

Abstract
Background
Immediate postpartum intrauterine device (PPIUD) is a good solution for reducing low contraceptive coverage in developing countries. However, its use in HIV-infected women is poorly documented. The objective of this study was to assess whether the risk of PPIUD complications was higher in HIV-infected women.
Methods
A retrospective cohort study compared 64 HIV-infected women to 128 HIV-negative women who had had a PPIUD at the University Hospital of Treichville between January 2016 and March 2017, with a match at the insertion time of the PPIUD. The complications considered were pelvic pain, metrorrhagia and genital infections. Chi-squared test and relative risk were used to investigate the association between HIV infection and PPIUD complications.
Results
HIV-infected patients had an average age of 33.1 years, and 85.9% of them were on antiretroviral therapy. PPIUD was inserted during cesarean section in 66.1% of cases. There was no significant association between HIV infection and PPIUD complications (RR = 0.7, 95% CI [0.4–1.3], p = 0.3). The risk of genital infections was not increased in HIV-infected women (RR = 0.6 [0.1–2.7], p = 0.7).
Conclusion
HIV infection does not increase the risk of PPIUD complications. This effective contraceptive strategy can be offered to HIV-infected women. It is therefore necessary to strengthen the training of maternity staff in the installation of PPIUD.
Keywords: HIV, AIDS infection, PPIUD, Copper IUD, Complications
Introduction
In most sub-Saharan countries, the prevalence of HIV/AIDS among women of childbearing age and the maternal mortality ratio are at levels of concern. According to UNAIDS, nearly 60% of adults infected with HIV in this region are women of childbearing age [1]. In addition, this region alone accounts for more than half of all maternal deaths worldwide each year [2].
Family planning by preventing unwanted pregnancies prevents almost one-third of maternal deaths [3]. In HIV-infected women, effective contraception prevents maternal mortality and vertical transmission of HIV [4].
Almost all countries in sub-Saharan Africa have low contraceptive prevalence [5]. Thus, according to United Nations, modern contraceptive prevalence in Côte d'Ivoire was only 16.3% in 2017 [6].
Moreover, in these countries, few women return to the postnatal visit and the gravid-puerperium remains their main moment of contact with the reproductive health services. Hence in recent years the emphasis is laid on immediate postpartum contraception, including the intrauterine device (IUD) and implant, to increase contraceptive coverage in these developing countries. The IUD is a safe, effective and inexpensive contraceptive method with good acceptability in the immediate postpartum [7]. A Cochrane review also provided evidence regarding the safety and feasibility of the IUD inserted in the immediate postpartum period [8]. Previous studies have shown that the IUD is safe for women infected with stable HIV, that is, patients who have no opportunistic infection or coexisting infection in progress [9]. However, the IUD in these studies was not inserted in the immediate postpartum period. The objective of this study was therefore to assess whether the risk of complications after insertion of PPIUD was higher in HIV-infected women than in uninfected women.
Materials and Methods
This is a retrospective cohort study carried out in the obstetrics and gynecology department of the University Hospital of Treichville between January 2016 and March 2017. It focused on women who refused the use of condom during sexual intercourse but who accepted the insertion of a PPIUD with a follow-up of at least 6 weeks during the study period. The IUD used was TCu 380A, and the insertion was done in eligible patients after counseling. An ultrasound was performed 6 weeks after the insertion of the PPIUD to check its right location. Among these women, those who were HIV-infected were identified and compared to HIV-negative women with a matching time of insertion of the PPIUD and at a rate of 1 HIV-positive woman for 2 HIV-negative women.
The criteria for non-inclusion were as follows: lost to follow-up patients, cases of IUD expulsion, incomplete files and patients with advanced stages of the HIV infection (coexisting infection or an extremely low CD4 count).
The data needed for our study were collected using a standardized questionnaire from the birth registry and medical records. The variables studied included socio-demographic data and medical data related to HIV infection (and PPIUD). PPIUD complications that were sought were pelvic pain, bleeding and genital infections.
Diagnosis of genital infections was based on the following criteria: abnormal vaginal discharge with positive sexually transmitted infection from vaginal swabs or pelvic tenderness with at least one of the following signs: temperature above 38 °C and positive C-reactive protein.
Data analysis was performed using SPSS.22 software. The relationship between PPIUD complications and HIV infection was investigated using the Pearson Chi-squared test or Fischer’s exact test (when recommended). A p value < 0.05 was accepted as the significance level. The risk of PPIUD complications related to HIV infection was estimated by the calculation of relative risk with a 95% confidence interval (95% CI).
The study being retrospective, it was not necessary to have the consent of patients. However, their confidentiality has been respected.
Results
During the study period, 901 PPIUDs were inserted, 67 of which (that is 7.4%) in HIV-infected women. But 64 of them were involved in the analysis, with an eligibility rate of 95.5% (Fig. 1).
Fig. 1.
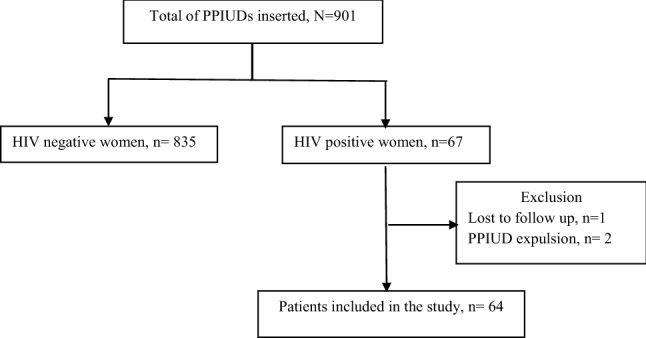
Enrollment process in the study
Table 1 presents the socio-demographic features of HIV-infected women in whom a PPIUD was inserted. Their mean age was 33.1 ± 5.8 years. They had a median parity of 3 with extremes at 0 and 7. Among them, 24 (37.5%) had scarred uterus.
Table 1.
Socio-demographic features of HIV-infected women with PPIUD (n = 64)
| Features | Number (N = 64) | Percentage (%) |
|---|---|---|
| Age (years) | ||
| < 20 | 1 | 1.6 |
| 20–29 | 21 | 32.8 |
| 30–39 | 36 | 56.2 |
| ≥ 40 | 6 | 9.4 |
| Parity | ||
| Primiparous (1 delivery) | 4 | 6.2 |
| Paucipara (2–3 deliveries) | 25 | 39.1 |
| Multiparous (≥ 4 deliveries) | 35 | 54.7 |
| Occupation | ||
| Liberal | 36 | 56.2 |
| Housewife | 20 | 31.3 |
| Employee | 6 | 9.4 |
| Pupil/student | 2 | 3.1 |
| School education level | ||
| Uneducated | 19 | 29.7 |
| Primary school level | 18 | 28.1 |
| Secondary school level | 20 | 31.3 |
| Higher level | 7 | 10.9 |
| Marital status | ||
| Single woman | 6 | 9.4 |
| Married woman | 58 | 90.6 |
| Scarred uterus | ||
| Yes | 24 | 37.5 |
| No | 40 | 62.5 |
The medical data of the infected women in whom a PPIUD was inserted are summarized in Table 2. For 53.1% of women, the HIV-positive status was known before pregnancy and 85.9% of them were on antiretroviral therapy. The IUD was inserted in the majority of them (65.6%) during cesarean section. The median duration of patients follow-up was 8 weeks (extremes at 6 and 24 weeks).
Table 2.
Medical data of HIV-infected women with PPIUDs (n = 64)
| Features | Number (N = 64) | Percentage (%) |
|---|---|---|
| Time of HIV testing | ||
| Before the current pregnancy | 34 | 53.1 |
| During the current pregnancy | 24 | 37.5 |
| At the maternity hospital | 6 | 9.4 |
| Antiretroviral therapy | ||
| Yes | 55 | 85.9 |
| No | 9 | 14.1 |
| CD4 count (elements/ml) | ||
| 200–349 | 7 | 10.9 |
| ≥ 350 | 45 | 70.3 |
| Unspecified | 12 | 18.8 |
| Mode of admission | ||
| Evacuated | 35 | 54.7 |
| Followed up in the department | 29 | 45.3 |
| Time of counseling for PPIUD | ||
| During prenatal consultations | 15 | 23.4 |
| In labor lag phase | 48 | 75.0 |
| Immediate postpartum | 1 | 1.6 |
| Time of insertion of PPIUD | ||
| Post-placental | 14 | 21.9 |
| Immediate postpartum | 8 | 12.5 |
| During cesarean section | 42 | 65.6 |
| Duration of follow-up | ||
| 8 weeks | 25 | 60.9 |
| ≥ 9 weeks | 39 | 39.1 |
The incidence of PPIUD complications was 18.7% in HIV-infected women versus 25.8% in the control group. This was a genital infection in two HIV-infected women (3.1%) and seven uninfected women (5.5%).
At the statistical analysis, HIV infection was not associated with a significant increase in the overall incidence of PPIUD complications (RR = 0.7 [0.4–1.3], p = 0.3). In addition, the risk of complications occurring in isolation was similar in both groups (Table 3).
Table 3.
Association between HIV infection and PPIUD complications
| PPIUD complications | Type of complications | |||||||
|---|---|---|---|---|---|---|---|---|
| Pain | Metrorrhagia | Genital infections | ||||||
| Yes | No | Yes | No | Yes | No | Yes | No | |
| HIV + (n = 64) | 12 (18.7%) | 52 | 8 | 56 | 2 | 62 | 2 | 62 |
| HIV − (n = 128) | 33 (25.8%) | 95 | 16 | 112 | 10 | 118 | 7 | 121 |
| RR [95% IC] | 0.7 [0.4–1.3] | 1 [0.4–2.2] | 0.4 [0.1–1.8] | 0.6 [0.1–2.7] | ||||
| p | 0.3 | 1.0 | 0.3 | 0.7 | ||||
RR relative risk, CI confidence interval, p p value
Discussion
In this study, HIV infection was not associated with increased risk of PPIUD complications. In fact, our analysis found that the rate of complications of PUPs in HIV-infected women and women without HIV was similar. Better still, the risk of genital infections after insertion of the PPIUD has not increased in HIV-infected women. There is insufficient data in the literature to assess the safety of the IUD inserted in the immediate postpartum period in HIV-infected women. The available data concern only the inserted IUD in HIV-infected women outside this critical period [10, 11]. Thus, a prospective cohort study assessed the risk of complications after insertion of the copper IUD in 156 HIV-infected women compared to 493 uninfected women in two family planning clinics in Nairobi. The authors noted that the risk of IUD complications was not significantly higher in HIV-infected women [12].
Furthermore, a controlled randomized trial comparing copper IUD and hormonal contraception for 2 years in 599 HIV-infected women showed that hormonal contraception was associated with a more rapid progression of HIV infection [13]. Unlike the copper IUD, hormonal contraceptives can affect the effectiveness of antiretrovirals through drug interactions [14, 15]. However, despite the lack of effect of the copper IUD on the course of HIV infection, it is recommended to limit its indications before the stage of AIDS disease [16].
These results demonstrate the safety of copper IUD in HIV-positive women in terms of the overall incidence of complications, incidence of genital infections and the progression of HIV infection. These results also indicate that PPIUD, is a deemed effective and safe contraceptive strategy, which may be appropriate for women living with HIV.
Conclusion
The benefits of safe and effective contraception for women living with HIV are enormous as they encompass the prevention of both maternal and pediatric AIDS. In this study, the insertion of PPIUD in HIV-positive women did not significantly increase the risk of IUD-related complications. In addition, HIV-infected women had no increased risk of developing genital infections after PPIUD insertion.
This study therefore suggests that IUD insertion in the immediate postpartum is safe for HIV-infected women. In an area of high prevalence of HIV infection such as ours, these results demonstrate that PPIUD should be considered as one of the appropriate contraceptive options for women living with HIV. This requires developing strategies to ensure the continued availability of IUDs in maternity hospitals and to train maternity care staff in counseling and PPIUD insertion. Further studies are needed to deepen the long-term impact of PPIUD on this population at risk.
Edouard N’guessan
is a professor-researcher at the Félix Houphouët-Boigny University, Abidjan Côte d'Ivoire. He is also a hospital practitioner in the department of Obstetrics and Gynecology, University Hospital of Treichville, Abidjan, Côte d’Ivoire and a focal point for the prevention of mother-to-child HIV transmission in this hospital. His research studies focus on HIV PMTCT, but also on the reproductive health of HIV-infected women. He is also interested in the epidemiological, clinical and prognostic particularities of cervical cancer in women living with HIV.
Compliance with Ethical Standards
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
None.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the institutional ethics committee and with the Declaration of Helsinki 1975, as revised in 2008 (5). Ethical consent for the work has been given by the ethical committee of our hospitals.
Informed Consent
Due to the retrospective nature of the study, patients’ consent was not required. However, the confidentiality of patients’ records was respected.
Footnotes
Edouard N’guessan is a Lecturer in Department of Obstetrics and Gynecology, Medical College and Research, Felix Houphouet-Boigny University in Abidjan, Côte d’Ivoire; Franck Gbeli is a resident in Department of Obstetrics and Gynaecology, University Hospital of Treichville, Abidjan, Côte d’Ivoire; Jean-Marc Dia is a Lecturer in Department of Obstetrics and Gynecology, Medical College and Research, Felix Houphouet-Boigny University, Abidjan, Côte d’Ivoire; Privat Guie is a Professor and Head of the Department of Obstetrics and Gynecology, University Hospital of Treichville, Abidjan, Côte d’Ivoire. Simplice Anongba is a honorary Professor and the past Head of the Department of Obstetrics and Gynecology, University Hospital of Treichville, Abidjan Côte d'Ivoire.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.UNAIDS . Fact sheet—latest statistics on the status of the AIDS epidemic. Geneva: UNAIDS; 2017. [Google Scholar]
- 2.Hogan MC, Foreman KJ, Naghavi M, et al. Maternal mortality for 181 countries, 1980–2008: a systematic analysis of progress towards millennium development goal 5. Lancet. 2010;375(9726):1609–1623. doi: 10.1016/S0140-6736(10)60518-1. [DOI] [PubMed] [Google Scholar]
- 3.Ahmed S, Li Q, Liu L, et al. Maternal deaths averted by contraceptive use: an analysis of 172 countries. Lancet. 2012;380(9837):111–125. doi: 10.1016/S0140-6736(12)60478-4. [DOI] [PubMed] [Google Scholar]
- 4.Sarnquist CC, Moyo P, Stranix-Chibanda L, et al. Integrating family planning and prevention of mother to child HIV transmission in Zimbabwe. Contraception. 2014;89(3):209–214. doi: 10.1016/j.contraception.2013.11.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Cahill N, Sonneveldt E, Stover J, et al. Modern contraceptive use, unmet need, and demand satisfied among women of reproductive age who are married or in a union in the focus countries of the family planning 2020 initiative: a systematic analysis using the family planning estimation tool. Lancet. 2018;391(10123):870–882. doi: 10.1016/S0140-6736(17)33104-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.United Nations (UN), Department of Economic and Social Affairs, Population Division. World Family Planning Highlights 2017. New York, UN; 2017. https://www.un.org/en/development/desa/population/publications/pdf/family/WFP2017_Highlights.pdf. Accessed 10 Aug 2019.
- 7.Pfitzer A, Mackenzie D, Blanchard H, et al. A facility birth can be the time to start family planning: postpartum intrauterine device experiences from six countries. Int J Gynecol Obstet. 2015;30:S54–S61. doi: 10.1016/j.ijgo.2015.03.008. [DOI] [PubMed] [Google Scholar]
- 8.Grimes D, Schulz K, Van Vliet H et al. Immediate postpartum insertion of intrauterine device: a systematic review. Cochrane Database Syst Rev. 2001(2):CD003036.
- 9.Kakaire O, Byamugisha JK, Tumwesigye NM, et al. Intrauterine contraception among women living with human immunodeficiency virus: a randomized controlled trial. Obstet Gynecol. 2015;126(5):928–934. doi: 10.1097/AOG.0000000000001087. [DOI] [PubMed] [Google Scholar]
- 10.Tepper NK, Curtis KM, Nanda K, et al. Safety of intrauterine devices among women with HIV: a systematic review. Contraception. 2016;94(6):713–724. doi: 10.1016/j.contraception.2016.06.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Haddad LB, Feldacker C, Jamieson DJ, et al. Medical eligibility, contraceptive choice, and intrauterine device acceptance among HIV-infected women receiving antiretroviral therapy in Lilongwe Malawi. Int J Gynaecol Obstet. 2014;126(3):213–216. doi: 10.1016/j.ijgo.2014.03.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Morrison CS, Sekadde-Kigondu C, Sinei SK, et al. Is the intrauterine device appropriate contraception for HIV-1-infected women? Br J Obstet Gynaecol. 2001;108:784–790. doi: 10.1111/j.1471-0528.2001.00204.x. [DOI] [PubMed] [Google Scholar]
- 13.Stringer EM, Kaseba C, Levy J, et al. A randomized trial of the intrauterine contraceptive device vs hormonal contraception in women who are infected with the human 8 infectious diseases in obstetrics and gynecology immunodefficiency virus. Am J Obstet Gynecol. 2007;197(2):144.e1–144.e8. doi: 10.1016/j.ajog.2007.03.031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Robinson JA, Jamshidi R, Burke AE. Contraception for the HIV-positive woman: a review of interactions between hormonal contraception and antiretroviral therapy. Infect Dis Obstet Gynecol. 2012;2012:890160. doi: 10.1155/2012/890160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Leticee N, Viard JP, Yamgnane A, et al. Contraceptive failure of etonogestrel implant in patients treated with antiretrovirals including efavirenz. Contraception. 2012;85(4):425–427. doi: 10.1016/j.contraception.2011.09.005. [DOI] [PubMed] [Google Scholar]
- 16.Vidal F, Paret L, Linet T, et al. Intrauterine contraception: CNGOF contraception guidelines. Gynecol Obstet Fertil Senol. 2018;46(12):806–822. doi: 10.1016/j.gofs.2018.10.004. [DOI] [PubMed] [Google Scholar]