2013.03.094. [DOI] [PubMed] [Google Scholar]
- 10.Liao HM, Niu DM, Chen YJ, Fang JS, Chen SJ, Chen CH, et al. Identification of a microdeletion at xp22.13 in a Taiwanese family presenting with Nance-Horan syndrome. J Hum Genet. 2011;56:8–11. doi: 10.1038/jhg.2010.121. [DOI] [PubMed] [Google Scholar]
- 11.Burdon KP, McKay JD, Sale MM, Russell-Eggitt IM, Mackey DA, Wirth MG, et al. Mutations in a novel gene, NHS, cause the pleiotropic effects of Nance-Horan syndrome, including severe congenital cataract, dental anomalies, and mental retardation. Am J Hum Genet. 2003;73:1120–30. doi: 10.1086/379381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Walsh FB, Wegman ME. Pedigree of hereditary cataract, illustrating sex-limited type. Bull Johns Hopkins Hosp. 1937;61:125–35. [Google Scholar]
- 13.van Dorp DB, Delleman JW. A family with X-chromosomal recessive congenital cataract, microphthalmia, a peculiar form of the ear and dental anomalies. J Pediatr Ophthalmol Strabismus. 1979;16:166–71. doi: 10.3928/0191-3913-19790501-08. [DOI] [PubMed] [Google Scholar]
- 14.Walpole IR, Hockey A, Nicoll A. The Nance–Horan syndrome. J Med Genet. 1990;27:632–4. doi: 10.1136/jmg.27.10.632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bixler D, Higgins M, Hartsfield J., Jr The Nance–Horan syndrome: A rare X-linked ocular-dental trait with expression in heterozygous females. Clin Genet. 1984;26:30–5. doi: 10.1111/j.1399-0004.1984.tb00783.x. [DOI] [PubMed] [Google Scholar]
- 16.Toutain A. Nance-Horan syndrome. Orphanet Encyclopedia. 2003:14. [Google Scholar]
- 17.Sharma S, Datta P, Sabharwal JR, Datta S. Nance-Horan syndrome: A rare case report. Contemp Clin Dent. 2017;8:469–72. doi: 10.4103/ccd.ccd_232_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hibbert S. A previously unreported association between Nance-Horan syndrome and spontaneous dental abscesses. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99:207–11. doi: 10.1016/j.tripleo.2004.07.004. [DOI] [PubMed] [Google Scholar]
- 19.Lewis RA. Mapping the gene for X-linked cataracts and microcornea with facial, dental, and skeletal features to xp22: An appraisal of the Nance-Horan syndrome. Trans Am Ophthalmol Soc. 1989;87:658–728. [PMC free article] [PubMed] [Google Scholar]