

Sir,
We read with interest the report by Garekar et al.[1] We congratulate the authors for using surface-rendered virtual three-dimensional (3D) heart model for surgical planning without physically printing the model. Any effort to save cost is commendable. The expenditure, however, is not only from the printing of the 3D model but also from the need for specialized software. As highlighted by the authors, the conversion of a volumetric dataset to a virtual 3D model requires advanced software and coordination among various experts. The requirement of such expensive software limits the use of 3D printing in clinical practice. A similar virtual 3D heart model can also be created using open-source software but mandates navigation through a nondedicated cumbersome workflow.
Virtual dissection, a modification of volume rendering, is yet another technique for the creation and visualization of virtual cardiac models.[2] Although computationally more complex compared to surface rendering, it is possible to achieve good-quality volume rendering even on a personal computer. We recently proposed a low-cost technique of virtual dissection using open-source software.[3] This technique can be easily performed on a Macintosh personal computer and provides excellent visualization of cardiac morphology.[3,4,5] The surface rendering utilizes only a portion of the dataset, while virtual dissection incorporates the whole of the dataset and produces high fidelity 3D cardiac model.[3] Real-time rotation and cropping of the virtual volume in Horos software permit visualization in clinically relevant views, making it a perfect tool for assessment of cardiac morphology for presurgical planning [Figure 1]. In contrast, virtual models created for 3D print can only be visualized in predefined slices of the heart limiting its potential in complete delineation of cardiac morphology.[1]
Figure 1.
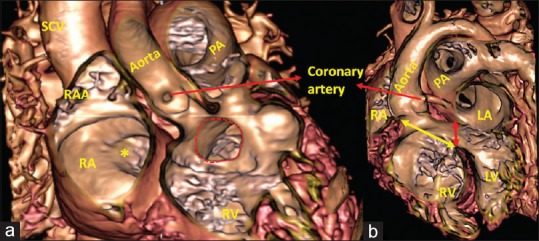
Virtual dissection from a 20-month-old child with double outlet right ventricle in anteroposterior (a) and left anterior oblique (b) projection. The interventricular communication (red dotted circle and double-headed red arrow) is located in the subaortic region. The relationship with the inflow and the outflow of the right ventricle confirms that the aorta can be committed to the left ventricle by simply placing a patch (double-headed yellow arrow). All other details including the fossa ovalis (*), ostium of the coronary artery, and right ventricular outflow are also well illustrated. LA: Left atrium, LV: Left ventricle, PA: Pulmonary trunk, RA: Right atrium, RAA: Right atrial appendage, RV: Right ventricle, SCV: Superior caval vein
We believe that a 3D model derived from Horos-based virtual dissection is a better alternative to a virtual 3D model obtained from surface rendering with the added advantage of saving cost.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Garekar S, Bharati A, Kothari F, Patil S, Dhake S, Mali S, et al. Virtual three-dimensional model for preoperative planning in a complex case of a double outlet right ventricle. Ann Pediatr Cardiol. 2019;12:295–7. doi: 10.4103/apc.APC_141_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mori S, Fukuzawa K, Takaya T, Takamine S, Ito T, Fujiwara S, et al. Clinical cardiac structural anatomy reconstructed within the cardiac contour using multidetector-row computed tomography: Atrial septum and ventricular septum. Clin Anat. 2016;29:342–52. doi: 10.1002/ca.22546. [DOI] [PubMed] [Google Scholar]
- 3.Gupta SK, Spicer DE, Anderson RH. A new low-cost method of virtual cardiac dissection of computed tomographic datasets. Ann Pediatr Cardiol. 2019;12:110–6. doi: 10.4103/apc.APC_167_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Talwar S, Siddharth B, Gupta SK, Bhoje A, Choudhary SK. Surgical repair for common arterial trunk with pulmonary dominance, hypoplasia of ascending aorta, and interrupted aortic arch. Ann Pediatr Cardiol. 2019;12:287–91. doi: 10.4103/apc.APC_147_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gupta SK, Aggarwal A, Shaw M, Gulati GS, Ramakrishnan S, Saxena A, et al. Clarifying the anatomy of common arterial trunk – A clinical study of 70 patients. Eur Heart J Cardiovasc Imaging. 2019 doi: 10.1093/ehjci/jez255. doi: 101093/ehjci/jez255 [Epub ahead of print] [DOI] [PubMed] [Google Scholar]