

Abstract
This article describes the process of infusing implementation strategies in the development of a school-based drug prevention curriculum for rural Native Hawaiian youth. The curriculum (Ho‘ouna Pono) is a video-enhanced, teacher-implemented curriculum developed using a culturally grounded and community-based participatory research approach. Throughout the development of the curriculum, strategies reflective of the domains of the Consolidated Framework for Implementation Research (CFIR) were integrated into the teacher training manual, in order to promote the implementation, adoption, and sustainability of the curriculum in rural Hawai‘i. These strategies were validated through qualitative data across two interrelated studies with community stakeholders in rural Hawai‘i. Implications for prevention, community, and educational practices are described in this article.
Keywords: Implementation, Native Hawaiian, culturally grounded, prevention, youth
Similar to other Indigenous youth populations, Native Hawaiian youth have been shown to have high rates of substance use/abuse, with significant adverse effects. In numerous studies, Native Hawaiian youth have been found to report the highest rate of alcohol, tobacco, and other drug use among ethnic groups in Hawai‘i (Glanz, Maskarinec, & Carlin, 2005; Glanz, Mau, Steffen, Maskarinec, & Arriola, 2007; Kim, Ziedonis, & Chen, 2007; Makini et al., 2001; Mayeda, Hishinuma, Nishimura, Garcia-Santiago, & Mark, 2006; Mokuau, 2002; Nigg, Anderson, Troumbley, Alam, & Keller, 2013; Nigg, Wagner, Garza, & Goya, 2017; Nishimura, Hishinuma, & Goebert, 2013; Wong, Klingle, & Price, 2004). For example, the 30-day marijuana use rate for Native Hawaiian high school students in 2015 (28.8%) is significantly higher than that of Filipinos, Japanese, and other Asians, and is also significantly higher than the 2015 national average (21.7%; Nigg et al., 2017). Drug use has been linked to poor academic performance (Hishinuma et al., 2006), increases in school absences, suspensions, and infractions (Hishinuma et al., 2006), higher rates of unsafe sexual practices (Ramisetty-Mikler, Caetano, Goebert, & Nishimura, 2004), and suicidal behavior (Else, Andrade, & Nahulu, 2007) of Native Hawaiian youth. These issues point to the need to develop culturally relevant interventions for these youth that are not only efficacious in content, but that are also able to be implemented and sustained in the community. Historically, the implementation of substance abuse prevention programs have been haphazard or poorly planned across rural Hawaiian communities (Waitzfelder, Engel, & Gilbert, 1998). By addressing both prevention efficacy and implementation, interventions will be able to effectively address health disparities of Native Hawaiian youth by exerting their maximum health impact over time.
This article describes the process of infusing implementation strategies in the development and evaluation of a culturally grounded drug prevention curriculum for rural Native Hawaiian youth. The curriculum, Ho‘ouna Pono, is a video-enhanced, interactive curriculum for middle/intermediate school youth that has been developed and evaluated over the past 12 years through community-based participatory research principles and practices. Through our collaboration with public school teachers, principals, and administrative staff, the curriculum has evolved by aligning prevention curricular content with dimensions of effective implementation (Damschroder & Hagedorn, 2011; Powell, Proctor, & Glass, 2014). Supported by data from two interrelated qualitative studies, this paper describes the dual processes of addressing both efficacy and implementation in the development and evaluation of the curriculum. It also describes the implications of this work for school-based prevention in rural and Indigenous communities.
Literature Review
The Ho‘ouna Pono Curriculum
The Ho‘ouna Pono curriculum is a culturally grounded, school-based drug prevention curriculum that was developed through a multi-university and community partnership in Hawai‘i (Helm & Okamoto, 2013; Helm et al., 2008). The nine-lesson curriculum provides resistance skills training through the use of video vignettes depicting relevant social and cultural contexts of rural Hawaiian youth identified through prior research (Okamoto, Helm, Giroux, Edwards, & Kulis, 2010; Okamoto, Helm, McClain, & Dinson, 2012). The video vignettes provide the platform for facilitated learning (Harthun, Dustman, Reeves, Marsiglia, & Hecht, 2009), in which youth are able to use life experiences stemming from the vignettes as part of the context for resistance skills training. Reviews of youth drug prevention programs have indicated resistance skills training to be one of the most effective preventative approaches, particularly when conducted within a social influence model of prevention (McBride, 2003; Skiba, Monroe, & Wodarski, 2004). Consistent with these reviews, Hopfer, Hecht, Lanza, Tan, and Xu (2013) found through a latent class analysis that pre-adolescents who were highly competent in using drug resistance skills had a significantly lower probability of recent substance use compared to other sampled youth.
The Ho‘ouna Pono curriculum promotes students’ exchanges of ideas and practice time, which is a hallmark of effective prevention programs (National Institute on Drug Abuse, 2003; Tobler & Stratton, 1997). It also uniquely focuses on the familial and relational context of drug offers in rural Hawai‘i. Guided by our prior federally-funded research with rural Hawaiian youth (Okamoto, Helm, Giroux, Kaliades, et al., 2010) and similar culturally grounded prevention research (Hecht et al., 2003; Kulis et al., 2005), core drug resistance strategies covered in the curriculum include overt refusal of drug offers, explaining personal reasons behind drug refusal, avoiding situations where drugs might be present, redirecting the topic away from drug use, and leaving a situation where drugs are present. The curriculum is implemented by public middle/intermediate school teachers once a week for 45–60 minutes over a 10-week academic quarter in a required physical/health education course. All sessions of the curriculum follow the same basic format–an introduction and/or review of the past lesson, a culture wall activity, a video, 1–2 interactive activities, and a wrap-up activity (Okamoto, Helm, & Dustman, 2015). The culture wall activity involves the discussion and application of Hawai‘i Island cultural concepts to drug prevention. For example, the concept of pu’uhonua (place of refuge) is used to introduce the concept of psychosocial “protection” in lesson two of the curriculum. The interactive activities following the videos introduce specific resistance skills and relate directly to the characters in the videos. Similar to prior research (Gosin, Dustman, Drapeau, & Harthun, 2003; Harthun, Drapeau, Dustman, & Marsiglia, 2002), the curriculum (i.e., nine lessons and eight video vignettes) was subjected to an expert analysis by relevant stakeholders (e.g., teachers, school counselors, and principals) to assess face validity (Okamoto, Helm, Ostrowski, & Flood, 2018).
Multiple evaluations with different samples have shown promising findings for the Ho‘ouna Pono curriculum. For example, a pilot evaluation (N = 213) across three waves of data (pre-test data collection prior to administering the curriculum, post-test data collection immediately following the delivery of the final lesson, and 6-month follow-up) demonstrated positive findings related to assessment of situational risk, use of drug resistance strategies, and dealing with interpersonal conflict (Okamoto, Kulis, Helm, Lauricella, & Valdez, 2016). Compared with youth in the control schools, paired sample t-tests of mean difference scores indicated that youth in the intervention schools thought significantly more about the consequences resulting from accepting drugs from pre-test to 6-month follow-up. Paired sample t-tests of mean difference scores also indicated that youth in the control schools had a significant decrease in the use of non-confrontational drug resistance strategies (avoid, explain, and leave) at 6-month follow-up (ps < .05), which was not observed with the intervention youth, suggesting that the curriculum may have helped maintain or sustain youths’ use of these types of strategies. Finally, youth in the control schools demonstrated a significant increase in fighting at 6-month follow-up (p < .05, Cohen’s d = −0.38), which was not observed in the intervention group. Mixed models controlling for random (nesting) effects further indicated a significant decrease in fighting for girls in the intervention group (Est β = −0.66, SE = 0.32, p < .05), supporting the gender-specific effectiveness of the curriculum in curbing aggressive behavior. These results were largely maintained at 12-month follow-up (Okamoto, Helm, & Kulis, 2015). More recently, a two-year longitudinal evaluation of the curriculum (N = 374) found small, significant findings in the intended direction for cigarette/e-cigarette use and hard drug use (Okamoto et al., in press), suggesting that the curriculum may have relevance for cancer prevention and control, and may help “interrupt” the transition from alcohol, tobacco, and other drug use to “harder” drug use.
The Consolidated Framework for Implementation Research (CFIR)
Through the community-based participatory research process, components of the Ho‘ouna Pono curriculum organically aligned themselves with the domains within the Consolidated Framework for Implementation Research (CFIR; Damschroder et al., 2009). CFIR provides one of the most comprehensive frameworks of key constructs informing implementation research and practice (Damschroder & Hagedorn, 2011; Powell et al., 2014). It is an overarching typology resulting from the synthesis of multidisciplinary implementation theories, empirical investigations, and conceptual studies. Thirty-nine constructs have been organized into 5 domains—(1) Intervention Characteristics (e.g., evidentiary support, relative advantage, adaptability), (2) Outer Setting (e.g., organizational connectedness, peer pressure), (3) Inner Setting (e.g., structural characteristics, readiness for implementation), (4) Characteristics of Individuals (e.g., knowledge, self-efficacy), and (5) Process (planning, engaging, executing, and reflecting/evaluating). These domains reflect the evidence base of factors most likely to influence implementation of interventions. The model has mainly been used to guide data analysis in implementation research (Kirk et al., 2016), although some research has integrated the model throughout different phases of the research process, such as data collection and reporting of actionable findings (Keith, Crosson, O’Malley, Cromp, & Taylor, 2017). The CFIR domains consolidate implementation theories, terminology, and concepts into one unifying model (Damschroder & Hagedorn, 2011), providing a solid theoretical foundation for the implementation of Ho‘ouna Pono.
The CFIR framework has been used by over 300 different studies; however, the bulk of the literature using the CFIR framework focuses on health care settings (Powell et al., 2014). Our program of prevention research contributes to the implementation science literature by applying the CFIR model to a unique setting (rural public schools). The State of Hawai‘i Department of Education (HIDOE) is a unique system in which to apply the CFIR framework. While most states’ educational systems consist of multiple public school districts that are autonomous in nature, the HIDOE is comprised of 15 school complex areas (i.e., a cluster of high schools and their respective feeder schools) within one district administered at the state level. Due to this structure, individual schools function within the context of their respective school complex areas, which are nested within the overall state-level district (see Figure 1), creating multiple levels to the inner setting of the HIDOE. Beyond this unique institutional setting, our program of prevention research contextualizes the CFIR model within a health disparities framework, specifically focusing on Native Hawaiian, Pacific Islander, and Indigenous youth populations.
Figure 1.
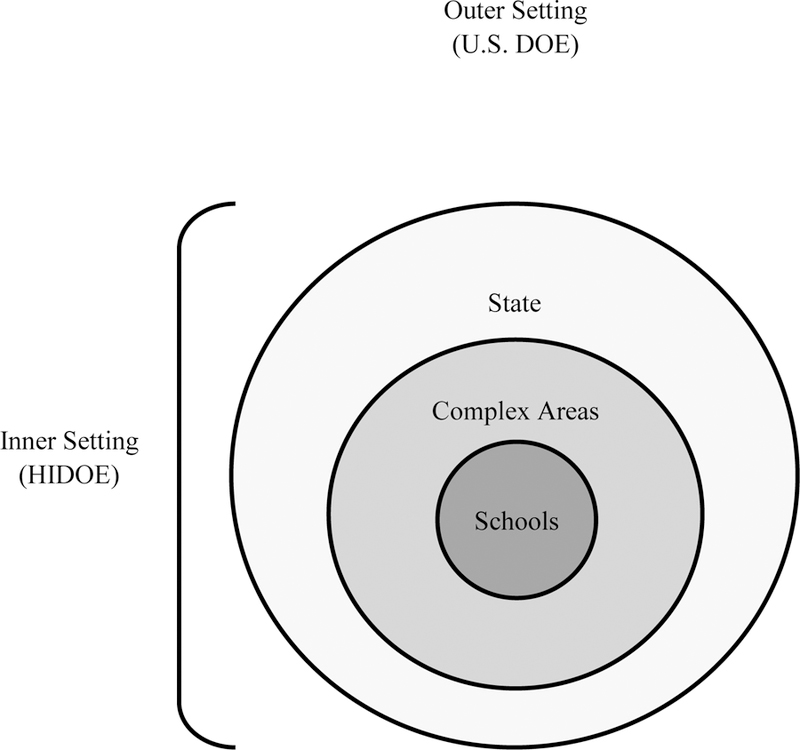
Structure of the State of Hawai‘i Department of Education (HIDOE)
Method
Participants and Procedures
Implementation strategies for Ho‘ouna Pono were the focus of two recent, interrelated qualitative studies—(1) a curriculum validation study, which occurred prior to the two-year efficacy trial of the curriculum, and (2) an implementation, adoption, and sustainability (IAS) pilot study, which occurred after the efficacy trial was completed. Two of the goals of the curriculum validation study were to refine and update implementation strategies generated from a pilot version of the curriculum, and to generate new strategies to incorporate into the full-scale version of the curriculum (Okamoto et al., 2018). For example, based on feedback from the curriculum validation study, multiple online platforms for implementation support that were used in the pilot study were consolidated into a teacher implementation website for the efficacy trial, and additional content related to common core was inserted into the final lesson of the curriculum as an optional summative assignment. The goals of the IAS pilot study were to examine barriers to systemic implementation across Hawai‘i Island and the HIDOE, and to examine factors that might promote uptake of the curriculum across public middle/intermediate schools on Hawai‘i Island and the HIDOE. Data from the IAS pilot study will be used to develop regionally tailored implementation plans across Hawai‘i Island communities in a future study.
Both studies involved in-depth interviews with educational stakeholders in all three school complex areas on Hawai‘i Island. The demographic characteristics of both samples are outlined in Table 1. The majority of the participants in both studies participated in individual interviews that were conducted on-site at their schools or administrative offices. In two interview sessions for the IAS pilot study, participants were interviewed on-site in dyads, upon their request. Interviews lasted approximately one hour, and were facilitated by the principal investigator, co-principal investigator, and/or the field site coordinator. Sample questions for the curriculum validation study included “What might be some issues in implementing the curriculum in the classroom setting? How might these issues be addressed?” “How easily do you see the curriculum fitting in with the current academic structure?” and “What types of support will teachers need to administer the curriculum successfully?” Sample questions for the IAS pilot study reflected the CFIR domains, such as “What can be done to further promote Ho‘ouna Pono’s alignment with teachers’ professional and educational needs?” (Intervention Characteristics), “How do local, state, or national performance measures or policies influence the implementation of Ho‘ouna Pono?” (Outer Setting), “Which administrative units/individuals within the Hawai‘i Department of Education should oversee the implementation of the curriculum? Why?” (Inner Setting), “How confident do you feel about implementing Ho‘ouna Pono in your classes? Do you think other teachers in your school will be able to use it?” (Characteristics of Individuals), and “Who do you see as the lead person implementing the curriculum in your school?” (Process). Although the studies were different in foci and purpose, the narrative data from both studies complimented each other and both data sets supported the CFIR framework. The curriculum validation study focused more on characteristics of the curriculum and the inner (school) setting, while the IAS pilot study addressed outer setting issues, such as state-level educational policies and their relationship to Federal educational mandates.
Table 1.
Participant Demographics for the Ho’ouna Pono Curriculum Validation Study and Implementation, Adoption, and Sustainability (IAS) Pilot Study
| Variable | Curriculum Validation (N = 8) | IAS Pilot (N = 16) | |
|---|---|---|---|
| Gender | Male | 37.5% | 57.0% |
| Female | 62.5% | 43.0% | |
| Age | 22–30 | 0 | 12.5% |
| 31–40 | 12.5% | 6.3% | |
| 41–50 | 37.5% | 37.5% | |
| 51–60 | 37.5% | 31.3% | |
| 61–70 | 12.5% | 12.5% | |
| Ethnicity | White | 62.5% | 43.8% |
| Japanese | 0 | 12.5% | |
| Hawaiian | 0 | 6.3% | |
| Multiracial | 37.5% | 37.5% | |
| Job Position | Superintendent | 0 | 12.5% |
| Principal/Vice Principal | 37.5% | 18.8% | |
| Teacher | 25.0% | 43.8% | |
| Counselor/School-Based Behavioral Health | 37.5% | 12.5% | |
| Other Complex-Level Staff | 0 | 12.5% | |
| Years with HIDOE | 3–5 | 0 | 6.3% |
| 6–10 | 12.5% | 18.8% | |
| 11–20 | 62.5% | 37.5% | |
| 21–30 | 25.0% | 31.3% | |
| 31+ | 0 | 6.3% | |
| Highest Education Level | Bachelor’s Degree | 0 | 31.3% |
| Master’s Degree | 87.5% | 62.5% | |
| Doctoral Degree | 12.5% | 6.3% | |
Data Analysis
The data analysis for both studies followed the same procedures. All interviews were audio recorded and transcribed verbatim by a member of the data analysis team. This team consisted of the principal investigator and co-principal investigator, both of whom were health promotion researchers affiliated with two large universities in the Pacific, and six student research assistants trained in psychology, public health, or social work. To ensure data quality, transcripts were reviewed for accuracy by at least two different research team members. Consistent with grounded theory, a comprehensive set of emergent open codes (Strauss & Corbin, 1990) were collaboratively identified by five research team members. A subset of frequently used codes emerging from the IAS pilot study, mapped by CFIR domains and constructs, are presented in Table 2. These codes were imported into a computer-assisted qualitative data analysis software program (NVivo 12, 2018). NVivo is one of several code-based, theory-building programs that allow the researcher to represent relationships among codes or build higher-order classifications (Weitzman, 2000). In order to establish intercoder reliability and validity, all members of the research team collectively coded one transcript, in order to clarify the definition and parameters of all of the codes. Then, all subsequent transcripts were separately coded by at least two of these research team members. A consensus coding technique was employed in this study, in which the content, length, and placement of narrative units were mutually agreed upon by the team members. Narrative segments that were not identically coded by the team members were identified, discussed, and justified for inclusion or exclusion in the data set. This process entailed explaining how the content and length of discrepant narrative units were consistent or inconsistent with the definition of the code, until consensus was achieved. Upon establishing intercoder reliability and validity, an analysis of the feedback of the Ho‘ouna Pono Curriculum Teacher Training Manual (Version 2) was conducted, in order to examine issues related to the implementation of the curriculum in public schools on Hawai‘i Island.
Table 2.
Frequently Used CFIR Codes from the IAS Pilot Study
| Code Name | CFIR Domain | CFIR Construct | Definition | Interviews Cited* |
|---|---|---|---|---|
| Student Experiences with Curriculum | Intervention Characteristics | Adaptability | Discussion of student experiences with the Ho‘ouna Pono (HP) curriculum | 71% |
| Promoting Cultural Knowledge | Intervention Characteristics | Relative Advantage | Discussion of how the HP curriculum promotes cultural knowledge (e.g., Hawaiian and/or rural culture) | 79% |
| Teacher Experiences with Curriculum | Characteristics of Individuals | Knowledge and Beliefs about the Intervention | Discussion of teacher experiences with and opinions of the HP curriculum | 71% |
| Teacher Autonomy | Characteristics of Individuals | Self-efficacy | Teachers descriptions of how they customized the curriculum to fit their own needs and/or the flexibility of the curriculum to adapt to their teaching style | 71% |
| Common Core/Standardized Testing | Outer Setting | External Policies and Incentives | Discussion of how pressures of standardized testing and Common Core requirements can compromise time and resources devoted to health curricula, such as HP. | 86% |
| Department of Education Funding/Resources | Outer Setting | External Policies and Incentives | Discussion of Department of Education funding and resources | 64% |
| Teacher Turnover | Inner Setting | Structural Characteristics | Implementation issues resulting from teachers leaving, new teachers from the mainland moving to Hawai‘i, the teacher retention rate, and/or other related staffing issues. | 50% |
| Curriculum Champion(s) | Inner Setting | Learning Climate/Leadership Engagement | Discussion of important individuals who can influence the IAS of HP. Discussion/description of individual(s) who may become advocates for the program within the DOE system. | 64% |
| Teacher Training | Process | Planning | Discussion of the role that teacher training would play in sustaining HP. | 86% |
| Implementation Structure and Logistics | Process | Planning | Discussion of administration, staffing, and content area logistics in sustaining the curriculum (e.g., courses where the curriculum would fit best for implementation, such as Advisory periods or Social Studies). | 100% |
“Interviews Cited” is the percentage of interviews in the data set that cited the corresponding code.
Results
Supported with data from the curriculum validation and IAS pilot studies, this section describes how four of the five domains in the CFIR model were reflected in the development of the Ho‘ouna Pono curriculum—Intervention Characteristics, Inner Setting, Characteristics of Individuals, and Process. It also describes how future implementation research will focus on the alignment of the curriculum with dramatic state-level policy changes (Qina’au, 2016), in order to promote the curriculum’s use as a standard educational health practice within the HIDOE.
Intervention Characteristics
The first major domain of the CFIR is related to the characteristics of the intervention being implemented in a particular setting or organization (Damschroder et al., 2009). This domain focuses on the features of an intervention that might influence implementation (Keith et al., 2017). Our program of prevention research has directly focused on the development of intervention characteristics that are culturally relevant, engaging for the classroom setting, and informed by best practices in prevention science. In the curriculum validation study, one participant indicated that HIDOE faculty and staff appreciated the Hawai‘i Island cultural references interwoven throughout the curriculum’s structure (Okamoto et al., 2018). He commented on the cultural validity of the videos in the curriculum, and the way in which they engaged youth in the drug prevention messages.
I thought that they were very [good]. I was very impressed at the level of the kids’ ability to come across genuine [in the videos] and of course the way in which Matt [the director] put the [videos] together. The way they were scripted was very genuine. And the [youth actors] did a great job and that, of course, will bite right into the other kids as they watch it, because you can really feel the emotion when you’re looking at ‘em. And I loved the cross section of where the vignettes occurred. I mean, awesome, awesome, awesome. I mean, a lot of the time people don’t want to talk about what’s happening at the house and the party on the weekend. And so I thought the videos were excellent.
Beyond its content, the curriculum also was designed to promote critical thinking through the use of an interactive, critical pedagogy. Interactive and/or critical pedagogy has been described as a characteristic of effective drug prevention programs for decades (Ennett et al., 2003), and also has been promoted as part of the best educational practices for HIDOE teachers through their Educator Effectiveness System (Hawai‘i State Department of Education, 2018). Specifically, the HIDOE adapted the Charlotte Danielson pedagogical framework for observational analysis, in order to evaluate the teaching efficacy of its faculty and staff (The Danielson Group, 2017). Characteristic of this model is the teachers’ effective use of a variety or series of questions or prompts to challenge students cognitively and to engage them in higher-level thinking. This approach is promoted in the curriculum through the analysis of video vignettes depicting common and challenging drug-related problem situations occurring within the cultural context of rural Hawai‘i. Teachers engage students through a series of interactive activities and discussions based on the videos that promote interpersonal problem-solving and higher-level thinking.
Inner Setting
The inner setting includes features of the implementing organization that might influence implementation, including the internal structural, political, and/or cultural contexts which impact the implementation process (Damschroder et al., 2009; Keith et al., 2017). The Ho‘ouna Pono curriculum was implemented in 12 different public middle, intermediate, and multi-level school across Hawai‘i Island. Each school had a unique inner setting, including differences in explicit and implicit leadership structure, curriculum sequencing, course scheduling, and educational priorities. This required our research team to design the curriculum to be able to address drastically different school contexts. For example, although the curriculum was used primarily in health and physical education courses, some schools considered implementing it in required advisory periods, so that more youth would be able to participate in the curriculum. This required the lessons to be broken up into smaller units, so that they could be implemented in a shortened (30-minute) time frame. In other schools, the curriculum was implemented in an assembly-style format over three weeks, requiring three to four lessons to be taught per week. In order to address these different time demands, each lesson included multiple activities, and additional steps within each activity, in order to customize the timing of each lesson.
More broadly, some schools expressed reluctance in committing too much of their health curricula on drug and alcohol use. For these schools, we emphasized that the curriculum also addressed managing significant interpersonal relationships within drug-related problem situations. This focus made it relevant for schools interested in bolstering social-emotional learning, interpersonal problem-solving abilities, and decision-making skills of their students. With this perspective, realistic offers to use drugs and alcohol become the context to practice situationally specific refusal strategies while also preserving relational harmony among peers and family members. A participant in the IAS pilot study highlighted this multidimensional perspective by describing the curriculum’s ability to address several content areas across the HIDOE health standards.
So, at my school, [we] might be focused [more] on drugs and alcohol, whereas another school might be focused more on relationships, because that’s what’s happening there. Another school might be focused more on violence, ‘cause that’s what’s happening there. Although [these] are all components of our health course and the [health] content, [other teachers are] gonna spend more time on [a topic other than drugs], because that’s what they need. So, what I like about this curriculum is everything is right there, easy to grab, easy to put into [action], but it covers a broad spectrum of our content area.
Within each school, we enlisted the support of a school-based liaison, who functioned as their school’s champion of the curriculum. This person supported implementation fidelity, and helped to coordinate the evaluation of the curriculum. Typically, the school-based liaison had a long-standing relationship with the research team, and participated in the early stages of the curriculum’s development. Their role was essential in maintaining the motivation and momentum involved in the successful implementation of Ho‘ouna Pono.
Characteristics of Individuals
The CFIR recognizes that the characteristics of individuals involved with the intervention and/or implementation process can influence the organizational structure and context for implementation (Damschroder et al., 2009). With this in mind, the curriculum was designed to address two common types of teachers—(1) experienced teachers who find manualized curricula pedagogically restrictive, and (2) new teachers who need the structure offered by manualized curricula. Experienced teachers who used the curriculum appreciated its flexibility and ability for customization. These teachers typically adhered to the basic components of the curriculum—the review of the prior lesson, the video, and a main activity—but changed other components of the curriculum to better fit the learning styles and needs of their students. One experienced teacher who was interviewed about the implementation of the curriculum for the IAS pilot study described how she customized it to fit the needs of her students.
I took a lot of the lessons [and changed them]. I knew there [were] some I couldn’t complete and finish, but I liked having those lessons available, in case I remembered, “Oh yeah, this is a good activity, I’m gonna open this one up and we’ll do this [one] today.” But, I was able to put [parts of the curriculum] into a PowerPoint [presentation]. I was able to, you know, prompt them with [a] little more, I would say, deeper thought, higher order thinking questions that I know my kids are being pushed at doing [in my classes].
On the other hand, new teachers appreciated the structure offered by the teacher training manual. The lessons provided specific steps for each activity, the time involved for each activity, specific ways to shorten or extend different activities, and the HIDOE-required health standards met by each lesson. One new teacher interviewed for the IAS pilot study indicated that the curriculum was “pretty self-explanatory, as far as what needed to be done [to get it] across to the students.” Another new teacher interviewed for the IAS pilot study described her appreciation for the structure and details of each lesson.
It’s easy and it’s accessible and there’s no reason not to [use it]. Again, you’ve made it very easy, you laid it all out, you aligned it all [with the Hawai‘i Content and Performance Standards for Health, and] you can see the “why” [of each activity]. It was presented very well. It’s compiled very well. I had no issue with any of that. It was great and easy to use.
Process
The CFIR Process domain includes strategies or tactics that might influence implementation (Keith et al., 2017). These strategies or tactics fall within four types of activities that are essential for the intervention to achieve its individual and organizational use as designed —(1) planning for the use of implementation strategies, (2) engaging appropriate individuals in the implementation and use of the intervention, (3) executing the intervention according to plan, and (4) reflecting/evaluating on the intervention through qualitative or quantitative feedback about the progress and quality of implementation (Damschroder et al., 2009). To facilitate the use of the curriculum, we made several modifications to the teacher training manual during the planning and engaging stages of the implementation process that incentivized the use of Ho‘ouna Pono. These were modifications that were not related to the core content of the curriculum; however, they were essential for promoting teachers’ motivation to use the curriculum, and the overall feasibility of the curriculum within HIDOE public schools. Specifically, each lesson was aligned with the Hawai‘i Content and Performance Standards for Health (6–8 grade) and/or the National Common Core Standards in public education, and teachers were trained to implement the curriculum through a hybrid (i.e., in-person and virtual), credit-granting course sanctioned through the HIDOE. These measures were designed to promote sustainability and adoption of the curriculum in Hawai‘i Island communities through garnering support across multiple levels in the HIDOE (see Figure 1). Given the rural locations of intervention schools, implementation fidelity was assessed using synchronous and asynchronous virtual methods (i.e., a weekly online class session and a discussion board facilitated by the program developers). Both of these methods were pilot-tested in prior research and consolidated into a teacher implementation website for the efficacy trial. The website allowed for schools dispersed across a wide geographic range to receive timely implementation support from faculty peers and the program developers. To further incentivize its use, teachers’ active participation in the online class and discussion board were required for them to earn continuing education credits.
Outer Setting
The outer setting refers to the economic, political, and social context within which an organization resides (Damschroder et al., 2009). The outer setting of the curriculum is the focus of future implementation research in rural Hawai‘i. The adoption and implementation of Ho‘ouna Pono has been challenged by the systemic focus on the nationally supported Common Core and standards-based education within the HIDOE. For example, an administrator interviewed for the IAS pilot study candidly described this issue.
Within the DOE, we’re concerned with literacy, we’re concerned with being able to [get kids] college-career ready [and] being able to find a job. And, that’s a higher critical need than [drugs]. At least, that’s the way I see it. So, the push is not gonna necessarily be health. Obviously, we don’t want to walk away from it, but it’s going to be, “how are we getting our children ready [for the future?] I just welcomed the class of 2025, which is scary and we’re not ready. There are things that we’re not ready for.
However, the U.S. Department of Education has recently allowed for more flexibility to implement educational standards at the state-level (U.S. Department of Education, 2016). As a potential outgrowth of this federal policy, the State Superintendent of the HIDOE has been emphasizing a more holistic, culturally grounded, and balanced approach to public education. In 2015, an advisory workgroup to the Board of Education, comprised of stakeholders from Native Hawaiian organizations and communities, developed the HĀ Framework (see Figure 2). The goal of the framework was to develop students’ cultural competence and character development alongside their academic achievement (Qina’au, 2016), by focusing on six interdependent outcomes that address the overall health and wellness of the “whole” child. Future research for Ho‘ouna Pono will examine how the curriculum compliments the HĀ Framework, and whether the alignment with this philosophical approach will enhance the adoption, implementation, and sustainability of the curriculum.
Figure 2.
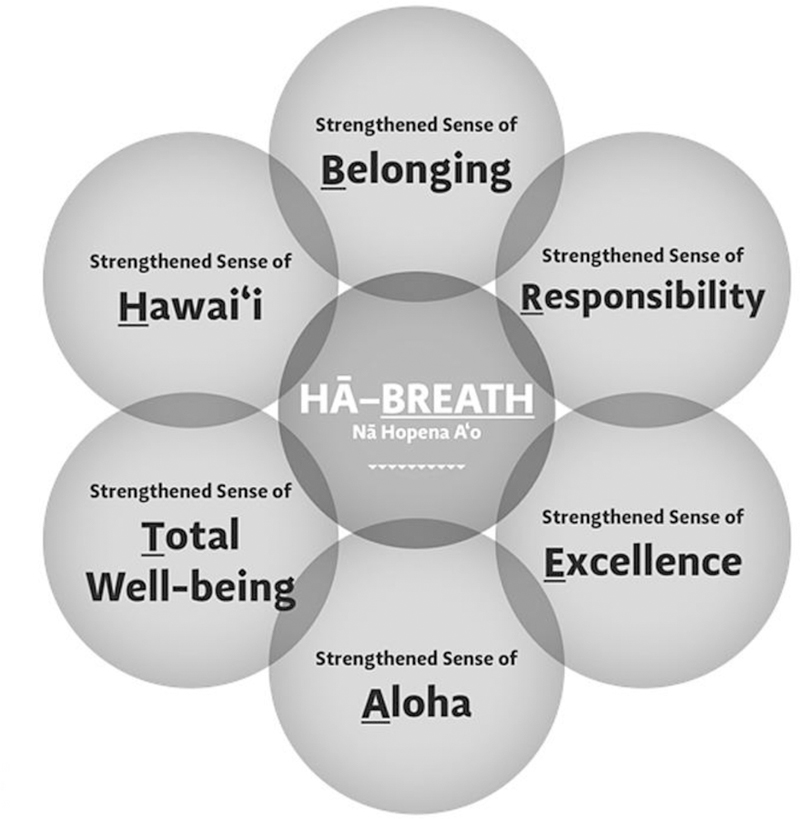
HĀ Framework (Lupenui et al., 2015)
Discussion
This article describes how implementation strategies were infused throughout the development of a culturally grounded, school-based, drug prevention curriculum for rural Native Hawaiian youth. Qualitative data from educational stakeholders on Hawai‘i Island were used to both guide and validate the process of implementation. For example, as a result of the interviews, we found areas in the curriculum to allow for implementation flexibility for teachers, while still ensuring fidelity to the curriculum. We also received validation in the interviews for curricular content decisions that were made in collaboration with DOE faculty and staff, such as aligning the curriculum with state-level health standards and the cultural context of Hawai‘i Island.
Some research has supported the focus on implementation strategies alongside the development of core curricular content. Glisson et al. (2010), for example, found that addressing implementation factors and strategies for an evidence-based intervention significantly ameliorated youth behavioral disorders beyond the application of the intervention without attention to these factors. For Ho‘ouna Pono, implementation strategies organically emerged throughout the development of the curriculum, and reflected the domains of the Consolidated Framework for Implementation Research (CFIR). Future work will focus on examining the outer setting of the HIDOE (i.e., the U.S. Department of Education) and the impact of local and state-level policy initiatives (e.g., HĀ) on the implementation, adoption, and sustainability of the curriculum in rural Hawai‘i. Specifically, this work might examine whether decreased federal oversight on Common Core and standardized testing will promote more academic flexibility at the complex and school levels, thereby promoting the implementation of culturally grounded prevention curricula such as Ho‘ouna Pono.
Implications for Community Practice
Our program of prevention research highlights the importance of acknowledging and reflecting implementation strategies in the development and evaluation of prevention curricula. For our team, this required an iterative, dynamic process with rural and/or Indigenous schools and communities in developing the content and delivery of the curriculum. Specifically, the content and delivery of the curriculum were adapted to reflect the structure and priorities of the HIDOE, which often were not central to the intervention. Nonetheless, these adaptations were necessary to enhance schools’ and teachers’ motivations to implement the curriculum, as well as the overall feasibility of the curriculum. Thus, they were treated as equally important to the core content. One lesson we learned was to broaden our focus beyond the narrow evaluation of prevention curricular content, and to align the components of the curriculum with the structure and priorities of the organizational system it is intended to serve.
Beyond promoting the internal validity and feasibility of the curriculum, our attention to implementation strategies also highlights the collaborative, community-based, and participatory nature of implementation research in rural and Indigenous communities. This requires university prevention researchers to relinquish some decision-making authority, and often work outside of their disciplinary expertise and foci, in order to allow communities to actively inform and shape the research process. In this way, the principles and practices of community-based participatory research directly inform the implementation science of school-based, substance use prevention for rural and Indigenous youth. We learned that the core of implementation research in rural, Indigenous communities is built upon collaborative relationships between researchers and stakeholders within these communities. These communities must have an active role in the development of interventions over time, in order for the interventions to be implemented and sustained in the community. In fact, without shared decision-making about implementation, adoption, and sustainability at multiple levels within school and community systems, we would argue that effective youth prevention interventions may continue to elude routine rural public health practice.
Conclusions
This article describes one approach to the application of implementation science within the context of youth drug prevention in rural Hawai‘i. We described the early stages of moving our evidence-based curriculum into becoming part of standard educational health practices in the Hawai‘i State Department of Education. Future considerations for implementation include ways to adapt the curriculum to respond to emerging state-level policy changes, ways to support the implementation of the curriculum outside of extramural research funding, and ways to sustain the motivation and enthusiasm for the use of the curriculum across the HIDOE and in rural Hawai‘i. These considerations will be examined in future research focused on implementation barriers and strategies in rural Hawai‘i, contributing to our understanding of the contextual determinants of implementation (Waltz, Powell, Fernandez, Abadie, & Damschroder, 2019).
Evidence of intervention efficacy alone is insufficient to motivate community stakeholders to adopt and implement an intervention over time. These interventions should align themselves with the professional demands, reward structures, and administrative priorities of the systems they are intended to serve. Researchers should consider systemic implementation strategies throughout the development of interventions, in order to promote their utility and long-term effectiveness. As a result, these interventions will be able to exert the maximum public health impact for communities affected by health disparities.
Acknowledgments
This study was funded by the National Institutes of Health/National Institute on Drug Abuse (R01 DA037836–01A1 and R34 DA046735–01A1), with supplemental funding from the College of Health and Society Scholarly Endeavors Program, Hawai‘i Pacific University. All authors declare no other conflicts of interest in the publication of this study. The authors would like to thank Nathalie Jones and Jason Seto for their assistance with data collection and data analysis for this study.
Contributor Information
Scott K. Okamoto, Hawai‘i Pacific University
Susana Helm, University of Hawai‘i at Mānoa.
Steven Keone Chin, Hawai‘i Pacific University.
Janice Hata, Hawai‘i Pacific University.
Emily Hata, Hawai‘i Pacific University.
Kelsie H. Okamura, State of Hawai‘i Department of Health
References
- Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, & Lowery JC (2009). Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implementation Science, 4(50), 1–15. doi: 10.1186/1748-5908-4-50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Damschroder LJ, & Hagedorn HJ (2011). A guiding framework and approach for implementation research in substance use disorders treatment. Psychology of Addictive Behaviors, 25(2), 194–205. doi: 10.1037/a0022284 [DOI] [PubMed] [Google Scholar]
- Else IRN, Andrade NN, & Nahulu LB (2007). Suicide and suicidal-related behaviors among Indigenous Pacific Islanders in the United States. Death Studies, 31(5), 479–501. doi: 10.1080/07481180701244595 [DOI] [PubMed] [Google Scholar]
- Ennett ST, Ringwalt CL, Thorne J, Rohrbach LA, Vincus A, Simons-Rudolph A, & Jones S (2003). A comparison of current practice in school-based substance use prevention programs with meta-analysis findings. Prevention Science, 4(1), 1–14. [DOI] [PubMed] [Google Scholar]
- Glanz K, Maskarinec G, & Carlin L (2005). Ethnicity, sense of coherence, and tobacco use among adolescents. Annals of Behavioral Medicine, 29(3), 192–199. [DOI] [PubMed] [Google Scholar]
- Glanz K, Mau M, Steffen A, Maskarinec G, & Arriola KJ (2007). Tobacco use among Native Hawaiian middle school students: Its prevalence, correlates and implications. Ethnicity & Health, 12(3), 227–244. doi: 10.1080/13557850701234948 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glisson C, Schoenwald SK, Hemmelgarn A, Green P, Dukes D, Armstrong KS, & Chapman JE (2010). Randomized trial of MST and ARC in a two-level evidence-based treatment implementation strategy. Journal of Consulting and Clinical Psychology, 78(4), 537–550. doi: 10.1037/a0019160 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gosin MN, Dustman PA, Drapeau AE, & Harthun ML (2003). Participatory action research: Creating an effective prevention curriculum for adolescents in the Southwestern US. Health Education Research: Theory & Practice, 18(3), 363–379. doi: 10.1093/her/cyf026 [DOI] [PubMed] [Google Scholar]
- Harthun ML, Drapeau AE, Dustman PA, & Marsiglia FF (2002). Implementing a prevention curriculum: An effective researcher-teacher partnership. Education and Urban Society, 34(3), 353–364. [Google Scholar]
- Harthun ML, Dustman PA, Reeves LJ, Marsiglia FF, & Hecht ML (2009). Using community-based participatory research to adapt keepin’ it REAL: Creating a socially, developmentally, and academically appropriate prevention curriculum for 5th graders. Journal of Alcohol and Drug Education, 53(3), 12–38. [PMC free article] [PubMed] [Google Scholar]
- Hawai‘i State Department of Education. (2018). EES 2018–19: Educator Effectiveness System Retrieved from https://www.hawaiipublicschools.org/DOE%20Forms/Educator%20Effectivness/EESManual.pdf
- Hecht ML, Marsiglia FF, Elek E, Wagstaff DA, Kulis S, Dustman P, & Miller-Day M (2003). Culturally grounded substance use prevention: An evaluation of the keepin’ it R.E.A.L. curriculum. Prevention Science, 4(4), 233–248. [DOI] [PubMed] [Google Scholar]
- Helm S, & Okamoto SK (2013). Developing the Ho‘ouna Pono substance use prevention curriculum: Collaborating with Hawaiian youth and communities. Hawai‘i Journal of Medicine & Public Health, 72(2), 66–69. [PMC free article] [PubMed] [Google Scholar]
- Helm S, Okamoto SK, Medeiros H, Chin CIH, Kawano KN, Po’a-Kekuawela K, … Sele FP (2008). Participatory drug prevention research in rural Hawai‘i with Native Hawaiian middle school students. Progress in Community Health Partnerships: Research, Education, and Action, 2(4), 307–313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hishinuma ES, Else IRN, Chang JY, Goebert DA, Nishimura ST, Choi–Misailidis S, & Andrade NN (2006). Substance use as a robust correlate of school outcome measures for ethnically diverse adolescents of Asian/Pacific Islander ancestry. School Psychology Quarterly, 21(3), 286–322. [Google Scholar]
- Hopfer S, Hecht ML, Lanza ST, Tan X, & Xu S (2013). Preadolescent drug use resistance skill profiles, substance use, and substance use prevention. The Journal of Primary Prevention, 34(6), 395–404. doi: 10.1007/s10935-013-0325-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keith RE, Crosson JC, O’Malley AS, Cromp D, & Taylor EF (2017). Using the Consolidated Framework for Implementation Research (CFIR) to produce actionable findings: A rapid-cycle evaluation approach to improving implementation. Implementation Science, 12(15), 1–12. doi: 10.1186/s13012-017-0550-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim SS, Ziedonis D, & Chen K (2007). Tobacco use and dependence in Asian American and Pacific Islander adolescents: A review of the literature. Journal of Ethnicity in Substance Abuse, 6(3), 113–142. doi: 10.1300/J233v06n03_05 [DOI] [PubMed] [Google Scholar]
- Kirk MA, Kelley C, Yankey N, Birken SA, Abadie B, & Damschroder LJ (2016). A systematic review of the use of the Consolidated Framework for Implementation Research. Implementation Science, 11(72), 1–13. doi: 10.1186/s13012-016-0437-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kulis S, Marsiglia FF, Elek E, Dustman P, Wagstaff DA, & Hecht ML (2005). Mexican/Mexican American adolescents and keepin’ it REAL: An evidence-based substance use prevention program. Children and Schools, 27(3), 133–145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lupenui CK, Sang DK, Seward H, Lee H, Walk K, Benioni K, … Kahumoku W (2015). Nā Hopena A’o Statements-HĀ: BREATH Honolulu, HI: Hawai‘i State Department of Education. [Google Scholar]
- Makini GK Jr., Hishinuma ES, Kim SP, Carlton BS, Miyamoto RH, Nahulu LB, … Else IRN (2001). Risk and protective factors related to Native Hawaiian adolescent alcohol use. Alcohol and Alcoholism, 36(3), 235–242. [DOI] [PubMed] [Google Scholar]
- Mayeda DT, Hishinuma ES, Nishimura ST, Garcia-Santiago O, & Mark GY (2006). Asian/Pacific Islander youth violence prevention center: Interpersonal violence and deviant behaviors among youth in Hawai‘i. Journal of Adolescent Health, 39(2), 276.e271–276.e211. doi: 10.1016/j.jadohealth.2005.12.006 [DOI] [PubMed] [Google Scholar]
- McBride N (2003). A systematic review of school drug education. Health Education Research, 18(6), 729–742. [DOI] [PubMed] [Google Scholar]
- Mokuau N (2002). Culturally based interventions for substance use and child abuse among Native Hawaiians. Public Health Reports, 117(1), S82–S87. [PMC free article] [PubMed] [Google Scholar]
- National Institute on Drug Abuse. (2003). Preventing drug use among children and adolescents: A research-based guide for parents, educators, and community leaders (2nd ed.). Bethesda, MD: U.S. Department of Health and Human Services. [Google Scholar]
- Nigg CR, Anderson JK, Troumbley R, Alam MM, & Keller S (2013). Recent trends in adolescent alcohol use in Hawai‘i: 2005–2011. Hawai‘i Journal of Medicine & Public Health, 72(3), 92–98. [PMC free article] [PubMed] [Google Scholar]
- Nigg CR, Wagner A, Garza CM, & Goya D (2017). State Epidemiological Profile 2011–2015: Selected youth and adult drug indicators Retrieved from https://health.hawaii.gov/substance-abuse/files/2018/02/Adult-and-Youth-Drug.pdf [Google Scholar]
- Nishimura ST, Hishinuma ES, & Goebert D (2013). Underage drinking among Asian American and Pacific Islander adolescents. Journal of Ethnicity in Substance Abuse, 12(3), 259–277. doi: 10.1080/15332640.2013.805176 [DOI] [PubMed] [Google Scholar]
- NVivo 12 [Computer software] (2018). Melbourne, Australia: QSR International. [Google Scholar]
- Okamoto SK, Helm S, & Dustman PJ (2015). Ho‘ouna Pono Drug Prevention Curriculum: Teacher training manual (2nd ed.). Honolulu, HI: Hawai‘i Pacific University. [Google Scholar]
- Okamoto SK, Helm S, Giroux D, Edwards C, & Kulis S (2010). The development and initial validation of the Hawaiian Youth Drug Offers Survey (HYDOS). Ethnicity & Health, 15(1), 73–92. doi: 10.1080/13557850903418828 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okamoto SK, Helm S, Giroux D, Kaliades A, Kawano KN, & Kulis S (2010). A typology and analysis of drug resistance strategies of rural Native Hawaiian youth. The Journal of Primary Prevention, 31(5–6), 311–319. doi: 10.1007/s10935-010-0222-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okamoto SK, Helm S, & Kulis S (2015). Pilot and feasibility testing of the Ho‘ouna Pono drug prevention curriculum: 12-month follow up findings Paper presented at the Society for Prevention Research, Washington, D.C. [Google Scholar]
- Okamoto SK, Helm S, McClain LL, & Dinson AL (2012). The development of videos in culturally grounded drug prevention for rural Native Hawaiian youth. The Journal of Primary Prevention, 33(5–6), 259–269. doi: 10.1007/s10935-012-0281-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okamoto SK, Helm S, Ostrowski LK, & Flood L (2018). The validation of a school-based, culturally grounded drug prevention curriculum for rural Hawaiian youth. Health Promotion Practice, 19(3), 369–376. doi: 10.1177/1524839917704210 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okamoto SK, Kulis S, Helm S, Lauricella M, & Valdez JK (2016). An evaluation of the Ho‘ouna Pono curriculum: A pilot study of culturally grounded substance abuse prevention for rural Hawaiian youth. Journal of Health Care for the Poor and Underserved, 27(2), 815–833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okamoto SK, Kulis SS, Helm S, Chin SK, Hata J, Hata E, & Lee A (in press). An efficacy trial of the Ho‘ouna Pono drug prevention curriculum: An evaluation of a culturally grounded substance abuse prevention program for rural Native Hawaiian youth. Asian American Journal of Psychology [DOI] [PMC free article] [PubMed] [Google Scholar]
- Powell BJ, Proctor EK, & Glass JE (2014). A systematic review of strategies for implementing empirically supported mental health interventions. Research on Social Work Practice, 24(2), 192–212. doi: 10.1177/1049731513505778 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qina’au J (2016). BOE Policy E-3: Nā Hopena A’o (HĀ) Honolulu, HI: McREL International. [Google Scholar]
- Ramisetty-Mikler S, Caetano R, Goebert D, & Nishimura ST (2004). Ethnic variation in drinking, drug use, and sexual behavior among adolescents in Hawaii. Journal of School Health, 74(1), 16–22. [DOI] [PubMed] [Google Scholar]
- Skiba D, Monroe J, & Wodarski JS (2004). Adolescent substance use: Reviewing the effectiveness of prevention strategies. Social Work, 49(3), 343–353. [DOI] [PubMed] [Google Scholar]
- Strauss A, & Corbin J (1990). Basics of qualitative research Thousand Oaks, CA: Sage. [Google Scholar]
- The Danielson Group. (2017). The framework for teaching Retrieved from https://www.danielsongroup.org/framework/
- Tobler NS, & Stratton HH (1997). Effectiveness of school-based drug prevention programs: A meta-analysis of the research. The Journal of Primary Prevention, 18(1), 71–128. [Google Scholar]
- U.S. Department of Education. (2016). ESEA flexibility Retrieved from https://www2.ed.gov/print/policy/elsec/guid/esea-flexibility/index.html
- Waitzfelder BE, Engel CC, & Gilbert FI (1998). Substance abuse in Hawaii: Perspectives of key local human service organizations. Substance Abuse, 19(1), 7–22. [DOI] [PubMed] [Google Scholar]
- Waltz TJ, Powell BJ, Fernandez ME, Abadie B, & Damschroder LJ (2019). Choosing implementation strategies to address contextual barriers: Diversity in recommendations and future directions. Implementation Science, 14(42), 1–15. doi: 10.1186/s13012-019-0892-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weitzman EA (2000). Software and Qualitative Research. In Denzin NK & Lincoln YS (Eds.), Handbook of Qualitative Research (2nd ed., pp. 803–820). Thousand Oaks, CA: Sage. [Google Scholar]
- Wong MM, Klingle RS, & Price RK (2004). Alcohol, tobacco, and other drug use among Asian American and Pacific Islander Adolescents in California and Hawaii. Addictive Behaviors, 29(1), 127–141. doi: 10.1016/S0306-4603(03)00079-0 [DOI] [PubMed] [Google Scholar]