

Abstract
Background
In the literature under review there are about 300 reported cases of vaginal leiomyomas with none from Cameroon. We report a case of vaginal leiomyoma and highlight the diagnostic challenges faced at the Douala Referral Hospital (DRH), Cameroon.
Case presentation
A 36-year-old G3P3002 sexually active Cameroonian married woman reported dysuria, dyspareunia, cessation of sexual intercourse and offensive smelling vaginal discharge for 6 months and a 3-year history of a vaginal tumour; she was misdiagnosed despite ultrasonography and magnetic resonance imaging (MRI) but was corrected by an experienced radiologist. She underwent first look laparoscopy, surgical excision of the tumour through the vagina and histopathology analysis that confirmed leiomyoma.
Conclusion
Posterior location of vaginal leiomyomas found in this case is a rare occurrence. The diagnosis is based on careful examination and preoperative imaging (ultrasonography and MRI). However, the definitive diagnosis is usually made intra-operatively. We combined laparoscopic exploration of the internal genital organs and per vaginal excision of the vaginal leiomyoma. Thus, we recommend frozen section biopsy to exclude leiomyosarcoma.
Keywords: Vaginal leiomyoma, Misdiagnosis, Laparoscopy, Magnetic resonance imaging, And ultrasonography
Background
Vaginal leiomyomas are rare benign tumours with only about 300 reported cases in medical literature [1]. To the best of our knowledge, there has been no case of vaginal leiomyoma reported in the medical literature from sub-Saharan Africa, and Cameroon in particular. These tumours usually arise from the anterior vaginal wall and, depending on the size and site, may cause varied clinical presentations such as dyspareunia, pain, or dysuria [2]. Vaginal leiomyomas sometimes occur concurrently with leiomyomas elsewhere in the body [3]. The clinical diagnosis of vaginal leiomyoma requires a high index of suspicion because the tumour could easily be mistaken for a cystocele, urethrocele, Skene duct abscess, Gartner duct cysts, urethral diverticulum, vaginal cysts, Bartholin gland cysts, or vaginal malignancy [4, 5]. The diagnosis is usually confirmed by histopathology.
We are reporting the case of a vaginal leiomyoma that we treated with first look laparoscopy and surgical excision through the vaginal route at the Douala Referral Hospital (DRH), Cameroon.
Case presentation
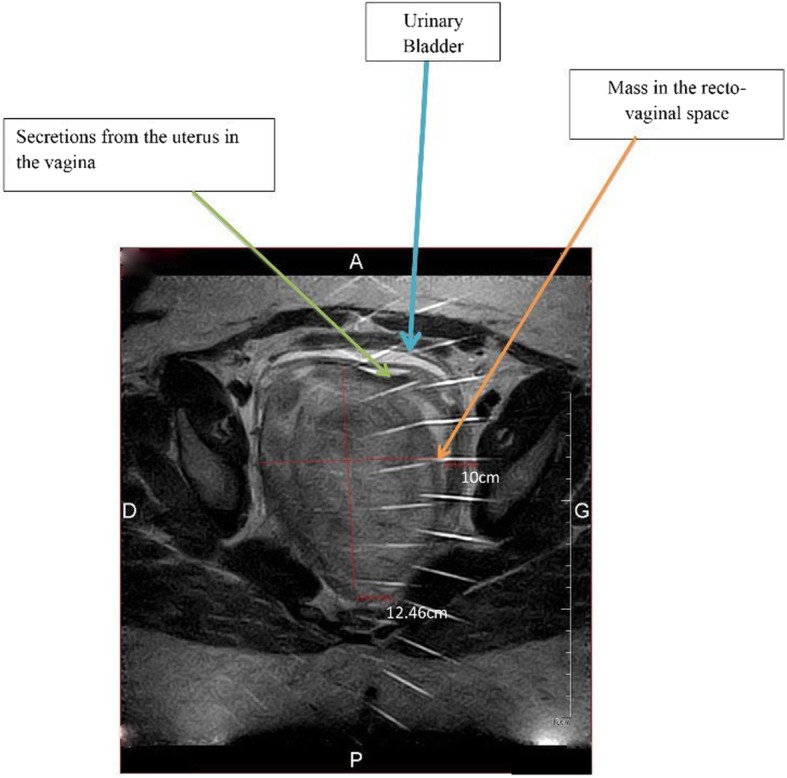
A 36-year-old G3P3002 sexually active Cameroonian married woman came to our department complaining of dysuria, dyspareunia, cessation of sexual intercourse and offensive foul-smelling vaginal discharge for a period of 6 months. She had noticed a growth bearing down on her vagina 3 years earlier and the growth rapidly increased in size in the last 6 months. On physical examination, she looked well; her blood pressure was 130/80 mmHg, pulse 84 beats/min. and temperature of 37.4 °C. She had a non-tender tumour that was rubbery in consistency and occluding the vagina thereby impeding access to the uterine cervix. On digital rectal examination, the tumour was impinging on and compressing both the bladder and the rectum (Fig. 1); allowing for micturition only in the erect position. Blood levels of tumour markers showed the following: CA 125; 12 IU/mL (normal value< 35 IU/mL), CA 19.9; 5.4 IU/mL (normal value < 37 IU/mL) and CA 15.3; 1.2 IU/mL (normal value< 31.3 IU/mL). Furthermore, hemoglobin level was 10.8 g/dL, hematocrit level 32.5%; aspartate aminotransferase (AST) 18.4 IU/L (normal value< 46 IU/L), alanine aminotransferase (ALT); 10.3 IU/L (normal value< 49 IU/L), blood urea nitrogen (BUN); 0.25 g/L (normal value; 0.15 to 0.45 g/L), and creatinine level 9.5 mg/L (normal value; 6 to 13 mg/L). Besides, immunohistochemistry was not accessible in the DRH during the period of study therefore we could not measure the LDH levels. An abdominal ultrasonography showed a 60 mm × 40 mm hypoechogenic tumour in the upper part of the vagina and pelvis. Magnetic resonance imaging (MRI) of the abdomen and pelvis had earlier misdiagnosed the tumour; right posterior pelvic peritoneal tumour measuring (137 × 73 × 118 mm). However, a re-examination of the MRI images by an experienced radiologist correctly diagnosed a vaginal tumour (102.7 × 175.8 mm) bulging through the posterior fornix and pushing up the pouch of Douglas and compressing the bladder and rectum, which is suggestive of vaginal leiomyoma (Fig. 2 and Fig. 3). The tumour was projecting through the vulva. A biopsy and histopathology of the visible vaginal tumour confirmed leiomyoma. At first look laparoscopy, the uterus and adnexa were normal and both deviated to the right side of the pelvis. We excised the leiomyoma through the vaginal route by sharp and blunt dissection. We removed a whorled whitish lobular vaginal fibroid (131.4 × 147.7 mm) occupying the rectovaginal space. The fourchette provided attachment for the vaginal leiomyoma (Fig. 4). Vaginal closure was in two layers and blood loss was minimal. The uterine cervix was microscopically normal (Fig. 5), and post-operative histopathology confirmed vaginal leiomyoma.
Fig. 1.
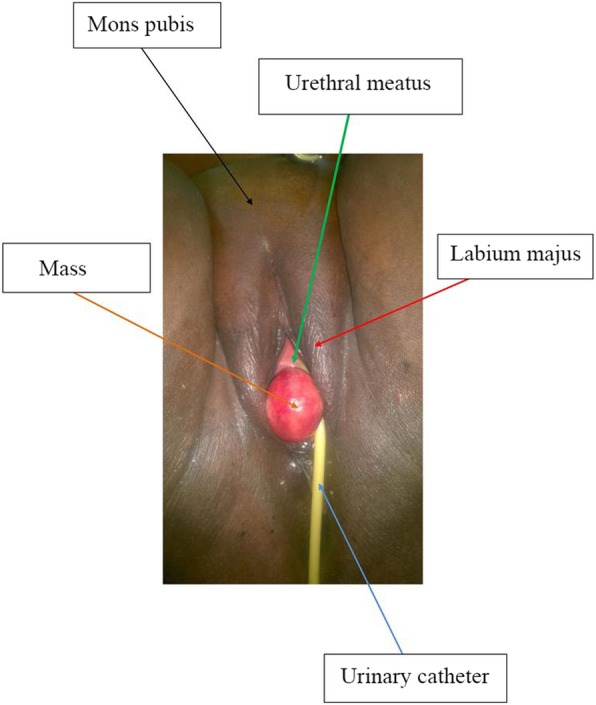
Tumour occluding and projecting through the vagina
Fig. 2.

Magnetic Resonance Image (longitudinal view) of the pelvis and perineum showing pelvic mass, and fluid collection in the vagina. The uterus is deviated by the mass with secretions flowing through the cervix. The mass compresses the bladder anteriorly and the rectum posteriorly
Fig. 3.
Magnetic resonance image (Cross-sectional view) of the pelvis and perineum. The uterus is not visualized in this section. The mass is seen with free fluid in the vagina
Fig. 4.
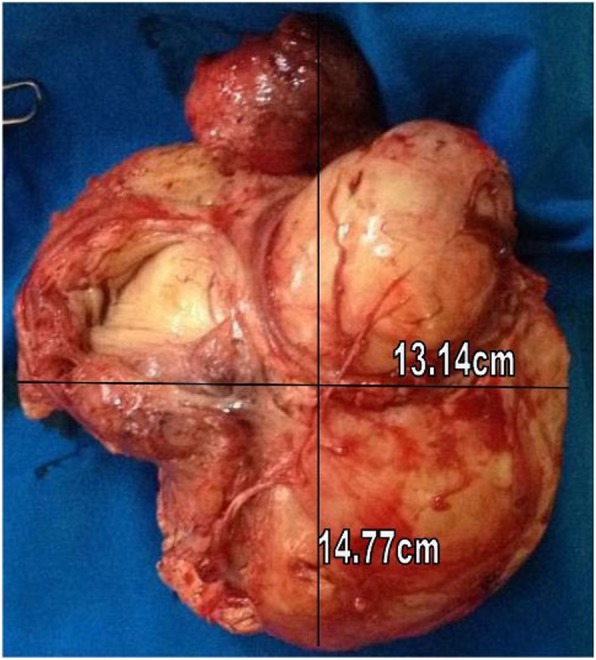
Vaginal tumour removed having whorled yellowish-white appearance characteristic of leiomyoma and measuring 13.14 cm × 14.77 cm
Fig. 5.
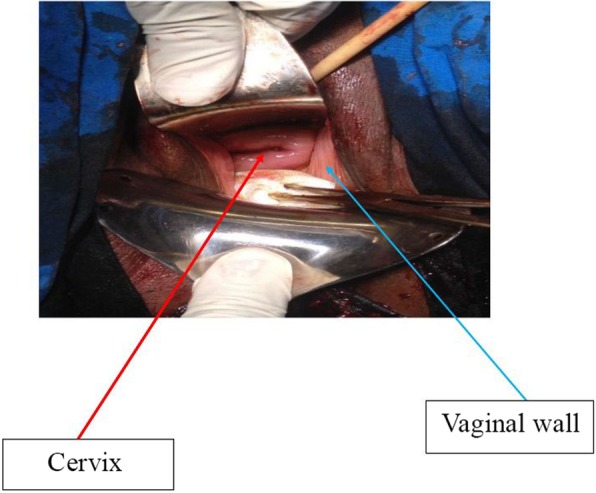
Vagina after removal of tumour. The uterine cervix is macroscopically normal
Discussion and conclusion
Leiomyomas are benign tumours of the female genital tract common among African-American and black women of reproductive age [6–8]. These tumours are common in the uterus and to some extent, in the cervix, the round ligament, uterosacral ligament, ovary, and inguinal canal, respectively [1].
Prevalence of vaginal leiomyoma
Leiomyomas of the vagina are rare and there are 300 reported cases in the medical literature we reviewed [1, 3]. Vaginal leiomyomas are common in women between 35 to 50 years and more common among Caucasian women [3]. Vaginal leiomyomas are rare in most sub-Saharan African countries, as opposed to uterine leiomyomas. The reason for this difference is attributed to misdiagnosis, failure to seek medical attention and lack of correct reporting.
Diagnosis of vaginal leiomyoma
These tumours usually occur as a single, well-circumscribed mass arising from the midline anterior wall, and less commonly from the anterior and lateral walls [9]. In our case, the tumour was not well circumscribed as described in the literature and was located in the posterior wall (recto-vaginal space), thereby decreasing the clinical likelihood of suspicion. Vaginal tumours are usually asymptomatic but may occasionally present symptoms ranging from lower abdominal pain, low back pain, vaginal bleeding, dyspareunia, urinary symptoms like frequency, dysuria or other features of vagina or urinary obstruction [2, 10]. Preoperative imaging and careful examination may help rule out a malignancy. However, this was not the case with the index case that underwent biopsy because tumour was accessible. Besides, others have reported abnormally high levels of CA 125, CA 19.9 and CA 15.3 in 19.7%, 6.6% and 5.1% of patients, respectively [11] but we did not find similar results in the index case. Furthermore, elevated levels of lactate dehydrogenase LDH-A and LDH-D were reported in patients with uterine leiomyosarcoma compared with those with uterine leiomyomas [12]. In addition, other studies have suggested that, the assessment of LDH isoenzymes may be relevant in the preoperative diagnosis of uterine sarcoma [13]. However, LDH assessment was not accessible to the index case because of lack of facilities to carry out immunohistochemistry at the time of study. We used ultrasonography and MRI in diagnosing vaginal tumour. At the DRH, magnetic resonance imaging (MRI) is meant for suspected malignancies because it is not accessible to most patients due to the cost (about $250). In MRI, the tumour appears as a well-demarcated solid mass of low signal intensity in T1 and T2 weighted images with homogenous contrast enhancement while leiomyosarcomas and other vaginal malignancies show characteristic high T2 signal intensity with irregular and heterogeneous areas of necrosis or haemorrhage [9, 14, 15]. The use of MRI is especially useful when fibroids are growing rapidly, have poor delineation on ultrasound and when there is suspicion of malignancy [16]. MRI is accurate in diagnosing a leiomyoma with a sensitivity of 88–93% and a specificity of 66–91% [6].
There is a reported case of necrotizing ruptured leiomyoma mimicking a malignant neoplasm that was clarified by MRI. The mass was 70 mm × 50 mm at the distal end of the left anterior aspect of the vagina displacing the urethra anteriorly. It has low signal intensity on T1-weighted image, high signal intensity on T2 weighted image and irregular enhancement on post-contrast-enhanced image as if it were a malignant tumour [4].
There is an estimated 2 to 5% error margin in radiological examinations in the medical literature and this may increase to 40% in emergencies. We attribute these errors to complacency, poor communication, staff shortage, heavy workloads, a dearth of earlier reports for comparison, and unavailability of trained radiologists [17–20]. In the present context, there is no study in the Department of Radiology of the DRH to estimate radiologic accuracy. There are an estimated 140 radiology examinations per day in the Radiology Department of the DRH. Assuming a 2 to 5% margin of error [16–18] in radiologic diagnosis as reported previously, a misdiagnosis in diagnostic radiology may occur several times per day at the DRH.
Management of Vaginal Leiomyomas
Surgical excision through the vaginal route has been the traditional approach for vaginal tumours but the abdominoperineal route is necessary for huge tumours [3, 19]. For the index case, we combined laparoscopic exploration of the abdominal cavity (internal genital organs) and per vaginal excision of the vaginal leiomyoma.
Some studies have reported the assessment of LDH isoenzymes levels by immunohistochemistry to differentiate between leiomyoma and leiomyosarcoma. However, because of the lack of immunohistochemistry facility and risk of misdiagnosis during MRI, frozen biopsy may be important to differentiate leiomyosarcoma from leiomyoma in our setting. Besides, other studies have reported that the overall accuracy of frozen section to determine the status of malignancy was 93.3% in patients with ovarian tumours [21]. Furthermore, another study have reported that Frozen section performed at the time of a total hysterectomy rendered the diagnosis of malignant mixed-müllerian tumour [22]. There are reports of laparoscopic ablation of a tumour with posterior colpotomy for the management of vaginal leiomyomas but this has not gained worldwide acceptance [23]. However, if vaginal leiomyoma is diagnosed before surgery, gonadotropin-releasing hormone analogues (GnRH-a) or selective progesterone receptor modulators (SPRM) to reduce tumour size or preoperative embolization to reduce intraoperative blood loss may be used [24]. Furthermore, there are reports of changes in sexuality and intimacy among patients after diagnosis and treatment of vaginal tumours [25]. This couple had also suspended sexual intercourse and therefore required psychological support.
Limitations
There is a reported correlation between estrogen (ER) and epidermal growth factor (EGFR) receptors and vaginal leiomyoma [22] but we did not have the facilities to do immunohistochemistry. The couple could not get psychological support because of a lack of staff to offer such services.
In conclusion, posterior location of vaginal leiomyomas found in this case is a rare occurence. The diagnosis is based on careful examination and preoperative imaging (ultrasonography and MRI). However, definitive diagnosis is usually made intra-operatively. We combined laparoscopic exploration of the internal genital organs and per vaginal excision of the vaginal leiomyoma. Thus, we recommend frozen section to exclude leiomyosarcoma.
Acknowledgements
We are grateful to the nurses and staff of the Douala Referral Hospital for their support during the management of the patient.
Abbreviations
- ALT
Alanine aminotransferase
- AST
Aspartate aminotransferase
- CA
Cancer antigen or carcinoma antigen
- DRH
Douala Referral Hospital
- EGFR
Epidermal growth factor
- ER
Estrogen receptor
- GnRH-a
Gonadotropin releasing hormone analog
- LDH
Lactate dehydrogenase
- MRI
Magnetic resonance imaging
- SPRM
Selective progesterone receptor modulator
Authors’ contributions
TOE, PNT contributed to the project development and manuscript writing/editing. TOE, FMK, MMJA, EBP: were a part of the surgical team and alongside author EMW, contributed in the imaging studies and editing of the manuscript. All authors read and approved the final manuscript.
Funding
None.
Availability of data and materials
Not applicable.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor-in-chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Thomas Obinchemti Egbe, Email: toegbe@gmail.com, Email: obinchemti@yahoo.com.
Fidelia Mbi Kobenge, Email: Fidelianew@hotmail.com.
Junette Arlette Mbengono Metogo, Email: junetmell@yahoo.fr.
Emmanuella Manka’a Wankie, Email: mankaawe@gmail.com.
Paul N. Tolefac, Email: ptolefac15@gmail.com
Eugene Belley-Priso, Email: robelsogene@yahoo.fr.
References
- 1.Young SB, Rose PG, Reuter KL. Vaginal fibromyomata: two cases with preoperative assessment, resection, and reconstruction. Obstet Gynecol. 1991;78(5 Pt 2):972–974. [PubMed] [Google Scholar]
- 2.Costantini E, Cochetti G, Porena M. Vaginal Para-urethral myxoid leiomyoma: case report and review of the literature. Int Urogynecology J. 2008;19:1183–1185. doi: 10.1007/s00192-008-0588-9. [DOI] [PubMed] [Google Scholar]
- 3.Chakrabarti I, De A, Pati S. Vaginal leiomyoma. J -Life Health. 2011;2:42–43. doi: 10.4103/0976-7800.83274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sim CH, Lee JH, Kwak JS, Song SH. Necrotizing ruptured vaginal leiomyoma mimicking a malignant neoplasm. Obstet Gynecol Sci. 2014;57:560–563. doi: 10.5468/ogs.2014.57.6.560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wu Y, Wang W, Sheng X, Kong L, Qi J. A misdiagnosed vaginal leiomyoma: case report. Urol Case Rep. 2015;3:82–83. doi: 10.1016/j.eucr.2015.02.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Khan AT, Shehmar M, Gupta JK. Uterine fibroids: current perspectives. Int J Women's Health. 2014;6:95–114. doi: 10.2147/IJWH.S51083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Vilos GA, Allaire C, Laberge P-Y, Leyland N, Vilos AG, Murji A, et al. The management of uterine leiomyomas. J Obstet Gynaecol Can. 2015;37:157–178. doi: 10.1016/S1701-2163(15)30338-8. [DOI] [PubMed] [Google Scholar]
- 8.Laughlin SK, Stewart EA. Uterine leiomyomas: individualizing the approach to a heterogeneous condition. Obstet Gynecol. 2011;117(2 Pt 1):396. doi: 10.1097/AOG.0b013e31820780e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Shimada K, Ohashi I, Shibuya H, Tanabe F, Akashi T. MR imaging of an atypical vaginal leiomyoma. Am J Roentgenol. 2002;178:752–754. doi: 10.2214/ajr.178.3.1780752. [DOI] [PubMed] [Google Scholar]
- 10.Asnani M, Srivastava K, Gupta HP, Kunwar S, Srivastava AN. A rare case of giant vaginal fibromyoma. Intractable Rare Dis Res. 2016;5:44–46. doi: 10.5582/irdr.2015.01037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Babacan A, Kizilaslan C, Gun I, Muhcu M, Mungen E, Atay V. CA 125 and other tumor markers in uterine leiomyomas and their association with lesion characteristics. Int J Clin Exp Med. 2014;7:1078–1083. [PMC free article] [PubMed] [Google Scholar]
- 12.Song K, Yu X, Lv T, Chen Y, Diao Y, Liu S, et al. Expression and prognostic value of lactate dehydrogenase-A and -D subunits in human uterine myoma and uterine sarcoma. Medicine (Baltimore). 2018;97. 10.1097/MD.0000000000010268. [DOI] [PMC free article] [PubMed]
- 13.Mollo A, Raffone A, Travaglino A, Di Cello A, Saccone G, Zullo F, et al. Increased LDH5/LDH1 ratio in preoperative diagnosis of uterine sarcoma with inconclusive MRI and LDH total activity but suggestive CT scan: a case report. BMC Womens Health. 2018;18. 10.1186/s12905-018-0662-5. [DOI] [PMC free article] [PubMed]
- 14.Shadbolt CL, Coakley FV, Qayyum A, Donat SM. MRI of vaginal leiomyomas. J Comput Assist Tomogr. 2001;25:355–357. doi: 10.1097/00004728-200105000-00005. [DOI] [PubMed] [Google Scholar]
- 15.Sherer DM, Cheung W, Gorelick C, Lee Y-C, Serur E, Zinn HL, et al. Sonographic and magnetic resonance imaging findings of an isolated vaginal leiomyoma. J Ultrasound Med Off J Am Inst Ultrasound Med. 2007;26:1453. doi: 10.7863/jum.2007.26.10.1453. [DOI] [PubMed] [Google Scholar]
- 16.Chin H, Ong XH, Yam PKL, Chern BSM. Extrauterine fibroids: a diagnostic challenge and a long-term battle. Case Rep. 2014;2014:bcr2014204928. doi: 10.1136/bcr-2014-204928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Brady A, Laoide RÓ, McCarthy P, McDermott R. Discrepancy and error in radiology: concepts, causes and consequences. Ulster Med J. 2012;81:3. [PMC free article] [PubMed] [Google Scholar]
- 18.Berlin L. Radiologic errors and malpractice: a blurry distinction. Am J Roentgenol. 2007;189:517–522. doi: 10.2214/AJR.07.2209. [DOI] [PubMed] [Google Scholar]
- 19.Pinto A, Brunese L. Spectrum of diagnostic errors in radiology. World J Radiol. 2010;2:377. doi: 10.4329/wjr.v2.i10.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pinto A, Pinto F, Faggian A, Rubini G, Caranci F, Macarini L, et al. Sources of error in emergency ultrasonography. Crit Ultrasound J. 2013;5:S1. doi: 10.1186/2036-7902-5-S1-S1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yarandi F, Eftekhar Z, Izadi-Mood N, Shojaei H. Accuracy of intraoperative frozen section in the diagnosis of ovarian tumors. Aust N Z J Obstet Gynaecol. 2008;48:438–441. doi: 10.1111/j.1479-828X.2008.00873.x. [DOI] [PubMed] [Google Scholar]
- 22.Sheyn I, Mira JL, Blanco R, Walton MB, Husseinzadeh N. Concomitant well-differentiated adenocarcinoma and leiomyosarcoma of the uterus. Arch Pathol Lab Med. 2000;124:1539–1541. doi: 10.5858/2000-124-1539-CWDAAL. [DOI] [PubMed] [Google Scholar]
- 23.Wehbe GS, Doughane M, Bitar R, Sleiman Z. Laparoscopic posterior Colpotomy for a Cervico-vaginal leiomyoma: hymen conservative technique. Facts Views Vis ObGyn. 2016;8:169. [PMC free article] [PubMed] [Google Scholar]
- 24.Egbe TO, Egbe TO. Prevalence and Outcome of Hysterectomy at the Douala General Hospital, Cameroon: A Cross-Sectional Study. Doi: 10.23937/2378-3397/1410092.
- 25.Hawkins Y, Ussher J, Gilbert E, Perz J, Sandoval M, Sundquist K. Changes in sexuality and intimacy after the diagnosis and treatment of cancer: the experience of partners in a sexual relationship with a person with cancer. Cancer Nurs. 2009;32:271–280. doi: 10.1097/NCC.0b013e31819b5a93. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.