

Abstract
Background
Neonatal sepsis is accounted for 30–50% of annual neonatal deaths in developing countries. We performed a systematic review and meta-analysis study to evaluate the national prevalence and identification of the etiological pathogens of neonatal sepsis in Iran.
Methods
A comprehensive literature search was done on the national and international databases for studies published between 2000 and 2019. The DerSimonian and Laird random-effects model was used to calculate pooled prevalence estimates, with 95% confidence intervals (CIs). Subgroup analyses and meta-regressions regarding the gender, type of sepsis and time during were also performed. Data were extracted, analyzed, and presented according to PRISMA guideline.
Results
Of 944 publications identified, 22 studies containing 14,683 neonates met the eligibility criteria. The pooled national prevalence of sepsis in Iran was 15.98% (95%CI, 11.96–20.46%; 1,367/14,683). Prevalence rate in boys (20.42%; 95%CI, 9.03–34.8%) was slightly higher than girls (18.5%; 95%CI, 7.4–32.8). A decreasing trend in prevalence of neonatal sepsis was found in recent years, although not statistically significant (c = -0.005; P value = 0.4). The most prevalent causative bacterial pathogens were Enterobacter spp. (23.04%), followed by Klebsiella pneumoniae (17.54%), coagulase-negative Staphylococci (14.06%), Escherichia coli (13.92%), Pseudomonas aeruginosa (12.67%), and Staphylococcus aureus (11.48%).
Conclusion
Our findings showed a high prevalence of neonatal sepsis in suspected neonates, suggesting the need to implement preventive measures, routine assessment, and close monitoring of neonates. Also, Enterobacter spp. and Klebsiella pneumoniae were identified as the principal bacterial pathogens responsible for neonatal septicemia in Iran.
Introduction
Sepsis is a serious cause of morbidity and mortality among neonates, killing approximately 3 million newborns each year [1]. The global burden of neonatal sepsis was measured as 2,202 per 100,000 live births [2]. Sepsis is a potentially life-threatening condition resulting from an extreme systemic immune response of the body to fight against an infection. This invasive infection, frequently bacterial, characterized by systemic signs of infection and isolation of bacteria from the bloodstream. Sepsis is one of the most important reasons for hospitalization of newborns in neonatal intensive care units (NICUs). Studies showed that neonatal sepsis is fatal and may quickly lead to septic shock and death if it's left untreated [3]. The therapy is often associated with an incontinent increase in antibiotic administration leading to development of antibiotic resistance.
Neonatal sepsis is categorized into either an early-onset neonatal sepsis (EOS) or late-onset sepsis (LOS) [4]. EOS is defined by bacteremia or meningitis occurring in newborns less than 3-days old [5]. EOS could be vertically transmitted infection that usually occurs as an ascending infection from the mother's cervix. Group B Streptococcus (GBS) is the leading cause of EOS [6] followed by Escherichia coli (E. coli) and Listeria monocytogenes [7]. Prematurity or low birth weight, birth asphyxia, prolonged rupture of membranes, and traumatic delivery are the major risk factors that contribute to the incidence of EOS [8]. LOS is defined as sepsis in infants during 4–90 days of life and could be caused either by vertically or horizontally transmitted infections [9]. The most important microorganisms involved in LOS include coagulase-negative Staphylococci (CoNS), Enterobacter spp., Escherichia coli, Pseudomonas aeruginosa, Klebsiella pneumonia, Staphylococcus aureus and Candida albicans [9, 10]. Some main risk factors associated with LOS are prematurity, low birth weight, poor hand hygiene, central venous catheters and prolonged mechanical ventilation [11].
In the past few years several studies were performed in Iran regarding the prevalence of neonatal sepsis in, although most of them were focused to limited geographical areas. Here, we performed a comprehensive systematic review and meta-analysis study to assess the prevalence of neonatal sepsis and identify the causative pathogens of the infection in Iranian neonates.
Materials and methods
We used stepwise approach specified in the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines [12] to perform of this systematic review and meta-analysis (S1 Checklist).
Search strategy and selection criteria
Four major Iranian biomedical literature database servers (Iranmedex, Magiran, Irandoc and SID) and five international electronic databases (PubMed/MEDLINE, EMBASE, Scopus, Web of Science and Google Scholar) were searched for articles reporting the prevalence of sepsis in neonates and published between 2000 and 2019. The search terms utilized were “Iran”, “sepsis”, “septicaemia”, “bacteraemia”, “neonatal”, “neonate” and “neonates” (See S1 Text: Supplementary file for the details of the databases searches). We restricted the literature search to reports in English and Persian languages and human subjects. Bibliographies of the obtained studies and the relevant review articles were carefully evaluated to identify the studies that primarily cover the sepsis and its causative pathogens, but were not found in databases search. We only included observational original studies that had information on the prevalence of sepsis, reported data on the number of children with sepsis and the causative organisms, and neonatal sepsis cases diagnosed according to the standard guidelines (blood culture). Studies were excluded if they were done in adults, investigated only a single pathogen of sepsis, had sample sizes less than 50 cases, duplicate studies, reviews, letters, case-reports or case series without original data.
Data extraction and quality assessment
After duplicates removal and screening of titles and abstracts, the full text of eligible studies were reviewed in depth by two independent reviewers (Z.A.R, and S.E). Data were extracted from all the eligible studies and compiled in Microsoft Excel spreadsheets. Inconsistencies were resolved by discussion and consensus with a third reviewer (A.R.). The following information were extracted from each study: first author last name, year of publication, study period, sample size, number of infected children, and number of bacterial pathogens. The quality of the studies was determined using Newcastle-Ottawa scale. Each item was scored for a maximum of six scores. Publications which scored 0–2, 3, 4 and 5 were classified as “unsatisfactory”, “satisfactory”, “good” and “very good”, respectively.
Meta-analyses
The pooled prevalence of sepsis in Iranian neonates at a 95% confidence interval (CI) was estimated using the DerSimonian and Laird random-effects model (REM). The I2 statistic was used to assess the heterogeneity of the estimates. Subgroup analyses were performed according to the gender, type of sepsis (EOS and LOS) and time during. The pooled prevalence of each bacterial pathogen was also calculated using REM. Forest plots were used for showing of pooled prevalence rates by REM. We did not undertake an assessment of publication bias, as it is not relevant for the prevalence studies [13]. All analyses were performed using STATA v.13 (STATA Corp., College Station, Texas, USA). Statistical tests were significant if P value was <0.05.
Results
In the preliminary search, a total of 944 potentially relevant studies were identified through the search of the national and international databases, and 909 studies were excluded after duplicates removal and further review of titles and abstracts. Finally, 35 studies were reviewed in depth and 22 study papers [14–35] involving 14,683 neonates were found to be eligible for meta-analysis (Fig 1). The studies included in meta-analysis represented 12 different provinces covering all parts of the country. The province with the highest number of studies was Tehran (7/22). Five and seven studies had extractable data regarding the gender (including 847 boys and 664 girls) and type of sepsis (EOS and LOS). All studies used blood culture methods to detect sepsis, while information regarding the bacterial pathogens was reported in 19 studies. All these studies cover only the hospitalized neonates. Main characteristics of studies included are summarized in S1 File and Table 1.
Fig 1. PRISMA flowchart showing the search and study selection strategy.
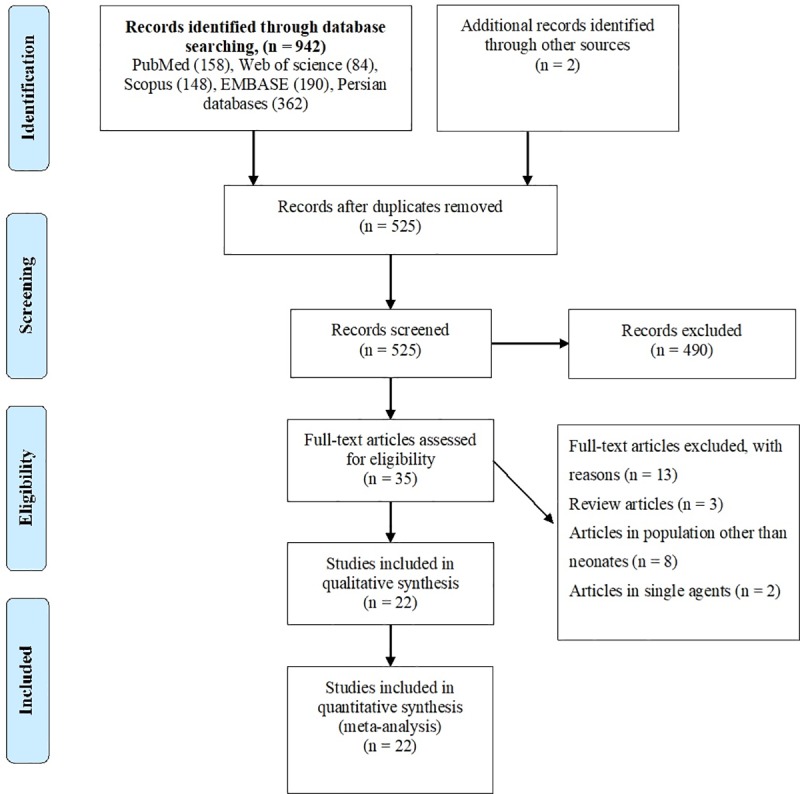
Table 1. Main characteristics studies reporting prevalence of neonatal sepsis in Iran.
| Authour | Publish year | Province | Number of neonates screened | Neonates with sepsis | Number of boys | Boys with sepsis | Number of girls | Girls with sepsis |
|---|---|---|---|---|---|---|---|---|
| Malakan Rad et al. [14] | 2004 | Isfahan | 453 | 136 | ND | ND | ND | ND |
| Fesharaki Nia et al. [15] | 2004 | South Khorasan | 67 | 6 | ND | ND | ND | ND |
| Khosravi et al.[16] | 2004 | Khozestan | 200 | 10 | 123 | 8 | 77 | 2 |
| Movahedian et al.[17] | 2006 | Isfahan | 1680 | 111 | ND | ND | ND | ND |
| Salamati et al.[18] | 2006 | Tehran | 52 | 11 | ND | ND | ND | ND |
| Milani et al.[19] | 2007 | Tehran | 104 | 31 | ND | ND | ND | ND |
| Nikavar et al. [20] | 2008 | Tehran | 240 | 56 | ND | ND | ND | ND |
| Ghorbani et al.[21] | 2009 | Guilan | 298 | 31 | ND | ND | ND | ND |
| Torkaman et al.[22] | 2009 | Tehran | 114 | 53 | ND | ND | ND | ND |
| Hashemizadeh et al.[23] | 2009 | Shiraz | 578 | 78 | ND | ND | ND | ND |
| Shahian et al. [24] | 2010 | Shiraz | 208 | 90 | 115 | 54 | 93 | 36 |
| Monsef et al.[25] | 2010 | Hamadan | 417 | 105 | 239 | 60 | 183 | 45 |
| Dezfouli Manesh et al.[26] | 2011 | Kermanshah | 2175 | 90 | ND | ND | ND | ND |
| Aletayeb et al. [27] | 2011 | Razavi Khorasan | 3700 | 153 | ND | ND | ND | ND |
| Adib et al.[28] | 2011 | Isfahan | 69 | 20 | ND | ND | ND | ND |
| Karambin et al.[29] | 2011 | Gilan | 611 | 64 | 331 | 37 | 280 | 27 |
| Besharati et al.[30] | 2011 | Khorasan | 100 | 7 | ND | ND | ND | ND |
| Mosayebi et al.[31] | 2013 | Tehran | 1126 | 104 | ND | ND | ND | ND |
| Ahmadi et al.[32] | 2014 | Khozestan | 405 | 55 | ND | ND | ND | ND |
| Sharifi Yazdi et al.[33] | 2014 | Tehran | 216 | 55 | ND | ND | ND | ND |
| Khosravi et al.[34] | 2017 | Tehran | 70 | 17 | 39 | 8 | 31 | 9 |
| Afsharpaiman et al.[35] | 2019 | Tehran | 1800 | 84 | ND | ND | ND | ND |
ND, not determined
Prevalence of sepsis among the studies was ranged from 4.14% (95% CI: 3.3–5.0%) in Kermanshah province in west of Iran to 46.49% (95% CI: 37.1–56.0%) in Tehran province in central part of Iran. The pooled national prevalence of sepsis in Iranian neonates (from 22 studies including 14,683 neonates) was 15.98% (95%CI, 11.96–20.46%; 1,367/14,683). Heterogeneity among studies was substantial (I2 = 97.7%, P < 0.001) (Fig 2). In a subgroup analysis with regards to type of sepsis, the pooled prevalence EOS and LOS were 10.96% (95%CI, 5.93–17.26%) and 6.85% (95%CI, 3.41–11.32%), respectively (Table 2, S1 Fig). With respect to gender, the pooled prevalence in boys (20.42%; 95%CI, 9.03–34.8%) was slightly higher than girls (18.5%; 95%CI, 7.4–32.8%), showing a trend that is not statistically significant (P value = 0.75) (Table 2, S2 Fig). Moreover subgroup analysis and meta-regression analyses showed a statistically non-significant but a decreasing trend in the prevalence of neonatal sepsis in recent years (c = -0.005; P value = 0.4; Table 2, S3 Fig and Fig 3).
Fig 2. Forest plot of the prevalence of neonatal sepsis in Iran.

ES: estimated prevalence.
Table 2. Prevalence of neonatal sepsis in Iran according to a priori defined stubgroups.
| Variable/subgroups | Number studies | Number of neonates screened (total) | Number of neonates with proved sepsis | Pooled Prevalence (95% CI) |
Heterogeneity I2 (%) |
|---|---|---|---|---|---|
| Gender | |||||
| Boy | 5 | 847 | 167 | 20.42 (9.03–34.83) | 95.0 |
| Girl | 5 | 664 | 119 | 18.51 (7.46–32.89) | 93.7 |
| Type of sepsis | |||||
| Early onset sepsis | 7 | 8025 | 411 | 10.96 (5.93–17.26) | 98.0 |
| Late onset sepsis | 7 | 8025 | 216 | 6.85 (3.41–11.32) | 97.3 |
| Year | |||||
| 2004–2008 | 7 | 2796 | 361 | 16.46 (7.73–27.58) | 97.1 |
| 2009–2012 | 11 | 9396 | 795 | 15.97 (10.31–22.57) | 98.1 |
| 2013–2019 | 4 | 2491 | 211 | 15.50 (5.80–28.66) | 97.3 |
Fig 3. Meta-regression analysis of the prevalence of neonatal sepsis in Iran according to implementation years of screening showing a statistically non-significant decreasing trend in prevalence in recent years (c = -0.005; P value = 0.4).

Among the bacterial pathogens causing the neonatal sepsis, our results indicated that the most prevalent causative pathogens belong to Enterobacter spp. (23.4%; 95%CI, 10.9–37.6%), followed by Klebsiella pneumoniae (17.5%; 95%CI, 9.7–26.8%), coagulase-negative Staphylococci (14.0%; 95%CI,8.9–19.9%), Escherichia coli (13.9%; 95%CI, 5.6–24.6%), Pseudomonas aeruginosa (12.6%; 95%CI, 5.3–22.1%), and Staphylococcus aureus (11.4%; 95%CI, 6.0–18.2%). Other minor bacterial pathogens were shown in Fig 4.
Fig 4. Forest Plot of the prevalence of each bacterial pathogens causing neonatal sepsis.

Discussion
Neonatal sepsis continues to be a major health issue worldwide. A recent recommendation by World Health Organization (WHO) listed it as a life-threatening infection and a key healthcare priority for the coming decades [36, 37]. Therefore, studies that estimate the national and global prevalence data could be very useful to prioritize the control measures for this preventable disease. In this study, we report a country-level estimate of neonatal sepsis in Iran. Our estimates showed that the prevalence of sepsis in Iranian neonates is about 16%, with high variability in different provinces. The prevalence estimates were limited to hospitalized neonates and do not cover the entire population. Prevalence rate estimated in Iran is lower than those reported from Egypt (44%) [38], Tanzania (39%) [39], Cameroon (37%) [40], and higher than those reported from Oman (3.5%) [41], USA (5.16 per 1,000) [42], and Australia (0.5 per 1,1000) [43]. Also, the prevalence of sepsis in other studies from Nepal and India was reported 36% and 46.8%, respectively [44, 45]. These geographical variation could be attributed to preventive strategies adopted in each country, clinical criteria for sepsis diagnosis, differential sensitivity and specificity of the culture methods in different laboratories, health status of mothers during pregnancy, sanitary status in delivery section, and social-economic status in different countries [46, 47].
In consistent with previous studies in some parts of the world [38, 41, 42, 48], we found that prevalence of neonatal sepsis in boys is higher than girls. It is assumed that variation in genetic factors especially genes located in chromosome X may be responsible for these gender based differences [49]. In meta-regression analysis we have found a statistically non-significant but a decreasing trend in the prevalence of neonatal sepsis in recent years. This could be due to sustainable improvement of the sanitary conditions and efforts undertaken to improve mother and child health in Iran during last years [50, 51].
With respect to the causative pathogens of neonatal sepsis, our study indicated that Enterobacter spp. (23.0%) and Klebsiella pneumoniae (17.4%) were the most common organisms responsible for neonatal sepsis. Another large systematic review on causative pathogens of community-acquired neonatal sepsis in low- and middle-income countries demonstrated the most prevalent bacterial pathogens for neonatal sepsis as S. aureus (14.9%), E. coli (12.2%), and Klebsiella species (11.6%). However, these pattern were varied between different regions, as S. aureus and Streptococcus pneumoniae were most prevalent in Africa; Klebsiella in South-East Asia; S. aureus and Klebsiella pneumoniae in Europe and Western Pacific regions, and finally Staphylococcus aureus and Haemophilus influenzae in Americas region [52]. Moreover in consistent with our findings, results from another large systematic review indicated that Enterobacter species, Klebsiella, Escherichia coli, Pseudomonas species, and Streptococcus pneumonia were recognized as the most common bacterial pathogens of neonatal sepsis in the Middle East region [52]. In a country-level meta-analysis in China, Li et al reported that Staphylococcus, Enterococcus, Escherichia, and Klebsiella were found to be the most common organisms responsible for neonatal septicaemia in China [53]. This variation could also be explained by differences in geographical and climatic parameters in different regions.
The current study had some limitations that need to be considered when interpreting the results of this work. First, the majority of studies included were published in local journals and may have resulted in a publication bias. Second, although we have performed a comprehensive literature search, data from several provinces were limited, therefore the same estimates cannot be guaranteed from further studies that include these regions in the future. Third, we could not perform a detailed sub-group analyses other than what was presented in the manuscript, because the majority of studies included in the meta-analysis did not classify the neonatal sepsis cases based on type of delivery, birth weight and community-onset/hospital-associated infections. Forth, our meta-analysis demonstrated a substantial heterogeneity of neonatal sepsis prevalence across studies, thus making it difficult for a direct comparison. Nevertheless, our study performed on a large sample size and a rigorous methodology provides useful information for national authorities to prioritize prevention efforts and intervention programs to reduce the burden of neonatal sepsis in Iran. Our finding showed that about 16% of newborn infants hospitalized in Iran had sepsis, a statistic that is higher than those reported from developed countries. This high rate of neonatal sepsis can lead to several neonatal death annually, and call for further measures and interventions to control and prevent sepsis in Iranian neonates.
Supporting information
(DOCX)
(TIF)
(TIF)
(TIF)
(DOCX)
(XLSX)
Data Availability
All relevant data are within the manuscript and its Supporting Information files.
Funding Statement
The author(s) received no specific funding for this work.
References
- 1.Mersha A, Worku T, Shibiru S, Bante A, Molla A, Seifu G, et al. Neonatal sepsis and associated factors among newborns in hospitals of Wolaita Sodo Town, Southern Ethiopia. Res Rep Neonatol. 2019;9:1 10.2147/RRN.S193074. [DOI] [Google Scholar]
- 2.Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, Schlapbach LJ, Reinhart K, Kissoon N. The global burden of paediatric and neonatal sepsis: a systematic review. The Lancet Respir Med. 2018;6(3):223–30. Epub 2018/03/07. 10.1016/S2213-2600(18)30063-8 . [DOI] [PubMed] [Google Scholar]
- 3.Shah BA, Padbury JF. Neonatal sepsis: an old problem with new insights. Virulence. 2014;5(1):170–8. Epub 2013/11/01. 10.4161/viru.26906 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Vergnano S, Sharland M, Kazembe P, Mwansambo C, Heath P. Neonatal sepsis: an international perspective. Arch Dis Child Fetal Neonatal Ed. 2005;90(3):220–4. 10.1136/adc.2002.022863 ; PMCID: PMC1721871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Giannoni E, Agyeman PKA, Stocker M, Posfay-Barbe KM, Heininger U, Spycher BD, et al. Neonatal Sepsis of Early Onset, and Hospital-Acquired and Community-Acquired Late Onset: A Prospective Population-Based Cohort Study. J Pediatr. 2018;201:106–14.e4. 10.1016/j.jpeds.2018.05.048 [DOI] [PubMed] [Google Scholar]
- 6.Koenig JM, Keenan WJ. Group B streptococcus and early-onset sepsis in the era of maternal prophylaxis. Pediatr Clin North Am. 2009;56(3):689–708. 10.1016/j.pcl.2009.04.003 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Simonsen KA, Anderson-Berry AL, Delair SF, Davies HD. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014;27(1):21–47. 10.1128/CMR.00031-13 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chacko B, Sohi I. Early onset neonatal sepsis. Indian J Pediatr. 2005;72(1):23–6. 10.1007/bf02760574 . [DOI] [PubMed] [Google Scholar]
- 9.Dong Y, Speer CP. Late-onset neonatal sepsis: recent developments. Arch Dis Child Fetal Neonatal Ed. 2015;100(3):257–63. 10.1136/archdischild-2014-306213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yadav NS, Sharma S, Chaudhary DK, Panthi P, Pokhrel P, Shrestha A, et al. Bacteriological profile of neonatal sepsis and antibiotic susceptibility pattern of isolates admitted at Kanti Children's Hospital, Kathmandu, Nepal. BMC Res Notes. 2018;11(1):301 10.1186/s13104-018-3394-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Freitas FTM, Araujo AFOL, Melo MIS, Romero GAS. Late-onset sepsis and mortality among neonates in a Brazilian Intensive Care Unit: a cohort study and survival analysis. Epidemiol Infect. 2019;147:e208 10.1017/S095026881900092X . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4(1):1 10.1186/2046-4053-4-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hunter JP, Saratzis A, Sutton AJ, Boucher RH, Sayers RD, Bown MJ. In meta-analyses of proportion studies, funnel plots were found to be an inaccurate method of assessing publication bias. J Clin Epidemiol. 2014;67(8):897–903. 10.1016/j.jclinepi.2014.03.003 . [DOI] [PubMed] [Google Scholar]
- 14.Rad EM, Momtazmanesh N. Neonatal sepsis due to klebsiella: frequency, outcome and antibiotic sensitivity. Iranian J Public Health. 2004:43–8. [Google Scholar]
- 15.Fesharaki Nia, Miri M. The investigation of newborn septicemia in Valiy-e-Aser Hospital of Birjand. J Birjand Univ Med Sci. 2004; 11(4):9–15 [Google Scholar]
- 16.Khosravi A, Najafabadi Farahani M. Neonatal septicemia caused by aerobic bacteria in newborn infants. J Qazvin Univ Med Sci. 2004;8(2):35–40. [Google Scholar]
- 17.Movahedian A, Moniri R, Mosayebi Z. Bacterial culture of neonatal sepsis. Iranian J Public Health. 2006:84–9. [Google Scholar]
- 18.Salamati P, Rahbarimanesh AA, Yunesian M, Naseri M. Neonatal nosocomial infections in Bahrami children hospital. Indian J Pediatr. 2006;73(3):197–200. 10.1007/bf02825479 . [DOI] [PubMed] [Google Scholar]
- 19.Milani S. Clinical Manifestations and mortality in neonatal septicemia Children Medical Center. Tehran Univ Med J. 2008;65(2):46–51. [Google Scholar]
- 20.Nickavar A, Nateghian A, Setarehshenas R, Sajadi A. Bacteriologic study of blood culture in children and neonates with bacterimia and septicemia. Iran J Nursing. 2007;20(52):87–94. [Google Scholar]
- 21.Ghorbani MG, Karam bin MM, Sobhani AR, Fasihi M, Parandakh Joshari S, Shahrami H. Comparison of Neonatal Bacterial Septicemia in 2007 and 1998–2000 Years. J Guilan Univ Med Sci. 2009;18(69):25–32. [Google Scholar]
- 22.Torkaman M, Afsharpaiman S, Hoseini M, Moradi M, Mazraati A, Amirsalari S, et al. Platelet count and neonatal sepsis: a high prevalence of Enterobacter spp. Singapore Med J. 2009;50(5):482–5. [PubMed] [Google Scholar]
- 23.Hashemizadeh Z, Bazargani A, Davarpanah MA. Blood culture contamination in a neonatal intensive care unit in Shiraz, Southwest-Central Iran. Med Princ Pract. 2011;20(2):133–6. 10.1159/000321237 . [DOI] [PubMed] [Google Scholar]
- 24.Shahian M, Pishva N, Kalani M. Bacterial etiology and antibiotic sensitivity patterns of early-late onset neonatal sepsis among newborns in Shiraz, Iran 2004–2007. Iranian J Med Sci. 2010;35(4):293–8. [Google Scholar]
- 25.Monsef A, Eghbalian F. Antibiotic sensitivity pattern of common bacterial pathogens in NICU and neonatal ward in Hamedan province of Iran. Health. 2010;2(06):625. [Google Scholar]
- 26.Dezfoulimanesh Z, Tohidnia MR, Darabi F, Almasi A. Prevalence of bacterial and antibiotic sensitivity in septicemia of neonates admitted to Kermanshah Imam Reza Hospital (2007–2008). J Kermanshah Univ Med Sci. 2011;15(2):e79381. [Google Scholar]
- 27.Aletayeb SMH, Khosravi AD, Dehdashtian M, Kompani F, Aramesh MR. Identification of bacterial agents and antimicrobial susceptibility of neonatal sepsis: A 54-month study in a tertiary hospital. Afr J Microbiol Res. 2011;5(5):528–31. [Google Scholar]
- 28.Adib M, Bakhshiani Z, Navaei F, Fosoul FS, Fouladi S, Kazemzadeh H. Procalcitonin: a reliable marker for the diagnosis of neonatal sepsis. Iranian J Basic Med Sci. 2012;15(2):777–82. ; PMCID: PMC3586883 [PMC free article] [PubMed] [Google Scholar]
- 29.Karambin M, Zarkesh M. Enterobacter, the most common pathogen of neonatal septicemia in Rasht, Iran. Iranian J Pediatr. 2011;21(1):83–7. ; PMCID: PMC3446115 [PMC free article] [PubMed] [Google Scholar]
- 30.Besharati R, Sadeghian A, Mamori G. Abundance of colonized bacteria as causative agent of septicemia in neonates hospitalized in the N.I.C.U Ward at Ghaem hospital in Mashhad. J North Khorasan Univ Med Sci. 2011;3(1):35–8. 10.29252/jnkums.3.1.5. [DOI] [Google Scholar]
- 31.Mosayebi Z, Movahedian AH, Soori T. Clinical and bacteriological characteristics of neonatal sepsis in an inten-sive care unit in Kashan, Iran: a 2 year descriptive study. Arch Pediatr Infect Dis. 2013;1(2):62. [Google Scholar]
- 32.Ahmadi K, Farajzadeh Sheikh A, Mardaneh J, Modarresi F, Shoja S. Detection of Enterobacter sakazakii in neonatal sepsis by PCR on 16S ribosomal RNA. Iran South Med J. 2014;17(3):272–9. [Google Scholar]
- 33.Sharifi Yazdi MK, Haghi Ashtiani MT, Nikmanesh B, Soltan Dallal MM. Comparison of antibiotic resistance of bacterial agents associated in septicaemia in children and infants. Iran South Med J. 2014;17(2):223–32. [Google Scholar]
- 34.Khosravi N, Noorbakhsh S, Javadinia S, Ashouri S. Determination the bacterial etiologies for sepsis in premature newborns admitted in neonatal intensive care unit. Tehran Univ Med J. 2017;74(11):791–7. [Google Scholar]
- 35.Afsharpaiman S, Torkaman M, Saburi A, Farzaampur A, Amirsalari S, Kavehmanesh Z. Trends in incidence of neonatal sepsis and antibiotic susceptibility of causative agents in two neonatal intensive care units in Tehran, IR Iran. J Clin Neonatol. 2012;1(3):124–30. 10.4103/2249-4847.101692 ; PMCID: PMC3762027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, Schlapbach LJ, Reinhart K, Kissoon N. The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Respir Med. 2018;6(3):223–30. 10.1016/S2213-2600(18)30063-8 . [DOI] [PubMed] [Google Scholar]
- 37.Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–10. 10.1001/jama.2016.0287 ; PMCID: PMC4968574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.El-Din S, Rabie EM, El-Sokkary MMA, Bassiouny MR, Hassan R. Epidemiology of neonatal sepsis and implicated pathogens: a study from Egypt. BioMed Res Int. 2015;2015 509484 10.1155/2015/509484 ; PMCID: PMC4471255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kayange N, Kamugisha E, Mwizamholya DL, Jeremiah S, Mshana SE. Predictors of positive blood culture and deaths among neonates with suspected neonatal sepsis in a tertiary hospital, Mwanza-Tanzania. BMC Pediatr. 2010;10(1):39 10.1186/1471-2431-10-39 ; PMCID: PMC2889942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Chiabi A, Djoupomb M, Mah E, Nguefack S, Mbuagbaw L, Zafack J, et al. The clinical and bacteriogical spectrum of neonatal sepsis in a tertiary hospital in Yaounde, Cameroon. Iranian J Pediatr. 2011;21(4):441–8. ; PMCID: PMC3446127. [PMC free article] [PubMed] [Google Scholar]
- 41.Abdellatif M, Al-Khabori M, Rahman AU, Khan AA, Al-Farsi A, Ali K. Outcome of Late-onset Neonatal Sepsis at a Tertiary Hospital in Oman. Oman Med J. 2019;34(4):302 10.5001/omj.2019.60 ; PMCID: PMC6642716 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Watson RS, Carcillo JA, Linde-Zwirble WT, Clermont G, Lidicker J, Angus DC. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med. 2003;167(5):695–701. 10.1164/rccm.200207-682OC . [DOI] [PubMed] [Google Scholar]
- 43.Braye K, Foureur M, de Waal K, Jones M, Putt E, Ferguson J. Epidemiology of neonatal early-onset sepsis in a geographically diverse Australian health district 2006–2016. PloS One. 2019;14(4):e0214298 10.1371/journal.pone.0214298 ; PMCID: PMC6453454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Gurung B, Shrestha L. Bacterial profile of Early versus Late onset neonatal sepsis and its antimicrobial susceptibility: A 1-year retrospective study in a tertiary level teaching hospital of Nepal. J Inst Med. 2017;39(3):40–46. [Google Scholar]
- 45.Anegundi R, Kulkarni RD, Chitharagi VB, Ajantha G, Shubhada C, Varaiya A. Bacteriological Profile and Clinical Outcome in Cases of Neonatal Sepsis. Int J Curr Microbiol App Sci. 2017;6(4):2206–14. [Google Scholar]
- 46.Yancey MK, Duff P, Kubilis P, Clark P, Frentzen BH. Risk factors for neonatal sepsis. Obstetr Gynecol. 1996;87(2):188–94. 10.1016/0029-7844(95)00402-5 [DOI] [PubMed] [Google Scholar]
- 47.Schuchat A, Zywicki SS, Dinsmoor MJ, Mercer B, Romaguera J, O'Sullivan MJ, et al. Risk factors and opportunities for prevention of early-onset neonatal sepsis: a multicenter case-control study. Pediatrics. 2000;105(1):21–6. 10.1542/peds.105.1.21 [DOI] [PubMed] [Google Scholar]
- 48.Tsai M-H, Chu S-M, Hsu J-F, Lien R, Huang H-R, Chiang M-C, et al. Risk factors and outcomes for multidrug-resistant Gram-negative bacteremia in the NICU. Pediatrics. 2014;133(2):322–9. 10.1542/peds.2013-1248 . [DOI] [PubMed] [Google Scholar]
- 49.Fanaroff AA, Martin RJ. Neonatal-perinatal medicine: diseases of the fetus and infant. 7th ed St. Louis: Mosby; 2002. [Google Scholar]
- 50.Asadi-Lari M, Sayyari A, Akbari M, Gray D. Public health improvement in Iran—lessons from the last 20 years. Public health. 2004;118(6):395–402. 10.1016/j.puhe.2004.05.011 . [DOI] [PubMed] [Google Scholar]
- 51.Danaei G, Farzadfar F, Kelishadi R, Rashidian A, Rouhani OM, Ahmadnia S, et al. Iran in transition. Lancet. 2019; 393(10184):1984–2005. 10.1016/S0140-6736(18)33197-0 . [DOI] [PubMed] [Google Scholar]
- 52.Waters D, Jawad I, Ahmad A, Lukšić I, Nair H, Zgaga L, et al. Aetiology of community-acquired neonatal sepsis in low and middle income countries. J Glob Health. 2011;1(2):154–70. PMCID: PMC3484773. [PMC free article] [PubMed] [Google Scholar]
- 53.Li J-y, Chen S-q, Yan Y-y, Hu Y-y, Wei J, Wu Q-p, et al. Identification and antimicrobial resistance of pathogens in neonatal septicemia in China—A meta-analysis. Int J Infect Dis. 2018;71:89–93. 10.1016/j.ijid.2018.04.794 . [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX)
(TIF)
(TIF)
(TIF)
(DOCX)
(XLSX)
Data Availability Statement
All relevant data are within the manuscript and its Supporting Information files.