

Abstract
Aims:
To assess the salivary flow rate levels and total antioxidant levels in ectodermal dysplasia (ED) patients and to compare with normal individuals.
Materials and Methods:
Unstimulated saliva sample of control and case were collected from the mouth to a pre-weighed Eppendorf tube using a Pasteur pipette for 4 min. Stimulated saliva of case and control was also collected after chewing paraffin wax for 30 s. Both the Eppendorf tubes were weighed again after collection of both the saliva samples. The flow rate was calculated as difference of weight of the tube divided by time (4 min). Both unstimulated and stimulated saliva was also separately collected for estimation for total antioxidant levels.
Statistical analysis:
For intergroup comparison, Mann–Whitney test was used, and for intragroup comparison, Wilcoxon signed-rank test was used.
Results:
In the intergroup comparison of both the salivary flow rate and total antioxidant levels, there was no statistically significant difference; however, there was statistically significant difference in the intragroup comparison of salivary flow rate and total antioxidant levels in case group.
Conclusions:
There was a diminished unstimulated salivary flow rate in ED group, but stimulated salivary flow rate was significantly high and the total antioxidant levels in unstimulated saliva of the case group were significantly higher than the stimulated antioxidant levels.
Keywords: Ectodermal dysplasia, salivary flow rate, total antioxidant levels
Introduction
Ectodermal dysplasias (EDs) are conditions constituting defect of developmental origin affecting two or more ectodermal evolved such as sweat glands, teeth, nails, and hairs. The ED was first published by Thurnam in 1848[1] and it was Weech[2] in 1929 who coined the term. The prevalence of ED has been assessed as between 1:10000 and 1:100000 live male birth.[3,4] To date, more than 192 distinctive ectodermal syndromes have been described.
The most common type of ED is the hypohidrotic ED (HED) and hidrotic ED. ED is constituted by frontal bossing, wrinkled and hyperpigmented skin around the eyes, saddle nose, thick and everted lips, sunken cheeks, and large, low-set ears. Delay in the eruption of permanent teeth, hypodontia, and conical shaped or pegged teeth are some of the dental manifestations.
Saliva depicts an individuals’ body health and therefore it is used to keep a check on health and diseased conditions. For the better understanding of involvement of the salivary gland in EDs, Nordgarden et al. conducted a study, wherein they found diminished flow of saliva from parotid and/or submandibular gland; moreover, a depleted unstimulated and stimulated salivary flow and submandibular glands is more affected than parotid glands in EDs.[5] Lexner et al. investigated female carriers along with genotype and phenotype in males influenced with X-linked HED. They concluded that oligodontia and subnormal saliva flow are strong clinical symptoms for potential female carriers.[6]
Free radicals are harmful for the body, and protection against these is provided by antioxidants which are present in all body fluids and tissues. These antioxidants have been contemplated as one of the vital contributing factors for the oral inflammatory pathologies.
Tulunoglu et al. examined saliva collected from caries-active and caries-free children for estimation of flow rates, pH, total proteins, buffer capacity, calcium, and antioxidant status. They could not find any union between salivary flow rate pH and buffering capacity values. Higher concentration of salivary calcium was shown by caries-free group, but caries-active groups gave a higher total protein and total antioxidant value.[7]
Preethi et al. studied caries-free and caries-prone children on the properties of saliva such as pH, flow rate, buffering capacity, calcium level, protein, and total antioxidant levels. The results depicted that in caries-prone children, the flow rate, pH, and buffering capacity were marginally diminished, but in caries-prone children, total antioxidant capacity and total protein of saliva consequently increased, and in caries-prone children, the total calcium significantly deprecated.[8]
Thus, the need of the hour is to detect how salivary flow rate affects ED children in the progression of caries since flow rate is one of the factors of the many multifactorial factors in caries. Knowing the possible risk in these children would promptly limit the progress of dental caries to avoid the debilitating outcomes. Various parameters in the saliva have been extensively studied when taken into account its relation to dental caries.
One such area with scope for exploration is the role of various total antioxidant levels in saliva and its important functions associated with counteracting inflammatory diseases. Thus, the role of salivary flow rate and total antioxidant levels as a marker for dental caries will prove very useful, especially while dealing with children with ED.
Methodology
Twenty children were selected to this study and divided into two groups of ten each one group of healthy individuals and the other with ED. Institutionalized ethical clearance and a signed patient consent form from each participant was obtained prior to the initiation of this study. Participants were asked not to drink alcohol or perform hard physical exercises the day before, and not to eat, drink, smoke, or brush their teeth in the last hour before the examination. They were asked to rinse oral cavity 20–30 min before collecting saliva to clear off any debris. Saliva was allowed to accumulate in the floor of the mouth. Unstimulated saliva was collected using a Pasteur pipette into a preweighed Eppendorf tube for 4 min [Figure 1].
Figure 1.

Collection of salivary sample using a Pasteur pipette
The stimulated saliva was collected after asking the patient to chew on a piece of paraffin at approximately 45 chews per minute. After which the stimulated saliva was collected similarly to unstimulated saliva. Immediately, the patients’ salivary flow rate for both the unstimulated and stimulated saliva flow was calculated followed by transportation in an ice box [Figure 2] for saliva sample analysis of total antioxidant levels. The Eppendorf tubes were pre-weighed in Sartorius weighing machine [Figure 3] and was found to be 1036 mg. After saliva sample collection, the Eppendorf tube was again weighed.
Figure 2.
Transportation of saliva samples in an ice Box
Figure 3.
Sartorius weighing machine
The total antioxidant levels were evaluated by antioxidant assay [Figure 4] using phosphomolybdenum method.[9]
Figure 4.

Total Antioxidant Assay Kit
The salivary flow rate was estimated = (Postweight measure − preweight measure)/collection period
Thus, the salivary flow rate was determined in g/min.
Results
The individual whole salivary flow rate of the control group (normal individuals) is presented in Table 1 and that of the case group (individuals having ED) is presented in Table 2.
Table 1.
Salivary flow rate of control group
| Serial number | Unstimulated saliva (mg/min) | Stimulated saliva (mg/min) |
|---|---|---|
| 1 | 139.9 | 184.5 |
| 2 | 24.3 | 45.15 |
| 3 | 72.7 | 93 |
| 4 | 83.5 | 108.7 |
| 5 | 46.6 | 72.8 |
| 6 | 107.7 | 116.4 |
| 7 | 62.6 | 76.6 |
| 8 | 93.1 | 103.7 |
| 9 | 83.7 | 119.2 |
| 10 | 91.7 | 152.2 |
| Mean | 80.5±32.07 | 107.22±40.02 |
Table 2.
Salivary flow rate of case group
| Serial number | Unstimulated saliva (mg/min) | Stimulated saliva (mg/min) |
|---|---|---|
| 1 | 83.7 | 205.8 |
| 2 | 29.7 | 99.3 |
| 3 | 38.1 | 101.1 |
| 4 | 57.2 | 144.7 |
| 5 | 24.8 | 73.4 |
| 6 | 30.2 | 140.8 |
| 7 | 63.5 | 75.6 |
| 8 | 39.7 | 89.4 |
| 9 | 172 | 227.1 |
| 10 | 106.4 | 129 |
| Mean | 64.53±45.95 | 128.62±52.78 |
The total antioxidant levels of controls are presented in Table 3 and the total antioxidant levels of the case group are presented in Table 4.
Table 3.
Total antioxidant levels of control group
| Serial number | Unstimulated antioxidants | Stimulated antioxidants |
|---|---|---|
| 1 | 1620 | 3220 |
| 2 | 460 | 1440 |
| 3 | 3420 | 2360 |
| 4 | 3440 | 3520 |
| 5 | 4810 | 3500 |
| 6 | 213 | 91 |
| 7 | 133 | 122 |
| 8 | 221 | 254 |
| 9 | 308 | 186 |
| 10 | 225 | 158 |
| Mean | 1485±1754.58 | 1485.10±1518.18 |
Table 4.
Total antioxidant levels of case group
| Serial number | Unstimulated antioxidants | Stimulated antioxidants |
|---|---|---|
| 1 | 2320 | 990 |
| 2 | 640 | 430 |
| 3 | 1280 | 750 |
| 4 | 500 | 340 |
| 5 | 810 | 710 |
| 6 | 89 | 21 |
| 7 | 85 | 19 |
| 8 | 61 | 16 |
| 9 | 21 | 12 |
| 10 | 83 | 19 |
| Mean | 588.90±737.46 | 330.70±373.44 |
Intergroup comparison of salivary flow rate
The mean unstimulated salivary flow rates in case and control were 64.53 ± 45.95 ml/min and 80.58 ± 32.07 ml/min, respectively. On applying MannWhitney U-test, P value obtained was 0.212. The inference is that there was no statistical difference in unstimulated salivary flow rate between case and control groups [Graph 1]. Similarly, the mean stimulated salivary flow rates in case and control were 128.62 ± 52.78 ml/min and 107.22 ± 40.02 ml/min, respectively. Comparison using Mann–Whitney U-test gave a P value of 0.496. The inference is that there was no statistical difference in flow rate of stimulated saliva between case and control groups [Graph 2].
Graph 1.
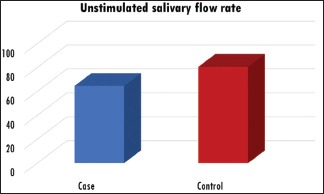
Comparison of unstimulated salivary flow rate between case and control groups
Graph 2.
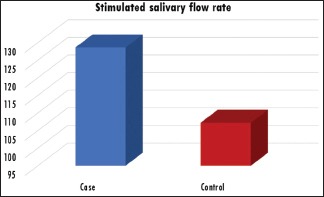
Comparison of stimulated salivary flow rate between case and control groups
Intergroup comparison of total antioxidant levels
The mean unstimulated total antioxidant levels in case and control groups were 588.90 ± 737.46 and 1485.00 ± 1754.58 μg/ml, respectively. On applying Mann–Whitney U-test, P value obtained was 0.151. This shows that there was no statistical difference between the total antioxidant levels in unstimulated saliva of case and control groups [Graph 3]. The mean total antioxidant levels of stimulated saliva in case and control were 330.70 ± 373.44 μg/ml and 1485.10 ± 1518.18 μg/ml, respectively. Comparison of these values using Mann–Whitney U-test gave a P value of 0.059. The inference is that there was no statistical difference in total antioxidant levels of stimulated saliva between case and control groups [Graph 4].
Graph 3.
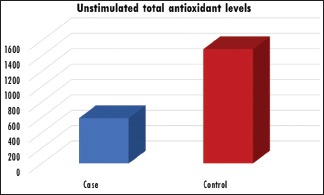
Comparison of unstimulated total antioxidant levels between case and control groups
Graph 4.
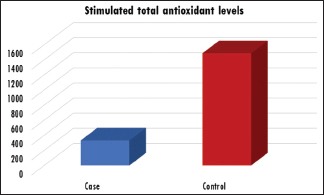
Comparison of stimulated total antioxidant levels between case and control groups
Intragroup comparison of salivary flow rate
The mean unstimulated and stimulated salivary flow rates in case group were 64.53 ± 45.95 ml/min and 128.62 ± 52.78 ml/min, respectively. On applying Wilcoxon signed-rank test, a P value of 0.005 was obtained. Since the P < 0.005, it was inferred that there was a statistically significant difference in unstimulated and stimulated salivary flow rate in the case group [Graph 5]. Similarly, the mean unstimulated and stimulated salivary flow rates in the control group were 80.58 ± 32.07 ml/min and 107.22 ± 40.02 ml/min, respectively. Comparison of these values using Wilcoxon signed-ranks test gave a P value of 0.005 which also showed a statistically significant difference between the two values [Graph 6].
Graph 5.
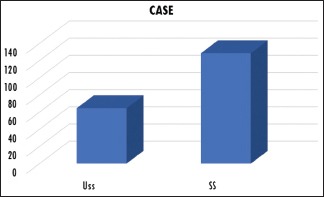
Comparison of unstimulated and stimulated salivary flow rate in the case group. USS = Unstimulated saliva, SS = Stimulated saliva
Graph 6.
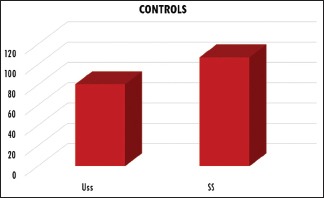
Comparison of unstimulated and stimulated salivary flow rate in the control group. Uss: Unstimulated saliva, SS: Stimulated saliva
Intragroup comparison of total antioxidant levels
The mean unstimulated and stimulated total antioxidant levels in the case group were 588.90 ± 737.46 μg/ml and 330.70 ± 373.44 μg/ml, respectively. On applying Wilcoxon signed-ranks test, to compare these two values, a P value of 0.005 was obtained. The inference is that there was a statistically significant difference in unstimulated and stimulated total antioxidant levels in case group [Graph 7]. The total antioxidant levels in unstimulated and stimulated saliva in the control group were 1485.00 ± 1754.58 μg/ml and 1485.10 ± 1518.18 μg/ml, respectively. The comparison of these two values using Wilcoxon signed-ranks test gave a P value of 0.646 which inferred that there was no statistically significant difference between the total antioxidant levels in unstimulated and stimulated saliva of control group [Graph 8].
Graph 7.
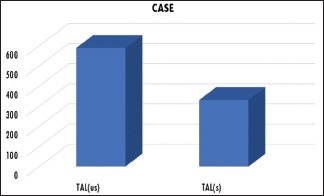
Comparison of unstimulated and stimulated total antioxidant levels in the case group. TAL(us): Unstimulated total antioxidant levels, TAL(s): Stimulated total antioxidant levels
Graph 8.
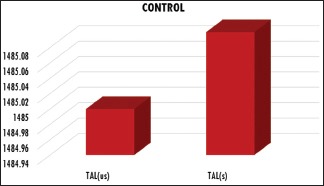
Comparison of unstimulated and stimulated total antioxidant levels in the control group. TAL(us): Unstimulated total antioxidant levels, TAL(s): Stimulated total antioxidant levels
Discussion
The teeth and oral mucosa constantly bathes in the saliva, which constitutes electrolytes, proteins, glycoproteins, and organic molecules conveyed from the blood. Whole saliva is a mixture of the secretions from the major (parotid, submandibular, sublingual) and minor salivary glands, as well as the gingival fluid. The quantity and composition of the salivary secretions determine its ability to affect caries development. In this study, the inclusion criteria in the case group were children of age 1–15 years having 2 or more defects in ectodermally derived structures which enabled us to consider them as having ED. Classifying them further into different variants was not done in this study. ED condition requires a multidisciplinary approach for diagnosis and treatment. The most important caries-preventive functions of saliva are the flushing and neutralizing effects. Greater the flow rate, brisker is the oral clearance.[10]
The collection of saliva was performed in this study to assess the salivary flow rate and total antioxidant levels which serve as biomarkers for dental caries. Saliva is an inherent factor, of human body being detrimental in the development and progression of caries. Since ED is associated with defects in ectodermally derived structures such as salivary glands, it could affect the salivary flow rate and composition, thereby increasing the caries risk. An attempt was made to demonstrate whether salivary flow rate and total antioxidant levels change in ED. In our study, ten children with ED and ten healthy children were selected for evaluation. Children with other systemic diseases, medically compromised conditions, and mentally and physically disabled children were excluded.
Before saliva collection, a general physical examination and a thorough oral examination was carried out. The instructions before collection of saliva that were followed were in accordance with previous studies done by Nordgarden et al.[5]
Navazesh[11] recommended that the finest two ways to collect whole saliva are the draining method and the dripping method. In the first method, saliva is allowed to drip off the lower lip, and in the second method, patient expectorates saliva into a test tube. Unstimulated saliva is usually collected by a method described by Mandel[12] by passive drooling into a graduated tube or preweighed vial. In this study, salivary flow rate was computed by suction method which was found to be more convenient. Saliva was collected using a pasture pipette and Eppendorf tube. The method of collection of saliva using polythene pipette and Eppendorf tube was used by Menon et al.[13] and Fathima and Balagopal.[14]
After collection of saliva, the samples were then stored under low temperature in an “ultra-cool temperature storage unit” at −80°C to prevent microbial growth and avoid degeneration of antioxidants present in the collected saliva until the analysis of total antioxidant levels. This methodology of storage at ultra-cool temperature was also performed by Menon et al.[13] and Fathima and Balagopal.[14] The saliva sample is transported from ultra-cool temperature storage in a hermetically sealed case containing ice within 30 min for the estimation of total antioxidants levels. The total antioxidant levels are evaluated by the phosphomolybdenum method. Similar evaluation methods of total antioxidant level was also done by Xavier et al. and Banda et al.[15,16]
In this study, the unstimulated salivary flow rate in case and control gave a mean of 64.53 ± 45.95 ml/min and 80.58 ± 32.07 ml/min, respectively. Similarly, the stimulated flow rate in case and control gave a mean of 128.62 ± 52.78 ml/min and 107.22 ± 40.02 ml/min, respectively. The diminished unstimulated salivary flow established in the ED group is in accordance with the formerly described findings of unstimulated salivary secretion in the ED group. Diminished salivary flow is seen in individuals with salivary gland hypoplasia and aplasia. However, no statistically significant differences in the unstimulated salivary flow rate between the control and the ED groups could be established in this study. Although the increased caries risk in ED group could primarily be attributed to the low salivary secretion, other etiological factors could also play a contributory role in caries development and progression. However, the stimulated salivary flow rate was marginally higher in ED group, showing that caries defense is correlated with stimulated saliva, rather than unstimulated saliva, maybe because stimulated saliva contains larger mineral content and leads to greater buffering capacity and salivary clearance.
The ectodermal derivatives in EDs range from normal to those severely affected. In addition, some variants are affected more than others. A few individuals in the ED group exhibited almost regular salivary flow rates, depicting conditions with moderate or no dysfunction of the salivary glands. Since this study did not classify ED in test group, this group had a wide spectrum of array of ED. There are several defensive and protective factors present in saliva and salivary analyses did not broaden to include more such parameters in this study.
Antioxidant system comprises enzymes such as superoxide dismutase, glutathione peroxidase, ceruloplasmin, albumin, catalase, ferritin, alpha tocopherol, beta carotene, uric acid, reduced glutathione, ascorbic acid, and bilirubin. The cumulative of endogenous and diet-derived antioxidants serves as the total antioxidant capacity of the body. Thus, the overall antioxidant capacity may provide more compatible information compared to that attained by the assessment of individual components.[16]
To the best of our knowledge, this is the first study assessing the total antioxidant levels in ED patients. Oxidative stress may play an important role in onset and development of several inflammatory oral pathologies and dental caries. In this study, total antioxidants in unstimulated saliva of the case group were significantly higher than stimulated antioxidant levels, which is in agreement with studies done by Tulunoglu et al.[7] and Preethi et al.[8] But, in the control group, difference in total antioxidant levels between unstimulated and stimulated saliva was not significant, but was comparable. This could be due to the absence of an infectious challenge in the form of caries.
In the different forms of ED, salivary glands are mostly affected. In patients suspected with ED, the health personnel should examine oral mucosa for dryness and do simple sialometric tests whenever symptoms are shown. Such tests contribute valuable information during oral prophylactic regimens in such individuals. Thus, assessment of salivary flow rate and total antioxidant levels in ED patients plays an important role in therapeutic and preventive strategies of dental caries.
Conclusions
Today, we have greater knowledge on the initiation, progression, and transmission of dental caries. However, we are not able to explain what causes the disease in some individuals while not in others, though the etiological factors and cariogenic microbes remain the same.
The outcomes of this study can be outlined as follows:
Although there was a diminished unstimulated salivary rate in the ED group, the stimulated salivary flow rate was high and the difference was statistically significant
The total antioxidant capacity in unstimulated saliva of the case group was significantly higher than the stimulated antioxidant levels.
A more detailed and extended investigation is however needed to be carried out, requiring that more samples and clinical studies are required to establish the exact relationship between the dental caries and physicochemical properties of saliva.
Monitoring of secretory function can be incorporated as a routine examination procedure by the dentist and can be a valuable adjunct to oral diagnosis, and clinical procedures can be initiated immediately to prevent the deleterious consequences of salivary gland hypofunction, especially in a systemic disease such as ED.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Thurnam J. Two cases in which the skin, hair and teeth were very imperfectly developed. Med Chir Trans. 1848;31:71–82. doi: 10.1177/095952874803100108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Weech AA. Hereditary ectodermal dysplasia (congenital ectodermal defect): A report of two cases. Am J Dis child. 1929;37:766–90. [Google Scholar]
- 3.Passi D, Mehta G, Vishwakerma K, Singh P. Ectodermal dysplasia: Case report & literature review. Eur J Dent Ther Res. 2013;3:170–3. [Google Scholar]
- 4.Renahan N, Raj R, Varma RB, Kumar JS. Christ siemens Touraine syndrome: Two case reports and felicitous approaches to prosthetic management. Contemp Clin Dent. 2015;6:274–6. doi: 10.4103/0976-237X.156066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Nordgarden H, Storhaug K, Lyngstadaas SP, Jensen JL. Salivary gland function in persons with ectodermal dysplasias. Eur J Oral Sci. 2003;111:371–6. doi: 10.1034/j.1600-0722.2003.00058.x. [DOI] [PubMed] [Google Scholar]
- 6.Lexner MO, Bardow A, Juncker I, Jensen LG, Almer L, Kreiborg S, et al. X-linked hypohidrotic ectodermal dysplasia. Genetic and dental findings in 67 Danish patients from 19 families. Clin Genet. 2008;74:252–9. doi: 10.1111/j.1399-0004.2008.01037.x. [DOI] [PubMed] [Google Scholar]
- 7.Tulunoglu O, Demirtas S, Tulunoglu I. Total antioxidant levels of saliva in children related to caries, age, and gender. Int J Paediatr Dent. 2006;16:186–91. doi: 10.1111/j.1365-263X.2006.00733.x. [DOI] [PubMed] [Google Scholar]
- 8.Preethi BP, Reshma D, Anand P. Evaluation of flow rate, pH, buffering capacity, calcium, total proteins and total antioxidant capacity levels of saliva in caries free and caries active children: An in vivo study. Indian J Clin Biochem. 2010;25:425–8. doi: 10.1007/s12291-010-0062-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Patni V, Baliga S, Sawal S. Saliva as a diagnostic tool for measurement of total antioxidant capacity in children with leprosy and born to leprosy parent. Indian J Lepr. 2015;87:17–21. [PubMed] [Google Scholar]
- 10.Miura H, Isogai E, Hirose K, Wakizaka H, Ueda I, Ito N, et al. Application of a sucrose indicator strip to evaluate salivary sucrose clearance. J Dent. 1991;19:189–91. doi: 10.1016/0300-5712(91)90016-r. [DOI] [PubMed] [Google Scholar]
- 11.Navazesh M. Methods for collecting saliva. Ann N Y Acad Sci. 1993;694:72–7. doi: 10.1111/j.1749-6632.1993.tb18343.x. [DOI] [PubMed] [Google Scholar]
- 12.Mandel ID. The diagnostic uses of saliva. J Oral Pathol Med. 1990;19:119–25. doi: 10.1111/j.1600-0714.1990.tb00809.x. [DOI] [PubMed] [Google Scholar]
- 13.Menon MM, Balagopal RV, Sajitha K, Parvathy K, Sangeetha GB, Arun XM, et al. Evaluation of salivary interleukin-6 in children with early childhood caries after treatment. Contemp Clin Dent. 2016;7:198–202. doi: 10.4103/0976-237X.183059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Fathima N, Balagopal RV. Importance of comprehensive dental treatment and health education for children with Down syndrome. Int J Paediatr Dent. 2015;25(Suppl S1):36. [Google Scholar]
- 15.Xavier AM, Rai K, Hegde AM. Total antioxidant concentrations of breastmilk – An eye-opener to the negligent. J Health Popul Nutr. 2011;29:605–11. doi: 10.3329/jhpn.v29i6.9897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Banda NR, Singh G, Markam V. Evaluation of total antioxidant level of saliva in modulation of caries occurrence and progression in children. J Indian Soc Pedod Prev Dent. 2016;34:227–32. doi: 10.4103/0970-4388.186747. [DOI] [PubMed] [Google Scholar]