

Introduction
Enterobius vermicularis is the most common human helminth infecting the intestine. Due to its low pathogenicity, infection is usually asymptomatic. Extraintestinal infections of E. vermicularis are extremely rare. The commonest extraintestinal site of infection is the female genital tract [1]. The male worm dies in the bowel during copulation, and the gravid female worm can migrate from the perianal region to the vagina and can ascend and reach peritoneum through the uterine cavity and fallopian tube. Various reports are available in the literature of the worm in the vagina, myometrium, endometrium, fallopian tube, ovary and pelvic peritoneum as well as an interesting incident of invasion of a human embryo [2–4].
Enterobius vermicularis infection is rarely reported to be associated with infertility. We report the detection of uterine endometrial E. vermicularis infestation in a woman who presented with primary infertility and subsequently conceived after treatment for the infection.
Case Report
A 38-year-old woman presented to our fertility clinic for evaluation of primary infertility. She was married for 15 years and had regular menstrual cycles. She had twice attempted intrauterine insemination unsuccessfully elsewhere. A hormonal assay showed normal results (FSH: 3.2 mIU/mL, LH: 5.5 mIU/mL, TSH: 1.6 mIU/mL, PRL: 7.03 ng/Ml and AMH: 1.2 ng/mL). An ultrasound evaluation revealed normal-appearing uterus and ovaries and a small right adnexal cyst. A sonohysterogram showed a normal uterine cavity, and a hysterosalpingogram confirmed the patency of both fallopian tubes. A semen analysis of her husband was also within normal limits.
An informed consent was obtained from the patient. She subsequently underwent hysterolaparoscopy. Laparoscopy revealed normal-appearing uterus and ovaries and a small fimbrial cyst which was excised. Histopathology evaluation suggested a paratubal cyst. On hysteroscopy, the uterine cavity appeared adequate. The endometrium, however, was looking irregular and polypoidal. Endometrial sampling was done and sent for histopathological evaluation which demonstrated the larvae of Enterobius vermicularis embedded within the endometrium (Figs. 1, 2). She was treated with a single dose of 400 mg of albendazole which was repeated after 2 weeks. In view of prolonged infertility and advanced age of the female, in vitro fertilization (IVF) was offered which resulted in a successful conception. She is into the sixth month of pregnancy at the moment.
Fig. 1.
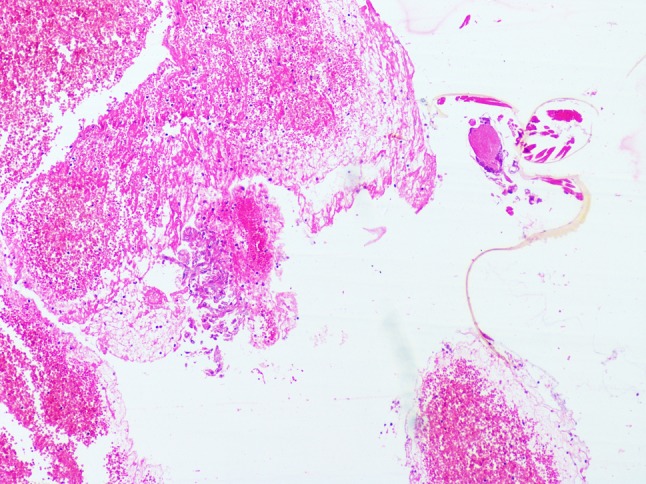
Hematoxylin & eosin stain of the endometrial sample showing E. vermicularis larva
Fig. 2.
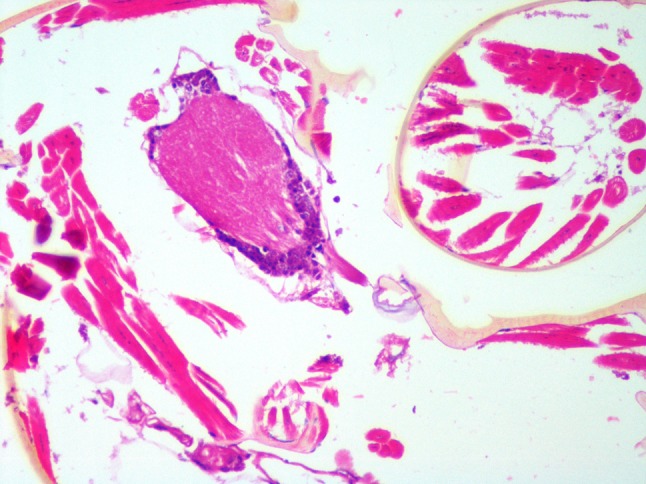
Hematoxylin & eosin stain of the endometrial sample showing the larva of E. vermicularis with its outer chitinous layer and internal organs
Discussion
Enterobiasis caused by E. vermicularis is one of the most common helminthic infestations of the cecum and adjacent gut. Ingestion of eggs present in the contaminated hands or food results in infection by this pinworm [2]. Scratching the perianal skin where the female worm has laid eggs results in hand contamination. The gravid female worm can migrate from the perianal area to the vagina and ascend through the fallopian tube to the peritoneum [3]. The worm can also pass through the intestinal wall and cause pelvic peritoneal granuloma. Such navigation by the larval and adult parasite can result in fallopian tube infiltration, tubo-ovarian abscess, salpingooophoritis or granulomata of the vulva, vagina, uterus, fallopian tubes or ovaries and rarely destruction of the human embryo [4].
Enterobius vermicularis granulomas do not usually cause clinical problems and are incidental findings. They have been reported to cause vulvovaginitis and can masquerade as cervical and endometrial carcinoma. Involvement of the pelvic peritoneum and the fallopian tube resulting in infertility has been reported [5, 6]. Ours is the first instance of uterine endometrial infection with the worm resulting in infertility. Since the patient has never undergone IVF before, the causality of this association cannot be established. The presence of unexplained infertility and its reversal after treatment of worm infestation may suggest causality. The diffuse endometrial inflammation caused by the worm could interfere with implantation and thus cause infertility. The subtle uterine irregularity was visible only on hysteroscopy.
Our case highlights the importance of ectopic enterobiasis in female reproductive ill health, especially in the tropical countries. In addition to the previously reported instances of ectopic enterobiasis-related pelvic inflammatory disease and tubal infection resulting in infertility, uterine endometrial involvement by the worm also seems to be another potential cause for infertility. Co-infection with other bacteria from the intestine and skin is another major concern as they seem to move to these sites along with the pinworm and contribute toward infection and inflammation [7]. We stress on the importance of close observation of the uterine cavity through hysteroscopy in all cases of prolonged unexplained infertility. An endometrial sampling can identify the pinworm infection and allow treatment which might restore fertility.
Dr. Hema Rajesh
is a consultant in the Department of Fertility and Reproductive Medicine, PSG Institute of Medical Sciences and Research, Coimbatore. After her post-graduation in Obstetrics and Gynecology, she completed her fellowship in Reproductive Medicine conducted by the National Board of Examinations. She established the Fertility Department at the PSG Hospitals. She has presented papers in many national and international conferences and is interested in clinical research.
Compliance with Ethical Standards
Conflict of interest
None.
Ethical Statement
This work has not been published before; it is not under consideration for publication anywhere else; its publication has been approved by all co-authors, as well as by the responsible authorities.
Footnotes
Dr. Hema Rajesh, Consultant in Reproductive Medicine, Department of Fertility & Reproductive Medicine, PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu, India. Balu Kuppusamy, Consultant Surgical Gastroenterologist in PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu, India. Chaitra Venkataswamy, Clinical Pathologist in PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu, India. Nidhya Ganesan, Clinical Pathologist in PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu, India.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Sizer AR, Nirmal DM, Shannon J, Davies NJ. A pelvic mass due to infestation of the fallopian tube with Enterobius vermicularis. J Obstet Gynaecol. 2004;24:462–463. doi: 10.1080/01443610410001696923. [DOI] [PubMed] [Google Scholar]
- 2.Erhan V, Zekioglu O, Ozdemir N, Sen S. Unilateral salpingitis due to Enterobius vermicularis. Int J Gynecol Pathol. 2000;19:188–189. doi: 10.1097/00004347-200004000-00017. [DOI] [PubMed] [Google Scholar]
- 3.Smolyakov R, Talalay B, Yanai-Inbar I, et al. Enterobius vermicularis infection of female genital tract: a report of three cases and review of the literature. Eur J Obstet Gynecol Reprod Biol. 2003;107:220–222. doi: 10.1016/S0301-2115(03)00003-4. [DOI] [PubMed] [Google Scholar]
- 4.Mendoza E, Jorda M, Rafel E, Simón A, Andrada E. Invasion of human embryo by Enterobius vermicularis. Arch Pathol Lab Med. 1987;111:761–762. [PubMed] [Google Scholar]
- 5.Neri A, Tadir Y, Grausbard G, Pardo J, Ovadia J, Braslavsky D. Enterobius (Oxyuris) vermicularis of the pelvic peritoneum—a cause of infertility. Eur J Obstet Gynecol Reprod Biol. 1986;23:239–241. doi: 10.1016/0028-2243(86)90153-X. [DOI] [PubMed] [Google Scholar]
- 6.Young C, Tataryn I, Kowalewska-Grochowska KT, Balachandra B. Enterobius vermicularis infection of the fallopian tube in an infertile female. Pathol Res Pract. 2010;206(6):405–407. doi: 10.1016/j.prp.2009.11.003. [DOI] [PubMed] [Google Scholar]
- 7.Siteti MC, Injete SD, Wanyonyi WA. Helminthiases: a neglected cause for reproductive ill-health and social stigma. Parasitol United J. 2015;8:87–94. doi: 10.4103/1687-7942.175003. [DOI] [Google Scholar]