

Abstract
Background
Hepatocellular carcinoma is the most common liver neoplasm and the sixth most common cancer worldwide. Its incidence has increased dramatically since the mid‐2000s. Although surgical resection and liver transplantation are the main curative treatments, only about 20% of people with early hepatocellular carcinoma may benefit from these interventions. Treatment options for unresectable hepatocellular carcinoma include ablative and transarterial interventions ‐ selective yttrium‐90 microsphere transarterial radioembolisation ‐ in addition to the drug sorafenib.
Objectives
To determine the benefits and harms of yttrium‐90 (Y‐90) microsphere transarterial radioembolisation given as monotherapy or in combination with other systemic or locoregional interventions versus placebo, no treatment, or other similar systemic or locoregional interventions for people with unresectable hepatocellular carcinoma.
Search methods
We performed electronic searches in the Cochrane Hepato‐Biliary Group (CHBG) Controlled Trials Register, CENTRAL, MEDLINE, Embase, Latin American Caribbean Health Sciences Literature (LILACS), Science Citation Index ‐ Expanded, and Conference Proceedings Citation Index – Science until September 2019. We manually checked the reference lists of primary studies and review articles.
Selection criteria
We searched for randomised clinical trials.
Data collection and analysis
We used standard Cochrane methods. We extracted information on participants, interventions, outcomes, trial design, and trial methods. We assessed risk of bias of the included trials using pre‐defined domains and the certainty of evidence using GRADE. Our primary review outcomes were all‐cause mortality, quality of life, and serious adverse events; our secondary outcomes were cancer‐related mortality, time to progression of the tumour, tumour response, non‐serious adverse events, and liver transplantation. For dichotomous variables, we calculated risk ratio (RR), and for continuous variables, we planned to calculate mean difference (MD) or standardised mean difference (SMD), with 95% confidence intervals (CIs). We based time‐to‐event data analyses on hazard ratios (HRs).
Main results
Six randomised trials with 1340 participants in total fulfilled the review inclusion criteria and provided data for one or more of our analysed outcomes. All trials were at high risk of bias. We assessed the certainty of evidence as low to very low.
One trial compared radioembolisation plus sorafenib versus sorafenib alone in people with advanced hepatocellular carcinoma. All‐cause mortality, health‐related quality of life, cancer‐related mortality, time to progression, and tumour response rates were not reported. Serious adverse events were reported in 63 trial participants (39.6%) in the radioembolisation plus sorafenib group versus 70 trial participants (38.5%) in the sorafenib group (very low‐certainty evidence). Hyperbilirubinaemia was approximately three times more common in the radioembolisation plus sorafenib group versus the sorafenib group (14.5% versus 4.4%; very low‐certainty evidence). Fatigue was more common in the radioembolisation plus sorafenib group than in the sorafenib group, at 35.2% versus 24.2% of trial participants. Two trials compared radioembolisation versus sorafenib for unresectable hepatocellular carcinoma in people with locally advanced hepatocellular carcinoma. From the data we could extract, one‐year all‐cause mortality was 62.7% in the radioembolisation group versus 53.0% in the sorafenib group (1 trial; n = 360; very low‐certainty evidence). There were no differences in the quality of life between radioembolisation and sorafenib groups (1 trial). Global health status subscore was better in the radioembolisation group than in the sorafenib group (P = 0.0048; 1 trial). Fewer participants had serious adverse events in the radioembolisation group than in the sorafenib group (27 (20.8%) in the radioembolisation group versus 57 (35.2%) in the sorafenib group; 1 trial). Median time to progression of the tumour in the radioembolisation group was 6.1 months versus 5.4 months in the sorafenib group (1 trial). The RR for disease control rate was 0.94 (95% CI 0.84 to 1.05; n = 748; 2 trials; very low‐certainty evidence), favouring neither radioembolisation nor sorafenib. In two trials with 734 participants, radioembolisation seemed to be less likely to be associated with hand‐foot skin reaction (RR 0.02, 95% CI 0.00 to 0.06; P < 0.001; low‐certainty evidence), skin rash (RR 0.11, 95% CI 0.04 to 0.34; low‐certainty evidence), diarrhoea (RR 0.11, 95% CI 0.04 to 0.34; low‐certainty evidence), and hypertension (RR 0.10, 95% CI 0.01 to 0.88; low‐certainty evidence). No trial reported cancer‐related mortality. Three trials compared radioembolisation versus chemoembolisation in people with intermediate‐stage hepatocellular carcinoma. From the data we could extract, none of these trials reported all‐cause mortality and cancer‐related mortality. The RR for serious adverse events was 1.41 (95% CI 0.63 to 3.14; n = 97; very low‐certainty evidence), favouring neither radioembolisation nor chemoembolisation. One trial reported quality of life and noted no differences between intervention groups with regard to this outcome at week 12 (very low‐certainty evidence). Median time to progression was not reached in the radioembolisation group and was 6.8 months in the chemoembolisation group (HR 0.122, 95% CI 0.027 to 0.557; 1 trial). Median time to progression of the tumour in the radioembolisation group was 371 days versus 336 days in the chemoembolisation group (P = 0.5764; 1 trial). Disease control rates (complete response + partial response + stable disease) were 73.3% with radioembolisation versus 76.9% with chemoembolisation (1 trial). According to World Health Organization (WHO) criteria, tumour response was reported in 52% of participants who received radioembolisation versus 63% of those who received chemoembolisation (1 trial). Patients in the chemoembolisation group experienced diarrhoea (P = 0.031; 1 trial) and hypoalbuminaemia (P < 0.001; 1 trial) more frequently.
Four trials were sponsored by industry, and two by University.
We found two ongoing trials.
Authors' conclusions
Evidence showing effects of radioembolisation with or without sorafenib compared with sorafenib alone in people with unresectable hepatocellular carcinoma is highly insufficient. We cannot determine if radioembolisation plus sorafenib compared with sorafenib alone affects all‐cause mortality or the occurrence of adverse events. Radioembolisation compared with sorafenib seemed to achieve equivalent survival and to cause fewer adverse effects, but our certainty was very low. Evidence showing effects of radioembolisation versus chemoembolisation in people with unresectable hepatocellular carcinoma is also highly insufficient. Radioembolisation did not seem to differ from chemoembolisation in terms of serious adverse events and quality of life, but the certainty of evidence was very low. Further high‐quality placebo‐controlled randomised clinical trials are needed to assess patient‐centred outcomes.
Plain language summary
Yttrium‐90 microsphere radioembolisation for advanced hepatocellular carcinoma (primary liver cancer)
Review question
What are the benefits and harms of yttrium‐90 microsphere radioembolisation compared with placebo, no intervention, or other available interventions in people with advanced liver cancer?
Background Hepatocellular carcinoma (i.e. primary liver cancer) is the most common malignant tumour of the liver and the fifth most common malignant tumour worldwide. In the majority of people, hepatocellular carcinoma is diagnosed at an advanced stage. For these people, treatment options include ablation therapy (which destroys the tumour), embolisation therapy (which uses substances to block or decrease the flow of blood through the hepatic artery to the tumour), radiotherapy, and sorafenib (targeted therapy that uses a substance to identify and attack cancer cells while avoiding normal cells). Yttrium microsphere radioembolisation involves injection into the blood supply of the tumour very small spheres that have radioactive material attached to them. The radioactivity is supposed to destroy the liver tumour without affecting other parts of the body.
Study characteristics Review authors searched for published medical articles to clarify the role of yttrium microsphere radioembolisation in the treatment of people with advanced liver cancer. Review authors looked for randomised clinical trials (where people were allocated at random to one of two or more treatments groups) to perform statistical analysis on which they could form conclusions about the intervention. Evidence is current to September 2019.
Funders and funding collaborators of these studies were Bayer, Sirtex Medical, Johannes Gutenberg University Mainz, and Northwestern University.
We also identified two ongoing randomised trials evaluating the topic of our review. One of them compared radioembolisation with chemoembolisation in intermediate‐stage hepatocellular carcinoma, and the other compared radioembolisation plus sorafenib versus sorafenib alone in advanced hepatocellular carcinoma.
Key results Review authors found six randomised clinical trials, in which 1340 people with advanced liver cancer were randomised. One trial compared radioembolisation plus sorafenib versus sorafenib alone. This trial suggested that combination treatment for this disease seems to be associated with similar risk of death compared with use of sorafenib alone. Two trials compared radioembolisation with sorafenib. There seems to be no difference in the risk of death between these interventions. Three trials compared radioembolisation with chemoembolisation. There seems to be no difference in serious toxicities between these interventions. Review authors identified two ongoing randomised clinical trials, the results of which have not been finalised.
Certainty of the evidence and conclusions
Evidence for the benefits and harms of radioembolisation with or without sorafenib and compared with sorafenib alone in people with unresectable hepatocellular carcinoma is highly insufficient. We cannot determine if radioembolisation plus sorafenib compared with sorafenib alone affects the occurrence of adverse events. Radioembolisation compared with sorafenib seemed to achieve equivalent survival and to cause fewer adverse effects, but our certainty is very low. Evidence for the benefits and harms of radioembolisation versus chemoembolisation in people with unresectable hepatocellular carcinoma is also highly insufficient. Radioembolisation did not seem to differ from chemoembolisation in terms of serious adverse events and health‐related quality of life, but the certainty of evidence was very low. Additional well‐performed and high‐quality placebo‐controlled randomised clinical trials are needed to assess patient‐centred outcomes.
Summary of findings
Background
Description of the condition
Hepatocellular carcinoma is the most common liver neoplasm and the sixth most common cancer worldwide (Graham 2013). Its incidence has increased dramatically since the mid‐2000s, and hepatitis C virus and hepatitis B virus infections are considered the most important risk factors for this disease (Schiefelbein 2012; Abdel‐Rahman 2013).
The aetiology of liver disease, and hence of hepatocellular carcinoma, differs geographically. In most areas, chronic viral hepatitis (due to either hepatitis B virus or hepatitis C virus) is the main cause of hepatocellular carcinoma (Masuzaki 2009). Approximately 340,000 liver cancers (54.4% globally) are attributable to hepatitis B virus and hepatitis C virus infection, with the majority of these in Africa, Asia, and the Western Pacific region (Sanyal 2010). In addition, chronic alcohol consumption plays an important role in the development of both cirrhosis and hepatocellular carcinoma. Older people, males, people with hepatitis C virus infection, and people who consume excessive amounts of alcohol are at higher risk for developing hepatocellular carcinoma after alcoholic cirrhosis (Kwon 2012).
The diagnosis of hepatocellular carcinoma may be made by biopsy or necropsy. Growing evidence suggests that non‐invasive diagnostic modalities may be used to make the diagnosis of hepatocellular carcinoma with high predictive values (Bartlett 2008). According to guidelines from the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver (Bruix 2011; EASL/EORTC 2012), hepatocellular carcinoma diagnosis can be based on biopsy or on imaging techniques fulfilling some well‐defined criteria. However, modification of the diagnostic algorithm and differing sensitivities of some tools, such as magnetic resonance imaging (MRI), could introduce some heterogeneity in the classification of patients and in the prognostic assessment (Bruix 2011).
Many staging systems have been advocated for prognostic classification of hepatocellular carcinoma. These include the American Joint Committee for Cancer staging system, the Okuda system, the Cancer of the Liver Italian Program system, and the Barcelona Clinic Liver Cancer system (Okuda 1985; Levy 2002; Liu 2014). The Barcelona Clinic Liver Cancer system is the most widely used system among specialists dealing with hepatocellular carcinoma worldwide, as it combines patient‐related factors (Eastern Cooperative Oncology Group performance score), tumour‐related factors, and liver disease‐related factors (Child‐Pugh class), and it has been endorsed by the American Association for the Study of Liver Disease, as well as the European Association for the Study of the Liver (Bruix 2011). Following the Barcelona Clinic Liver Cancer system, hepatocellular carcinoma has five stages: (1) 0 ‐ very early stage; single nodule < 3 cm; Child‐Pugh class A; Eastern Cooperative Oncology Group (ECOG) performance status: 0; (2) A ‐ early stage; one to three nodules, all < 3 cm; Child‐Pugh class A or B; ECOG performance status: 0; (3) B ‐ intermediate stage; multi‐nodular tumour; Child‐Pugh class A or B; ECOG performance status: 0; (4) C ‐ advanced stage; portal invasion and extra‐hepatic spread; Child‐Pugh class A or B; ECOG performance status: 1 or 2; and (5) D ‐ terminal stage; severe liver damage; Child‐Pugh class C; ECOG performance status: 3 or 4 (Medscape 2018).
Current effective treatment options for hepatocellular carcinoma include liver resection, transplantation, and various local ablative and transarterial interventions, as well as sorafenib for advanced or metastatic (or both) disease (Oliveri 2011; Weis 2013). Although surgical resection and liver transplantation are the main curative treatments, only around 20% of people with very early and early disease ‐‐ most often diagnosed by regular screening ‐‐ may benefit from these interventions (Yau 2008; Abdel‐Rahman 2013).
Despite improvement in survival following surgical resection or transplantation, the incidence of tumour recurrence and associated mortality is high (Mazzaferro 1996). Therefore, most people with unresectable or recurrent disease are eventually relegated for consideration of various forms of local‐regional in situ cytoreductive treatments.
Description of the intervention
Yttrium‐90 (Y‐90) microsphere radioembolisation is a promising outpatient transarterial therapy for unresectable hepatocellular carcinoma (Venkatanarasimha 2017). It is a very specialised procedure that shares characteristics of radiopharmaceuticals and a radiation therapy source, requiring multi‐disciplinary involvement. Knowledge of technical aspects of embolisation, hepatic artery anatomy, and flow characteristics is essential for safe and effective delivery of this new intervention. Published data from multiple independent sources support enhancement of survival in a distinct subset of people with hypervascular tumours and intact liver function (Rhee 2005; Kulik 2006; Saini 2019). Unlike what is considered a contraindication for other embolointerventions, portal vein thrombosis is not considered to be a major contraindication for Y‐90 radioembolisation. This intervention seems an effective instrument for downstaging the tumour to resection or providing a bridge to liver transplantation. Compared to historical controls, the post‐embolisation syndrome following Y‐90 microsphere radioembolotherapy is milder than following chemoembolisation (Murthy 2011; Saini 2019).
Two products are commonly available for Y‐90 microsphere radioembolisation: TheraSphere and SIR‐Spheres. SIR‐Spheres have much lower specific activity per particle and result in a much higher embolic load than TheraSpheres. SIR‐Spheres are not preferred in people with portal vein thrombosis. In contrast, TheraSpheres have high specific activity and a much lower embolic load per treatment (D'Avola 2009; Lewandowski 2009; Salem 2010).
How the intervention might work
Although external beam radiotherapy represents a very effective tumoricidal modality for hepatocellular carcinoma, it has limited applicability because of intrinsic low radiation tolerance of the innocent bystander 'normal' liver tissue (Abdel‐Rahman 2013). Therefore, use of techniques that circumvent this limitation of external radiotherapy is important to enhance clinical outcomes. One such method exploits the preferential arterial flow and enhanced microvascular density of hepatic neoplasia that is central to the efficacy of other more common transarterial interventions such as hepatic artery chemoembolisation (Abdel‐Rahman 2018). Biocompatible microspheres acting as carriers can conceptually deliver radiation preferentially to tumours following hepatic artery delivery via embolisation in the tumour‐related vessels. Furthermore, employing high‐energy beta radiation as opposed to a traditional gamma radiation would create an intense local radiotherapeutic effect that is proportionate to the density of microsphere distribution. Y‐90 that is incorporated on appropriately calibrated microspheres fulfils these criteria as the prototypical device that has been used for decades for treatment of hepatic neoplasia including hepatocellular carcinoma.
Why it is important to do this review
Despite encouraging data for radioembolisation in hepatocellular carcinoma, some international organisations are reluctant to incorporate it into official guidelines due to lack of clear level one evidence of efficacy. Thus, we think that the conduct of well‐designed systematic reviews and health technology assessments based on well‐conducted randomised clinical trials is of paramount significance to assess the benefits and harms of this new technology.
Objectives
To determine the benefits and harms of yttrium‐90 (Y‐90) microsphere transarterial radioembolisation given as monotherapy or in combination with other systemic or locoregional interventions versus placebo, no treatment, or other similar systemic or locoregional interventions for people with unresectable hepatocellular carcinoma.
Methods
Criteria for considering studies for this review
Types of studies
We sought to identify all randomised clinical trials comparing Y‐90 microsphere radioembolisation versus placebo, no treatment, or similar systemic or locoregional interventions for unresectable hepatocellular carcinoma. We did not limit our search for randomised clinical trials in terms of language or year of publication.
During the selection of trials, when we identified observational studies (e.g. quasi‐randomised studies, cohort studies, case reports) that reported adverse events during the study period, we read these studies for a narrative review of the reported adverse events only. We did not specifically search for observational studies for inclusion in this review, which is a limitation. We are conscious that by not looking for all observational studies on adverse events, we allow the risks of putting greater emphasis on potential benefits than on potential harms, and of overlooking uncommon and late adverse events (Storebø 2018).
Types of participants
We included all trial participants with histologically or radiologically diagnosed unresectable hepatocellular carcinoma who were older than 18 years.
Types of interventions
We included Y‐90 microsphere radioembolisation versus placebo, no treatment, or systemic or locoregional interventions.
Co‐interventions were allowed if administered equally to all trial intervention groups.
Types of outcome measures
Primary outcomes
All‐cause mortality (which can be reported as median overall survival)
Quality of life as reported by participants and as assessed by standard grading systems (e.g. Functional Assessment of Cancer Therapy‐Hepatobiliary) (FACT‐Hep 2007)
Serious adverse events as defined by the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use (ICH) Guidelines for Good Clinical Practice, as any untoward medical occurrence that at any dose resulted in death, was life‐threatening, required hospitalisation or prolongation of existing hospitalisation, resulted in persistent or significant disability or incapacity, or was a congenital anomaly/birth defect, or any medical event that might have jeopardised the person or required intervention to prevent it (ICH‐GCP 1997)
Secondary outcomes
Cancer‐related mortality
Time to progression of the tumour (reported as median time to progression)
-
Tumour response assessments as recommended by the response evaluation in solid tumours criteria (Eisenhauer 2009)
Complete response: disappearance of all target lesions. Any pathological lymph nodes (whether target or non‐target) must have reduction in the short axis to less than 10 mm
Partial response: at least a 30% decrease in the sum of diameters of target lesions, taking as reference the baseline sum diameters
Progressive disease: at least a 20% increase in the sum of diameters of target lesions, taking as reference the smallest sum on study (this included the baseline sum if that was the smallest on study). In addition to the relative increase of 20%, the sum must have demonstrated an absolute increase of at least 5 mm (note: the appearance of one or more new lesions was also considered as progression)
Stable disease: neither sufficient shrinkage to qualify for partial response nor sufficient increase to qualify for progressive disease, taking as reference the smallest sum diameters while on study
In addition, we considered the European Association for the Study of the Liver disease response evaluation criteria and the World Health Organization response evaluation criteria, and we considered the positron emission tomography Response Criteria in Solid Tumors when appropriate (Choi 2005; Riaz 2011; Maffione 2013; EASL 2018).
Non‐serious adverse events: any medical occurrences not necessarily having a causal relationship with the treatment but causing dose reduction or discontinuation of treatment.
Liver transplantation following treatment.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Hepato‐Biliary Group Controlled Trials Register (maintained and searched internally by the CHBG Information Specialist via the Cochrane Register of Studies Web; September 2019); the Cochrane Central Register of Controlled Trials (CENTRAL; 2019; Issue 9), in the Cochrane Library; MEDLINE Ovid (1946 to September 2019); Embase Ovid (1974 to Spetember 2019); Latin American Caribbean Health Sciences Literature (LILACS) (Bireme; 1982 to September 2019); Science Citation Index ‐ Expanded (Web of Science; 1900 to September 2019); and Conference Proceedings Citation Index – Science (Web of Science; 1990 to September 2019) (Royle 2003). We searched all the listed databases from their date of inception onwards to September 2019. Appendix 1 shows the search strategies with time spans for searches of the various databases. An additional search for ongoing and completed trials within the clinicaltrials.gov registry and WHO Clinical Trials Registry was done up to September 2019.
Searching other resources
We checked the reference lists of primary original studies and review articles manually for further related articles (cross‐references).
Data collection and analysis
We performed the review according to the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We performed data analyses using the Cochrane statistical software, Review Manager 5 (Review Manager 2014). We resolved any discordance by consensus.
Selection of studies
Review authors, independently of each other, identified the trials for inclusion.
We excluded duplicate records based on review of titles. We reviewed abstracts of the remaining articles. We went through the full text of the remaining articles for relevancy to the review. We listed the excluded studies with the reasons for exclusion.
Data extraction and management
We extracted the data individually. We extracted details of study population, interventions, and outcomes using a standardised data extraction form, which included the following items.
Publication year.
Country.
Year the trial was conducted.
Inclusion and exclusion criteria.
Whether the trial performed sample size calculation.
Population characteristics such as age and sex ratios.
Baseline characteristics including Child‐Pugh class, Eastern Cooperative Oncology Group Performance Status, Barcelona Clinic Liver Cancer stage, and proportions of participants positive for hepatitis B and C virus.
Outcomes (Types of outcome measures).
Risk of bias (Assessment of risk of bias in included studies).
Whether the trial performed an intention‐to‐treat analysis.
Assessment of risk of bias in included studies
Two review authors independently assessed the risk of bias of each potentially included trial according to the recommendations from the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
We used the following definitions in the assessment of risk of bias (Schulz 1995; Moher 1998; Kjaergard 2001; Wood 2008; Savović 2012a; Savović 2012b; Savović 2018).
Allocation sequence generation
Low risk of bias: sequence generation was achieved using computer random number generation or a random numbers table. Drawing lots, tossing a coin, shuffling cards, and throwing dice were adequate if performed by an independent person not otherwise involved in the trial
Unclear risk of bias: the method of sequence generation was not specified
High risk of bias: the sequence generation method was not random
Allocation concealment
Low risk of bias: participant allocations could not have been foreseen in advance of, or during, enrolment. Allocation was controlled by a central and independent randomisation unit. The allocation sequence was unknown to the investigators (e.g. the allocation sequence might have been hidden in sequentially numbered, opaque, and sealed envelopes)
Unclear risk of bias: the method used to conceal the allocation was not described so that intervention allocations may have been foreseen in advance of, or during, enrolment
High risk of bias: the allocation sequence was likely to be known to the investigators who assigned participants
Blinding of participants and personnel
Low risk of bias: it was mentioned that both participants and personnel providing the interventions were blinded, and the method of blinding was described, so that knowledge of allocation was prevented during the trial
Unclear risk of bias: it was not mentioned if the trial was blinded, or the trial was described as blinded, but the method or extent of blinding was not described, so that knowledge of allocation was possible during the trial
High risk of bias: the trial was not blinded, so that allocation was known during the trial
Blinded outcome assessment
Low risk of bias: outcome assessment was carried out blinded for all relevant outcomes, and the method of blinding was described, so that knowledge of allocation was prevented
Unclear risk of bias: blinding of outcome assessment was not described, or the outcome assessment was described as blinded but the method of blinding was not described, so that knowledge of allocation was possible
High risk of bias: outcome assessment was not blinded, so that allocation was known to outcome assessors
Incomplete outcome data
Low risk of bias: missing data were unlikely to make treatment effects depart from plausible values. Sufficient methods, such as multiple imputation, were employed to handle missing data
Unclear risk of bias: information was insufficient to assess whether missing data in combination with the method used to handle missing data were likely to induce bias on the results
High risk of bias: results were likely to be biased due to missing data
Selective outcome reporting
Low risk of bias: the trial reported the following pre‐defined outcomes: all‐cause mortality, serious adverse events, and cancer‐related mortality. If the original trial protocol was available, the outcomes should be those called for in that protocol. If the trial protocol was obtained from a trial registry (e.g. www.clinicaltrials.gov), the outcomes sought should have been those enumerated in the original protocol if the trial protocol was registered before or at the time that the trial was begun. If the trial protocol was registered after the trial was begun, those outcomes will not be considered to be reliable
Unclear risk of bias: not all pre‐defined outcomes were reported fully, or it was unclear whether data on these outcomes were recorded or not
High risk of bias: one or more pre‐defined outcomes were not reported
We considered a trial at 'low risk of bias' if assessed as 'low risk of bias' in all specified individual domains. We considered a trial at 'high risk of bias' if assessed as having 'unclear risk of bias' or 'high risk of bias' in one or more of the specified individual domains.
We discussed any disagreements between us, and we intended to contact the authors of the trial if consensus was needed.
Measures of treatment effect
For dichotomous variables, we calculated risk ratios (RRs) with 95% confidence intervals (CIs). For continuous variables, we planned to calculate mean differences (MDs) or standardised mean differences (SMDs) with 95% CIs. Time‐to‐event data analyses are usually based on hazard ratios (HRs); so when these data were provided, we used HRs. If HR data were not provided, we planned to calculate the ln(HR) and its standard error indirectly, or we planned to use a computer software for obtaining the exact HRs (Parmar 1998). When the results of health‐related quality of life were reported through different scales in different studies, we reported the results of each study independently, and we did not plan to combine the results.
We undertook meta‐analyses only when this was meaningful (i.e. when treatments, participants, and the underlying clinical question were similar enough for a meta‐analysis to make sense, and when the data were accurate).
Unit of analysis issues
The unit of analysis is the group of participants per intervention group for randomised clinical trials with parallel‐group design. For trials with multiple intervention groups, we planned to collect data for all trial intervention groups that meet our inclusion criteria. We planned to divide the control group into two to avoid double‐counting, in case this was a common comparator (this did not happen because neither of the included trials was a multiple‐intervention trial). In the case of cross‐over trials, we planned to use data from the first trial period only (this did not happen because neither of the included trials was a cross‐over trial).
Dealing with missing data
When data could not be extracted from the text, or when a statistic was missing, we contacted the authors of the original article to request the necessary information.
Intention‐to‐treat analyses
We performed our analyses based on the intention‐to‐treat principle, whenever possible. Regarding the primary outcomes, we planned to include participants with incomplete or missing data in sensitivity analyses by imputing them according to the following scenarios (Hollis 1999).
Extreme case analysis favouring the experimental intervention ('best‐worse' case scenario): none of the dropouts/participants lost from the experimental group, but all of the dropouts/participants lost from the control group, experienced the outcome, including all randomised participants in the denominator.
Extreme case analysis favouring the control ('worst‐best' case scenario): all dropouts/participants lost from the experimental group, but none lost from the control group, experienced the outcome, including all randomised participants in the denominator.
Because of the nature of the clinical trials included in the review, we could not conduct any of the above extreme case analyses.
Assessment of heterogeneity
We used the Chi² test to obtain an indication of between‐trial heterogeneity. In addition, we quantified the degree of heterogeneity observed in the results using the I² statistic, which can be interpreted as the percentage of variation observed between trials attributable to between‐trial differences rather than to sampling error (chance). We planned to perform a subgroup analysis to compare the intervention effect in trials with low risk of bias to that in trials with unclear or high risk of bias. We based analyses on intention‐to‐treat data (when allowed by published data).
Assessment of reporting biases
We carried out a comprehensive search to minimise publication bias. If we had identified a sufficient number of trials for inclusion (at least 10 trials), we planned to use a funnel plot to explore bias (Egger 1997; Macaskill 2001).
Data synthesis
Review authors followed instructions on data synthesis obtained from the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Meta‐analysis
For meta‐analyses, we used a random‐effects model as well as a fixed‐effect model (Mantel 1959; DerSimonian 1986; DeMets 1987). In case of discrepancy between the two models (e.g. one giving a significant intervention effect, the other no significant intervention effect), we reported both results; otherwise, we reported only results from the random‐effects model.
Subgroup analysis and investigation of heterogeneity
We planned to perform the following subgroup analyses to compared intervention effects.
Trials at low risk of bias compared to trials at high risk of bias because risk of bias is an important determinant of the quality of evidence.
People with Child‐Pugh A unresectable hepatocellular carcinoma compared to people with Child‐Pugh B unresectable hepatocellular carcinoma because Child‐Pugh is an important determinant of hepatocellular carcinoma outcomes.
Eastern Cooperative Oncology Group score 0 compared to score 1 or 2 because performance status is an important determinant of hepatocellular carcinoma outcomes.
Radioembolisation used alone compared to radioembolisation in combination with other systemic or locoregional interventions (e.g. sorafenib) because composition of the experimental group is an important determinant of hepatocellular carcinoma study outcomes.
Previous locoregional interventions (e.g. radiofrequency ablation, chemoembolisation) compared to no previous locoregional interventions because previous locoregional treatment is an important determinant of hepatocellular carcinoma outcomes.
Sensitivity analysis
We planned to perform sensitivity analyses according to identified clinical and methodological variations, such as the tumour response assessment model.
We planned to assess the GRADE imprecision assessment (see below) to that obtained by Trial Sequential Analysis (Castellini 2018; Gartlenher 2018). The latter considers the meta‐analytic model and diversity.
Trial Sequential Analysis
We examined intervention effects using Trial Sequential Analyses to evaluate if these apparent effects could be caused by random error ('play of chance') (Brok 2008; Wetterslev 2008; Brok 2009; Thorlund 2009; Wetterslev 2009; Thorlund 2010; Thorlund 2011; TSA 2011; Wetterslev 2017). We applied Trial Sequential Analysis, as cumulative meta‐analyses are at risk of producing random errors due to sparse data and repetitive testing of accumulating data (Wetterslev 2008; Wetterslev 2009). To control random errors, we calculated the required information size (i.e. the number of participants needed in a meta‐analysis to detect or reject a certain intervention effect). The required information size calculation should also account for the diversity present in the meta‐analysis (Wetterslev 2009). In our meta‐analysis, the diversity‐adjusted required information size was based on the event proportion in the control group; the assumption of a plausible RR reduction of 20% or the RR reduction observed in the included trials; a risk of type I error of 2.5% because of three primary outcomes; a risk of type II error of 10%; and the diversity of the meta‐analysis. We did not plan to perform Trial Sequential Analysis for the secondary outcomes. The underlying assumption of Trial Sequential Analysis is that testing for significance may be performed each time a new trial is added to the meta‐analysis. We added trials according to the year of publication, and, if more than one trial was published in a year, we would have added trials alphabetically according to the last name of the first author. On the basis of the diversity‐adjusted required information size, we planned to construct trial sequential monitoring boundaries (Thorlund 2011). These boundaries would determine the statistical inference one may draw regarding the cumulative meta‐analysis that has not reached the required information size. If the cumulative Z‐curve crossed the trial sequential monitoring boundary for benefit or harm before the diversity‐adjusted required information size was reached, firm evidence may perhaps be established and further trials may turn out to be superfluous. In contrast, if the boundary was not surpassed, it was most probably necessary to continue doing trials to detect or reject a certain intervention effect. This could have been determined by assessing if the cumulative Z‐curve crossed the trial sequential monitoring boundaries for futility.
'Summary of findings' tables
We presented the evidence in 'Summary of findings' tables using the GRADE profiler software (GRADEpro GDT). For the outcomes of Grading of Recommendations Assessment, Development and Evaluation (GRADE), we used the definitions given in Table 4. We evaluated the certainty of evidence for the first three primary and four secondary outcomes if the trials reported data on these outcomes. Otherwise, we stated in the tables for the respective outcome that data were not reported. The outcomes we assessed were as follows: all‐cause mortality; health‐related quality of life; serious adverse events; cancer‐related mortality; time to progression of the tumour; tumour response assessments; non‐serious adverse events, considering within‐study risk of bias; indirectness of evidence (population, intervention, control, outcomes); unexplained heterogeneity or inconsistency of results (including problems with subgroup analyses); imprecision of results (wide CIs); and high probability of publication bias (Balshem 2011; Guyatt 2011a; Guyatt 2011b; Guyatt 2011c; Guyatt 2011d; Guyatt 2011e; Guyatt 2011f; Guyatt 2011g; Guyatt 2011h; Guyatt 2013a; Guyatt 2013b; Guyatt 2013c; Guyatt 2013d; Mustafa 2013; Guyatt 2017). We provided the time of longest follow‐up and the range of trial data collection, when possible, for the outcomes included in the 'Summary of findings' tables
1. Explanations of the 'Summary of findings' table.
| Outcomes | The tables provide findings for the most important outcomes for someone making a decision. These include potential benefits and harms, whether or not the included studies provide data for these outcomes. Additional findings may be reported elsewhere in the review |
| Assumed control group risk | Assumed control group risks can be based on the control group risks reported in the included studies or on epidemiological data from elsewhere. When only 1 control group risk is provided, it is normally the median control group risk across studies that provided data for that outcome Risk is the probability of an outcome occurring. The control group risk is the risk of an outcome occurring in the comparison group (without the intervention) |
| Corresponding intervention group risk | Risk is the probability of an outcome occurring. The intervention group risk is the risk of an outcome occurring in the group receiving the intervention |
| Relative effect |
Relative effect or risk ratio (RR) Relative effects are ratios Risk is the probability of an outcome occurring. An RR is the ratio between the risk in the intervention group and the risk in the control group. If the risk in the control group is 10% (100 per 1000) and the risk in the intervention group is 1% (10 per 1000), the RR is 10/100 or 0.10 If the RR is exactly 1.0, this means that there is no difference between occurrence of the outcome in intervention and control groups. It is unusual for the RR to be exactly 1.0, and understanding what it means if it is above or below this value depends on whether the outcome being counted is judged to be good or bad If the RR is greater than 1.0, the intervention increases the risk of the outcome. If it is a good outcome (e.g. the birth of a healthy baby), an RR > 1.0 indicates a desirable effect for the intervention. Whereas if the outcome is bad (e.g. death), an RR > 1.0 would indicate an undesirable effect If the RR is less than 1.0, the intervention decreases the risk of the outcome. This indicates a desirable effect if it is a bad outcome (e.g. death), and an undesirable effect if it is a good outcome (e.g. birth of a healthy baby) |
|
What is the difference between absolute and relative effects? The effect of an intervention can be described by comparing the risk in the intervention group with the risk in the control group. Such a comparison can be made in different ways One way to compare 2 risks is to calculate the difference between the risks. This is the absolute effect Consider the risk for blindness in a person with diabetes over a 5‐year period. If the risk for blindness is found to be 20 in 1000 (2%) in a group of people treated conventionally and 10 in 1000 (1%) among people treated with a new drug, the absolute effect is derived by subtracting the intervention group risk from the control group risk: 2%/1% = 1%. Expressed in this way, it can be said that the new drug reduces the 5‐year risk for blindness by 1% (absolute effect is 10 fewer per 1000) Another way to compare risks is to calculate the ratio of the 2 risks. Given the data above, the relative effect is derived by dividing the 2 risks, with the intervention risk divided by the control risk: 1% ÷ 2% = ½ (0.50). Expressed in this way, as the 'relative effect', the 5‐year risk for blindness with the new drug is 1/2 the risk with the conventional drug Here the table presents risks as x per 1000 (or 100, etc.) instead of %, as this tends to be easier to understand. Whenever possible, the table presents the relative effect as the RR. Usually the absolute effect is different for groups that are at high and low risk, whereas the relative effect often is the same. Therefore, when it is relevant, we have reported indicative risks for groups at different levels of risk. 2 or 3 indicating control group risks and the corresponding intervention group risks are presented when there are important differences across different populations | |
| Mean difference | The mean difference (MD) is the average difference between the intervention group and the control group across studies. Here a weighted MD is used, which means that results of some of the studies make a greater contribution to the average than others. Studies with more precise estimates for their results (narrower confidence intervals) are given more weight This way of measuring effect is used when data are combined or compared for continuous outcomes, such as weight, blood pressure, or pain measured on a scale. When different scales are used to measure the same outcome (e.g. different pain scales), a standardised mean difference (SMD) may be provided. This is a weighted mean difference standardised across studies giving the average difference in standard deviations for measures of that outcome |
| Confidence interval | A confidence interval (CI) is a range around an estimate that conveys how precise the estimate is; in this example, the result is the estimate of the intervention group risk. The CI is a guide to how sure we can be about the quantity we are interested in (here, the true absolute effect). The narrower the range between the 2 numbers, the more confident we can be about what the true value is; the wider the range, the less sure we can be. The width of the CI reflects the extent to which chance may be responsible for the observed estimate (with a wider interval reflecting more chance) |
| 95% CI | As explained above, the CI indicates the extent to which chance may be responsible for the observed numbers. In the simplest terms, a 95% CI means that we can be 95% confident that the true size of effect is between the lower and upper confidence limits (e.g. 0 and 3 in the blindness drugs example mentioned above). Conversely, there is a 5% chance that the true effect is outside of this range |
| Not statistically significant | Statistically significant means that a result is unlikely to have occurred by chance. The usual threshold for this judgement is that the results, or more extreme results, would occur by chance with a probability of < 0.05 if the null hypothesis (no effect) was true. When results are not statistically significant, as in this example, this is stated to alert users to the possibility that the results may have occurred by chance |
| No. of participants (studies) | The table provides the total number of participants across studies and the number of studies that provided data for that outcome. This indicates how much evidence is available for the outcome |
| Quality of the evidence | The quality of the evidence is a judgement about the extent to which we can be confident that the estimates of effect are correct. These judgements are made using the GRADE system, and they are provided for each outcome. Judgements are based on the type of study design (randomised trials vs observational studies), the risk of bias, the consistency of the results across studies, and the precision of the overall estimate across studies For each outcome, the quality of the evidence is rated as high, moderate, low, or very low using the following definitions:
|
Results
Description of studies
We identified 7490 citations through our database searches.
Results of the search
Among the 7490 citations identified, we removed 2067 duplicate references. Therefore, we screened 5423 references. Based on titles and abstracts, we excluded 5414 references. We then retrieved nine full‐text papers (Figure 1). Based on review of the full‐text papers, we found six randomised clinical trials to be eligible for our systematic review (Kolligs 2015; Pitton 2015; Salem 2016; Vilgrain 2017; Chow 2018; Ricke 2019). We excluded the remaining three studies (Mazzaferro 2013; Kulik 2014; El Fouly 2015).
1.
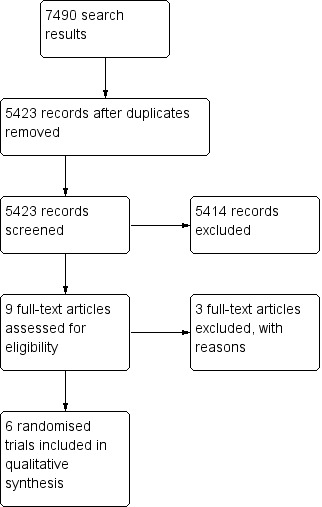
Study flow diagram.
We also identified two ongoing randomised trials: one comparing radioembolisation versus chemoembolisation (NCT01381211), and one, radioembolisation plus sorafenib versus sorafenib alone (NCT01556490).
Included studies
We included six randomised clinical trials in which 1340 participants were randomised. One trial compared radioembolisation plus sorafenib versus sorafenib alone in people with advanced hepatocellular carcinoma (Ricke 2019). This trial is a European multi‐centre phase II randomised clinical trial that comprised two cohorts: one local ablation cohort, randomised to radiofrequency ablation with or without sorafenib, and one palliative treatment cohort, randomised to radioembolisation with or without sorafenib. The publication included in the current Cochrane Review is the one related to the palliative treatment cohort (results for the other cohort have not yet been published). Participants in the palliative treatment group were people with unresectable hepatocellular carcinoma who were poor candidates for transarterial (chemo)embolisation. Bayer and Sirtex Medical were collaborating sponsors for this trial. Two trials compared radioembolisation versus sorafenib for people with locally advanced hepatocellular carcinoma (Vilgrain 2017; Chow 2018). Sirtex Medical was a collaborating sponsor of Chow 2018 and funded Vilgrain 2017. Three trials compared radioembolisation with chemoembolisation in people with intermediate‐stage hepatocellular carcinoma (Kolligs 2015; Pitton 2015; Salem 2016). Kolligs 2015 was supported by Sirtex Medical, Pitton 2015 by Johannes Gutenberg University Mainz, and Salem 2016 trial by Northwestern University.
We found no eligible trials that compared radioembolisation versus sham radioembolisation, best supportive care, cryotherapy, laser‐induced thermotherapy, radiofrequency ablation, or high‐frequency ultrasound.
Excluded studies
We excluded three studies, as they did not fulfil our inclusion criteria. Kulik 2014 compared radioembolisation plus sorafenib in one intervention group versus radioembolisation alone in the other group. El Fouly 2015 was a retrospective study. Mazzaferro 2013 was a non‐randomised phase II observational study. We included below information about adverse effects of radioembolisation from these studies.
Risk of bias in included studies
For graphical presentation of risk of bias of the included studies, see Figure 2 and Figure 3.
2.
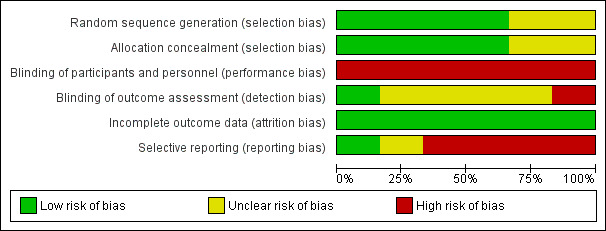
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included trials.
3.
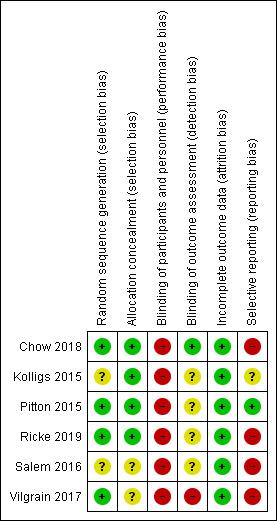
Risk of bias summary: review authors' judgements about each risk of bias item for each included trial.
Allocation
Four trials clearly reported the method of allocation sequence generation (Pitton 2015; Vilgrain 2017; Chow 2018; Ricke 2019). The remaining two trials did not clearly report generation of the allocation sequence (Kolligs 2015; Salem 2016). Kolligs 2015,Pitton 2015,Vilgrain 2017,Chow 2018, and Ricke 2019 clearly reported allocation concealment, and reporting of allocation concealment was unclear in Salem 2016.
Blinding
Reasonable blinding of an investigator or an informed participant could not be achieved due to differences in the nature of the procedures. Thus, all included studies had high risk of performance bias.
Chow 2018 reported detection bias clearly. Kolligs 2015; Pitton 2015; Salem 2016; and Ricke 2019 are at unclear risk of detection bias. Vilgrain 2017 is at high risk of detection bias.
Incomplete outcome data
We judged all included trials to be at low risk of attrition bias.
Selective reporting
Pitton 2015 is at low risk of reporting bias. Kolligs 2015 is at unclear risk of reporting bias. The remaining four trials are at high risk of reporting bias (Salem 2016; Vilgrain 2017; Chow 2018; Ricke 2019).
Other potential sources of bias
We found no evidence of other biases in the included trials.
Overall, we assessed all of the included trials to be at high risk of bias in at least one of the above domains; thus, we considered all trials to have high overall risk of bias.
Effects of interventions
See: Table 1; Table 2; Table 3
Summary of findings for the main comparison. Radioembolisation plus sorafenib compared with sorafenib monotherapy for unresectable hepatocellular carcinoma.
| Radioembolisation plus sorafenib compared with sorafenib monotherapy for unresectable hepatocellular carcinoma | ||||||
|
Patient or population: people with hepatocellular carcinoma Settings: specialist hospital Intervention: radioembolisation plus sorafenib Comparison: sorafenib | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Sorafenib | Radioembolisation and sorafenib | |||||
| All‐cause mortality at 1 year | Not reported | ‐ | ‐ | ‐ | All‐cause mortality was not reported. In 1 trial (424 participants – ITT), median overall survival was 11.4 months in the sorafenib group and 12.1 months in the radioembolisation plus sorafenib group (HR 1.01, 95% CI 0.81 to 1.25; P = 0.95) Based on survival curves, we can assume that 1‐year survival is 50% for the combination group vs 47% for the sorafenib group. Provided that no trial participants were censored because of short or missed survival follow‐up, this should translate to a 1‐year mortality rate of 50% for trial participants in the combination group, and 53% for trial participants in the sorafenib group |
|
| Health‐related quality of life | Not reported | ‐ | ‐ | ‐ | ‐ | |
| Serious adverse events | 38.5% | 39.6% | ‐ | 341 (safety population) (1 RCT) |
⊕⊝⊝⊝ Very lowa,b,c |
Median follow‐up of 9.4 months (IQR 12.6) in the radioembolisation + sorafenib group and 6.57 months (IQR 11.1) in the sorafenib group |
| Cancer‐related mortality | Not reported | ‐ | ‐ | ‐ | ‐ | |
| Time to progression of the tumour (median time to progression) | Not reported | ‐ | ‐ | ‐ | ‐ | |
| Tumour response assessments | Not reported | ‐ | ‐ | ‐ | ‐ | |
| Non‐serious adverse events (hyperbilirubinaemia: most frequent) | 4.4% | 14.4%. | ‐ | 341 (safety population) (1 RCT) |
⊕⊝⊝⊝ Very lowa,b,c |
‐ |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; HR: hazard ratio; IQR: interquartile range; ITT: intention‐to‐treat; RCT: randomised controlled trial. | ||||||
| GRADE Working Group grades of evidence. High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
aWe downgraded the certainty of evidence by one level for within‐study risk of bias (high risk of performance bias, unclear detection bias). bWe downgraded the certainty of evidence by one level for unassessable publication bias (only one trial). cWe downgraded the certainty of evidence by one level for imprecision (the effect estimate crosses 1).
Summary of findings 2. Radioembolisation compared with sorafenib for unresectable hepatocellular carcinoma.
| Radioembolisation compared with sorafenib for unresectable hepatocellular carcinoma | ||||||
|
Patient or population: people with hepatocellular carcinoma Settings: specialist hospital Intervention: radioembolisation Comparison: sorafenib | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | №. of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with sorafenib | Risk with radioembolisation | |||||
| All‐cause mortality at 1 year | All‐cause mortality at 1 year was 62.7% in the radioembolisation group vs 53.0% in the sorafenib group | ‐ | 360 (1 RCT) |
⊕⊝⊝⊝ Very lowa,b,c |
Another trial reported only median overall survival. Based on the survival curves in this trial, we can assume that 1‐year survival is 40% for trial participants in the radioembolisation group vs 38% for trial participants in the sorafenib group. Provided that no cases were censored because of short‐ or missed survival follow‐up, this should translate to a 1‐year mortality rate of 62% for trial participants in the radioembolisation group and 60% for trial participants in the sorafenib group | |
| Health‐related quality of life | Health‐related quality of life was reported in Chow 2018, according to the EuroQol‐5 Dimension (EQ‐5D) questionnaire. There were no differences in the EQ‐5D index between radioembolisation and sorafenib groups throughout the trial. In Vilgrain 2017, quality of life was reported according to the European Organisation for Research and Treatment of Cancer (EORTC) quality of life questionnaire (QLQ‐C30; version 3) and its specific hepatocellular carcinoma module. It showed that the global health status subscore was better in the radioembolisation group than in the sorafenib group (group effect P = 0.0048; time effect P < 0.0001) and the between‐group difference tended to increase with time (group‐time interaction P = 0·0447) | ‐ | 360 (1 RCT) 467 (1 RCT) |
⊕⊝⊝⊝ Very lowa,b,c |
The method of assessment of quality of life was different in both trials; thus, it was not possible to pool them | |
| Serious adverse events | In Chow 2018 trial, fewer trial participants in the radioembolisation group experienced serious adverse events compared with trial participants in the sorafenib group: 27 (20.8%) in the radioembolisation group vs 57 (35.2%) in the sorafenib group (Fisher's exact test statistical value of 0.0016). In Vilgrain 2017, reporting of serious adverse events was not complete | ‐ | 360 (1 RCT) 467 (1 RCT) |
⊕⊝⊝⊝ Very lowa,b,c |
||
| Cancer‐related mortality | Not reported | ‐ | ‐ | ‐ | ‐ | |
| Time to progression of the tumour (median time to progression) |
Median time to progression of the tumour in the radioembolisation group was 6.1 months vs 5.4 months in the sorafenib group in Chow 2018. Time to progression of the tumour was not reported in Vilgrain 2017. Median progression‐free survival was, however, reported as 4.1 months (95% CI 3.8 to 4.6) in the radioembolisation group vs 3.7 months (3.3 to 5.4) in the sorafenib group (Vilgrain 2017) | ‐ | 360 (1 RCT) 467 (1 RCT) |
⊕⊝⊝⊝ Very lowa,b,c |
‐ | |
| Disease control rate | 588 per 1000 | 553 per 1000 (494 to 629) | RR 0.94 (0.84 to 1.05) | 748 (2 RCTs) | ⊕⊝⊝⊝ Very lowa,b,c |
‐ |
| Non‐serious adverse events (hand‐foot skin reaction) | 392 per 1000 | 4 per 1000 (0 to 23) | RR 0.02 (0.00 to 0.06) | 734 (2 RCTs) | ⊕⊕⊝⊝ Lowa,c |
‐ |
| *The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RCT: randomised controlled trial. | ||||||
| GRADE Working Group grades of evidence. High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
aWe downgraded the certainty of evidence by one level for within‐study risk of bias (high risk of detection and reporting biases). bWe downgraded the certainty of evidence by one level for imprecision. cWe downgraded the certainty of evidence by one level for unassessable publication bias (only two trials).
Summary of findings 3. Radioembolisation compared with chemoembolisation for unresectable hepatocellular carcinoma.
| Radioembolisation compared with chemoembolisation for unresectable hepatocellular carcinoma | ||||||
|
Patient or population: people with hepatocellular carcinoma Settings: specialist hospital Intervention: radioembolisation Comparison: chemoembolisation | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No. of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Chemoembolisation | Radioembolisation | |||||
| All‐cause mortality at 1 year | All‐cause mortality at 1 year was not reported in any of the 3 included studies | ‐ | ‐ | ‐ | All‐cause mortality was not reported in Salem 2016; median overall survival was reported as 18.6 months for trial participants in the radioembolisation group vs 17.7 months for trial participants in the chemoembolisation group. Based on the survival curves provided in the final publication of Salem 2016, we can assume that 1‐year survival is 70% for both groups. Provided that no trial participants were censored because of short or missed survival follow‐up, this should translate to a 1‐year mortality rate of 30% for both groups In Pitton 2015, the median overall survival of trial participants was 592 days in the radioembolisation group vs 788 days in the chemoembolisation group. Based on the survival curves provided in the final publication of Pitton 2015, we can assume crudely that 1‐year survival is 55% for both intervention groups. Provided that no trial participants were censored because of short or missed survival follow‐up, this should translate to a 1‐year mortality rate of 45% for both groups Kolligs 2015 did not report all‐cause mortality nor median overall survival |
|
| Health‐related quality of life | In a single study, health‐related quality of life was not different between the 2 treatment modalities (at week 12). The other 2 studies in this comparison did not report on quality of life | ‐ | 28 (1 RCT) |
⊕⊝⊝⊝ Very lowa,b,c |
‐ | |
| Serious adverse events | 146 per 1000 | 206 per 1000 (92 to 458) | RR 1.44 (0.66‐ 3.25) | 97 (3 RCTs) |
⊕⊝⊝⊝ Very lowa,d,e |
‐ |
| Cancer‐related mortality | Not reported | ‐ | ‐ | ‐ | ‐ | |
| Time to progression of the tumour (median time to progression) |
Median time to progression of the tumour was longer in the radioembolisation group in Salem 2016. Median time to progression was not reached in the radioembolisation arm and was 6.8 months in the chemoembolisation arm (HR 0.122, 95% CI 0.027 to 0.557; P = 0.007). In Pitton 2015, the median time to progression of the tumour in the radioembolisation group was 371 days vs 336 days in the chemoembolisation group (P = 0.5764). Because of the variable definition of progression used in these 2 trials (and thus, non‐standardised assessment of time to progression in the 2 trials), we considered the data too heterogeneous to be included in a meta‐analysis Kolligs 2015 did not report the time to progression of the tumour. This trial reported median progression‐free survival as 3.6 months (95% CI 2.3 to 6.2) with radioembolisation and 3.7 months (95% CI 1.6 to 11.0) with chemoembolisation interventions (Kolligs 2015) |
‐ | 97 (3 RCTs) |
⊕⊝⊝⊝ Very lowa,b,c |
‐ | |
| Disease control rate | Kolligs 2015 assessed tumour response using response evaluation criteria in solid tumours. Disease control rates (complete response + partial response + stable disease) were 73.3% with radioembolisation vs 76.9% with chemoembolisation (Kolligs 2015). Salem 2016 assessed tumour response using WHO and EASL criteria. According to WHO criteria, tumour response was reported in 12 of 23 evaluable trial participants (52%) who received radioembolisation vs 12 of 19 evaluable participants (63%) who received chemoembolisation (Fisher's exact test statistical value of 0.7998). According to EASL criteria, tumour response was reported in 20/23 evaluable participants (87%) in the radioembolisation group vs 14/19 evaluable participants (74%) in the chemoembolisation group. Because of the variable definition of tumour response used in both trials, we considered the data too heterogeneous to be included in a meta‐analysis. Pitton 2015 did not report tumour response | ‐ | 97 (3 RCTs) |
⊕⊝⊝⊝ Very lowa,b,c |
‐ | |
| Non‐serious adverse events | One person in each group suffered from vascular complications including common femoral artery pseudoaneurysm in Salem 2016. There was a trend for more fatigue in people who received radioembolisation than chemoembolisation (P = 0.08). The chemoembolisation group experienced more diarrhoea (P = 0.031) and increased hypoalbuminaemia (P < 0.001) Kolligs 2015 reported clinically relevant abnormal laboratory results for 4 participants in the radioembolisation group and 3 participants in the chemoembolisation group (P = 0.67). Radioembolisation appeared to have a greater impact than chemoembolisation on total bilirubin grade at 3 months, but both treatment groups had a similar proportion of people with increased total bilirubin grade at 6 months. Otherwise, changes in laboratory results were unremarkable between the 2 groups. Because Kolligs 2015 did not report clear numbers for specific non‐serious adverse events, these data cannot be meta‐analysed together with those from Salem 2016. There was no specific mention of non‐serious adverse events in Pitton 2015 |
‐ | 97 (3 RCTs) |
⊕⊝⊝⊝ Very lowa,b,c |
‐ | |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; EASL: European Association for the Study of the Liver; HR: hazard ratio; RCT: randomised controlled trial; RR: risk ratio; WHO: World Health Organization. | ||||||
| GRADE Working Group grades of evidence. High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
aWe downgraded the certainty of evidence by one level for within‐study risk of bias (performance and reporting biases). bWe downgraded the certainty of evidence by one level for unassessable publication bias (only one trial). cWe downgraded the certainty of evidence by one level for imprecision (small number of events). dWe downgraded the certainty of evidence by one level for unassessable publication bias (only three trials). eWe downgraded the certainty of evidence by one level for imprecision (the effect estimate crosses 1).
Radioembolisation plus sorafenib versus sorafenib
All‐cause mortality
All‐cause mortality was not among the outcomes of Ricke 2019. Trial authors reported overall survival, and trial results showed that in the intention‐to‐treat population, the median overall survival was 12.1 months in the radioembolisation (selective internal radiation therapy – with yttrium‐90 (Y‐90) resin microspheres) plus sorafenib group versus 11.4 months in the sorafenib group (hazard ratio (HR) 1.01, 95% confidence interval (CI) 0.81 to 1.25; P = 0.95). Based on the survival curves provided in the final publication of the study, we can assume crudely that one‐year survival is at 50% for the combination group versus 47% for the sorafenib group. Provided that no trial participants were censored because of short or missed survival follow‐up, this should translate to a one‐year mortality rate of 50% for trial participants in the combination arm and 53% for trial participants in the sorafenib arm.
Health‐related quality of life
Ricke 2019 did not report data on quality of life.
Serious adverse events
Serious adverse events were reported in 63 trial participants (39.6%) in the radioembolisation plus sorafenib group and in 70 trial participants (38.5%) in the group that received only sorafenib (P = 0.911) (safety population for this trial comprised 159 participants for the radioembolisation plus sorafenib group and 182 participants for the sorafenib monotherapy group). The Fisher's exact test statistical value is 0.9186.
Trial authors reported the following deaths as adverse events: one person died of decreased appetite in the sorafenib group, one person died of radiation pneumonitis in the radioembolisation group (because of overexposure beyond the proposed 30‐Gy limit due to a technical failure), and one person receiving radioembolisation died only of liver failure. Another two deaths were recorded as due to hepatic encephalopathy and as a surgical complication of pulmonary thromboembolectomy. Hepatic failure as a serious adverse event was reported in six trial participants (3.8%) in the selective internal radiation therapy (SIRT) + sorafenib group and in eight participants (4.1%) in the sorafenib group.
Cancer‐related mortality
Ricke 2019 did not report cancer‐related mortality.
Time to progression of the tumour (reported as median time to progression)
Ricke 2019 did not report median time to progression of the tumour.
Tumour response assessments
Ricke 2019 did not report tumour response rates.
Non‐serious adverse events
Among the most frequent adverse events, categorised according to Common Terminology Criteria for Adverse Events (CTCAE), was hyperbilirubinaemia. It was approximately three times more common in the radioembolisation plus sorafenib group versus the sorafenib group (14.5% versus 4.4%; Fisher's exact test statistical value is 0.0032). Fatigue was more common in the radioembolisation plus sorafenib group than in the sorafenib group, with 35.2% versus 24.2% of trial participants (Fisher's exact test statistical value of 0.1116).
Liver transplantation following treatment
Ricke 2019 did not report any trial participants who received post‐treatment liver transplantation.
Radioembolisation versus sorafenib
All‐cause mortality
All‐cause mortality at six months in Chow 2018 was 33.3% in the radioembolisation group versus 33.5% in the sorafenib group; all‐cause mortality at one year in the radioembolisation group was 62.7% versus 53.0% in the sorafenib group. All‐cause mortality was not specifically reported in Vilgrain 2017. Based on the survival curves provided in the final publication of Vilgrain 2017, we can assume crudely that one‐year survival among trial participants in the radioembolisation group is 40% versus 38% in the sorafenib group. Provided that no cases were censored because of short or missed survival follow‐up, this should translate to a one‐year mortality rate of 62% for trial participants in the radiomebolisation group and 60% for trial participants in the sorafenib group. The meta‐analysed hazard ratio for death was 1.12 (95% CI 0.97 to 1.30; P = 0.11; 734 participants; 2 trials; I² = 0%; Analysis 1.1), favouring neither radiomebolisation nor sorafenib. Given the fact that the mortality ratios in Vilgrain 2017 are based on our visual guess‐estimates, which are almost certainly inaccurate, we did not conduct a meta‐analysis for all‐cause mortality.
1.1. Analysis.
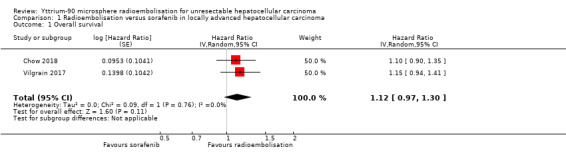
Comparison 1 Radioembolisation versus sorafenib in locally advanced hepatocellular carcinoma, Outcome 1 Overall survival.
Health‐related quality of life
Health‐related quality of life was reported in Chow 2018, according to the EuroQol‐5‐Dimension (EQ‐5D) questionnaire. There were no differences in the EQ‐5D index between the radioembolisation and sorafenib groups throughout the trial. Vilgrain 2017 reported quality of life according to the European Organisation for Research and Treatment of Cancer (EORTC) quality of life questionnaire (QLQ‐C30; version 3) and its specific hepatocellular carcinoma module. Trial authors showed that the global health status subscore was better in the radioembolisation group than in the sorafenib group (group effect P = 0.0048; time effect P < 0.0001) and the between‐group difference tended to increase with time (group‐time interaction; P = 0·0447).
Serious adverse events
Fewer trial participants experienced serious adverse events in the radioembolisation group than in the sorafenib group in Chow 2018: 27 (20.8%) in the radiomebolisation group versus 57 (35.2%) in the sorafenib group (Fisher's exact test statistical value of 0.0016). Vilgrain 2017 reported 13 treatment‐related deaths in the radioembolisation group versus 12 treatment‐related deaths in the sorafenib group. Vilgrain 2017 did not, however, report specifically other forms of serious adverse events (i.e. those that were life‐threatening or those that led to hospitalisation). Thus, reporting of serious adverse events in Vilgrain 2017 was not complete, and we did not consider data appropriate for meta‐analysis.
Cancer‐related mortality
Neither of the two trials reported cancer‐related mortality (Vilgrain 2017; Chow 2018).
Time to progression of the tumour
The median time to progression of the tumour in the radioembolisation group was 6.1 months versus 5.4 months in the sorafenib group in Chow 2018. Time to progression of the tumour was not reported in Vilgrain 2017. Median progression‐free survival was, however, reported as 4.1 months (95% CI 3.8 to 4.6) in the radioembolisation group versus 3.7 months (95% CI 3.3 to 5.4) in the sorafenib group (Vilgrain 2017).
Tumour response assessments
Both Vilgrain 2017 and Chow 2018 used response evaluation criteria in solid tumours for assessment of tumour response. Disease control rate was defined in both trials as complete response plus partial response plus stable disease. The risk ratio (RR) for the disease control rate was 0.94 (95% CI 0.84 to 1.05; P = 0.27; 748 participants; 2 trials; I² = 0%; Analysis 1.2), favouring neither radioembolisation nor sorafenib.
1.2. Analysis.
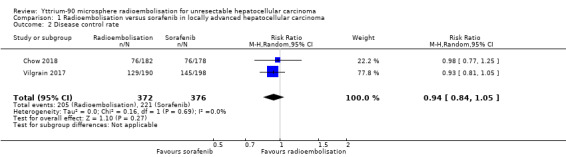
Comparison 1 Radioembolisation versus sorafenib in locally advanced hepatocellular carcinoma, Outcome 2 Disease control rate.
Non‐serious adverse events
Both trials reported several adverse events of interest, including fatigue (RR as reported by the fixed‐effect model 0.43, 95% CI 0.25 to 0.73; P = 0.002; 734 participants; 2 trials; I² = 60%; Analysis 1.3), favouring radioembolisation (Vilgrain 2017; Chow 2018). When the analysis was repeated with the random‐effects model, results were as follows: RR 0.42, 95% CI 0.17 to 1.02; P = 0.06; 734 participants; 2 trials; I² = 60%, favouring neither radioembolisation nor sorafenib (Vilgrain 2017; Chow 2018).
1.3. Analysis.
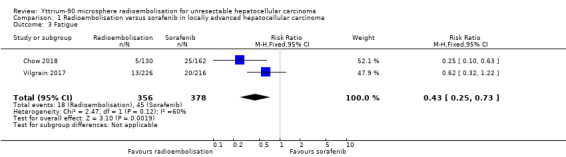
Comparison 1 Radioembolisation versus sorafenib in locally advanced hepatocellular carcinoma, Outcome 3 Fatigue.
Other reported adverse events include hand‐foot skin reaction (RR 0.02, 95% CI 0.00 to 0.06; P < 0.001; 734 participants; 2 trials; I² = 0%; Analysis 1.4), skin rash (RR 0.11, 95% CI 0.04 to 0.34; P < 0.001; 734 participants; 2 trials; I² = 0%; Analysis 1.5), diarrhoea (RR 0.11, 95% CI 0.04 to 0.34; P < 0.001; 734 participants; 2 trials; I² = 63%; Analysis 1.6), and hypertension (RR 0.10, 95% CI 0.01 to 0.88; P = 0.04; 734 participants; 2 trials; I² = 59%; Analysis 1.7), all favouring radioembolisation; and hypoalbuminaemia (RR 1.08, 95% CI 0.84 to 1.38; P = 0.56; 734 participants; 2 trials; I² = 0%; Analysis 1.8), favouring neither radioembolisation nor sorafenib (Vilgrain 2017; Chow 2018).
1.4. Analysis.
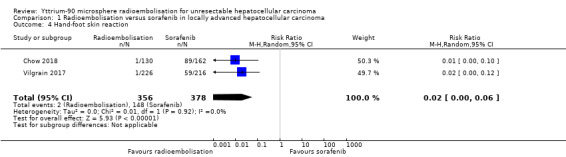
Comparison 1 Radioembolisation versus sorafenib in locally advanced hepatocellular carcinoma, Outcome 4 Hand‐foot skin reaction.
1.5. Analysis.
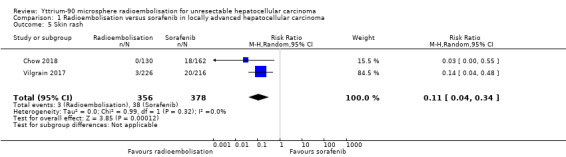
Comparison 1 Radioembolisation versus sorafenib in locally advanced hepatocellular carcinoma, Outcome 5 Skin rash.
1.6. Analysis.
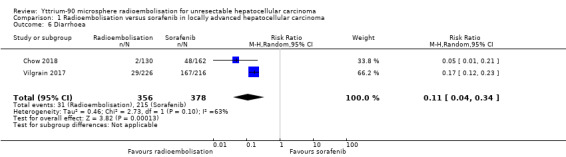
Comparison 1 Radioembolisation versus sorafenib in locally advanced hepatocellular carcinoma, Outcome 6 Diarrhoea.
1.7. Analysis.
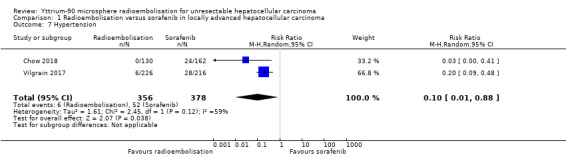
Comparison 1 Radioembolisation versus sorafenib in locally advanced hepatocellular carcinoma, Outcome 7 Hypertension.
1.8. Analysis.
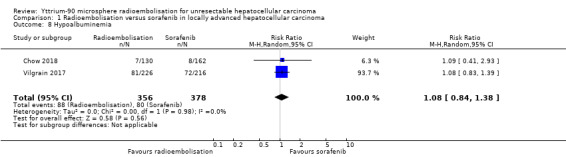
Comparison 1 Radioembolisation versus sorafenib in locally advanced hepatocellular carcinoma, Outcome 8 Hypoalbuminemia.
Liver transplantation following treatment
Neither of the two trials reported liver transplantation following treatment (Vilgrain 2017; Chow 2018).
Radioembolisation versus chemoembolisation
All‐cause mortality
All‐cause mortality was not reported in the Salem 2016 trial; median overall survival was reported as 18.6 months for trial participants in the radioembolisation group versus 17.7 months for those in the chemoembolisation group. Based on the survival curves provided in the final publication of Salem 2016, we can assume crudely that one‐year survival is 70% for both intervention groups. Provided that no trial participants were censored because of short or missed survival follow‐up, this should translate to a one‐year mortality rate of 30% for both intervention groups. The median overall survival of trial participants was 592 days in the radioembolisation group versus 788 days in the chemoembolisation group in Pitton 2015. Based on the survival curves provided in the final publication of Pitton 2015, we can assume crudely that one‐year survival is 55% for both intervention groups. Provided that no trial participants were censored because of short or missed survival follow‐up, this should translate to a one‐year mortality rate of 45% for both groups. Neither trial reported sufficient data about observed and expected deaths so that we could calculate hazard ratios according to the Parmar 1998 equation. Kolligs 2015 did not report all‐cause mortality nor median overall survival.
Given the fact that the above estimated mortality ratios are based on visual guess‐estimates that are almost certainly inaccurate, we did not perform a meta‐analysis for all‐cause mortality.
Health‐related quality of life
Health‐related quality of life was reported in Kolligs 2015, and at week 12, neither the chemoembolisation nor radioembolisation intervention had a different impact on quality of life as measured by Functional Assessment of Cancer Therapy‐Hepatobiliary total or its subscales. Pitton 2015 and Salem 2016 did not report quality of life.
Serious adverse events
In Kolligs 2015, seven participants in the radioembolisation group and five participants in the chemoembolisation group were hospitalised with serious adverse events; all treatment‐related serious adverse events in both groups were resolved with active management with no procedure‐related deaths. In Pitton 2015, one person in each group died of cardiovascular complications. In Salem 2016, one potentially life‐threatening adverse event was reported in each study group (bacterial peritonitis in the radioembolisation group and sepsis in the chemoembolisation group). The RR for serious adverse events was 1.47 (95% CI 0.66 to 3.25; P = 0.34; 97 participants; 3 trials; I² = 0%; Analysis 2.1), favouring neither radioembolisation nor chemoembolisation.
2.1. Analysis.
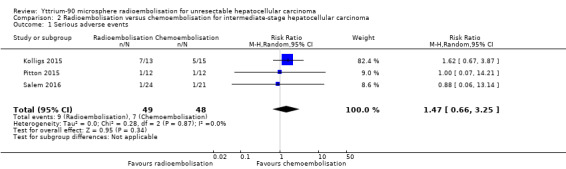
Comparison 2 Radioembolisation versus chemoembolisation for intermediate‐stage hepatocellular carcinoma, Outcome 1 Serious adverse events.
Sensitivity analysis
We conducted Trial Sequential Analysis on the outcome of serious adverse events for radioembolisation versus chemoembolisation in the three included trials (Kolligs 2015; Pitton 2015; Salem 2016). The diversity‐adjusted required information size was calculated based on event proportion in the chemoembolisation group of 14.5% (RR reduction of 20%), with type I error 2.5% because of our three primary outcomes (Jakobsen 2014), type II error of 10% (90% power), and diversity of 0%. The required information size was 6699 participants. The monitoring boundaries were ignored because only 1.45% (97/6699) of the information size was accrued (data not shown). Thus, it is not possible to derive much from this Trial Sequential Analysis, apart from the fact that the data are highly insufficient.
Cancer‐related mortality
None of the three trials reported cancer‐related mortality.
Time to progression of the tumour
The definition of time to progression of the tumour was different in the three trials: it was based on World Health Organization (WHO) and European Association for the Study of the Liver (EASL) criteria (Salem 2016); on modified response evaluation criteria in solid tumours (Pitton 2015); and on response evaluation criteria in solid tumours (Kolligs 2015).
The median time to progression of the tumour was longer in the radioembolisation group in Salem 2016. The median time to progression was not reached in the radioembolisation arm but was 6.8 months in the chemoembolisation arm (HR 0.122, 95% CI, 0.027 to 0.557; P = 0.007). In Pitton 2015, the median time to progression of the tumour in the radioembolisation group was 371 days versus 336 days in the chemoembolisation group (P = 0.5764). Because of the variable definition of progression used in these two trials (and thus, non‐standardised assessment of time to progression in the two trials), we considered the data too heterogeneous to be included in a meta‐analysis.
Kolligs 2015 did not report the time to progression of the tumour. Trial authors reported median progression‐free survival as 3.6 months (95% CI 2.3 to 6.2) with radioembolisation and 3.7 months (95% CI 1.6 to 11.0) with chemoembolisation interventions (Kolligs 2015).
Tumour response assessments
Kolligs 2015 assessed tumour response using response evaluation criteria in solid tumours. Disease control rates (complete response + partial response + stable disease) were 73.3% with radioembolisation versus 76.9% with chemoembolisation (Fisher's exact test statistical value of 0.9139) (Kolligs 2015). Salem 2016 assessed tumour response using WHO and EASL criteria. According to WHO criteria, tumour response was reported in 12 of 23 evaluable trial participants (52%) who received radioembolisation versus 12 of 19 evaluable participants (63%) who received chemoembolisation (Fisher's exact test statistical value of 0.7998). According to EASL criteria, tumour response was reported in 20 of 23 evaluable participants (87%) in the radioembolisation group versus 14 of 19 evaluable participants (74%) in the chemoembolisation group. Because of the variable definition of tumour response used in both trials, we considered the data too heterogeneous to be included into a meta‐analysis. Pitton 2015 did not report tumour response.
Non‐serious adverse events
One person in each group had vascular complications including common femoral artery pseudoaneurysm in Salem 2016. A trend showed more fatigue among people who received radioembolisation than among those who received chemoembolisation (P = 0.08). The chemoembolisation group experienced more diarrhoea (P = 0.031) and increased hypoalbuminaemia (P < 0.001).
Kolligs 2015 reported clinically relevant abnormal laboratory results for four participants in the radioembolisation group and three participants in the chemoembolisation group (P = 0.67). Radioembolisation appeared to have a greater impact than chemoembolisation on total bilirubin grade at three months, but both treatment groups had a similar proportion of people with increased total bilirubin grade at six months. Otherwise, changes in laboratory results were unremarkable between the two groups. Because Kolligs 2015 did not report clear numbers for specific non‐serious adverse events, data from Kolligs 2015 cannot be pooled together with those from Salem 2016 in a single meta‐analysis. Pitton 2015 did not specifically mention non‐serious adverse events.
Liver transplantation following treatment
Salem 2016 conducted a subgroup analysis for a subset of participants on the liver transplantation list. Rates of liver transplantation following locoregional treatment among trial participants on the list were 87% (13/15) after radioembolisation and 70% (7/10) after chemoembolisation. Only one trial participant in the chemoembolisation group underwent liver transplantation following locoregional treatment in Pitton 2015, and one person in the radioembolisation group and two in the chemoembolisation group underwent liver transplantation following locoregional treatment in Kolligs 2015. Because information about people on the transplant list before inclusion within each trial was available for only one trial, we considered the data too heterogeneous to be included in a meta‐analysis.
Subgroup analyses
It was not possible to conduct any of the planned subgroup analyses because of data limitations.
Sensitivity analysis
We could perform sensitivity analysis only for serious adverse events for radioembolisation versus chemoembolisation in the three included trials (Kolligs 2015; Pitton 2015; Salem 2016), using Trial Sequential Analysis. We could not perform a sensitivity analysis of tumour response assessment because of the nature of the available data.
'Summary of findings' tables
Table 1; Table 2; and Table 3 present our findings on the below three comparisons for the outcomes of all‐cause mortality, health‐related quality of life, serious adverse events, cancer‐related mortality; time to progression of the tumour, tumour response assessments; and non‐serious adverse events. When possible, we have provided time points or ranges, or both, for data collection.
GRADE assessment
Radioembolisation plus sorafenib versus sorafenib
The evidence, as evaluated by the GRADE approach, was of very low certainty for the reported outcomes of overall survival, serious adverse events, and non‐serious adverse events (Table 1).
Radioembolisation versus sorafenib
The evidence, as evaluated by the GRADE approach, was of very low certainty for the reported outcomes of overall survival and disease control rate, and of low certainty for non‐serious adverse events (Table 2).
Radioembolisation versus chemoembolisation
The evidence, as evaluated by the GRADE approach, was of very low certainty for the reported outcomes of serious adverse events and health‐related quality of life (Table 3).
Report on the adverse effects of radioembolisation from the three excluded studies
El Fouly 2015, a retrospective study, reports that in radioembolisation‐treated people, unspecific abdominal pain occurred in 5% and post‐embolisation fatigue syndrome in 40% of them. In Mazzaferro 2013, the most commonly reported clinical toxicities following radioembolisation included anorexia (15.4%) and clinically detectable ascites (9.6%). In Kulik 2014, fatigue was reported in 65% and abdominal pain in 25% of radioembolisation‐treated people.
Discussion
Summary of main results
On the basis of a single randomised trial, we found very low‐certainty evidence that radioembolisation combined with sorafenib might be associated with higher rates of non‐serious adverse events compared to sorafenib monotherapy. Overall survival, however, does not seem to differ between treatment approaches. Data for this comparison were sparse, and accordingly, we could not exclude even large differences. On the basis of two randomised clinical trials, we have low‐certainty evidence suggesting that radioembolisation achieves overall survival and a disease control rate that is comparable to sorafenib monotherapy among participants with locally advanced hepatocellular carcinoma. Moreover, the risk of non‐serious adverse events seems to be lower with radioembolisation compared with sorafenib interventions. On the basis of three small randomised clinical trials comparing radioembolisation versus chemoembolisation in intermediate‐stage hepatocellular carcinoma, we found low‐certainty evidence suggesting that the risk of serious adverse events is similar between radioembolisation and chemoembolisation. The results of two ongoing randomised trials are awaited to provide data for radioembolisation versus no intervention or versus chemoembolisation for unresectable hepatocellular carcinoma (NCT01381211; NCT01556490).
Overall completeness and applicability of evidence
The search strategy was very wide, and by searching the reference lists of the included trials, and by checking recent review articles, we aspired to include all relevant trials. Publication bias might be an issue here; however, because of the limited number of trials for each of the three comparisons, it was not possible to assess this formally. Due to the nature of the experimental intervention, all trials ought to have used sham intervention in the control group or blinded outcome assessors, or both. Without proper blinding, we will not obtain unbiased reporting.
Quality of the evidence
Using the GRADE approach (GRADEpro GDT; Balshem 2011), we assessed the certainty of evidence for the following.
For the comparison of radioembolisation plus sorafenib versus sorafenib, we assessed overall evidence as having very low certainty because of risk of bias (high risk of performance bias and unclear detection bias), imprecision, and publication bias in the Ricke 2019 publication.
For the comparison of radioembolisation versus sorafenib, we assessed the overall evidence as having very low certainty because of risk of bias (high risk of detection and reporting biases), as well as imprecision.
For the comparison of radioembolisation versus chemoembolisation, we assessed the overall evidence as having very low certainty because of risk of bias (high risk of performance and reporting biases).
Potential biases in the review process
Two review authors selected trials and extracted data independently. This secures objective data. We discussed our analyses among ourselves, as well as with the review editors. We feel relatively confident that we have identified most of the relevant English language publications, but we cannot exclude that we might have missed trials published in Chinese or other languages.
Most of the data were irregularly reported, and we need guideline definitions for reporting of core outcome measures, as well as more complete reporting of adverse events.
Agreements and disagreements with other studies or reviews
We found one meta‐analysis comparing Y‐90 microsphere radioembolisation with chemoembolisation for treatment of hepatocellular carcinoma (Facciorusso 2016). This meta‐analysis contains only two randomised trials that are also included in our systematic review. This meta‐analysis suggests that there is no observed clinical or statistical difference between the two modalities in terms of survival, response rate, or safety. Our results rather point to the lack of sufficient data.
Authors' conclusions
Implications for practice.
Evidence for the benefits and harms of radioembolisation with or without sorafenib and compared with sorafenib alone in people with unresectable hepatocellular carcinoma is highly insufficient. We cannot determine if radioembolisation plus sorafenib compared with sorafenib alone affects all‐cause mortality or the occurrence of adverse events. Radioembolisation compared with sorafenib seemed to achieve equivalent survival and to cause fewer adverse effects, but our level of certainty was very low. Evidence for the benefits and harms of radioembolisation versus chemoembolisation in people with unresectable hepatocellular carcinoma is also highly insufficient. Radioembolisation did not seem to differ from chemoembolisation in terms of serious adverse events and health‐related quality of life, but the certainty of evidence was very low. Additional well‐performed and high‐quality placebo‐controlled randomised clinical trials are needed to assess patient‐centred outcomes.
Implications for research.
Large randomised clinical trials of good quality examining yttrium‐90 microsphere radioembolisation for people with unresectable hepatocellular carcinoma are needed. It is important that the randomisation process is clearly described, as well as the interventions. The participant flow should be well specified, as should the method of data handling. Standardisation of the staging systems of hepatocellular carcinoma and of the tools used to assess different outcomes in these studies is needed (including response evaluation criteria and quality of life assessment tools). Trials must be designed and described by presenting the SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) statement (spirit‐statement.org), along with the CONSORT (CONsolidated Standards of Reporting Trials) statement (consort‐statement.org).
One ongoing randomised trial is evaluating radioembolisation versus chemoembolisation for intermediate‐stage hepatocellular carcinoma (NCT01381211), and another ongoing randomised trial is evaluating the combination of radioembolisation plus sorafenib versus sorafenib alone in advanced hepatocellular carcinoma (NCT01556490).
What's new
| Date | Event | Description |
|---|---|---|
| 16 October 2019 | New citation required and conclusions have changed | In the previously published review version, we concluded that evidence was insufficient to assess the beneficial and harmful effects of yttrium‐90 microsphere radioembolisation compared with no treatment, sham radioembolisation, or other systemic or locoregional therapies for people with hepatocellular carcinoma In this updated review version, we added to the previous conclusion that "...Radioembolisation compared with sorafenib seemed to achieve equivalent survival and to cause less adverse effects, but our certainty is low to very low", and in general, better formulated our conclusions |
| 27 September 2019 | New search has been performed | We updated searches and search results. We identified 4 new trials for inclusion in the review |
Acknowledgements
We thank the Cochrane Hepato‐Biliary Group and their supporting editorial team.
Review update Peer reviewers: Miny Samuel, Singapore Contact editors: Rosanna Simonetti, Italy Sign‐off editor: Christian Gluud, Denmark Abdominal and Endocrine Network Associate Editor: Liz Bickerdike, UK
Cochrane Review Group funding acknowledgement: the Danish State is the largest single funder of the Cochrane Hepato‐Biliary Group through its investments in The Copenhagen Trial Unit, Centre for Clinical Intervention Research, Rigshospitalet, Copenhagen University Hospital, Denmark.
Disclaimer: The views and opinions expressed in this review are those of the authors and do not necessarily reflect those of the Danish State or The Copenhagen Trial Unit.
Appendices
Appendix 1. Search strategies
| Database | Time span | Search strategy |
| Cochrane Hepato‐Biliary Group Controlled Trials Register | September 2019 | (radioembol* or embol* or TheraSphere or SIR‐Sphere) and (((liver or hepato*) and (carcinom* or cancer* or neoplasm* or malign* or tumo*)) or HCC) |
| Cochrane Central Register of Controlled Trials Register (CENTRAL) in the Cochrane Library | 2019, Issue 9 | #1 MeSH descriptor: [Embolization, Therapeutic] explode all trees #2 radioembol* or embol* or TheraSphere or SIR‐Sphere #3 #1 or #2 #4 MeSH descriptor: [Carcinoma, Hepatocellular] explode all trees #5 MeSH descriptor: [Liver Neoplasms] explode all trees #6 ((liver or hepato*) and (carcinom* or cancer* or neoplasm* or malign* or tumo*)) or HCC #7 #4 or #5 or #6 #8 #3 and #7 |
| MEDLINE Ovid | 1946 to September 2019 | 1. exp Embolization, Therapeutic/ 2. (radioembol* or embol* or TheraSphere or SIR‐Sphere).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] 3. 1 or 2 4. exp Carcinoma, Hepatocellular/ 5. exp Liver Neoplasms/ 6. (((liver or hepato*) and (carcinom* or cancer* or neoplasm* or malign* or tumo*)) or HCC).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] 7. 4 or 5 or 6 8. 3 and 7 9. (random* or blind* or placebo* or meta‐analys*).mp. [mp=title, abstract, original title, name of substance word, subject heading word, keyword heading word, protocol supplementary concept word, rare disease supplementary concept word, unique identifier] 10. 8 and 9 |
| Embase Ovid | 1974 to September 2019 | 1. exp yttrium 90/ 2. exp artificial embolism/ 3. (radioembol* or embol* or TheraSphere or SIR‐Sphere).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword] 4. 1 or 2 or 3 5. exp liver cell carcinoma/ 6. exp liver tumor/ 7. (((liver or hepato*) and (carcinom* or cancer* or neoplasm* or malign* or tumo*)) or HCC).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword] 8. 5 or 6 or 7 9. 4 and 8 10. (random* or blind* or placebo* or meta‐analys*).mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer, device trade name, keyword]. 11. 9 and 10 |
| LILACS (Bireme) | 1982 to September 2019 | (radioembol$ or embol$ or TheraSphere or SIR‐Sphere) [Words] and (((liver or hepato$) and (carcinom$ or cancer$ or neoplasm$ or malign$ or tumo$)) or HCC) [Words] |
| Science Citation Index ‐ Expanded (Web of Science) | 1900 to September 2019 | #5 #4 AND #3 #4 TS=(random* or blind* or placebo* or meta‐analys*) #3 #2 AND #1 #2 TS=(((liver or hepato*) and (carcinom* or cancer* or neoplasm* or malign* or tumo*)) or HCC) #1 TS=(radioembol* or embol* or TheraSphere or SIR‐Sphere) |
| Conference Proceedings Citation Index – Science (Web of Science) |
1990 to September 2019 | #5 #4 AND #3 #4 TS=(random* or blind* or placebo* or meta‐analys*) #3 #2 AND #1 #2 TS=(((liver or hepato*) and (carcinom* or cancer* or neoplasm* or malign* or tumo*)) or HCC) #1 TS=(radioembol* or embol* or TheraSphere or SIR‐Sphere) |
Data and analyses
Comparison 1. Radioembolisation versus sorafenib in locally advanced hepatocellular carcinoma.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Overall survival | 2 | Hazard Ratio (Random, 95% CI) | 1.12 [0.97, 1.30] | |
| 2 Disease control rate | 2 | 748 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.84, 1.05] |
| 3 Fatigue | 2 | 734 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.43 [0.25, 0.73] |
| 4 Hand‐foot skin reaction | 2 | 734 | Risk Ratio (M‐H, Random, 95% CI) | 0.02 [0.00, 0.06] |
| 5 Skin rash | 2 | 734 | Risk Ratio (M‐H, Random, 95% CI) | 0.11 [0.04, 0.34] |
| 6 Diarrhoea | 2 | 734 | Risk Ratio (M‐H, Random, 95% CI) | 0.11 [0.04, 0.34] |
| 7 Hypertension | 2 | 734 | Risk Ratio (M‐H, Random, 95% CI) | 0.10 [0.01, 0.88] |
| 8 Hypoalbuminemia | 2 | 734 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.84, 1.38] |
Comparison 2. Radioembolisation versus chemoembolisation for intermediate‐stage hepatocellular carcinoma.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Serious adverse events | 3 | 97 | Risk Ratio (M‐H, Random, 95% CI) | 1.47 [0.66, 3.25] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Chow 2018.
| Methods | Randomised phase III trial in the Asia‐Pacific region | |
| Participants | 360 patients with locally advanced HCC (defined as BCLC B or C without extrahepatic disease) were randomly assigned from 11 countries in the Asia‐Pacific region. Patients may or may not have portal vein thrombosis, and they were not amenable to curative treatment modalities. Mean age was 59.5 years for the radioembolisation group vs 57.7 years for the sorafenib group. Males represent 80.8% of trial participants in the radioembolisation group and 84.8% of those in the sorafenib group | |
| Interventions | Group 1: yttrium‐90 microsphere radioembolisation (182 participants) Group 2: sorafenib monotherapy (178 participants) | |
| Outcomes | Overall survival; progression‐free survival (according to RECIST); tumour response rate; disease control rate | |
| Notes | Sirtex Medical was a collaborating sponsor of the trial, as reported in the clinicaltrial.gov record of the trial | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random assignment was performed through an Internet application at the patient level |
| Allocation concealment (selection bias) | Low risk | Random assignment was performed through an Internet application at the patient level |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | This is an open‐label study |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Tumour response was assessed every 12 weeks from the date of random assignment to disease progression, through central review by radiologists at the National Cancer Center Singapore, who were blinded to the treatment received |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | The publication contains a flow diagram clarifying the fate of all participants who were assessed for eligibility |
| Selective reporting (reporting bias) | High risk | Liver resection rate and liver transplantation rate were reported as endpoints in the clinicaltrials.gov record of the study, but they cannot be found in the final publication |
Kolligs 2015.
| Methods | Multi‐centre pilot randomised trial (conducted at the University of Munich, Germany, and the Clinica Universidad de Navarra, Pamplona, Spain) | |
| Participants | Between July 2007 and June 2011, 28 people with unresectable hepatocellular carcinoma without portal vein occlusion were randomised to either: Group 1: radioembolisation (13 participants) or Group 2: chemoembolisation (15 participants) Mean age was 65.8 years for the radioembolisation group vs 66.7 years for the TACE group. Males represent 84.6% of patients in the radioembolisation arm and 86.7% of those in the TACE arm |
|
| Interventions | Either chemoembolisation (at 6‐weekly intervals until tumour enhancement was not observed on magnetic resonance imaging or disease progression) or single‐session radioembolisation (yttrium‐90 resin microspheres) | |
| Outcomes | Health‐related quality of life; progression‐free survival; overall survival; overall response rate (using RECIST); disease control rate | |
| Notes | The trial was supported by Sirtex Medical | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The method of sequence generation was not specified |
| Allocation concealment (selection bias) | Low risk | Each site received a series of consecutively numbered sealed envelopes, containing a card indicating the randomisation result |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Practically, participants and personnel must have known the allocation during treatment (either radioembolisation or chemoembolisation) |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of outcome assessment was not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There was no evidence of missing data within the final publication. The fate of all initially screened patients was described |
| Selective reporting (reporting bias) | Unclear risk | We could not locate a clinicaltrial.gov record for this trial for comparison with the final publication |
Pitton 2015.
| Methods | Prospective, single‐centre, randomised trial with 2 parallel treatment groups (Johannes Gutenberg University Medical Centre, Germany) A reliable power calculation was not feasible; thus, this study was labelled a pilot study This study is registered at www.clinicaltrials.gov as NCT01798160 |
|
| Participants | 24 participants with histologically proven intermediate‐stage HCC (BCLC B), Child‐Pugh class A‐B7, and ECOG of 0. Mean age for the radioembolisation group was 71.8 years vs 70.5 years for the TACE group. 8 trial participants in the radioembolisation group were males as were 10 participants in the TACE group | |
| Interventions | Group 1: radioembolisation (12 participants) Group 2: drug‐eluting bead transarterial chemoembolisation (DEB‐TACE) (12 participants) | |
| Outcomes | Progression‐free survival (according to mRECIST); overall survival; time to progression; time to locally non‐treatable progression | |
| Notes | The trial was sponsored by Johannes Gutenberg University Mainz (as per clinicaltrial.gov record) with no evidence of industry involvement | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Treatment allocation was pre‐determined by an independent statistician and used a randomised block design |
| Allocation concealment (selection bias) | Low risk | Treatment allocation was pre‐determined by an independent statistician and used a randomised block design |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Practically, it is impossible to blind participants or personnel in this trial given the completely different procedure associated with experimental intervention vs control intervention |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of outcome assessment was not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | The publication contains a flow diagram clarifying the fate of all participants who were assessed for eligibility |
| Selective reporting (reporting bias) | Low risk | All outcomes provided in the clinicaltrials.gov record of the trial were reported in the final publication |
Ricke 2019.
| Methods | SORAfenib in combination with local MICro‐therapy guided by gadolinium‐EOB‐DTPA‐enhanced MRI (SORAMIC) (EudraCT2009‐012576‐27, NCT0112 6645) is a prospective study that comprised 3 substudies (i) Comparison of gadolinium‐ethoxybenzyl‐diethylenetriamine pentaacetic acid (gadoxetate disodium[Gd‐EOB‐DTPA] Primovist)‐enhanced magnetic resonance imaging (MRI) vs contrast‐enhanced multi‐slice computed tomography (CT) for stratification of patients to a local ablation (curative treatment) or palliative treatment group (ii) Comparison of radiofrequency ablation (RFA) plus sorafenib vs control (RFA plus matching placebo) on time to recurrence (iii) Comparison of selective internal radiation therapy (SIRT; also known as radioembolisation) with 90‐yttrium‐loaded (Y‐90) resin microspheres combined with sorafenib compared with control (sorafenib alone) on overall survival (OS) Ricke 2019 reports on the outcomes of the part iii study (the palliative treatment group). See above SORAMIC is a randomised controlled trial comprising diagnostic, local ablation, and palliative cohorts. Based on diagnostic study results, patients were assigned to local ablation or palliative cohorts. In the palliative cohort, patients not eligible for TACE were randomised 11:10 to SIRT plus sorafenib (SIRT + sorafenib) or sorafenib alone The study was conducted at 38 sites in 12 countries in Europe and Turkey. Patients were recruited into the SORAMIC study between 5 January 2011 and 19 April 2016, and 424 were allocated to the palliative treatment cohort In the ITT palliative treatment cohort, 216 participants were randomised to SIRT + sorafenib and 208 to sorafenib alone The PP population comprised 114 participants randomised to SIRT + sorafenib and 174 who received sorafenib alone The safety population comprised 159 participants who received SIRT + sorafenib and 182 who received sorafenib alone Median age was 66 years in both groups. Males represent 85.4% in the combination group vs 85.5% in the sorafenib group |
|
| Participants | Participants in the palliative treatment group were people with unresectable hepatocellular carcinoma who were poor candidates for transarterial (chemo)embolisation (including those not responding to transarterial chemoembolisation) with preserved liver function (Child‐Pugh ≤ B7) and Eastern Cooperative Oncology Group performance status < 2 | |
| Interventions | For the palliative treatment group: Radioembolisation with yttrium‐90 resin microspheres followed by sorafenib or sorafenib only Group 1 (radioembolisation plus sorafenib): 216 participants Group 2 (sorafenib only): 208 participants |
|
| Outcomes | For the palliative treatment group, the primary outcome was overall survival (OS; Kaplan‐Meier analysis) in the intention‐to‐treat population | |
| Notes | Bayer and Sirtex Medical were collaborating sponsors for this trial We contacted the corresponding author of this publication through email on 6/10/2019 to inquire about some missing data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Following a pre‐defined randomisation plan, patients eligible for the palliative treatment group were randomised 11:10 to the SIRT + sorafenib or sorafenib arm. The 11:10 ratio was chosen to account for patients lost in the combination arm for technical ineligibility of SIRT, assuming an equal patient number as a result. Randomisation was performed by employing an interactive voice response system (IVRS) |
| Allocation concealment (selection bias) | Low risk | Randomisation was done by employing an IVRS Randomisation and stratification were carried out by centre and separately for participants with and without portal vein thrombosis |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | This is an open‐label study |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of outcome assessment was not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | There was no evidence of missing data within the final publication. The fate of all initially screened patients was described Any withdrawals from the study due to AEs were reported |
| Selective reporting (reporting bias) | High risk | Quality of life was reported as an endpoint in the clinicaltrials.gov record, but not in the final publication |
Salem 2016.
| Methods | Randomised phase II trial | |
| Participants | 45 participants with BCLC A or B HCC were enrolled. Patients have unablatable/unresectable disease, no vascular invasion, and Child‐Pugh A/B | |
| Interventions | Conventional chemoembolisation (21 participants) or yttrium‐90 microsphere radioembolisation (24 participants) | |
| Outcomes | Overall survival; time to progression; adverse events | |
| Notes | Progression was defined as follows:
WHO: 25% increase in bi‐dimensional cross‐product
EASL: 25% increase in arterial enhancement Portal vein tumour thrombus development Index lesions: lesions requiring re‐treatment because of worsening circumferential enhancement New lesions or extrahepatic metastases There was no evidence of industry participation; the study was sponsored by Northwestern University |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The method of sequence generation was not specified |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation was not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | This is an open‐label study |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Blinding of outcome assessment was not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | The publication contains a flow diagram clarifying the fate of all patients who were assessed for eligibility |
| Selective reporting (reporting bias) | High risk | Quality of life was one of the secondary endpoints in the clinicaltrials.gov record; however, it was not reported in the final publication |
Vilgrain 2017.
| Methods | Multi‐centre, open‐label, randomised, controlled, investigator‐initiated, phase III trial done at 25 centres specialising in liver diseases in France Between 5 December 2011 and 12 March 2015, 467 patients were randomly assigned after 8 patients withdrew consent |
|
| Participants | 459 participants with HCC were included in the intention‐to‐treat population. They had ECOG performance status of 0 or 1, Child‐Pugh class A or B7, and locally advanced hepatocellular carcinoma (BCLC stage C) or new hepatocellular carcinoma not eligible for surgical resection, liver transplantation, or thermal ablation after a previously cured hepatocellular carcinoma (cured by surgery or thermoablative therapy), or hepatocellular carcinoma with 2 unsuccessful rounds of transarterial chemoembolisation. Patients should not have had extrahepatic disease | |
| Interventions | Group 1: yttrium‐90 microsphere radioembolisation 2 to 5 weeks after randomisation (237 participants)
Group 2: sorafenib monotherapy (400 mg twice daily) (222 participants) In the SIRT group, 53 (22%) of 237 participants did not receive SIRT; 26 (49%) of these 53 participants were treated with sorafenib Median follow‐up was 27.9 months (IQR 21·9–33·6) in the SIRT group and 28.1 months (20·0–35·3) in the sorafenib group |
|
| Outcomes | Overall survival; progression‐free survival (defined by RECIST); disease control rate; response rate; quality of life | |
| Notes | This trial was funded by Sirtex Medical | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Patients were randomly assigned (1:1) by a permutated block method with block sizes 2 and 4 to receive continuous oral sorafenib (400 mg twice daily) or selective internal radiation therapy (SIRT) with 90Y‐loaded resin microspheres 2 to 5 weeks after randomisation. Patients were stratified according to randomising centre |
| Allocation concealment (selection bias) | Unclear risk | The randomisation list was prepared by a computer‐generated permutated block method |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | This is an open‐label study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | The funder, investigators, patients, and research staff remained masked to the randomisation list but were not masked to treatment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | The publication contains a flow diagram clarifying the fate of all patients who were assessed for eligibility |
| Selective reporting (reporting bias) | High risk | Healthcare costs were reported as one of the secondary endpoints at clinicaltrials.gov, but they were not commented upon in the primary publication of the study (study authors mentioned that they will report it subsequently elsewhere, but these data were not published yet) |
BCLC: Barcelona Clinic Liver Cancer; EASL: European Association for the Study of the Liver; ECOG: Eastern Cooperative Oncology Group; DEB‐TACE: drug‐eluting beads‐transarterial chemoembolisation; HCC: hepatocellular carcinoma; mRECIST: modified RECIST; RECIST: Response Evaluation Criteria in Solid Tumors; TACE: transarterial chemoembolisation; WHO: World Health Organization.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| El Fouly 2015 | Retrospective study |
| Kulik 2014 | Radioembolisation administered in both study groups |
| Mazzaferro 2013 | Single‐arm non‐randomised study |
Characteristics of ongoing studies [ordered by study ID]
NCT01381211.
| Trial name or title | Transarterial radioembolisation versus chemoembolisation for the treatment of HCC: a multicenter randomised controlled trial (TRACE trial) |
| Methods | Randomised phase II |
| Participants | People with intermediate‐stage hepatocellular carcinoma |
| Interventions | Intervention 1: yttrium‐90 radioembolisation Intervention 2: transarterial chemoembolisation with drug‐eluting beads |
| Outcomes | Primary outcome
Secondary outcomes
|
| Starting date | September 2011 |
| Contact information | Prof. Luc Defreyne: luc.defreyne@ugent.be |
| Notes | Estimated enrolment: 140. On review of the clinicaltrial.gov record of this trial in October 2019, its recruitment status seems to be unknown. Email was sent to the corresponding author on 6/10/2019 to get an update about the recruitment status. The reply from study authors suggests that they plan to present their results in 2020 |
NCT01556490.
| Trial name or title | A phase III clinical trial of intra‐arterial theraSphere® in the treatment of patients with unresectable hepatocellular carcinoma |
| Methods | Randomised phase III |
| Participants | People with unresectable hepatocellular carcinoma for whom treatment with standard‐of‐care sorafenib is planned |
| Interventions | Intervention 1: standard‐of‐care sorafenib plus TheraSphere (yttrium‐90 microspheres) Intervention 2: standard‐of‐care sorafenib, with no added therapy |
| Outcomes | March 2012 |
| Starting date | Primary outcome
|
| Contact information | Clinical development, BTG Email: TheraSphereClinical@btgplc.com |
| Notes | Actual enrolment: 526. This trial is currently active, not recruiting |
HCC: hepatocellular carcinoma.
Differences between protocol and review
The following modifications were made.
The all‐cause mortality outcome was modified to include median overall survival; it now reads as follows: "All‐cause mortality (which can be reported as median overall survival)". This was done because most of the radioembolisation trials report this outcome as median overall survival, not as one‐year mortality.
We added post hoc the outcome "Liver transplantation following treatment", which is one of the frequently measured outcomes in trials of radioembolisation for people with early‐ or intermediate‐stage hepatocellular carcinoma.
Contributions of authors
Omar Abdel‐Rahman: wrote the review. Zeinab Elsayed: revised the review. Both review authors accepted the final review for publication.
Sources of support
Internal sources
None, Other.
External sources
None, Other.
Declarations of interest
Omar Abdel‐Rahman: none known. Zeinab Elsayed: none known.
New search for studies and content updated (conclusions changed)
References
References to studies included in this review
Chow 2018 {published data only}
- Chow PKH, Gandhi M, Tan SB, Khin MW, Khasbazar A, Ong J, et al. SIRveNIB: selective internal radiation therapy versus sorafenib in Asia‐Pacific patients with hepatocellular carcinoma. Journal of Clinical Oncology 2018;36(19):1913‐21. [DOI] [PubMed] [Google Scholar]
Kolligs 2015 {published data only}
Pitton 2015 {published data only}
- Pitton MB, Kloeckner R, Ruckes C, Wirth GM, Eichhorn W, Worns MA, et al. Randomized comparison of selective internal radiotherapy (SIRT) versus drug‐eluting bead transarterial chemoembolization (DEB‐TACE) for the treatment of hepatocellular carcinoma. Cardiovascular and Interventional Radiology 2015;38(2):352‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ricke 2019 {published data only}
- Ricke J, Klumpen HJ, Amthauer H, Bargellini I, Bartenstein P, Toni EN, et al. Impact of combined selective internal radiation therapy and sorafenib on survival in advanced hepatocellular carcinoma. Journal of Hepatology 2019;71(6):1164‐74. [DOI] [PubMed] [Google Scholar]
Salem 2016 {published data only}
- Salem R, Gordon AC, Mouli S, Hickey R, Kallini J, Gabr A, et al. Y90 radioembolization significantly prolongs time to progression compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology 2016;151(6):1155‐63. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vilgrain 2017 {published data only}
- Vilgrain V, Pereira H, Assenat E, Guiu B, Ilonca AD, Pageaux GP, et al. Efficacy and safety of selective internal radiotherapy with yttrium‐90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): an open‐label randomised controlled phase 3 trial. Lancet Oncology 2017;18(12):1624‐36. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
El Fouly 2015 {published data only}
- Fouly A, Ertle J, Dorry A, Shaker M, Dechêne A, Abdella H, et al. In intermediate stage hepatocellular carcinoma: radioembolization with yttrium 90 or chemoembolization?. Liver International 2015;35:627‐35. [DOI] [PubMed] [Google Scholar]
Kulik 2014 {published data only}
- Kulik L, Vouche M, Koppe S, Lewandowski R, Mulcahy M, Ganger D, et al. Prospective randomized pilot study of Y90 +/‐ sorafenib as bridge to transplantation in hepatocellular carcinoma. Journal of Hepatology 2014;61(2):309‐17. [DOI] [PubMed] [Google Scholar]
Mazzaferro 2013 {published data only}
- Mazzaferro V, Sposito C, Bhoori S, Romito R, Chiesa C, Morosi C, et al. Yttrium‐90 radioembolization for intermediate‐advanced hepatocellular carcinoma: a phase 2 study. Hepatology (Baltimore, Md.) 2013;57(5):1826‐37. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
NCT01381211 {published data only}
- Transarterial radioembolisation versus chemoembolisation for the treatment of HCC: a multicenter randomised controlled trial (TRACE trial). Ongoing study September 2011.
NCT01556490 {published data only}
- A phase III clinical trial of intra‐arterial theraSphere® in the treatment of patients with unresectable hepatocellular carcinoma. Ongoing study Primary outcomeOverall survival.
Additional references
Abdel‐Rahman 2013
- Abdel‐Rahman O, Elsayed Z. Combination trans arterial chemoembolization (TACE) plus sorafenib for the management of unresectable hepatocellular carcinoma: a systematic review of the literature. Digestive Disease and Science 2013;58(12):3389‐96. [DOI: 10.1007/s10620-0132872-x] [DOI] [PubMed] [Google Scholar]
Abdel‐Rahman 2018
- Abdel‐Rahman O, Cheung WY. The expanding role of systemic therapy in the management of hepatocellular carcinoma. Canadian Journal of Gastroenterology & Hepatology 2018;2018:4763832. [DOI] [PMC free article] [PubMed] [Google Scholar]
Balshem 2011
- Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines 3: rating the quality of evidence ‐ introduction. Journal of Clinical Epidemiology 2011;64:401‐6. [DOI] [PubMed] [Google Scholar]
Bartlett 2008
- Bartlett A, Heaton N. Hepatocellular carcinoma: defining the place of surgery in an era of organ shortage. World Journal of Gastroenterology 2008;14(28):4445‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Brok 2008
- Brok J, Thorlund K, Gluud C, Wetterslev J. Trial sequential analysis reveals insufficient information size and potentially false positive results in many meta‐analyses. Journal of Clinical Epidemiology 2008;61:763‐9. [DOI] [PubMed] [Google Scholar]
Brok 2009
- Brok J, Thorlund K, Wetterslev J, Gluud C. Apparently conclusive meta‐analyses may be inconclusive ‐ trial sequential analysis adjustment of random error risk due to repetitive testing of accumulating data in apparently conclusive neonatal meta‐analyses. International Journal of Epidemiology 2009;38(1):287‐98. [DOI] [PubMed] [Google Scholar]
Bruix 2011
- Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology (Baltimore, Md.) 2011;53(3):1020‐2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Castellini 2018
- Castellini G, Bruschettini M, Gianola S, Gluud C, Moja L. Assessing imprecision in Cochrane systematic reviews: a comparison of GRADE and Trial Sequential Analysis. Systematic Reviews 2018;7(1):110. [DOI] [PMC free article] [PubMed] [Google Scholar]
Choi 2005
- Choi J‐H, Ahn M‐J, Rhim H‐C, Kim J‐W, Lee G‐H, Lee Y‐Y, et al. Comparison of WHO and RECIST criteria for response in metastatic colorectal carcinoma. Cancer Research and Treatment 2005;37(5):290‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
D'Avola 2009
- D'Avola D, Lñarrairaegui M, Bilbao JI, Martinez‐Cuesta A, Alegre F, Herrero JI, et al. A retrospective comparative analysis of the effect of Y90‐radioembolization on the survival of patients with unresectable hepatocellular carcinoma. Hepato‐gastroenterology 2009;56(96):1683‐8. [PubMed] [Google Scholar]
DeMets 1987
- DeMets DL. Methods of combining randomised clinical trials: strengths and limitations. Statistics in Medicine 1987;6(3):341‐50. [DOI] [PubMed] [Google Scholar]
DerSimonian 1986
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7(3):177‐88. [DOI] [PubMed] [Google Scholar]
EASL 2018
- EASL. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. Journal of Hepatology 2018;69(1):182‐236. [DOI] [PubMed] [Google Scholar]
EASL/EORTC 2012
- European Association for the Study of the Liver, European Organisation for Research and Treatment of Cancer. EASL‐EORTC clinical practice guidelines: management of hepatocellular carcinoma. Journal of Hepatology 2012;56(4):908‐43. [DOI] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ (Clinical Research Ed.) 1997;315:629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Eisenhauer 2009
- Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). European Journal of Cancer 2009;45(2):228‐47. [DOI] [PubMed] [Google Scholar]
Facciorusso 2016
- Facciorusso A, Serviddio G, Muscatiello N. Transarterial radioembolization vs chemoembolization for hepatocarcinoma patients: a systematic review and meta‐analysis. World Journal of Hepatology 2016;8(18):770‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
FACT‐Hep 2007
- FACT‐Hep: For patients with Hepatobiliary cancer (liver, bile duct and pancreas). www.facit.org/FACITOrg/Questionnaires 2007 (accessed 3 December 2019).
Gartlenher 2018
- Gartlehner G, Nussbaumer‐Streit B, Wagner G, Patel S, Swinson‐Evans T, Dobrescu A. Increased risks for random errors are common in outcomes graded as high certainty of evidence. Journal of Clinical Epidemiology 2019;106:50‐9. [DOI] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 4 December 2018. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Graham 2013
- Graham J, Newman D, Smirniotopolous J, Shetty K, Slidell M, Johnson L. Transplantation for hepatocellular carcinoma in younger patients has an equivocal survival advantage as compared with resection. Transplantation Proceedings 2013;45(1):265‐71. [DOI] [PubMed] [Google Scholar]
Guyatt 2011a
- Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction ‐ GRADE evidence profiles and summary of findings tables. Journal of Clinical Epidemiology 2011;64(4):383‐94. [PUBMED: 21195583] [DOI] [PubMed] [Google Scholar]
Guyatt 2011b
- Guyatt GH, Oxman AD, Kunz R, Atkins D, Brozek J, Vist G, et al. GRADE guidelines: 2. Framing the question and deciding on important outcomes. Journal of Clinical Epidemiology 2011;64(4):395‐400. [PUBMED: 21194891] [DOI] [PubMed] [Google Scholar]
Guyatt 2011c
- Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso‐Coello P, et al. GRADE guidelines: 4. Rating the quality of evidence ‐ study limitations (risk of bias). Journal of Clinical Epidemiology 2011;64(4):407‐15. [PUBMED: 21247734] [DOI] [PubMed] [Google Scholar]
Guyatt 2011d
- Guyatt GH, Oxman AD, Montori V, Vist G, Kunz R, Brozek J, et al. GRADE guidelines: 5. Rating the quality of evidence ‐ publication bias. Journal of Clinical Epidemiology 2011;64(12):1277‐82. [PUBMED: 21802904] [DOI] [PubMed] [Google Scholar]
Guyatt 2011e
- Guyatt GH, Oxman AD, Kunz R, Brozek J, Alonso‐Coello P, Rind D, et al. GRADE guidelines: 6. Rating the quality of evidence ‐ imprecision. Journal of Clinical Epidemiology 2011;64(12):1283‐93. [PUBMED: 21839614] [DOI] [PubMed] [Google Scholar]
Guyatt 2011f
- Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 7. Rating the quality of evidence ‐ inconsistency. Journal of Clinical Epidemiology 2011;64(12):1294‐302. [PUBMED: 21803546] [DOI] [PubMed] [Google Scholar]
Guyatt 2011g
- Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. GRADE guidelines: 8. Rating the quality of evidence ‐ indirectness. Journal of Clinical Epidemiology 2011;64(12):1303‐10. [PUBMED: 21802903] [DOI] [PubMed] [Google Scholar]
Guyatt 2011h
- Guyatt GH, Oxman AD, Sultan S, Glasziou P, Akl EA, Alonso‐Coello P, et al. GRADE guidelines: 9. Rating up the quality of evidence. Journal of Clinical Epidemiology 2011;64(12):1311‐6. [PUBMED: 21802902] [DOI] [PubMed] [Google Scholar]
Guyatt 2013a
- Guyatt G, Oxman AD, Sultan S, Brozek J, Glasziou P, Alonso‐Coello P, et al. GRADE guidelines: 11. Making an overall rating of confidence in effect estimates for a single outcome and for all outcomes. Journal of Clinical Epidemiology 2013;66(2):151‐7. [DOI] [PubMed] [Google Scholar]
Guyatt 2013b
- Guyatt GH, Oxman AD, Santesso N, Helfand M, Vist G, Kunz R, et al. GRADE guidelines: 12. Preparing Summary of Findings tables ‐ binary outcomes. Journal of Clinical Epidemiology 2013;66(2):158‐72. [DOI] [PubMed] [Google Scholar]
Guyatt 2013c
- Guyatt GH, Thorlund K, Oxman AD, Walter SD, Patrick D, Furukawa TA, et al. GRADE guidelines: 13. Preparing Summary of Findings tables ‐ continuous outcomes. Journal of Clinical Epidemiology 2013;66(2):173‐83. [DOI] [PubMed] [Google Scholar]
Guyatt 2013d
- Guyatt G, Andrews J, Oxman AD, Alderson P, Dahm P, Falck‐Ytter Y, et al. GRADE guidelines: 15. Going from evidence to recommendations: the significance and presentation of recommendations. Journal of Clinical Epidemiology 2013;66(7):719‐25. [DOI] [PubMed] [Google Scholar]
Guyatt 2017
- Guyatt GH, Ebrahim S, Alonso‐Coello P, Johnston BC, Mathioudakis AG, Briel M, et al. GRADE guidelines 17: assessing the risk of bias associated with missing participant outcome data in a body of evidence. Journal of Clinical Epidemiology 2017;87:14‐22. [PUBMED: 28529188] [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JP, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 6 (updated July 2019). The Cochrane Collaboration, 2019. Available from www.cochrane‐handbook.org.
Hollis 1999
- Hollis S, Campbell F. What is meant by intention to treat analysis? Survey of published randomised controlled trials. BMJ (Clinical Research Ed.) 1999;319:670‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
ICH‐GCP 1997
- International Conference on Harmonisation Expert Working Group. International conference on harmonisation of technical requirements for registration of pharmaceuticals for human use. ICH harmonised tripartite guideline. Guideline for good clinical practice CFR & ICH Guidelines. Vol. 1, Philadelphia (PA): Barnett International/PAREXEL, 1997. [Google Scholar]
Jakobsen 2014
- Jakobsen J, Wetterslev J, Winkel P, Lange T, Gluud C. Thresholds for statistical and clinical significance in systematic reviews with meta‐analytic methods. BMC Medical Research Methodology 2014;14(120):1‐13. [DOI: 10.1186/1471-2288-14-120] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kjaergard 2001
- Kjaergard LL, Villumsen J, Gluud C. Reported methodologic quality and discrepancies between large and small randomised trials in meta‐analyses. Annals of Internal Medicine 2001;135(11):982‐9. [DOI] [PubMed] [Google Scholar]
Kulik 2006
- Kulik LM, Atassi B, Holsbeeck L, Souman T, Lewandowski RJ, Mulcahy MF, et al. Yttrium‐90 microspheres (TheraSphere) treatment of unresectable hepatocellular carcinoma: down staging to resection, RFA and bridge to transplantation. Journal of Surgical Oncology 2006;94:572‐86. [DOI] [PubMed] [Google Scholar]
Kwon 2012
- Kwon O, Jung Y, Bae K. Anti‐hepatitis B core positivity as a risk factor for hepatocellular carcinoma in alcoholic cirrhosis: a case‐control study. Alcohol (Fayetteville, N.Y.) 2012;46:537‐41. [DOI] [PubMed] [Google Scholar]
Levy 2002
- Levy I, Sherman M. Staging of hepatocellular carcinoma: assessment of the CLIP, Okuda, and Child‐Pugh staging systems in a cohort of 257 patients in Toronto. Gut 2002;50(6):881‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lewandowski 2009
- Lewandowski RJ, Kulik LM, Riaz A, Senthilnathan S, Mulcahy MF, Ryu RK, et al. A comparative analysis of transarterial down staging for hepatocellular carcinoma: chemoembolization versus radioembolization. American Journal of Transplantation 2009;9(8):1920‐8. [DOI] [PubMed] [Google Scholar]
Liu 2014
- Liu C, Duan LG, Lu WS, Yan LN, Xiao GQ, Jiang L, et al. Prognosis evaluation in patients with hepatocellular carcinoma after hepatectomy: comparison of BCLC, TNM and Hangzhou Criteria Staging Systems. PLoS One 2014;9(8):e103228. [DOI] [PMC free article] [PubMed] [Google Scholar]
Macaskill 2001
- Macaskill P, Walter SD, Irwig L. A comparison of methods to detect publication bias in meta‐analysis. Statistics in Medicine 2001;20:641‐54. [DOI] [PubMed] [Google Scholar]
Maffione 2013
- Maffione AM, Ferretti A, Vinjamuri S, Rubello D. The PERCIST criteria: an insightful appraisal. Nuclear Medicine Communications 2013;34(7):619‐20. [DOI] [PubMed] [Google Scholar]
Mantel 1959
- Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. Journal of the National Cancer Institute 1959;2(4):719‐48. [PubMed] [Google Scholar]
Masuzaki 2009
- Masuzaki R, Yoshida H, Omata M. Hepatitis C and hepatocellular carcinoma. Hepatocellular Carcinoma Diagnosis and Treatment. New York: Humana Press, 2009:45‐50. [Google Scholar]
Mazzaferro 1996
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. New England Journal of Medicine 1996;334:693‐9. [DOI] [PubMed] [Google Scholar]
Medscape 2018
- Patel A. Hepatocellular Carcinoma Staging. https://emedicine.medscape.com/article/2007061‐overview 2008; last date of access 22/1/2020.
Moher 1998
- Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et al. Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta‐analyses?. Lancet 1998;352(9128):609‐13. [DOI] [PubMed] [Google Scholar]
Murthy 2011
- Murthy R, Mutha P, Gupta S. Yttrium‐90 radioembolotherapy for hepatocellular cancer. Hepatocellular Carcinoma: Targeted Therapy and Multidisciplinary Care. New York: Springer, 2011:50‐60. [Google Scholar]
Mustafa 2013
- Mustafa RA, Santesso N, Brozek J, Akl EA, Walter SD, Norman G, et al. The GRADE approach is reproducible in assessing the quality of evidence of quantitative evidence syntheses. Journal of Clinical Epidemiology 2013;66(7):736‐42; quiz 742.e1‐5. [PUBMED: 23623694] [DOI] [PubMed] [Google Scholar]
Okuda 1985
- Okuda K, Ohtsuki T, Obata H, Tomimatsu M, Okazaki N, Hasegawa H, et al. Natural history of hepatocellular carcinoma and prognosis in relation to treatment: study of 850 patients. Cancer 1985;56:918‐28. [DOI] [PubMed] [Google Scholar]
Oliveri 2011
- Oliveri RS, Wetterslev J, Gluud C. Transarterial (chemo)embolisation for unresectable hepatocellular carcinoma. Cochrane Database of Systematic Reviews 2011, Issue 3. [DOI: 10.1002/14651858.CD004787.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Parmar 1998
- Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta‐analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17(24):2815‐34. [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- The Nordic Cochrane Centre, Cochrane. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, Cochrane, 2014.
Rhee 2005
- Rhee TK, Omary RA, Gates V, Mounajjed T, Larson AC, Barakat O, et al. The effect of catheter‐directed CT angiography on yttrium‐90 radioembolization treatment of hepatocellular carcinoma. Journal of Vascular and Interventional Radiology 2005;16:1085‐91. [DOI] [PubMed] [Google Scholar]
Riaz 2011
- Riaz A, Memon K, Miller FH, Nikolaidis P, Kulik LM, Lewandowski RJ, et al. Role of the EASL, RECIST, and WHO response guidelines alone or in combination for hepatocellular carcinoma: radiologic‐pathologic correlation. Journal of Hepatology 2011;54(4):695‐704. [DOI] [PMC free article] [PubMed] [Google Scholar]
Royle 2003
- Royle P, Milne R. Literature searching for randomised controlled trials used in Cochrane reviews: rapid versus exhaustive searches. International Journal of Technology Assessment in Health Care 2003;19(4):591‐603. [DOI] [PubMed] [Google Scholar]
Saini 2019
- Saini A, Wallace A, Alzubaidi S, Knuttinen MG, Naidu S, Sheth R. History and evolution of yttrium‐90 radioembolization for hepatocellular carcinoma. Journal of Clinical Medicine 2019;8(1):55. [10.3390/jcm8010055] [DOI] [PMC free article] [PubMed] [Google Scholar]
Salem 2010
- Salem R, Lewandowski RJ, Mulcahy MF, Riaz A, Ryu RK, Ibrahim S, et al. Radioembolization for hepatocellular carcinoma using yttrium‐90 microspheres: a comprehensive report of long‐term outcomes. Gastroenterology 2010;138(1):52‐64. [DOI] [PubMed] [Google Scholar]
Sanyal 2010
- Sanyal AJ, Yoon SK, Lencioni R. The etiology of hepatocellular carcinoma and consequences for treatment. Oncologist 2010;15(Suppl 4):14‐22. [DOI] [PubMed] [Google Scholar]
Savović 2012a
- Savović J, Jones HE, Altman DG, Harris RJ, Jüni P, Pildal J, et al. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Health Technology Assessment 2012;16(35):1‐82. [DOI] [PubMed] [Google Scholar]
Savović 2012b
- Savović J, Jones HE, Altman DG, Harris RJ, Jüni P, Pildal J, et al. Influence of reported study design characteristics on intervention effect estimates from randomized, controlled trials. Annals of Internal Medicine 2012;157(6):429‐38. [DOI] [PubMed] [Google Scholar]
Savović 2018
- Savović J, Turner RM, Mawdsley D, Jones HE, Beynon R, Higgins JP, et al. Association between risk‐of‐bias assessments and results of randomized trials in Cochrane Reviews: the ROBES Meta‐Epidemiologic Study. American Journal of Epidemiology 2018;187(5):1113‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schiefelbein 2012
- Schiefelbein E, Zekri AR, Newton DW, Soliman GA, Banerjee M, Hung ChW, et al. Hepatitis C virus and other risk factors in hepatocellular carcinoma. Acta Virologica 2012;56(3):235‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schulz 1995
- Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995;273(5):408‐12. [DOI] [PubMed] [Google Scholar]
Storebø 2018
- Savović J, Turner RM, Mawdsley D, Jones HE, Beynon R, Higgins JPT, et al. Association between risk‐of‐bias assessments and results of randomized trials in Cochrane Reviews: The ROBES Meta‐Epidemiologic Study. American Journal of Epidemiology 2018;187(5):1113‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
Thorlund 2009
- Thorlund K, Devereaux PJ, Wetterslev J, Guyatt G, Ioannidis JP, Thabane L, et al. Can trial sequential monitoring boundaries reduce spurious inferences from meta‐analyses?. International Journal of Epidemiology 2009;38(1):276‐86. [DOI] [PubMed] [Google Scholar]
Thorlund 2010
- Thorlund K, Anema A, Mills E. Interpreting meta‐analysis according to the adequacy of sample size. An example using isoniazid chemoprophylaxis for tuberculosis in purified protein derivative negative HIV‐infected individuals. Clinical Epidemiology 2010;2:57‐66. [DOI] [PMC free article] [PubMed] [Google Scholar]
Thorlund 2011
- Thorlund K, Engstrøm J, Wetterslev J, Brok J, Imberger G, Gluud C. User manual for Trial Sequential Analysis (TSA). ctu.dk/tsa/files/tsa_manual.pdf 2011 (accessed 3 December 2019).
TSA 2011 [Computer program]
- Copenhagen Trial Unit. TSA ‐ Trial Sequential Analysis. Version 0.9.5.10 Beta. Copenhagen: Copenhagen Trial Unit, 2011.
Venkatanarasimha 2017
- Venkatanarasimha N, Gogna A, Tong KTA, Damodharan K, Chow PKH, Lo RHG, et al. Radioembolisation of hepatocellular carcinoma: a primer. Clinical Radiology 2017;72(12):1002‐13. [DOI] [PubMed] [Google Scholar]
Weis 2013
- Weis S, Franke A, Mössner J, Jakobsen JC, Schoppmeyer K. Radiofrequency (thermal) ablation versus no intervention or other interventions for hepatocellular carcinoma. Cochrane Database of Systematic Reviews 2013, Issue 12. [DOI: 10.1002/14651858.CD003046.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wetterslev 2008
- Wetterslev J, Thorlund K, Brok J, Gluud C. Trial sequential analysis may establish when firm evidence is reached in cumulative meta‐analysis. Journal of Clinical Epidemiology 2008;61(1):64‐75. [DOI] [PubMed] [Google Scholar]
Wetterslev 2009
- Wetterslev J, Thorlund K, Brok J, Gluud C. Estimating required information size by quantifying diversity in a random‐effects meta‐analysis. BMC Medical Research Methodology 2009;9:86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wetterslev 2017
- Wetterslev J, Jakobsen JC, Gluud C. Trial Sequential Analysis in systematic reviews with meta‐analysis. BMC Medical Research Methodology 2017;17(1):39. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wood 2008
- Wood L, Egger M, Gluud LL, Schulz KF, Jüni P, Altman GD, et al. Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions and outcomes: meta‐epidemiological study. BMJ (Clinical Research Ed.) 2008;336:601‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Yau 2008
- Yau T, Chan P, Epstein R, Poon RT. Evolution of systemic therapy of advanced hepatocellular carcinoma. World Journal of Gastroenterology 2008;14(42):6437‐41. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Abdel‐Rahman 2014
- Abdel‐Rahman OM, Elsayed Z. Yttrium‐90 microsphere radioembolisation for unresectable hepatocellular carcinoma. Cochrane Database of Systematic Reviews 2014, Issue 9. [DOI: 10.1002/14651858.CD011313] [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
Abdel‐Rahman 2016
- Abdel‐Rahman OM, Elsayed Z. Yttrium‐90 microsphere radioembolisation for unresectable hepatocellular carcinoma. Cochrane Database of Systematic Reviews 2016, Issue 2. [DOI: 10.1002/14651858.CD011313.pub2] [DOI] [PubMed] [Google Scholar]