

Abstract
Unguarding of an atrioventricular valvar orifice is a rare form of congenital heart disease that requires staged functionally univentricular palliation. Unguarding of the mitral valvar orifice has previously been reported in the setting of mirror-imaged atrial arrangement. We report a neonate with unguarding of the mitral valvar orifice in the setting of usual atrial arrangement, but with discordant atrioventricular connections and pulmonary atresia.
Keywords: Atrioventricular discordance, mitral incompetence, pulmonary atresia
INTRODUCTION
Unguarded atrioventricular valve orifices are rare congenital cardiac malformations. In this regard, unguarding of the tricuspid orifice has been reported with some degree of frequency.[1] Unguarding of the mitral valve orifice, in contrast, is less common. Of reported cases, all bar one of which we are aware have featured mirror-imaged atrial arrangement with discordant atrioventricular connections and pulmonary atresia.[2,3,4,5] We have now encountered similar findings, however, in the setting of usual atrial arrangement.
CASE REPORT
A 22-year-old female in her first pregnancy was referred for fetal echocardiography at 30 weeks of gestation. The fetal echocardiogram revealed discordant atrioventricular connections with pulmonary atresia and a small ventricular septal defect. Delivery at a cardiac center was recommended. The baby was born by normal vaginal delivery at term and weighed 2.46 kg. The perinatal period was uneventful. The saturation of oxygen in room air was 86%. The cardiac impulse was palpable in the right hemithorax, the second heart sound was single, and a continuous murmur was heard in the infraclavicular region. On the frontal chest radiograph, the heart was noted to occupy the right hemithorax [Figure 1]. The stomach bubble was visible on the left, with the liver shadow on the right side. The electrocardiogram was consistent with usual atrial arrangement.
Figure 1.

Chest radiograph in the anteroposterior projection. The stomach is seen to the spine and the liver to the right suggesting normal abdominal organ arrangement. The cardiac silhouette lies in the right hemithorax with cardiomegaly. The pulmonary blood flow appears attenuated
A detailed echocardiogram was obtained postnatally. The abdominal aorta was present to the left of the spine, with the inferior caval vein to the right. The heart was right sided, with the apex pointing to the right. The systemic veins drained into the right-sided atrium, while all four pulmonary veins drained into the left-sided atrium. The atrioventricular connections were discordant. The left-sided tricuspid valve was morphologically normal and competent, and the left-sided morphologically right ventricle showed normal systolic function. It gave rise to both arterial roots, but with pulmonary atresia [Figure 2a]. Thus, the aorta arose anteriorly and to the left of the atretic pulmonary trunk, which was aligned with the cavity of the morphologically right ventricle. The pulmonary root was small but well formed. The aortic outflow tract was unobstructed. Confluent but mildly hypoplastic pulmonary arteries were supplied by a vertical and tortuous persistent arterial duct, which originated from the underside of the aortic arch. The right-sided atrioventricular junction was dilated. Neither leaflet tissue nor chordal tissue was demonstrable within the right-sided morphologically left ventricle [Figure 2b]. Doppler examination at the atrioventricular junction revealed to-and-fro flow at low velocity [Figure 2c]. The free wall of the ventricle was thin, contracting poorly, and the ventricular septum was now seen to be intact. The final diagnosis was unguarded mitral orifice in the setting of usual atrial arrangement, discordant atrioventricular connections, and double-outlet right ventricle with pulmonary atresia. We proposed a staged functionally univentricular strategy for palliation. The parents, however, declined consent for an intervention, and hence, only palliative care was provided. Consent for postmortem was not provided.
Figure 2.
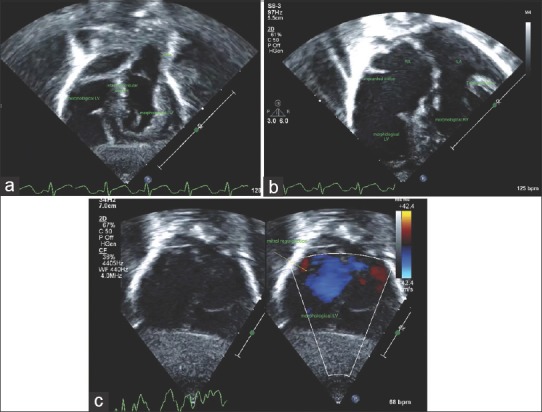
(a) Echocardiogram image from the subcostal position. The morphological right ventricle is on the left side and gives rise to the aorta. The interventricular septum appears intact and the morphological left ventricle appears thin walled. (b) Echocardiogram image from the four-chamber view. There are discordant atrioventricular connections. There is unguarding of the mitral valve orifice and a thin-walled left ventricle, (c) Echocardiogram with color Doppler from the subcostal view showing unguarding of the mitral orifice with severe regurgitation
DISCUSSION
Unguarding of an atrioventricular orifice is a rare congenital anomaly. It has most commonly been reported involving the tricuspid valve in the setting of pulmonary atresia with an intact ventricular septum. Both partial and complete forms have been described. They are differentiated from Ebstein's malformation by the absence of any valvar leaflet tissue within the right ventricle.[6] The leaflets of the atrioventricular valves develop by undermining of the ventricular myocardium, with this process being deficient when the atrioventricular junction remains unguarded. Pathogenesis has yet to be elucidated although there is some evidence supporting apoptosis as playing a key role.[7] A primary mesenchymal abnormality has also been postulated.[2]
The few cases of unguarding of the mitral valve orifice reported in the English literature have all involved mirror-imaged arrangement of both the organs and the atrial chambers, in other words so-called “situs inversus.” All cases but one have also involved discordant connections across the atrioventricular junctions, with double-outlet right ventricle, but no egress from the morphologically left ventricle apart from a small interventricular communication in two instances. In the only reported case of which we are aware with usual atrial arrangement, there was aortic atresia. All reported cases also had a thin-walled and poorly contractile morphologically left ventricle. These findings could be interpreted as supporting the concept of a primary mesenchymal abnormality, resulting in the failure of formation of the leaflets of the atrioventricular valve, as well as poor ventricular function. Our neonate shows comparable findings, however, in the setting of usual atrial arrangement. This suggests that the disorder is genetically unrelated to abnormalities in the development of the left–right axis. It also raises the possibility of an entirely hemodynamic mechanism, relating to outflow obstruction, ventricular dysfunction, and severe regurgitation of the atrioventricular valves in the early gestational period. Evidence in support of such a progression would require serial ultrasound evaluation from early in gestation or access to relevant animal models. It is of note, therefore, that similar morphology has not been described in fetal animal models of aortic stenosis.[8]
Management should be on the lines of functionally univentricular palliation. In our child, the first stage would have been creation of a systemic-to-pulmonary arterial shunt or stenting of the persistently patent arterial duct. As the morphologically right ventricle would remain the systemic ventricle, the long-term prognosis would be more guarded than in other forms of functionally univentricular heart, such as tricuspid atresia or double-inlet left ventricle.[9] In this regard, three of the five patients thus far described did not survive, while one other child developed severe ventricular dysfunction. These previous experiences were a key factor in the decision of the parents not to pursue active treatment.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Kaneko Y, Takeda T, Yoda H, Kobayashi J, Takada N, Tsuchiya K, et al. Right ventricular plication in a neonate with an unguarded tricuspid valvar orifice. Ann Thorac Surg. 2009;87:305–7. doi: 10.1016/j.athoracsur.2008.06.017. [DOI] [PubMed] [Google Scholar]
- 2.Yasukochi S, Satomi G, Park I, Ando M, Momma K. Unguarded mitral orifice, mirror-imaged atrial arrangement, and discordant atrioventricular connections. Cardiol Young. 1999;9:478–83. doi: 10.1017/s1047951100005382. [DOI] [PubMed] [Google Scholar]
- 3.Earing MG, Edwards WD, Puga FJ, Cabalka AK. Unguarded mitral orifice associated with discordant atrioventricular connection, double-outlet right ventricle, and pulmonary atresia. Pediatr Cardiol. 2003;24:490–2. doi: 10.1007/s00246-002-0389-8. [DOI] [PubMed] [Google Scholar]
- 4.Hwang MS, Chang YS, Chu JJ, Lin WS, Su WJ. A potential new constellation of defects: Unguarded mitral orifice associated with double-outlet right ventricle {I, D, D} and pulmonary atresia/stenosis. Int J Cardiol. 2011;148:354–7. doi: 10.1016/j.ijcard.2010.06.004. [DOI] [PubMed] [Google Scholar]
- 5.Kishi K, Katayama H, Ozaki N, Odanaka Y, Masuda M, Nemoto S, et al. Fatal cardiac anomaly of unguarded mitral orifice with asplenia syndrome. J Cardiol Cases. 2017;15:6–9. doi: 10.1016/j.jccase.2016.09.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Anderson RH, Silverman NH, Zuberbuhler JR. Congenitally unguarded tricuspid orifice: Its differentiation from Ebstein's malformation in association with pulmonary atresia and intact ventricular septum. Pediatr Cardiol. 1990;11:86–90. doi: 10.1007/BF02239568. [DOI] [PubMed] [Google Scholar]
- 7.James TN, Nichols MM, Sapire DW, DiPatre PL, Lopez SM. Complete heart block and fatal right ventricular failure in an infant. Circulation. 1996;93:1588–600. doi: 10.1161/01.cir.93.8.1588. [DOI] [PubMed] [Google Scholar]
- 8.Eghtesady P, Michelfelder E, Altaye M, Ballard E, Hirsh R, Beekman RH., 3rd Revisiting animal models of aortic stenosis in the early gestation fetus. Ann Thorac Surg. 2007;83:631–9. doi: 10.1016/j.athoracsur.2006.09.043. [DOI] [PubMed] [Google Scholar]
- 9.d'Udekem Y, Xu MY, Galati JC, Lu S, Iyengar AJ, Konstantinov IE, et al. Predictors of survival after single-ventricle palliation: The impact of right ventricular dominance. J Am Coll Cardiol. 2012;59:1178–85. doi: 10.1016/j.jacc.2011.11.049. [DOI] [PubMed] [Google Scholar]